
Abstract
Intussusception is a common surgical emergency in children. Clinical suspicion and radiological evaluation confirm the diagnosis of the disease. Enema reduction is the first line of management. This study aimed to explore the risk factors associated with enema reduction failure. A retrospective analysis of patients diagnosed with intussusception at three different hospitals in different countries from January 2016 to December 2022. Data collected included demographics, presenting symptoms, duration of symptoms, management, outcomes, and follow-ups. A total of 290 cases of intussusception were included in the study. Ages ranged from 1 to 36 months, with a median age of 15 months. All children underwent an enema reduction which was successful in 92.4%. Failure of reduction was seen in 16.7% of females compared to 6.4% of males, and it was significantly seen in children below the age of 1 year compared to older children. Failure of reduction significantly increases with the duration of symptoms and in children who present with bilious vomiting and currant jelly stool. In conclusion, Failure of enema reduction was more prevalent in females, in children below the age of 1 year and who present late, as well as children who had bilious vomiting and currant jelly stool. This study identified several risk factors associated with failed enema reduction in children with intussusception. Recognizing the risk factors can help guide clinicians in the management and anticipation of outcomes.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Intussusception is a common surgical emergency in children, with an incidence rate of approximately one to four cases per 2000 newborns and children1. It is a significant cause of intestinal obstruction and a leading cause of abdominal emergency in the pediatric population1,2,3,4,5. Intussusception can occur at any age, but it is more commonly observed during the first two years of life. The male-to-female ratio ranges from 3:2 to 2:1, indicating a higher incidence in males1,2,3. Colicky intermittent abdominal pain, vomiting, a palpable abdominal mass, and currant jelly stool are the classic clinical presentations1,2. These symptoms are present in approximately 50% of cases. However, 20% of patients are symptom-free at initial clinical presentation1. Early recognition and prompt treatment are crucial, as delayed diagnosis and management can lead to significant morbidity and mortality3,6. Plain abdominal radiographs may show characteristic findings such as a soft tissue mass, target sign, meniscus sign, absence of air in the ascending colon, and/or small bowel dilatation1,2. The diagnosis is usually confirmed by findings of the target or donut sign in the abdomen ultrasonography1,2.
Delayed presentation of intussusception reduces the success rate of reduction procedures. Thus, prompt diagnosis and timely initiation of treatment are crucial for favorable outcomes2,3. Delayed presentation, characterized by prolonged symptom duration before seeking medical help, can hinder the effectiveness of non-surgical reduction methods. Hydrostatic and pneumatic reduction were monitored fluoroscopically to accurately determine the success of the intervention3. Identifying the risk factors associated with failed reduction in cases of delayed presentation is crucial for enhancing management approaches and optimizing patient outcomes1,2,3. Successful non-operative reduction can prevent the need for surgical intervention and associated complications3,4. While previous studies have identified certain risk factors for failed enema reduction in intussusception, the findings have been inconsistent across different populations and settings1,2,3,4. There is an ongoing need to better understand the specific factors that contribute to reduction failure, as this can inform treatment protocols and improve outcomes for these pediatric patients. Some studies have reported higher rates of failure in younger infants or those with prolonged symptoms durations, but the strength and consistency of these associations remain unclear1,2,3,4,5,6,7. Further exploration of the risk profile for unsuccessful non-operative management is warranted to optimize the management of intussusception and reduce the need for surgical intervention. This study aims to explore the risk factors associated with failure of enema reduction as all patients included in the study were hospitalized for monitoring and interventions.
Methodology and materials
Study design and setting
This is a retrospective, multicenter study conducted at the Department of Surgery at King Saud University Medical City (KSMUC) in Riyadh, Saudi Arabia, Hamad Medical Corporation (HMC) in Doha, Qatar, and AlQasimi Women’s and Children’s Hospital, Sharjah, United Arab Emirates. The study was approved by the ethical committee of the respective institutions between the years 2016 and 2023. All methods were performed in accordance with the relevant guidelines and regulations.
Inclusion criteria
-
1.
Children less than 3 years of age.
-
2.
Idiopathic Ileo-colic intussusception.
-
3.
Confirmed diagnosis of intussusception based on clinical and radiological findings.
-
4.
No signs of sepsis or peritonitis.
