
Abstract
Air Force pilots and some athletes (e.g., in sledding sports) are frequently exposed to high G-forces. High-intensity physical activity is essential to withstand gravitational acceleration, and morphological symmetry and functional movement are directly related to injury in those who perform these activities. However, the relationship between G-endurance and physical imbalance and the effect on physical performance is poorly understood. This study aimed to analyze the physical performance of those exposed to a high load of G-tolerance and who performed high-intensity physical activity. A total of 363 male cadets from the Korean Air Force Academy underwent functional movement screen tests, anatomical structure measurements, G-tests (fourth grade), and body composition and physical fitness tests. Participants were classified into the G-test-pass and -fail groups depending on the G-test results. The pass group showed significantly different bilateral imbalance in active straight leg raises (p < 0.05), while the fail group showed a significant difference in deep squats (p < 0.05), shoulder mobility (p < 0.01), rotary stability (p < 0.05), and functional leg length (p < 0.05). Leg length was significantly correlated with the hurdle step (p < 0.01), inline lunge (p < 0.01), and active straight leg raise (p < 0.01). Functional leg lengths on both sides and structural leg lengths were also significantly correlated (p < 0.01). High body balance positively affects gravitational acceleration and exercise performance. Therefore, functional movement and physical imbalance affect performance in pilots affected by gravitational acceleration. This study can also be applied to strengthen the performance of winter sports athletes affected by gravitational acceleration.
Similar content being viewed by others


Introduction
Exercise complexity, including balance and body structure, helps improve motor function and strengthens high acceleration resistance in pilots1,2. The structural features of the human body and movement patterns are closely related, and balance and symmetry significantly affect body movements and injuries3. Functional leg-length imbalance is inversely proportional to the quality of movement and directly proportional to chronic tension in the spinal cord, causing pain and, in severe cases, scoliosis4. Morphological symmetry and movement pattern analysis are particularly important to people who regularly perform high-strength physical activities at a professional level5.
Although various testing tools are utilized in the field to predict morphological symmetry, functional movement screen (FMS) and functional limb symmetry measurements are the most highly used tools in the field. FMS is a tool developed to accurately analyze asymmetric body parts6 and identify musculoskeletal damage risk. FMS uses a total of seven test methods, with the highest score being 21 points; however, it is classified as a test method with a high risk of injury7.
Recent studies using FMS have reported that the morphological symmetry of pilots’ lower extremities has a significant effect on whether they pass the G-test8. Pilots are frequently exposed to high loads, and continuous exposure to G-forces above 7 G can cause musculoskeletal injuries, such as those of the cervical and lumbar vertebrae9,10. Therefore, pilots are trained with the same high intensity as elite athletes and maintain their stamina to withstand this acceleration of gravity11. However, 36% of South Korean pilots still complain of back pain. Similarly, winter sports and some racing athletes are also likely to be exposed to the same damage as they can be affected by the acceleration of gravity.
Although gravity-based data is essential for athletes who compete in sledding events (such as bobsleigh and skeleton) and G-durable athletes (such as racing drivers), obtaining G-test data for elite athletes is challenging. Therefore, this study aimed to analyze the relationship between physical imbalance characteristics and the physical abilities of Air Force cadets in more detail. Identifying the relationship between G-endurance and body imbalance will provide the data necessary for athletes participating in winter sports and pilots, prevent injuries, and improve exercise functions. However, this relationship has not yet been studied, to the best of our knowledge. Through this study, we aimed to provide meaningful data that can promote the relief of injuries and improve the physical abilities of those who engage in high-intensity physical activities and athletes exposed to gravitational acceleration.
Results
FMS measurements
Table 1 presents the physical characteristics of the study participants. Table 2 presents the FMS measurement results according to the grade. The FMS scores appeared in the order grade 1 > grade 3 > grade 4 > grade 2 for most items, but large variations were observed with variations in grade and measurement items.
