
Abstract
Crystalline silica has emerged as a prominent occupational toxicant over extended periods, leading to the development of lung disease and cancer. The objective of this investigation is to establish a benchmark dose (BMD) for crystalline silica micro and nanoparticles based on the dehydrogenase activity of the A549 lung-cell line. The impact of exposure to crystalline silica micro-particles (C–SiO2 MPs) and crystalline silica nanoparticles (C–SiO2 NPs) on A549 epithelial lung cells was examined for durations of 24 and 72 h to evaluate cell viability using the MTT (3-(4, 5-dimethylthiazolyl-2)-2, 5-diphenyltetrazolium bromide) assay. The determination of dose-response and BMD was carried out through the BMD software v 3.2. The findings reveal a dose-dependent relationship between cell viability and both C–SiO2 MPs and -NPs. The BMDL values for 24 h treatment of C–SiO2 MPs and -NPs were determined to be 2.26 and 0.97 µg/ml, respectively, based on exponential models. Correspondingly, these values were found to be 1.17 and 0.85 µg/ml for the 72 h treatment. This investigation underscores the significance of particle size as a contributing factor in assessing occupational health risks. Moreover, the utilization of BMDL can facilitate the determination of more precise values for occupational exposures by considering various parameters associated with particle presence.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Occupational exposure to crystalline silica can lead to adverse health effects, including lung inflammation, silicosis, autoimmune disorders (AIDs), renal diseases, and lung cancer1. Although coating technologies have been developed to inhibit the toxic effects of silica, both through wet and dry methods, which show promising results2. Exposure to respirable crystalline silica (RCS) persists in traditional sectors such as construction and stone processing3. Workers in industries such as construction, mining, sandblasting, masonry, and machinery are particularly at risk4. The U.S. Occupational Safety and Health Administration (OSHA) has implemented a new standard for workplace crystalline silica, which sets levels at 50 µg/m3 for an 8-h workday, half of the previous standard5. Inspectors have found that the permissible exposure limit for silica is exceeded in 48% of industries where respirable quartz was measured6. It is estimated that over two million workers in the European Union are exposed to crystalline silica, with over 50 thousand workers in Poland exceeding the occupational exposure limit7. Silica exposure in Iran is a significant occupational health concern. Several studies have investigated silica dust levels in various industries and found that workers are exposed to high levels of crystalline silica dust, exceeding national and international standards. The mean exposure levels in different industries ranged from 0.008 to 2.81 mg/m3. The mortality rate due to silicosis was found to be between 1 and 52 per 1000 exposed individuals. Additionally, the risk of mortality due to lung cancer ranged from 4 to 129 per 1000 exposed individuals8,9,10.
Benchmark dose (BMD) modeling is a method used in chemical toxicology to determine the point of departure from a dose-response curve associated with a health-related outcome11. It involves fitting mathematical models to dose-response data and identifying the BMD, or its lower bound. This approach has been extensively used in chemical hazard assessments and is considered statistically preferable to identifying no observed adverse effects levels (NOAEL). BMD modeling has also been explored in the analysis of transcriptional data for the development of quantitative adverse outcome pathways12. It has been shown that BMDs derived from molecular endpoints can correlate with apical endpoints of interest for regulatory decisions11. It is widely used in risk assessment to establish health standards and guidelines for exposure to toxins. In the case of crystalline silica, one study measured ambient silica levels and reported average and upper-bound quartz levels of 3 and 8 μg/m3, respectively12. Overall, the BMD approach provides a useful tool for estimating dose-response relationships and determining safe exposure levels for various substances, including crystalline silica.
The assessment of exposure limits was concentrated on the evaluation of the allowable daily exposure13. The estimation of occupational exposure limits (OEL) in global organizations, such as the American Conference of Governmental Industrial Hygienists (ACGIH), is primarily based on individual exposure to specific chemicals. Owing to the constraints associated with the absence of observable detrimental effects at any dose level (NOAEL), the utilization of the lower confidence interval of the benchmark dose (BMDL) as an OEL level has gained traction in recent years due to its superior advantages over NOAEL14.
