
Abstract
Data sources
Medline, Embase, OpenGrey, Journal of Clinical Periodontology, Journal of Periodontology and a hand search of the bibliographies of retrieved publications.
Study selection
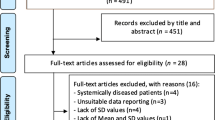
Two reviewers screened the title and abstract of 1134 studies from the literature and selected 37 suitable publications for inclusion following full text analysis of 109 papers and agreement between both reviewers. The search included observational, epidemiological studies and clinical trials that fufilled the inclusion criteria. The publications assessed contained a periodontal clinical examination and a validated OHRQoL questionnaire. There were no language restrictions and the review was performed according to the MOOSE statement.
Data extraction and synthesis
Data were extracted from each study applying the PECO format. The quality of the observational studies was evaluated by the Newcastle Ottawa Scale (NOS) and clinical trials by the (MINORS) methodological index for non-randomised studies. The Strength of Grading Taxonomy (SORT) was utilised to assess the level of evidence and strength of recommendation of the included studies. A meta-analysis was not undertaken due the heterogeneity of the included studies, therefore results were synthesised by applying a vote counting method.
Results
Thirty-seven studies included in the review were evaluated by the vote counting method. According to NOS and MINORS the risk of bias was identified as moderate with most studies assessing 50% to 83% of the parameters established. A level two for quality of evidence and a level B for strength of recommendation were applicable for the relationship between clinically diagnosed periodontal disease and OHRQoL. The evidence level was consistent across the studies. Nineteen of the studies examined a distinct population group with respect to diagnosis of systemic disease, socioeconomic status, demographic background or periodontal diagnosis. Twenty-eight of the included studies reported an association between periodontal diseases and OHRQoL while eight of the publications highlighted a dose-response relationship between and extent and severity of periodontal disease and the impact on OHRQoL.
Conclusions
The findings support the association between clinically diagnosed periodontal diseases and subjectively assessed OHRQoL with a dose-response relationship demonstrated. In summation, periodontal diseases play a significant role in oral health and impact on the QoL of affected individuals. In publications that undertook a full mouth recording the results were more evident, therefore a comprehensive periodontal exam in conjunction with a validated OHRQoL questionnaire is recommended.
Similar content being viewed by others


Commentary
The recognition that health and well-being is not merely a medical concept but is encompassed by the biopsychosocial model has been accepted for many years. The American Dental Association states ‘Oral health is a functional, structural, aesthetic, physiologic and psychological state of well-being and is essential to an individual's general health and quality of life’.1 The high prevalence and global health burden of periodontal diseases is well documented in the literature,2, 3 as is the associated systemic health impact on susceptible individuals.4, 5 Frequently, periodontal disease advances over many years often unknown to the patient, in spite of its ubiquitous nature and deleterious impact on the periodontium. It is often considered a ‘silent disease’ as the condition may present with swelling, bleeding and or tooth mobility in the complete absence of pain. The paper therefore raises a question - is periodontal disease actually a silent disease or does it impact on the OHRQoL of a patient? A useful previous review demonstrated an impairment of OHRQoL in patients with periodontal disease, but this paper was limited to seven publications (Al-Harthi et al. 2013).6
The aim of this review was to elucidate the relationship between clinical parameters of periodontal diseases and the impact on OHRQoL and to investigate the potential relationship between disease severity and the level of perceived impairment.
The authors searched extensively through the literature and included a concise and accurate flowchart to reflect the robust study selection process. To compliment this a search of Latin American and Chinese databases as well as a search for colloquial terms such as ‘gum disease’ may have been beneficial. The reviewers positively applied validated and recognised tools to evaluate the quality of the included studies. The studies were assessed by the Newcastle Ottawa Scale (NOS) and methodological index for non-randomised studies (MINORS) to analyse bias. The review also applied the SORT grading system to provide a recommendation for strength of evidence and level for quality of evidence. SORT is a validated grading system that evaluates the quantity, quality and consistency of evidence to guide authors in rating a single study or body or evidence.
The authors attempt to focus the review by applying the PECO format, however the diversity of studies perhaps creates too broad a data range for this to be effective. The heterogeneity of the studies included makes comparison and analysis difficult, for example one paper evaluates pregnant patients and another an elderly population. This is reflected by the broad range in the categories of population, intervention and outcome measures. The interventions evaluate dual diseases of gingivitis and periodontitis and there is a range of disease from mild to severe. The classification system for ‘disease state’ and periodontal clinical parameters contrasts between most of the studies as does the OHRQoL assessment tool. With respect to the OHRQoL, eight different survey formats are applied, an abbreviated format of the Oral Health Impact Profile was the most commonly utilised survey tool in 17 of the 37 studies included; this variety of tools makes synthesis of the data challenging, particularly in the case of a systematic review. The author discusses these limitations though and suggests the need for globally accepted definitions of periodontal diseases and OHRQoL to support future research. The analysis of results does highlight though that 28 of the studies demonstrate a relationship between periodontal diseases and OHRQoL. Within these results it is observed that the use of a full mouth recording system reveals this association far more frequently than partial mouth recording.
