
Abstract
A rise in bone turnover markers (BTM) after bariatric surgery predicts poor bone health years later. This study explored factors associated with BTM and changes in BTM after bariatric surgery. Inclusion criteria were subjects 18 to 65 years of age with morbid obesity undergoing bariatric surgery. All data were measured before and 6 and 12 months after surgery. The study included 104 subjects: women/men: 83/21; mean age 43.1 (SD 8.4) years; BMI: 38.8 kg/m2 (SD 3.8). Surgery with Roux-en-Y gastric bypass (RYGB) and sleeve gastrectomy (SG) was performed in 84 (81%) and 20 (19%) subjects, respectively. From before to 6–12 months after surgery, procollagen type 1 N-terminal propeptid (P1NP) increased by 45.6 µg/L (95% CI 41.5–50.0, p < 0.001), and alkaline phosphatase (ALP) by 10 U/L (95% CI 7–14, p < 0.001). The increases were significantly larger after RYGB than after SG. The APOE- Ɛ3 allele was associated with low levels of BTM and high levels of leptin. There was an unfavourable increase in BTM after bariatric surgery. SG compared to RYGB and the presence of the APOE-Ɛ3 allele were associated with less unfavourable effects. The study emphasises the importance of optimal prophylactic interventions after bariatric surgery to prevent osteoporosis.
Similar content being viewed by others

Introduction
Reduced bone mineral density (BMD), osteoporosis and fractures are long-term side effects of bariatric surgery. Bone loss occurs as early as 6 months after surgery, and the increased fracture risk starts gradually three years after surgery and is increased by 21–44%1,2. Surgery with Roux-en-Y Gastric Bypass (RYGB) has, in several studies, been associated with a greater increase in bone turnover markers (BTM) and risk of fractures, and reduction of BMD than Sleeve Gastrectomy (SG)1.
BTM are products of the bone remodelling process, either markers of bone formation such as procollagen type 1 N-terminal propeptide (P1NP) and bone-specific alkaline phosphatase (ALP), or markers of bone resorption, such as carboxy-terminal cross-linked telopeptide type 1 collagen (CTX-1)3,4. They respond rapidly to changes in bone turnover but have limited specificity3. The rapid response makes them suitable for monitoring response to and compliance with treatment3. The role of BTM, either alone or combined into a risk score, as a predictor of fractures has been shown in several studies, reviews, and meta-analyses but is still not established4,5,6. It is, however, reasonable to believe that reducing BTM lowers the risk of osteoporotic fractures after bariatric surgery.
Changes in nutritional factors, gut hormones, oestrogen, adipokines, neuroendocrine hormones, fat and muscle mass, and reduced mechanical load due to weight loss result in poor bone health after bariatric surgery1,7. Knowledge about the importance of each factor associated with BTM is a prerequisite for implementing targeted treatment and thereby reduce the loss of BMD and the risk of fractures. This specific knowledge is, in large, missing.
The study aimed primarily to explore associations between BTM and changes in BTM from before to 6–12 months after bariatric surgery on one side and nutritional factors, endocrine changes, APOE genotypes, and surgical methods. The secondary aim was to study changes from before to after surgery in multiple variables related to bone health.
Participants and methods
Design
Data from the prospective cohort study MO-BiPS (Morbid Obesity—Bio-Psycho-Social disorders) were used8. Blood samples from a biobank were analysed and used in this retrospective cohort study.
Participants
Subjects 18 to 65 years of age with morbid obesity (i.e. BMI > 40 or > 35 kg/m2 with complications related to obesity) referred by general practitioners to the Obesity Unit, Innlandet Hospital Trust, Gjøvik, Norway, from December 2012 to September 2014 for evaluation of bariatric surgery were asked for inclusion. Exclusion criteria were alcohol and drug abuse, previous major gastrointestinal surgery, and somatic and psychiatric comorbidity unrelated to obesity and in need of treatment. After inclusion, 6 months of preparation for surgery followed. During this period, there were regular follow-ups by doctors, nurses, and dieticians with information about the consequences of bariatric surgery, the need for dietary changes, weight loss, and physical activity. A strict "crispbread diet" or a meal replacement powder diet containing less than 4200 kJ/day was implemented in the last three weeks before surgery. Bariatric surgery was performed as RYGB or SG, decided by the surgeon in agreement with the subject9,10. After surgery, the participants were prescribed a multivitamin- and mineral supplement, calcium carbonate with vitamin D (1000 mg/800 IU) and oral iron (100 mg Fe2+ for men and post-menopausal women and 200 mg Fe2+ for pre-menopausal women) daily, and vitamin B12-injections every 3 months. Blood samples from immediately before surgery and 6 and 12 months after surgery were used in this study. More information about the participants and the design is given in previous publications8,11.