Correlation analysis between leg length and FMS measurements
The results of the correlation analysis between leg length and FMS scores are shown in Table 3. Leg length showed a statistically significant correlation with hurdle step (p < 0.01), inline lunge (p < 0.01), and active straight leg raise (p < 0.01). Functional and structural leg lengths also showed statistically significant correlations.
Imbalance analysis results according to G-test
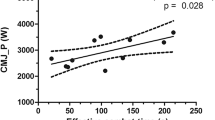
Figure 1 presents the left and right imbalance analysis results based on the G-test. A statistically significant difference in left and right imbalance was observed in active straight leg raise (p < 0.05) in the G-test-passed (GP) group, deep squat (p < 0.05), and shoulder mobility (p < 0.01) in the G-test-failed (GF) group, and rotary stability (p < 0.05) and functional leg length (p < 0.05) in both groups.

Left and right imbalance analysis results according to G-test results.
Discussion
High-intensity training is essential in improving the body's function; however, continuous high-intensity training that is not based on the structure and function of the human body may lead to poor exercise function12. FMS is easily used to assess individual limitations and asymmetry along the movement chain to prevent injuries13,14. This test is widely used in various fields15,16, and has been effectively applied to body asymmetry and functional movement measurements5,17.
The FMS test is used to assess elite sports athletes and Air Force pilots who perform high-intensity physical activity18,19. The body asymmetry of the Air Force cadets, as measured by FMS, affects G-force resistance under gravitational acceleration8. Our study confirmed that the difference in lower extremity imbalance affects the G-test result of cadets, and similar results were seen in previous studies. In addition, the FMS of cadets in the GF group showed a particularly significant difference in the three events of the one-sided measurement, namely the hurdle step, inline lunge, and active straight leg raising. Similar results were also seen in a previous study conducted on Air Force cadets8. This implies that the results of the FMS one-sided measurement vary based on physical imbalance, proving the need for an alternative procedure to complement the training process and prevent injury. Since movement restrictions and asymmetry are closely related to injury, developing strategies to prevent injury and improve function is necessary.
This conclusion also applies to athletes who must endure G-tolerance during sporting sports. Our results indicate that functional movement and physical imbalance can affect the performance of athletes competing in sports affected by gravity acceleration (e.g., sledding sports). Because winter sports, as well as some racing sports, may be affected by gravity acceleration, the physical ability to overcome this phenomenon is also important. For example, sledding sports, such as bobsleigh, are exposed to 4–5 G of gravitational acceleration during training and competition. Historically, the emphasis on functional and balance training in winter sports has been comparatively limited. Additionally, gravity-based data is essential for athletes who are affected by G-tolerance, such as racers and athletes in sledding events such as bobsleigh and skeleton, but surprisingly, such research in sports has not been documented as far as we know20. This is believed to be due to practical difficulties in obtaining G-test data for these athletes, unlike Air Force facilities equipped with experimental environments. Additionally, deriving meaningful data is challenging due to the low number of athletes. To overcome these limitations, we conducted a study targeting Air Force Academy cadets, a special group exposed to gravitational acceleration. Based on the FMS and G-test results, body imbalance was related to athletic ability; these results suggest that athletic ability, asymmetry, damage measurement, and management are essential for athletes responding to gravitational acceleration. In particular, FMS measurements discerned functional movements and showed that concentrating on rectifying human body imbalances can enhance G-resistance and overall athletic performance in winter sports.
Although a limitation is that this study was not conducted on actual athletes, this study can still provide valuable insights as it is the first to suggest applicability to sports players affected by gravitational acceleration by targeting air force pilots under gravitational acceleration. It is considered that further studies will provide meaningful data for utilizing the data of actual winter sports athletes. Notably, according to the results of this study, a high left–right side balance can positively affect exercise performance and will help improve the performance of sports athletes who endure gravitational acceleration.
