
Abstract
Data sources
Medline/PubMed, SCOPUS and Google Scholar.
Data extraction and synthesis
Studies were split according to the type of teeth and the overjet threshold used, thus obtaining three subsets; primary teeth – overjet threshold 3-4 mm; permanent teeth – overjet threshold 3-4 mm and permanent teeth – overjet threshold 6 ± 1 mm. Pooled odds ratios for TDI were estimated for each dataset.
Results
Fifty-four studies were included involving patients from five continents. The adjusted pooled odds ratios were 2.31 (95%CI; 1.01–5.27) for primary teeth with 3-4 mm overjet; 2.01 (95%CI; 1.39–2.91) for permanent teeth with 3-4 mm overjet and 2.24 (95%CI; 1.56–3.21) for permanent teeth with 6 ± 1 mm overjet.
Conclusions
The present meta-analysis of observational studies showed that large overjet may double or even triple the risk for TDI to anterior primary and permanent teeth and that, at global level, large overjet is partly responsible for 100-300 million TDIs
Similar content being viewed by others

Commentary
This meta-analysis was performed with two main aims in mind. The first aim was to associate 'large' overjet to traumatic dental injuries (TDI), while the second one was to provide risk estimates that could be generalisable at a global level.
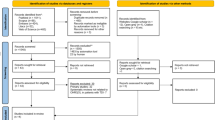
The authors performed a thorough search in three databases that resulted in including 54 studies with more than 10,000 patients from five continents; Europe, Asia, Africa and the Americas. The patient pool included adults, adolescents and children. For the sake of generalisability (external validity), the authors didn't assess the risk of bias in included studies to avoid exclusion of studies based on their quality. This would definitely jeopardise the validity of final pooled estimate and explains the wide confidence interval attained.
Many questions would arise after reading this meta-analysis; what is the limit of generalisability? Is it appropriate to pool results from different continents with different culture, life style and disease burden in one estimate? And what information would be more beneficial to stakeholders and clinical decision makers; the own population risk or the global one? The answer to these questions might justify or nullify undertaking such meta-analyses in the future.
Regarding the first aim of this meta-analysis, the authors didn't provide an exact definition of the ambiguous word 'large' overjet, rather, they sub-grouped the results in permanent teeth into (3-4 mm) and (6 ± 1 mm) overjet groups with incisor trauma prevalence of (27.5%) and (9%) respectively. Here comes the dilemma of using the word 'large' when describing a (3-4 mm) overjet. In their study of normal occlusion in the Finnish population,1 found that the mean overjet of 10-year-old children to be 3.45 ± 0.8 mm. Hence, 3-4 mm overjet is considered 'normal' rather than 'large' in some populations. Thus, the inclusion of these millions of injuries attributable to 'large' overjet in this meta-analysis would be over-exaggerated.
The final question would be: what is the clinical implication of such a meta-analysis? Would early orthodontic treatment prevent TDI associated with large overjet? A recent Cochrane systematic review2 tackled this question concluding that the only benefit of providing early treatment of class II malocclusion is reducing the incidence of incisor trauma when compared to one course treatment in adolescents. With over 200 million injuries to anterior teeth attributable to large overjet, the defenders of two-phase (early) treatment protocol for class II malocclusion would have a good – but not quite valid – premise when facing the single-phase (late) treatment protocol supporters.
References
Heikinheimo K, Nyström M, Heikinheimo T, Pirttiniemi P, Pirinen S . Dental arch width, overbite, and overjet in a Finnish population with normal occlusion between the ages of 7 and 32 years. Eur J Orthod 2012; 34: 418–426.
Thiruvenkatachari B, Harrison JE, Worthington HV, O'Brien KD . Orthodontic treatment for prominent upper front teeth (Class II malocclusion) in children. Cochrane Database Syst Rev 2013; 11: CD003452.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Prof. Stefano Petti, DMD, Department of Public Health and Infectious Diseases, Sapienza University, Piazzale Aldo Moro 5, Rome I-00185, Italy. E-mail: stefano.petti@uniroma1.it
Petti S. Over two hundred million injuries to anterior teeth attributable to large overjet: a meta-analysis. Dent Traumatol 2015; 31: 1–8.
Rights and permissions
About this article

Cite this article
Elkhadem, A. Large overjet may double the risk of dental trauma. Evid Based Dent 16, 56 (2015). https://doi.org/10.1038/sj.ebd.6401099
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401099
- Springer Nature Limited