Intussusception examination and reduction protocols
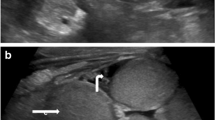
The Ultrasound examinations were performed using a high-resolution machine with a linear transducer probe (L12-5 MHz). Patients were scanned systematically in supine position, focusing on the right upper quadrant where intussusceptions typically present. Doppler imaging was utilized to assess bowel perfusion. Ultrasound findings documented included intussusception size, presence of a lead point, and signs of obstruction or ischemia. The duration of symptoms prior to ultrasound was also recorded4.
Pneumatic reduction done under continuous fluoroscopic guidance. A rectal catheter was inserted, and air was slowly insufflated into the rectum. The pressure was gradually increased until the intussusception was reduced, as visualized by the ileocecal valve returning to its normal position, or until a maximum pressure of 120 mmHg was reached. If the initial attempt was unsuccessful, a second attempt could be made after a brief rest period4,14. While the hydrostatic reduction, a Foley catheter was inserted into the rectum and connected to a saline-filled bag elevated 60–100 cm above the patient. Saline was slowly infused under fluoroscopic monitoring until the intussusception was reduced, visualized by the return of the ileocecal valve to its normal position. If the initial hydrostatic attempt was unsuccessful, a second attempt could be performed after a short rest period15.
In both reduction methods, fluoroscopic images were reviewed by the pediatric radiologist to confirm complete reduction. Based on the available resources, pneumatic reduction is the first choice if equipment available, otherwise hydrostatic reduction is performed.
Data collection and analysis
Data collection included information on patients with the final diagnosis of intussusception. Demographics, presenting symptoms, duration of symptoms, management, results, and follow-ups were all collected.
Statistical Package for Social Sciences version 21 (SPSS: An IBM Company) was used for data collection and analysis. All statistical methods were two-tailed with an alpha level of 0.05 and a P-value significance of less than or equal to 0.05. Descriptive analysis was done by prescribing frequency distribution and percentage for study variables, including case age and gender, clinical presentation, and clinical outcome. Intussusception cases were cross-tabulated to determine factors associated with failed reduction performed with a Pearson chi-square test for significance and an exact probability test for small frequency distributions.
Results
A total of 290 cases with intussusception were included. Ages ranged from 1 to 36 months with a median age of 15 months, 112 (36.6%) were less than 1 year, 98 (32%) were aged 1 to 2 years, and 80 (27.5%) were aged 2 to 3 years. A total of 190 (65.6%) cases were males. The duration of symptoms was less than 24 h in most cases 189 (65.1%), 24 to 48 h in 48 cases (16.5%), and more than 48 h in 41 cases (13.4%). The most common symptoms were bilious vomiting in 155 cases (53.4%), Currant jelly stool in 77 cases (25.2%), and fever in 20 cases (6.8%) [Table 1].
All cases underwent an enema reduction trial, mainly pneumo-reduction among in 177 cases (61%) and hydro-reduction in 95 cases (32.8%), and 18 (6.2%) of recruited patients needing both. Failure of enema reduction was reported among 22 (7.6%) of patients. All failed cases underwent surgical intervention and seven out of 22 cases who needed surgery for reduction required bowel resection with primary anastomosis or ileostomy due to bowel ischemia [Table 2].
Failure of reduction was seen in 16 (16.7%) of females compared to 6 (6.4%) of males (P = 0.003). Failure of reduction was significantly seen in children below the age of 1 year compared to children more than two years (P = 0.035). Failure of reduction significantly increased with the duration of symptoms; it was reported among 12 cases (29.3%) who presented with symptoms for more than 48 h compared to 3 cases (1.6%) of others with symptoms for less than 24 h (P = 0.001). Failure of reduction was significantly seen with children who had bilious vomiting (P = 0.048) and currant jelly stool (P = 0.012) but was not significant among those who had fever (P = 0.810) [Table 3].
Logistic regression was carried out for binary variables to determine the predictability of independent variables, namely, age, gender, duration of symptoms (less than 24 h, 24–48 h, and more than 48 h), bilious vomiting, jelly stool, and fever. Predictors with significant odds ratio (OR) are used to perform multiple logistic regressions to determine the predictability of a combination of independent variables. R language programming was used to perform logistic regression utilizing the glm function from the stats library (Dobson and Barnett, 201828; Ripley, 20024). Additionally, to provide visualizations of the data, the ggplot2() library was employed to create the necessary visual representations (Wickham and Wickham, 20165). [Tables 4, 5] illustrated the univariable and multivariable logistic regressions of predictors for surgical intervention versus enema reduction among children with intussusception [Fig. 1].

Frequency of the predictors against intervention, either surgery or reduction.