The author undertook commendable effort in this review to address an important issue, however quality of outcome was simply restricted by the paucity of high quality publications available and the high degree of heterogeneity as discussed above. This review will help to inform the planning for future valuable research and raised important issues around full mouth recording in periodontal research and the need for uniform internationally recognised classification systems for periodontal diseases and OHRQoL assessment in future research.
Although the quality of the review is diminished by the heterogeneity of the included studies and the fact that a meta-analysis is not feasible, it does make the findings more applicable to the general population and it would be reasonable to apply the findings of the research to our local population. Due to the broad diversity of the sample populations in the various studies with a vast range of age, gender, ethnicity, socioeconomic and medical backgrounds the findings of the review could reasonably be applied to a number of different settings.
Examining the comparable literature, another recently published systemic review also examines this issue.7 There are a number of differences though in the study hypothesis and methodology. The PECO question evaluates dentate patients as opposed to adults and only included patients in the comparison group without periodontal disease. The Ferreira paper conducts the review applying PRISMA guidelines in contrast to the MOOSE statement. Also, clinical trials were excluded as were studies including patients with a systemic disease that may impact on periodontal health. Despite these differences, the main finding that periodontal disease has a negative impact on OHRQoL and the extent of this impact is related to disease severity is analogous to the Buset et al. review.
Practice point
-
As clinicians, it is important we consider the relationship between periodontal diseases and oral health and the impact this can have on quality of life for our patients. Clinicians should be aware of the influence of periodontal diseases on OHRQoL and the impact it has on mastication, speech, social interactions and psychological well-being.
References
Glick M, Meyer DM . Defining oral health: a prerequisite for any health policy. J Am Dent Assoc 2014; 145:519–520.
Eke PI, Dye BA, Wei L, et al. Update on Prevalence of Periodontitis in Adults in the United States: NHANES 2009 to 2012. J Periodontol 2015; 86:611–622.
Chapple IL . Genco R ; Working group 2 of joint EFP/AAP workshop. Diabetes and periodontal diseases: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J Clin Periodontol 2013; 40:S106–112.
Linden GJ . Herzberg MC ; Working group 4 of joint EFP/AAP workshop. Periodontitis and systemic diseases: a record of discussions of working group 4 of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J Clin Periodontol 2013; 40:S20–23.
Al-Harthi LS, Cullinan MP, Leichter JW, Thomson WM . The impact of periodontitis on oral health-related quality of life: a review of the evidence from observational studies. Aust Dent J 2013; 58:274–277.
Ferreira MC, Dias-Pereira AC, Branco-de-Almeida LS, Martins CC, Paiva SM . Impact of periodontal disease on quality of life: a systematic review. J Periodontal Res 2017; 52:651–665.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Nicola U. Zitzmann, Department of Periodontology Endodontology and Cariology, University Center for Dental Medicine, University of Basel, Switzerland. E-mail: n.zitzmann@unibas.ch
Buset SL, Walter C, Friedmann A, Weiger R, Borgnakke WS, Zitzmann NU. Are periodontal diseases really silent? A systematic review of their effect on quality of life. J Clin Periodontol 2016; 43: 333-344. doi: 10.1111/jcpe.12517. Epub 2016 Mar 29. Review. PubMed PMID: 26810308.
Rights and permissions
About this article

Cite this article
Reynolds, I., Duane, B. Periodontal disease has an impact on patients' quality of life. Evid Based Dent 19, 14–15 (2018). https://doi.org/10.1038/sj.ebd.6401287
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401287
- Springer Nature Limited
This article is cited by
-
Association between the systemic immune inflammation index and periodontitis: a cross-sectional study
Journal of Translational Medicine (2024)
-
Associations between different triglyceride glucose index-related obesity indices and periodontitis: results from NHANES 2009–2014
Lipids in Health and Disease (2024)
-
Effectiveness of chlorhexidine gels and chips in Periodontitis Patients after Scaling and Root Planing: a systematic review and Meta-analysis
BMC Oral Health (2023)
-
Anti-resorptive therapy in the osteometabolic patient affected by periodontitis. A joint position paper of the Italian Society of Orthopaedics and Traumatology (SIOT) and the Italian Society of Periodontology and Implantology (SIdP)
Journal of Orthopaedics and Traumatology (2023)
-
Measures of oral health-related quality of life in patients with bone graft and implant prosthetic rehabilitation at the anterior of mandible/maxilla among young and middle-aged adults: a retrospective pilot study
International Journal of Implant Dentistry (2023)