This study proposed an OEL through the utilization of a benchmark dose approach for crystalline silica micro-particles (C–SiO2 MPs) and crystalline silica nanoparticles (C–SiO2 NPs). The exposure was controlled by laboratory treatment on the A549 human lung epithelial cell line. Cell death is employed as the toxicity mechanism caused by silica in the benchmark dose estimation.
Results
Chemical and biological analysis
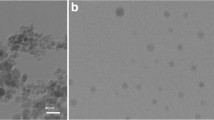
The analysis revealed that after acid treatment the presence of metallic impurities was found to be below 1%, while the ultimate level of purity of the crystalline silica was estimated to be approximately 98%. Table 1 provides a representation of the concentration of metals within the silica powder, while Fig. 1a illustrates the purity of the crystalline silica during XRD analysis. In contrast, Fig. 1b and c display the transmission electron microscopy (TEM) images of nanoparticles and the Phase-contrast microscopy (PCM) analysis of micro-sized particles, respectively. The results of the Dynamic light scattering (DLS) analysis are presented in Table 2. In the DLS analysis, it was observed that 90% of the nanoparticles were smaller than 5883 nm in size, whereas 90% of the micro-sized particles were smaller than 503 nm. Additionally, the analysis revealed the zeta potential values of − 38 ± 10 mV and − 34 ± 9 mV for micro and nanoparticles, respectively. The negative zeta potential values indicated that the agglomeration of nanoparticles was not stable in the culture medium.

(a) XRD analysis of treated silica powder. (b) PCM analysis for micro size particles34. (c) TEM analysis of nano-particles.
The MTT assay revealed that cell death exhibited a dose-dependent response following treatment for both 24 and 72 h. Furthermore, a noteworthy increase in cell death was observed in every concentration of C–SiO2 NPs when compared to the control (P < 0.05). Conversely, when the concentration of C–SiO2 MPs was at 10 µg/mL, no statistically significant difference was found in comparison to the control group. Figure 2 depicts the cell viability of A549 cells following treatment with C–SiO2 NPs and C–SiO2 MPs for 24 and 72 h. The findings also unveiled that C–SiO2 NPs caused a higher mortality rate within studied cells.

Cell viability of A549 cells after crystalline silica treatment for C–SiO2 MPs and C–SiO2 NPs after 24 and 72 h (star (*) represent significant values in compare to the controls).
Benchmark dose (BMD) estimation
After calculating the sediment dose of particles in a given portion, we proceeded to estimate the equivalent dose for the human lung using Eq. 2. The uncertainty factor was determined to be 500, which was derived from the multiplication of the factors for occupational setups15. Subsequently, we determined the concentration of 0.093 and 0.082 mg/m3 for 24 and 72-h exposures to C–SiO2 NPs, respectively. Conversely, for C–SiO2 MPs, the software indicated concentrations of 0.50 and 0.26 mg/m3 for 24 and 72-h exposures, respectively. The best BMD was reported based on AIC and P > 0.116 (Table 3 & 4). In every tested model the relationship of dose-response was proved. Figure 3 depicts the best dose-response model for various conditions.

The selected dose-response models for various particle and time silica treatments. (a) Exponential degree 4 for C–SiO2 MPs A549 treatment for 24 h. (b) Exponential degree 5 for C–SiO2 MPs A549 treatment for 72 h. (c) Exponential degree 4 for C–SiO2 NPs A549 treatment for 24 h. (d) Exponential degree 4 for C–SiO2 NPs A549 treatment for 72 h.
Discussion
In the present study, we aimed to determine the BMD of crystalline silica based on A549 response to cell death for C–SiO2 MPs and C–SiO2 NPs. According to our results, the BMDL for C–SiO2 NPs for the duration of 24 and 72 h treatment was determined 0.97 and 0.85 µg/mL respectively. Furthermore, these values were 2.26 and 1.17 µg/mL for C–SiO2 MPs after 24 and 72 h treatment. In other studies, significant (compared to untreated cells) cytotoxic effects were observed only at or above the concentration of 25 μg/ml17,18.