Variables
The following variables were used. Abbreviations and reference values in brackets. The participants were asked to meet at the hospital in a fasting state in the morning, but persons living far away from the hospital might have had a small meal before leaving home.
-
Demographic and anthropometric data: Age (years). Biological sex (male/female). Height (m). Body weight (kg). Body mass index (BMI; kg/m2).
-
BTM (serum): Serum procollagen type 1 N-terminal propeptide (P1NP): (11–94 µG/L). Total serum alkaline phosphatase (ALP): (35–105 U/L). P1NP and bone-specific ALP are markers of osteoblast activity. Changes in total ALP related to changes in the liver-specific markers alanine aminotransferase (ALAT) and gamma-glutamyltransferase (gamma GT) were judged as changes in bone-specific ALP.
-
Biochemistry (serum): C-reactive protein (CRP): (< 4 mg/L). Ionised Calcium (iCa): (1.15–1.33 mmol/L). Phosphate (Ph): (0.7–1.7 mmol/L). Magnesium (Mg): (0,71–0,94 mmol/L). ALAT: (10–70 U/L). Gamma GT: (10–115 U/L).
-
Hormones: Free thyroxin (FT4): (8.5–16.5 pmol/L). Thyroid stimulating hormone (TSH): (0.44–3.1 mU/L). Leptin: (BMI < 25: women/men: 80–2500/ < 950 pmol/L). Adiponectin: (women/men: 4–22/2–20 mg/L). Parathyroid hormone (PTH): (1.2–7.1 pmol/L).
-
Vitamins: Pyridoxal-5’-phosphate (Vitamin B6): (15–160 nmol/L). 25-Hydroxyvitamin D (Vitamin D): (37–131 nmol/L).
-
Apolipoprotein E (APOE) genotypes: (Ɛ2Ɛ2, Ɛ2Ɛ3, Ɛ3Ɛ3, Ɛ2Ɛ4, Ɛ3Ɛ4, and Ɛ4Ɛ4). Genotyping was performed with allele-specific real-time polymerase chain reactions. Analyses unveiled significant differences between carriers and noncarriers of the APOE-Ɛ3 allele, and this post hoc dichotomisation was used in the analyses.
Statistics
Descriptive data are reported as the mean (SD) and number with proportion (%). A linear mixed regression model for repeated analyses based on 10,000 bootstrap samples was used and reported as estimated marginal means or estimated coefficients (B-values) with 95% confidence intervals (percentiles) and p values. The changes in the variables from 6 to 12 months after surgery were judged as insignificant. Therefore, and to increase the power of the study, in the subjects with data from both 6 and 12 months after surgery, these results were combined in the analyses and compared with the data before surgery. The analyses were performed with IBM SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY, USA).
Results
Out of 152 correctly included subjects, 115 completed the lifestyle intervention and underwent bariatric surgery. This study included 104 subjects (women/men: 83/21 with a mean age of 43.1 (SD: 8.4) years, BMI: 38.8 kg/m2 (SD 3.8), with an APOE genetic test and at least one P1NP analysis. P1NP analyses were available in 96, 93 and 85 subjects before, and 6 and 12 months after surgery, respectively. Sixty-one subjects had leptin and adiponectin analyses before and 12 months after surgery. At inclusion, 20 (19%) were daily smokers, and 18 (17%) had diabetes. Surgery with RYGB and SG was performed in 84 (81%) and 20 (19%) subjects, respectively. The distribution of the APOE genetic variants was as follows: Ɛ2Ɛ2: 0 (0%); Ɛ2Ɛ3: 10 (10%); Ɛ3Ɛ3: 54 (52%); Ɛ2Ɛ4: 3 (3%); Ɛ3Ɛ4: 35 (34%), and Ɛ4Ɛ4: 2 (2%).