Discussion
Intussusception is a common surgical emergency in children that needs prompt intervention. Cases of intussusception are more commonly seen in males during the first two years of life. The main approach for uncomplicated cases is non-surgical reduction using either hydrostatic or pneumatic enemas. Surgical intervention is usually reserved for cases of peritonitis, perforation, and unsuccessful enema reduction3. Diagnosis is confirmed through abdominal ultrasonography, specifically the target or donut sign. Delayed presentation makes non-surgical reduction methods less effective1. Therefore, the identification of risk factors related to failed enema reduction is paramount in cases of delayed presentation to optimize management and outcome1,2,3,4. The current study was conducted to explore the potential risk of enema reduction failure, both pneumatic and hydrostatic.
The age and sex of infants is emphasized in the literature as risk factors for the occurrence of intussusception. Out of 125 patients who underwent attempted enema reduction, nearly 62% were males with an average age of 30 months5. Moreover, male infants (54%) more frequently present emergency intussusception, with a male-to-female ratio of 1.19:1 and a peak age of onset at 3–4 years6,7,8. According to a recent study, male patients made up the majority of the study population, accounting for 64% of participants. The male-to-female ratio was observed to be close to 2:1. Additionally, the data revealed that the incidence of intussusception, a medical condition, was notably higher among children aged between 6 months and 2 years, with this age group compromising nearly 60% of the total participants recruited for the study7. In the current study, male infants were predominant with a median age of 17 months.
Recent studies have shown a clear relationship between patient age and the success of enema reduction for intussusception, a common pediatric emergency. Infants under 1 year have a significantly lower likelihood of successful enema reduction, while children over 2 years are more prone to recurrence after successful treatment. Geographical variation exist, with earlier median ages observed in Africa (29 weeks) compared to Asia (35 weeks). The current study highlights the critical importance of considering patient age, as failure of enema reduction is strongly correlated with age extremes, while those between 1–2 years have high success rates, underscoring the need for tailored management strategies8,9,10,11. The regression analysis results show that with each additional month of age, the need for surgery decreases, but this effect is not linear and does not imply a 100% success rate for children older than two years. Therefore, it should be emphasized that the age of onset is an important determinant of enema reduction success and can be a predictor of intervention success.
In one study unsuccessful reduction was 71% in males compared to 28% in females. However, the difference was statistically insignificant9. Regarding the debate in the literature on the implications of sex in predicting surgical intervention success, our study showed that enema reduction was significantly higher in females compared to males. Moreover, 66% of female patients with intussusception had enema reduction success and were less likely to undergo surgery.
Short duration of symptoms presenting less than 12 and 24 h respectively is associated with a high probability of enema reduction success10. Further research concurred that infants presenting for 24 h or less after the onset of symptoms were more likely to pass enema reduction successfully11,12,13,14,15. The current study matches the results reported in the literature. There was a significantly greater failure rate of enema reduction among patients who presented later compared to those who presented earlier than 24 h. According to the regression analysis, the duration of symptoms (24–48 h, and > 48 h) cannot be considered as predictors for intervention. Consequently, early presentation of infants is considered an important factor for a successful enema reduction approach. Reduction failure is more likely in infants with intussusception accompanied by fever, rectal bleeding, and vomiting; It is also prevalent in infants with ascites, left-sided intussusception, and trapped fluid detected by ultrasound16,17,18,19. Patients with fever at presentation are less likely to experience a short-term recurrence, whereas those without fever are more likely to do6,20.
Bloody stool is significantly associated with unsuccessful enema reduction requiring surgical intervention, but abdominal pain, vomiting, and restlessness are not20,21. Consistent with the literature, this current study finds that failure of enema reduction is correlated to vomiting, bloody stool, and fever. Based on logistic regression analysis, bilious vomiting, and temperature were not predictive of success. Yet, a bloody stool was found to increase the likelihood of surgical intervention.
In this context, a systematic review of 15 articles concluded that enema reduction of ileocolic intussusception can be conducted as an outpatient approach22,23,24,25. Managing intussusception as an outpatient following successful enema reduction leads to shorter hospital stays without any notable difference in the rate of revisiting the emergency, recurrence, need for surgery, or increased mortality rate26,27,28,29. There were no significant differences in outcomes between patients who were admitted for intussusception management and those who were discharged30,31,32,33.