In our research, the viability of the A549 human lung cell line was reduced as a result of exposure to nano-particles and micro-particles. Furthermore, it has been determined that the severity of toxic effects was influenced by two factors, exposure time and concentration19. This observation is consistent with the outcomes of McCarthy et al.’s research, which demonstrated that cell survival is diminished in a concentration-dependent manner when exposed to silica nanoparticles20. Additionally, Duan et al.’s study reported that toxicity resulting from exposure to silica nanoparticles is dependent on both time and concentration21. Moreover, other studies conducted on the A549 cell line, which was exposed to silica nanoparticles, have also shown that the survival rate is greatly impacted by two variables, concentration and time22,23.
On the contrary, particle size plays a significant role in the biological environment. Earlier research has demonstrated that altering the size can impact the toxicity of the particles24,25. This study, along with its findings, has substantiated that nano and micro-particles exhibit distinct cellular toxicity. Moreover, the presence of nanoparticles in the mixture of airborne dust also has a substantial impact on health outcomes and can potentially lead to acute and chronic health issues, particularly in occupational settings and within shorter timeframes.
Most agencies set 0.05 mg/m3 for an 8-h workday as the exposure limit based on silicosis for crystalline Silica dust26. ACGIH was recommended the TLV-TWA (8 h) to be 0.025 mg/m327. Yet there is no consensus on the cut-off point that should be used to set a C–SiO2 exposure limit in the work environment26. The epidemiologic studies indicate that the NOAEL varied from 7 to 100 µg/m3 and the LOAEL ranged from 8 to 252 µg/m3 for silicosis28.
In our study, the predicted exposed dose for C–SiO2 NPs was determined by comparing their impact on the viability of human lung cells during 24 and 72 h of exposure. The PED values obtained were 0.093 and 0.03 mg/m3, respectively. In contrast, the cut-off points for C–SiO2 MPs, during 24 and 72 h of exposure, was found to be 0.50 and 0.087 mg/m3, respectively. These values were 5.4 and 3 times higher than those estimated for C–SiO2 NPs in this study.
Collins et al. derive a chronic reference exposure level (REL) of 3 µg/m3 for silicosis in environmental exposure using both benchmark concentration (BMC) and LOAEL/NOAEL approaches29. The reported concentration is much lower than in our study.
Study limitation
The primary limitation in our current investigation revolved around the utilization of a single viability assessment method (MTT) BMD estimation. Additional restrictions encompassed the utilization of a singular cell line (A549), using transformed cells, and submerge model for occupational exposure risk assessment.
Material and methods
Particle preparation
The Merck Company provided crystalline silica particles, measuring between 0.2 and 0.8 mm in size. These particles were then subjected to milling using a ball mill powered at 380 V and 0.75 kW. The milling process continued until the particles reached the intended size. PMC verified the micro-particles to be within the range of 1–10 µm. Then the grinding process continued on a part of the obtained microparticles until nanometer size were reached and TEM confirmed the presence of nanoparticles measuring below 40 nm.
Particle purification
For purification, the particles underwent three rounds of washing with hydrochloric acid (1 M). Each tube was subjected to stirring for a duration of 15 min and subsequently left undisturbed for a sedimentation period of 10 min. Following this, all the tubes were subjected to centrifugation at a speed of 5000 rpm for an interval of 20 min. Subsequently, the particles were subjected to treatment with concentrated nitric acid at a temperature of 60 °C for a duration of 20 min, three times. Finally, the particles were neutralized using deionized water and dried at a temperature of 40 °C for a period of 2 h. The particles were subjected to ICP-OES analysis to determine any metal impurities present, while XRD was employed to assess the silica component within the particle contents. Furthermore, transmission electron microscopy (TEM) and dynamic light scattering (DLS) were performed for nano-particles physical characterization. For micro size particles, phase contrast microscopy (PCM) analysis were performed.