Conclusions
For people constantly subjected to gravitational acceleration, improving human asymmetry and functional movement is important in preventing injury and improving motor function. Research data on winter sports are scarce compared to those on summer sports. The present study's findings can be used as data to strengthen the performance of winter sports participants and sports athletes affected by gravity acceleration. Applying FMS to training programs to prevent injuries to athletes should be encouraged.
Methods
Participants
A total of 363 male volunteers from the Air Force Academy participated in this study. After checking the number of cases required using G*Power, it was determined that 82 study participants were needed per group under the conditions of effect size (0.25), α error (0.05), and power (0.80)21. Since male cadets account for 90% of the Air Force cadets, only male cadets were enrolled in this study. The FMS test and leg length measurements without a G-test were conducted for freshmen to third graders (273 volunteers). For fourth graders (94 volunteers), a G-test was conducted in addition to the above tests. Before the study, body composition measurements, such as weight (kg), skeletal muscle mass (%), body fat mass (kg), and body mass index (kg/m2) were performed on all volunteers. Body composition was measured two weeks before the G-test using InBody 720 (Biospace Co., Ltd., Seoul, Republic of Korea). The test was conducted 7 a.m. to maintain an empty stomach. Before every examination, all volunteers were provided with a detailed description of the study’s aim, methods, and possible risks. They were also informed that they could withdraw from the experiment at any time, if desired. Subsequently, participants signed an informed consent form. All study procedures were approved by the Institutional Bioethics Committee of the Air Force Aerospace Medical Center (ASMC-22-IRB-002). The study was conducted following the principles of the Declaration of Helsinki.
FMS test
The FMS was measured by certified inspectors in compliance with methods used in previous studies22,23,24. The test was conducted after explaining the seven motions and scoring criteria to all participants in detail. Test movements consisted of a deep overhead squat, hurdle step, inline lunge, trunk stability push-up, active straight leg raise, shoulder mobility, and rotary stability (Fig. 2). Informed consent was obtained from volunteers for participation in the study and for posting of images in online public publications. Five movements were used to evaluate symmetry by measuring right- and left-side movements. Each test was scored on a scale of 0–3, with 0 being the lowest and 3 being the highest. Pain identified during the examination was assigned a score of 0. A score of 1 was awarded when the participant could not complete the motion or when the performance was incorrect. A score of 2 indicates that the action can be completed but must be compensated somehow. A score of 3 indicates normal performance without any reward. The lowest score measured on both sides was taken as the overall score.

Details of the seven motions for functional movement screen (FMS) measurements.
Leg-length measurements
Functional and structural measurements were performed to determine leg length. After assuming a supine position with light clothing, the participants spread both legs and maintained them 15–20 cm apart. The functional leg length test was performed from the umbilicus to the medial malleolus of the tibia, and the structural leg length test was performed from the anterior superior iliac spine to the medial malleolus of the tibia. The average value was derived for all measurements by measuring each side three times using a Martin-type anthropometer (PMII, TTM, Japan).
G-test measurements
The volunteers sat in the cockpit seats of a high-speed centrifugal gondola and performed a G-test for 30 s at a 5 G acceleration of gravity. Immediately after commencing the test, the gondola started rotating at a speed of 0.8 G, and acceleration of gravity increased to 5 G as soon as the participants pulled the lever. The measurement ended 30 s after commencement, when the participant pushed the lever, or when the participant lost consciousness owing to G-LOC25,26. The criteria for G-LOC were met when the participant's upper body was bent forward, the eyes were heavy with an acceleration of gravity, the jaw muscles were relaxed, and the mouth was opened. Before commencing the G-test, instructors with more than 20 years of experience conducted training on postures, L-1 breathing methods (anti-G training maneuvers), and precautions required for the G-test3. Based on test results, the participants were classified into the GP and GF groups. The G-test was performed using a high-speed centrifugal gondola (ETC, Southampton, PA, USA) equipped at the Air Force Academy of the Aerospace Medical Center.