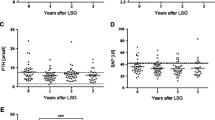
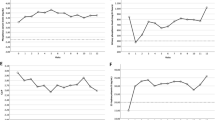
The BTM P1NP and ALP increased significantly after surgery and significantly more after RYGB than after SG. Most variables changed significantly from before to after surgery: Ph, vitamin D, and adiponectin increased, and CRP, vitamin B6, ALAT, gamma GT, FT4 and leptin decreased. Only the changes in P1NP and ALP were dependent on the surgical method. Table 1 gives the characteristics of the participants at inclusion and 6–12 months after surgery, comparisons between before and after surgery, and comparisons between the changes from before to after surgery with RYGB and SG.
Four variables showed significant differences between subjects with and without the APOE-Ɛ3 allele. The levels of P1NP, ALP, and PTH were lower, and leptin was higher in subjects with the Ɛ3 allele than in those without. Table 2 gives the results. Other significant differences between subjects with and without the e3 allele were not found, and no changes from before to after surgery were dependent on the Ɛ3 allele (data not shown).
There was a significant positive association between P1NP and ALP (Table 3). Associations between the BTM P1NP and ALP and variables known to be associated with BMD and osteoporosis are given in Table 3. P1NP and ALP were positively associated with PTH. None of the associations between P1NP and ALP on one side and one by one of leptin, adiponectin, iCa, Ph, Mg, vitamin D, vitamin B6, FT4, and TSH were statistically significant.
Associations between P1NP and ALP on one side and BMI, smoking habits, diabetes and CRP in addition to age, sex, point of time, surgical method, and APOE-Ɛ3 are given in Table 4. Age was positively associated with P1NP and ALP, and female sex was positively associated with ALP.
Discussion
The main findings were the significant increase in the P1NP and ALP 6–12 months after bariatric surgery. The strong association between P1NP and ALP indicates a common cause of the changes. The increases were significantly higher after RYGB than after SG, a difference that has also been reported in other studies1,12,13,14,15. Changes in other variables were not dependent on the surgical method. An interesting finding was the low levels of P1NP and ALP in subjects with the APOE-Ɛ3 allele. For the maintenance of good bone health after bariatric surgery, SG is preferable to RYGB, especially in subjects without the APOE-Ɛ3 allele.
P1NP and CTX-1 are elevated in subjects with osteoporosis and are recommended as biomarkers of bone formation and resorption, respectively3. Several studies indicate that P1NP and other BTM predict bone loss and progression toward osteoporosis and fractures4,5,6. Increased fracture risk and clinically overt osteoporosis take years to develop1. However, the detrimental effects of bariatric surgery on bone mass and microarchitecture are detectable 6 months postoperatively, which is in accordance with the rapid increase in BTM seen in this and other studies2. The differences in BTM after RYGB and SG agree with studies showing a reduction in BMD and increased risk of fractures after RYGB compared with SG1,14,15,16. SG is a purely restrictive procedure, while RYGB is a combined restrictive and malabsorptive procedure with a higher impact on fat and micronutrient absorption and bone health.
The associations between APOE-Ɛ3 and low values of BTM and PTH and high leptin values indicate a protective effect of the Ɛ3 allele on bone health. The role of APOE as a genetic risk factor for bone turnover, BMD, osteoporosis, and fractures in humans is inconclusive, which contrasts with the established role in mice17,18. The comprehensive meta-analysis by Lumsden et al. reports no significant associations between APOE genotypes and osteoporosis, osteopenia, pathological fractures or other disorders of the bone and cartilage19. In contrast, several studies have reported significant associations between APOE genetic polymorphisms and bone disease. Diekmann et al. reported increased levels of bone formation and resorption markers and reduced trabecular bone in Ɛ2 carriers, both in mice and humans, and concluded that the Ɛ2 allele is a genetic risk factor for low bone mass and fractures20. Other studies have reported associations between the Ɛ4 allele and hip fractures in a community-based study of older adults, reduced BMD in postmenopausal women with rheumatoid arthritis and the Ɛ4 allele, and reduced BMD and increased incidence of fractures in postmenopausal women with Ɛ2 and Ɛ4 compared with Ɛ3 carriers21,22,23. These findings agree with this study's favourable effects of the Ɛ3 allele. All Ɛ3-associated effects, low P1NP, ALP, and PTH and high leptin, are favourable for bone health.