ICP-OES analysis
In this study, 400 mg of silicon dioxide samples, processed both before and after purification, were analyzed using an ICP-OES tool. The types of metals present in the silicon dioxide samples and their concentrations were determined. Subsequently, the degree of impurity in the samples was calculated (Arcos EOP, Spectro Co., Germany).
XRD analysis
According to the NIOSH 7500, particles were treated with hot phosphoric acid to eliminate interfering compounds. For X-ray diffraction qualitative analysis, wet sieve with a 10 µm sieve, 2-propanol, and an ultrasonic bath were used. To this end, particles were washed by 2-propanol followed by evaporating excess alcohol, drying in an oven for 2 h, and overnight storage in a desiccator.
TEM analysis
To this end, nano-particles were suspended in isopropanol solution followed by dispersing in ultrasonic tank (Olympus KS-2, UK). Then 100 µL of suspension loaded on TEM frame (copper grid with carbon frame). The frame dried at room temperature (RT).
PCM analysis
For PCM analysis, 1 µg of particles was suspended in 10 mL of deionized water. From this suspension, 100 µL was loaded onto a mixed cellulose ester (MCE) membrane filter, which was subsequently cleared using acetone vapor. The size of 1000 particles across various fields on the S1 eye graticule filter was then examined using phase-contrast microscopy (Dialux 22 EB, Germany). The average particle size was reported as the size of the SiO2 microparticles.
DLS analysis
100 µg/mL of nano and micro-particles suspension prepared in culture medium kept 1 h at 25 °C for 1 h, then for 20 min at 240 V (60 Hz) was sonicated. Size distribution of suspensions were measured by DLS (Nanophox 90-246V, Germany). Particles (50 µg/mL) charge also was determined by zetasizer (Malvern, UK).
Cell culture and exposure
The cell line A549, derived from human lung epithelial cells, was procured from the Iranian Biological Resource Center (IBRC). These cells were cultivated in a T-25 culture flask using the Dulbecco’s modified eagle medium (DMEM) culture medium (Gibco, USA), supplemented with 10% fetal bovine serum (FBS) (Gibco, USA) and 1% Pen-Strep (Sigma, USA). To provide optimal conditions for cell growth, the culture was maintained at a temperature of 37 ºC, with a 5% CO2 concentration in a humidified atmosphere.
Before the commencement of the experiment, 100 µL of culture medium containing 10,000 cells were seeded into each wells (96-well plate), allowing for a period of 24 h for cell attachment. The silica concentrations for C–SiO2 MPs and C–SiO2 NPs (10, 50, 100, and 250 µg/mL) were then prepared in the cell culture medium without FBS and suspended through the process of ultra-sonication, after which they were gently added to each well. It is important to highlight that the experiments were conducted in triplicate, with appropriate control groups being included. The duration of particle exposure for all experiments was either 24 or 72 h.
Cell viability estimation
To conduct the thiazolyl blue tetrazolium bromide assay (MTT), a total of 10,000 cells were introduced into the 96-well plate a day before the commencement of the experiment. The cells were subsequently subjected to varying concentrations (0, 10, 50, 100, and 250 µg/mL) of both C–SiO2 MPs and C–SiO2 NPs. Following a treatment duration of either 24 or 72 h, the wells were thoroughly rinsed with phosphate-buffered saline (PBS) on two separate occasions. Next, 100 mL of MTT solution, prepared at a concentration of 5 µg/mL using Sigma (USA) as the source, was added to each well and allowed to incubate for a duration of 4 h at 37 ºC. Once the MTT solution was removed to facilitate the dissolution of formazan crystals, 100 µL of Dimethyl sulfoxide (Merck, Germany) was gently introduced into each well and mixed in the absence of light for a period of 20 min at room temperature. Subsequently, the supernatant was removed, and the cell surface was washed twice with PBS to remove any remaining particles. The cells were then exposed to the ROS reagent, and the wells were analyzed from the bottom of each plate using a plate reader (BioTek Instruments, USA) at a wavelength of 580 nm.