Statistical analysis
All statistical analyses were conducted using IBM® SPSS Statistics® for Windows (version 22.0; IBM Corp., Armonk, NY, USA), and all data are presented as mean ± standard deviation values. All data were subjected to normal verification and homogeneity verification, and normal distribution was confirmed. One-way analysis of variance with post-hoc Tukey's test was used to analyze left–right imbalance by the grade level of Air Force cadets. An independent samples t-test was used to analyze FMS test results and functional leg length differences according to whether the grade 4 cadets passed the G-test. Moreover, correlation analysis was conducted to confirm the correlation between FMS and functional leg length. Statistical significance was set at p < 0.05.
Institutional review board statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Bioethics Committee of the Air Force Aerospace Medical Center (ASMC-22-IRB-002).
Informed consent
Informed consent was obtained from all participants involved in the study.
Data availability
The data presented in this study are available on request from the corresponding author.
References
Wochyński, Z. Evaluation of judo practitioners’ motor performance in relation to the criterion of targeted fitness of pilot cadets after a six-month training process. Arch. Budo 17, 319–328 (2021).
Prokopczyk, A. & Wochyński, Z. Changes in physical fitness and body composition of pilot cadets before and after a process of directed flight preparation. BMC Sports Sci. Med. Rehabil. 14(1), 153 (2022).
Pavlović, M., Ogrinc, N. & Šarabon, N. Body asymmetries as risk factors for musculoskeletal injuries in dancesport, hip-hop and ballet dancers?. Eur. J. Transl. Myol. 32(4), 11020 (2022).
Yoon, D. Y., Choi, J. S., Jeong, S. H. & Kim, S. J. The analysis of erector spinae muscle on difference of functional leg length inequality—Through meridian electromyography. J. Korean Med. Rehabil. 21(3), 13–20 (2011).
Friberg, O. R. A. Clinical symptoms and biomechanics of lumbar spine and hip joint in leg length inequality. Spine 8(6), 643–651 (1983).
Cook, G., Burton, L., Hoogenboom, B. J. & Voight, M. Functional movement screening: The use of fundamental movements as an assessment of function-part 1. Int. J. Sports Phys. Ther. 9(3), 396 (2014).
Cook, G., Burton, L., Hoogenboom, B. J. & Voight, M. Functional movement screening: The use of fundamental movements as an assessment of function-part 2. Int. J. Sports Phys. Ther. 9(4), 549 (2014).
Jeong, D. H., Lee, D. R., Lee, K. L. & Sung, J. Y. Gravitational acceleration test results according to functional movement screen and morphological symmetry results of air force cadets. Symmetry 15(4), 804 (2023).
Chumbley, E. M., Stolfi, A. & McEachen, J. C. Risk factors for cervical pain in F-15C pilots. Aerosp. Med. Hum. Perform. 88(11), 1000–1007 (2017).
Shiri, R. et al. Cervical and lumbar pain and radiological degeneration among fighter pilots: A systematic review and meta-analysis. Occup. Environ. Med. 72(2), 145–150 (2015).
Sung, J. Y., Kim, I. K. & Jeong, D. H. Gravitational acceleration test results by lifestyle and physical fitness of air force cadets. Aerosp. Med. Hum. Perform. 94(5), 384–388 (2023).
Ludwig, O. & Kelm, J. Groin pain and muscular imbalance of quadriceps and hamstrings in an elite soccer player—A case study. Sportverletz Sportschaden 30(3), 163–167 (2016).
Bardenett, S. M. et al. Functional movement screen normative values and validity in high school athletes: Can the FMS™ be used as a predictor of injury?. Int. J. Sports Phys. Ther. 10(3), 303–308 (2015).
Schneiders, A. G., Davidsson, A., Hörman, E. & Sullivan, S. J. Functional movement screen normative values in a young, active population. Int. J. Sports Phys. Ther. 6(2), 75–82 (2011).