Strengths and limitations of the study
The main strength of the current study is that it is multidisciplinary, involving three tertiary hospitals in three countries: Saudi Arabia, Qatar, and the United Arab Emirates. A regression analysis was employed to detect the predictability of certain variables pertaining to intussusception. However, this study is limited by the small sample size and its retrospective observational approach. This means that only frequency and correlation can be inferred.
Conclusion
The current multicenter study on pediatric intussusception found that failure of enema reduction was more prevalent in females, children under 1 year of age, those with a longer duration of symptoms, and those presenting with bilious vomiting and currant jelly stool. These risk factors should be carefully considered when managing intussusception cases, as they can help guide clinicians towards more expedient surgical intervention in high-risk patients, while allowing for more conservative reduction attempts in low-risk cases. The findings from this large, multinational analysis provide valuable evidence to optimize treatment strategies and improve outcomes for children with this common surgical emergency. Further research is needed to explore additional factors and develop guidelines to reduce delayed presentation and enhance outcomes in intussusception cases.
Data availability
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request. The datasets generated and/or analyzed during the current study are not publicly available due to institutions’ policies and regulations but are available from the corresponding author on reasonable request.
References
Sorantin, E. & Lindbichler, Franz. Management of intussusception. Rofo 14, L146–L154. https://doi.org/10.1007/s00330-003-2033-2 (2004).
Khorana, J. et al. Enema reduction of intussusception: The success rate of hydrostatic and pneumatic reduction. Ther. Clin. Risk Manag. https://doi.org/10.2147/tcrm.s92169 (2015).
Beres, A. L. & Baird, R. An institutional analysis and systematic review with meta-analysis of pneumatic versus hydrostatic reduction for pediatric intussusception. Surgery 154, 328–334. https://doi.org/10.1016/j.surg.2013.04.036 (2013).
Ripley, B. D. Modern Applied Statistics with S (Springer, 2002).
Wickham, H. & Wickham, H. Data Analysis (Springer, 2016).
Sun, Z., Song, G., Lian, D., Zhang, Q. & Dong, L. Process management of intussusception in children: A retrospective analysis in China. Pediatr. Emerg. Care 38, 321 (2022).
Litz, C. N. et al. Outpatient management of intussusception: A systematic review and meta-analysis. J. Pediatr. Surg. 54, 1316–1323 (2019).
Hadidi, A. T. & El Shal, N. Childhood intussusception: A comparative study of nonsurgical management. J. Pediatr. Surg. 34, 304–307. https://doi.org/10.1016/s0022-346890196-3 (1999).
Delgado-Miguel, C. et al. Intussusception management in children: A 15 year experience in a referral center. Indian J. Pediatr. 19, 1–6 (2022).
Deshmukh, S. N., Sanghvi, Z. N. & Pawar, R. R. Intussusception in children: A prospective cohort study. Int. J. Anatomy Radiol. Surg. (2022).
Kim, P. H. et al. Predictors of failed enema reduction in children with intussusception: A systematic review and meta-analysis. Eur. Radiol. 31, 8081–8097 (2021).
Xie, X. et al. A randomized trial of pneumatic reduction versus hydrostatic reduction for intussusception in pediatric patients. J. Pediatr. Surg. 53, 1464–1468 (2018).
Carroll, A. G. et al. Comparative effectiveness of imaging modalities for the diagnosis and treatment of intussusception. AJR Am. J. Roentgenol. 24, 521–529. https://doi.org/10.1016/j.acra.2017.01.002 (2017).
Ng, A. W. Y. et al. Childhood intussusception: 17 year experience at a tertiary referral centre in Hong Kong. HKMJ 21, 518–524 (2015).
Sadigh, G., Zou, K. H., Razavi, S. A., Khan, R. & Applegate, K. E. Meta-analysis of air versus liquid enema for intussusception reduction in children. AJR Am. J. Roentgenol. 205, W542–W549. https://doi.org/10.2214/ajr.14.14060 (2015).
Chukwu, I. S., Ekenze, S. O., Ezomike, U. O., Emeka, C. K. & Ekpemo, S. C. Ultrasound-guided reduction of intussusception in infants in a developing world: Saline hydrostatic or pneumatic technique?. Eur. J. Pediatr. 182, 1049–1056. https://doi.org/10.1007/s00431-022-04765-5 (2022).
Fakhry, T., Fawzy, A. N. & Mahdy, A. T. The efficacy of delayed, repeated reduction enema in management of intussusception. Ann. Pediatr. Surg. 17, 1–5 (2021).
Ma, G. M., Lillehei, C. & Callahan, M. J. Air contrast enema reduction of single and recurrent ileocolic intussusceptions in children: Patterns, management and outcomes. Pediatr. Radiol. 50, 664–672 (2020).