BMD estimation
The BMD evaluation employed the EPA benchmark dose software, version 3.2. The viability of the cells served as the response parameter. However, a continuous response method was implemented to estimation the BMD and BMDL. Various mathematical models, including exponential 2, exponential 4, hill, polynomial degree 4, polynomial degree 3, polynomial degree 2, power, and linear, were utilized for the dose-response evaluation. The BMD level was calculated by selecting the benchmark response (BMR) one standard deviation from the control. The appropriate model was chosen based on the criteria of goodness of P-value > 0.1, low χ2-scaled residual values (within ± 2 units), smallest Akaike Information Criterion (AIC), and visual inspection. Finally, among the appropriate fitted models, model with the lowest BMDL was selected.
BMD extrapolation from A549 to human subjects
The application of the multiple path particle deposition (MPPD) mathematical model, initially introduced by the Hammer Institute of Health Science in 1995, was justified to transfer data from in vitro experiments to human subjects. Within this mathematical framework, an estimation of the deposition and clearance rate of particles in the lungs is calculated. Consequently, the dose of particles can be determined utilizing Eq. 1.
where DAin vitro represents the mass dose per unit area measured in μg/cm2, C denotes the concentration of the treated solution in terms of BMDL levels measured in μg/mL, V stands for the volume of the treated solution (0.1 ml), and Awell represents the surface area of the in vitro well equal to 0.32 cm2. Finally, the concentration of aerosols deposited in the lung was predicted in terms of μg/m3 using the method described in Eq. 2.
The concentration of Deq is the amount deposited in the human lung (μg/m3). AP, the area of the human pulmonary, is equal to 1,020,000 cm2. Minute ventilation (MV) is 20,000 mL/min13. The exposure duration, denoted by T (min), is the length of time of the exposure (24 or 72 h). The deposition efficiency, denoted by DE, was 0.1 and 0.23 for C–SiO2 MPs and C–SiO2 NPs, determined using the MPPD software version 2.1130.
The concentration of particles deposited in the lungs was converted to airborne concentration with the utilization of appropriate uncertainty factors [Eq. (3)]. The PED human, which represents the Predicted Exposed Dose (PED) in humans, is measured in μg/m3.
The aforementioned factors F1, F2, and F3 play a significant role in this regard.
F1 (intra-species variation): based on the assumption that the variability in the general population, including children, the elderly, and diseased individuals, is higher than in workers, A default value of 5 for workers was applied31,32.
F2 (LOAEL to NOAEL extrapolation): the BMDL10 is considered a LOAEL since the biological effect was a 10% increase in cancer incidence. A maximum factor of 10 is used when deriving an OEL from a LOAEL, instead of a NOAEL31.
F3 represents the short-term exposure; this factor is assigned a value of 1033.
Statistical analysis
In this research, SPSS version 21 statistical software was used to analyze the results obtained from tests. In order to evaluate the effect of time and dimensions on the toxicity level and also to compare the toxicity of the studied compounds, the independent sample T-test statistical test was used and to evaluate the difference between the sample groups and the control group, the one-way ANOVA followed by Tukey’s Post Hoc statistical test was used followed by Tukey’s Post Hoc test. A statistical significance level of 0.05 was considered in all tests.
Data availability
The datasets generated during and/or analyzed during the current study are not publicly available due to reasons of sensitivity of funding organization but are available from the corresponding author via this email: panjali.z68@gmail.com on reasonable request.
References
Liu, J. Y. & Sayes, C. M. A toxicological profile of silica nanoparticles. Toxicol. Res. 11(4), 565–582 (2022).
Pavan, C. et al. The puzzling issue of silica toxicity: Are silanols bridging the gaps between surface states and pathogenicity?. Part. Fibre Toxicol. 16(1), 1–10 (2019).
Salamon, F. et al. Occupational exposure to crystalline silica in artificial stone processing. J. Occup. Environ. Hyg. 18(12), 547–554 (2021).