Smith, C. A., Chimera, N. J., Wright, N. J. & Warren, M. Interrater and intrarater reliability of the functional movement screen. J. Strength Cond. Res. 27(4), 982–987 (2013).
Cuchna, J. W., Hoch, M. C. & Hoch, J. M. The interrater and intrarater reliability of the functional movement screen: A systematic review with meta-analysis. Phys. Ther. Sport 19, 57–65 (2016).
Gulgin, H. & Hoogenboom, B. The functional movement screening (fms)™: An inter-rater reliability study between raters of varied experience. Int. J. Sports Phys. Ther. 9(1), 14–20 (2014).
Cook, G., Burton, L. & Hoogenboom, B. Pre-participation screening: The use of fundamental movements as an assessment of function—Part 1. N. Am. J. Sports Phys. Ther. 1(2), 62–72 (2006).
Minthorn, L. M., Fayson, S. D., Stobierski, L. M., Welch, C. E. & Anderson, B. E. The functional movement screen’s ability to detect changes in movement patterns after a training intervention. J. Sport Rehabil. 24(3), 322–326 (2015).
Rausch, M. et al. The effects of 12 weeks of functional strength training on muscle strength, volume and activity upon exposure to elevated G z forces in high-performance aircraft personnel. Mil. Med. Res. 8, 15 (2021).
Faul, F., Erdfelder, E., Buchner, A. & Lang, A. G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 41(4), 1149–1160 (2009).
Bodden, J. G., Needham, R. A. & Chockalingam, N. The effect of an intervention program on functional movement screen test scores in mixed martial arts athletes. J. Strength Cond. Res. 29(1), 219–225 (2015).
Butler, R. J. et al. Modifiable risk factors predict injuries in firefighters during training academies. Work 46(1), 11–17 (2013).
Frost, D. M., Beach, T. A., Callaghan, J. P. & McGill, S. M. FMS scores change with performers’ knowledge of the grading criteria-are general whole-body movement screens capturing “Dysfunction”?. J. Strength Cond. Res. 29(11), 3037–3044 (2015).
Kim, I. K., Jeong, D. H., Sung, J. Y. & Kim, K. S. Analysis of G-test results according to fatigue, physical fitness and body composition of air force cadets using smart watches. Exerc. Sci. 31(1), 98–104 (2022).
Sung, J. Y. & Lee, K. L. Physical strength, body composition, and G-test results of air force cadets based on nutrition knowledge differences. Sci. Rep. 14(1), 3083 (2024).
Acknowledgements
We would like to thank all the Republic of Korea Air Force Academy cadets who participated in the study. In addition, we would like to express my deep gratitude to Professor S.H.L. of the Department of System Engineering of the Republic of Korea Air Force Academy and Professor E.W.L. of the Department of Mathematics for helping organize the data and providing statistical advice. This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (NRF-2022R1I1A1A01063123).
Funding
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (NRF-2022R1I1A1A01063123).
Author information
Authors and Affiliations
Contributions
All authors were well-informed of the WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects—and confirmed that the present study fulfilled the declaration. None of the authors have financial or private relationships with commercial, academic, or political organizations or people that may have improperly influenced this research. J.-Y.S. contributed to the overall planning of the research, data acquisition, analysis and interpretation, and major drafting and revision of manuscript submission; D.-H.J. contributed to data acquisition, analysis, and interpretation, and major drafting and revision of manuscript submission; K.-L.L. contributed to the anatomical and clinical opinion for conception, overall organization, and direct supervision of the research.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sung, JY., Jeong, DH. & Lee, KL. Analysis of the relationship between body imbalance characteristics and physical ability in air force cadets: physical function and gravity acceleration resistance. Sci Rep 14, 19795 (2024). https://doi.org/10.1038/s41598-024-70531-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-70531-2
- Springer Nature Limited