Not only did P1NP and ALP change significantly after surgery. Changes in macro- and micronutrients, inflammatory markers, adipokines and gastrointestinal hormones are common after bariatric surgery and are involved in bone health1,7,24,25. In this study, Ph, vitamin D, and adiponectin increased, and CRP, ALAT, gamma GT, vitamin B6, FT4, and leptin decreased.
BTM were positively associated with age, female sex, PTH, RYGB, and absence of the APOE-Ɛ3 allele26. The associations with age and female sex were as expected. The prevalence of osteoporosis is higher in females than in men and increases with age. Secondary hyperparathyroidism, sometimes defined as an elevated PTH without elevated iCa, is a known complication after bariatric surgery14,27. This study gives no indication of secondary hyperparathyroidism. The expected decrease in iCa and increase in PTH were not observed, probably due to supplementation of vitamin D and Ca7,27.
The decrease in CRP and leptin and the increase in adiponectin after bariatric surgery and weight loss are well-known changes25. Leptin acts on bone metabolism through a central pathway, which inhibits bone formation and promotes resorption, and a peripheral pathway with opposite effects; the net result in most studies is a positive association between leptin and BMD1,24,28. Adiponectin and inflammatory markers such as CRP, which both putatively aggravate bone loss, changed in opposite directions after surgery1,24. The reduced levels of FT4, vitamin B6, and Mg, although not associated with BTM in this study, also affect bone health. Hypothyroidism increases bone mass and mineralisation, changes the bone structure, and increases the incidence of fractures26,29. Vitamin B6 is positively associated with BMD30. Smoking and low Mg values are related to osteoporosis, and Mg supplementation favours BMD and reduces fracture risk31,32. The lack of associations between BMI, smoking, diabetes, CRP, Mg, vitamin B6, FT4, leptin, adiponectin, CRP on one side and P1NP and ALP on the other could indicate that these factors affect bone health by mechanisms other than activation of BTM.
Impaired bone health after bariatric surgery occurs despite individual follow-up, nutritional advice and adequate supplementation of Ca and vitamin D. Pre- and postsurgery deficiencies in macro- and micronutrients (e.g. vitamins A, B1, D, K, and folate, iron, zink and selenium) are most likely involved in the pathogenesis33,34.
Strengths and limitations
This study population, which was unselected subjects from the general population referred to the only obesity unit in the region, is representative of subjects undergoing bariatric surgery. The follow-up rate was satisfactory, and appropriate variables, including genetic markers, were used in the analyses. Most studies include both markers of bone formation and bone resorption. In this study, only markers of bone formation (P1NP and ALP) were used. CTX-1, a marker of bone resorption often measured in combination with P1NP, is sensitive to correct sampling and storing and was omitted because analyses in blood samples stored for ten years in a biobank might be unreliable. P1NP seems more sensitive to changes in bone metabolism than CTX-115,26. Minor differences in the ratio between these two markers of bone formation and resorption could mean net bone gain or loss. Total ALP was used instead of bone-specific ALP. The increase in ALP and fall in ALAT and gamma GT after surgery render it likely that the increase in ALP is an increase in bone-specific ALP. The results based on the genetic marker APOE are encumbered with uncertainty because the dichotomisation into the APOE-Ɛ3 and non Ɛ3 groups was performed post hoc. The dichotomisation was one of several ways to dichotomise the variable, and the non Ɛ3 group was small. The results, which could be a type I error, were, however, in accordance with other reports20,21,22,23. The fact that most changes in the variables were within the normal ranges (the reference ranges) could question the clinical relevance of the changes. The identical pattern in the changes, which were highly significant, substantiates the clinical relevance. The use of a linear mixed regression model with bootstrapping is a recommended method for analyses of repeated measurements and reduces uncertainty about normality of the data.