Cooper, J. Global occupational hazard: Silica dust. In ASME International Mechanical Engineering Congress and Exposition (American Society of Mechanical Engineers, 2012).
OSHA Occupational safety and health standards; toxic and hazardous substances. In Respirable Crystalline Silica (OSHA, 2019).
Freeman, C. S. & Grossman, E. A. Silica exposures in workplaces in the United States between 1980 and 1992. Scand. J. Work Environ. Health 21(2), 47-49 (1995).
Maciejewska, A. Occupational exposure assessment to crystalline silica dust: Approach in Poland and worldwide. Int. J. Occup. Med. Environ. Health 21(1), 1–23 (2008).
Golbabaei, F., Gholami, A., Teimori-Boghsani, G., Yaseri, M. & Kianmehr, M. Evaluation of occupational exposure to silica dust in mining workers in eastern Iran. Open Environ. Res. J. 12(1), 1–6 (2019).
Omidianidost, A., Ghasemkhani, M., Kakooei, H., Shahtaheri, S. J. & Ghanbari, M. Risk assessment of occupational exposure to crystalline silica in small foundries in Pakdasht, Iran. Iran. J. Public Health 45(1), 70–75 (2016).
Mohammadyan, M., Rokni, M. & Yosefinejad, R. Occupational exposure to respirable crystalline silica in the Iranian Mazandaran province industry workers. Arch. Ind. Hyg. Toxicol. 64(1), 139–142 (2013).
Chauhan, V. et al. Considerations for application of benchmark dose modeling in radiation research: Workshop highlights. Int. J. Radiat. Biol. 99, 1320–1331 (2023).
Budtz-Jorgensen, E. & Grandjean, P. Developments in benchmark modeling of epidemiological data. ISEE Conf. Abstr. https://doi.org/10.1289/isee.2022.O-SY-111 (2022).
Kuempel, E. D., Sweeney, L. M., Morris, J. B. & Jarabek, A. M. Advances in inhalation dosimetry models and methods for occupational risk assessment and exposure limit derivation. J. Occup. Environ. Hyg. 12(1), S18–S40 (2015).
Vahabi Shekarloo, M. et al. Application of a novel exposure limit approach for co-exposure of chemicals: A field study by in-vitro design. Int. J. Environ. Health Res. 33(12), 1269–1277 (2023).
Lipscomb, J. C. & Ohanian, E. V. Toxicokinetics and Risk Assessment (Informa Healthcare, 2007).
USEPA. Benchmark dose technical guidance. Risk Assessment Forum. Accessed 2024. https://www.epa.gov/risk/benchmark-dose-technicalguidance (US Environmental Protection Agency, Office of the Science Advisor, USA, 2012).
Ahamed, M. Silica nanoparticles-induced cytotoxicity, oxidative stress and apoptosis in cultured A431 and A549 cells. Hum. Exp. Toxicol. 32(2), 186–195 (2013).
Murugadoss, S. et al. Toxicology of silica nanoparticles: An update. Arch. Toxicol. 91(9), 2967–3010 (2017).
Rafieepour, A., Azari, R. M. & Khodagholi, F. Cytotoxic effects of crystalline silica in form of micro and nanoparticles on the human lung cell line A549. Toxicol. Ind. Health 39(1), 23–35 (2023).
McCarthy, J., Inkielewicz-Stepniak, I., Corbalan, J. J. & Radomski, M. W. Mechanisms of toxicity of amorphous silica nanoparticles on human lung submucosal cells in vitro: Protective effects of fisetin. Chem. Res. Toxicol. 25(10), 2227–2235 (2012).
Duan, J. et al. Toxic effect of silica nanoparticles on endothelial cells through DNA damage response via Chk1-dependent G2/M checkpoint. PLoS One 8(4), e62087 (2013).
Park, E.-J. & Park, K. Oxidative stress and pro-inflammatory responses induced by silica nanoparticles in vivo and in vitro. Toxicol. Lett. 184(1), 18–25 (2009).