Binu, V. et al. Ultrasound guided hydrostatic enema reduction of ileocolic intussusception: a safe and effective technique. ANZ J. Surg. 93, 1993–1998 (2023).
Radu, S., Lin, S., Le, L. D., Fialkowski, E. & Zigman, A. Delayed repeat contrast enema for treatment of pediatric intussusception. J. Surg. Res. 275, 109–114 (2022).
Yu, F. et al. A technique to reduce the early recurrence of intussusception in ultrasound-guided hydrostatic reduction. J. Ultrasound Med. 41, 2467–2473 (2022).
Ravitch, M. M. Diagnosis and treatment intussusception—a surgical condition. Pediatrics 38, 122–123 (1966).
Al-Tokhais, T. et al. Antibiotics administration before enema reduction of intussusception: Is it necessary?. J. Pediatr. Surg. 47, 928–930. https://doi.org/10.1016/j.jpedsurg.2012.01.050 (2012).
Attoun, M. A. et al. The management of intussusception: A systematic review. Cureus 15, e49481. https://doi.org/10.7759/cureus.49481 (2023).
Binu, V. et al. Ultrasound guided hydrostatic enema reduction of ileocolic intussusception: A safe and effective technique. ANZ J. Surg. 93, 1993–1998. https://doi.org/10.1111/ans.18502 (1993).
Chukwu, I. S., Ekenze, S. O., Ezomike, U. O., Chukwubuike, K. E. & Ekpemo, S. C. Ultrasound-guided reduction of intussusception in infants in a developing world: Saline hydrostatic or pneumatic technique?. Eur. J. Pediatr. 182, 1049–1056. https://doi.org/10.1007/s00431-022-04765-5 (2023).
Chukwubuike, K. E. & Nduagubam, O. C. Hydrostatic reduction of intussusception in children: A single centre experience. Pan. Afr. Med. J. 36, 263 (2020).
Dobson, A. J. & Barnett, A. G. An Introduction to Generalized Linear Models (Chapman and Hall/CRC, 2018).
Lindbichler, F. & Sorantin, E. Management of intussusception. Eur. Radiol. Suppl. 14, L146–L154. https://doi.org/10.1007/s00330-003-2033-2 (2004).
Liu, L. et al. Air enema reduction versus hydrostatic enema reduction for intussusceptions in children: A systematic review and meta-analysis. PLoS ONE 19, e0297985. https://doi.org/10.1371/journal.pone.0297985 (2024).
Öztaş, T. & Deveci, G. Is phosphate enema treatment effective in ileocolic intussusception?. HK J. Paediatr. (New Series). 28(1), 8–12 (2023).
Shen, G. et al. Risk factors for short-term recurrent intussusception and reduction failure after ultrasound-guided saline enema. Pediatr. Surg. Int. 34, 1225–1231. https://doi.org/10.1007/s00383-018-4340-3 (2018).
Taher, H. E. H., Abd El-Aziz, M., Mostafa, A. A. A. F. & Ali, Y. M. A. Comparative study between hydrostatic and pneumatic reduction for early intussusception in pediatrics. Al Azhar Int. Med. J. 3, 1–6. https://doi.org/10.21608/aimj.2022.113210.1756 (2022).
Author information
Authors and Affiliations
Contributions
All authors contributed equally in this study. Tuqa AlSinan and Tariq AlTokhais formulated the study idea and methods. Tuqa AlSinan, Tariq AlTokhais, Fatimah AlShayeb, Amro Hajja, Mohammad AlBoukai, Sulaiman Alsalameh, Renad AlDahleh, Shamah Shabi, and Shams Almubayadh wrote proposal and manuscript, data collection and analysis from Saudi Arabia. Dollis de jesus Rodriquez Ruano and Amani AlAnsari wrote manuscript and data collection and analysis from Qatar. Khalid AlAli wrote manuscript and data collection and analysis from United Arab Emirates. Tuqa AlSinan, Tariq AlTokhais, and Amani AlAnsari reviewed and edited the study.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical considerations
The RB Approval of Research Project No. E-23-7774 had waived the informed consent from this retrospective study.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Alsinan, T., Altokhais, T., Alshayeb, F. et al. Risk factors for failure of enema reduction of intussusception in children. Sci Rep 14, 20786 (2024). https://doi.org/10.1038/s41598-024-71289-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-71289-3
- Springer Nature Limited