Lin, W., Huang, Y.-W., Zhou, X.-D. & Ma, Y. In vitro toxicity of silica nanoparticles in human lung cancer cells. Toxicol. Appl. Pharmacol. 217(3), 252–259 (2006).
Kim, I.-Y., Joachim, E., Choi, H. & Kim, K. Toxicity of silica nanoparticles depends on size, dose, and cell type. Nanomed. Nanotechnol. Biol. Med. 11(6), 1407–1416 (2015).
Jaganathan, H. & Godin, B. Biocompatibility assessment of Si-based nano-and micro-particles. Adv. Drug Deliv. Rev. 64(15), 1800–1819 (2012).
Rey-Brandariz, J. et al. Occupational exposure to respirable crystalline silica and lung cancer: A systematic review of cut-off points. Environ. Health 22(1), 82–95 (2023).
ACGIH. Threshold limit values for chemical substances and physical agents and biological exposure indices: American Conference of Governmental Industrial Hygienists. Accessed 20 Mar 2024. http://www.acgih.org/tlv-bei-guidelines/ (2023).
Rice, F. L. & Stayner, L. T. Assessment of silicosis risk for occupational exposure to crystalline silica. Scand. J. Work Environ. Health 21(2), 87-90 (1995).
Collins, J. F., Salmon, A. G., Brown, J. P., Marty, M. A. & Alexeeff, G. V. Development of a chronic inhalation reference level for respirable crystalline silica. Regul. Toxicol. Pharmacol. 43(3), 292–300 (2005).
ARA. Multiple-path particle deposition (MPPD 2.1 version): A model for human and rat airway particle dosimetry, by Applied Research Associates, Inc., Raleigh, NC. Accessed 2024. https://www.ara.com/mppd/ (Applied Research Associates, Inc, Albuquerque, New Mexico, 2024).
Blum, K., FitzGerald, R., Wilks, M. F., Barle, E. L. & Hopf, N. B. Use of the benchmark-dose (BMD) approach to derive occupational exposure limits (OELs) for genotoxic carcinogens: N-nitrosamines. J. Appl. Toxicol. 43, 1183–1200 (2023).
ECHA. Guidance R.8. Guidance on information requirements and chemical safety assessment - chapter R.8: Characterisation of dose [concentration]-response for human health. Accessed 2024. https://echa.europa.eu/guidance-documents/guidance-on-information-requirements-and-chemical-safety-assessment (Finland European Chemicals Agency (ECHA), 2012).
Gollapudi, B. B. et al. Genotoxicity as a toxicologically relevant endpoint to inform risk assessment: A case study with ethylene oxide. Environ. Mol. Mutagen. 61(9), 852–871 (2020).
Rafieepour, A. et al. The effect of particle size on the cytotoxicity of amorphous silicon dioxide: An in vitro toxicological study. Asian Pac. J. Cancer Prev. 22(2), 325–332 (2021).
Acknowledgements
The authors of this study are grateful to the Iran University of Medical Sciences for providing laboratory facilities and financial support for the present study [grant number: 1402-1-9925888].
Funding
This study was supported by Air Pollution Research Center, 1402-1-9925888.
Author information
Authors and Affiliations
Contributions
Athena Rafieepour and Zahra Panjali conceived of the presented idea. Masoomeh Vahabi Shekarloo developed the theory and performed the computations. Athena Rafieepour and Masoomeh Vahabi Shekarloo carried out the experiment. Zahra Panjali wrote the manuscript with support from Azadeh Ashtarinezhad. Azadeh Ashtarinezhad and Iraj Alimohammadi contributed to the interpretation of the results. All authors discussed the results and contributed to the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Rafieepour, A., Shekarloo, M.V., Ashtarinezhad, A. et al. Benchmark dose determining airborne crystalline silica particles based on A549 lung-cell line survival in an in vitro study. Sci Rep 14, 21458 (2024). https://doi.org/10.1038/s41598-024-72607-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-72607-5
- Springer Nature Limited