Conclusions
BTM increased significantly after bariatric surgery. The significant increase in P1NP and ALP 6–12 months after surgery, with a significantly higher increase following RYGB than SG, predicts bone loss with progression toward osteoporosis and fractures. High BTM (P1NP and ALP) was positively associated with female sex, age, and PTH, which are risk factors for osteoporosis and fractures. The presence of the APOE-Ɛ3 allele was associated with low BTM and PTH, and high leptin, which are favourable for bone health. The increase in adiponectin, and decrease in vitamin B6, FT4, and leptin were markers of unfavourable changes, whereas the increase in vitamin D and lower CRP were favourable changes. The changes in these variables, which affect bone health, were not associated with the BTM in this study and might act on other mechanisms. This study indicates that SG is preferable to RYGB for preserving good bone health after bariatric surgery. However, RYGB might have other metabolic advantages to SG that must be considered when choosing the type of surgery. The study emphasises the importance of optimal preventive intervention, especially in predisposed subjects, to avoid a detrimental effect of bariatric surgery on bone health. Supplementation with vitamin D, vitamin B6, and Ca is mandatory to avoid secondary hyperparathyroidism and micronutrient deficiencies.
Ethics approval and consent to participate
The study was approved by the Norwegian Regional Committees for Medical and Health Research Ethics, PB 1130, Blindern, 0318 Oslo, Norway (reference number 2012/966 with an amendment of June 28, 2018). The study was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants before inclusion.
Data availability
The raw datasets generated and analysed during the current study are not publicly available to protect participant confidentiality. Case report forms (CRFs) on paper are safely stored. The data were transferred to SPSS for statistical analyses, and the data files are stored by Innlandet Hospital Trust, Brumunddal, Norway, on a server dedicated to research. The security follows the rules given by The Norwegian Data Protection Authority, P.O. Box 8177 Dep. NO-0034 Oslo, Norway. The data are available on request to the author.
Abbreviations
- ALAT:
-
Alanine aminotransferase
- ALP :
-
Alkaline phosphatase
- APOE :
-
Apolipoprotein E genotypes
- BMD:
-
Bone mineral density
- BMI :
-
Body mass index
- BTM :
-
Bone turnover markers
- CTX-1 :
-
Carboxy-terminal cross-linked telopeptide type 1 collagen
- CI:
-
Confidence interval
- CRP :
-
C-reactive protein
- Gamma GT:
-
Gamma-Glutamyltransferase
- FT4 :
-
Free thyroxin
- iCA:
-
Ionised Calcium
- Mg :
-
Magnesium
- P1NP :
-
Procollagen type 1 N-terminal propeptide
- Ph :
-
Phosphate
- PTH :
-
Parathyroid hormone
- RYGB :
-
Roux-en-Y Gastric Bypass
- SD :
-
Standard deviation
- SG :
-
Sleeve gastrectomy
- TSH :
-
Thyroid stimulating hormone
- Vitamin B6 :
-
Pyridoxal-5’-phosphate
- Vitamin D :
-
25-Hydroxyvitamin D
References
Paccou, J. et al. Bariatric surgery and skeletal health: A narrative review and position statement for management by the European calcified tissue society (ECTS). Bone 154, 116236. https://doi.org/10.1016/j.bone.2021.116236 (2022).
Schafer, A. L. et al. Effects of gastric bypass surgery on bone mass and microarchitecture occur early and particularly impact postmenopausal women. J. Bone Miner. Res. 33, 975–986. https://doi.org/10.1002/jbmr.3371 (2018).
Williams, C. & Sapra, A. Osteoporosis Markers (StatPearls, Treasure Island, 2023).
Schini, M., Vilaca, T., Gossiel, F., Salam, S. & Eastell, R. Bone turnover markers: Basic biology to clinical applications. Endocr. Rev. 44, 417–473. https://doi.org/10.1210/endrev/bnac031 (2023).
Kim, B. J., Lee, S. H. & Koh, J. M. Potential biomarkers to improve the prediction of osteoporotic fractures. Endocrinol. Metab. 35, 55–63. https://doi.org/10.3803/EnM.2020.35.1.55 (2020).
Finnes, T. E. et al. Procollagen type 1 amino-terminal propeptide (P1NP) and risk of hip fractures in elderly Norwegian men and women. A NOREPOS study. Bone 64, 1–7. https://doi.org/10.1016/j.bone.2014.03.010 (2014).
Liu, C. et al. Changes in bone metabolism in morbidly obese patients after bariatric surgery: A meta-analysis. Obes. Surg. 26, 91–97. https://doi.org/10.1007/s11695-015-1724-5 (2016).
Farup, P. G. Are the results of a combined behavioural and surgical treatment of morbid obesity satisfactory and predictable?. Nutrients https://doi.org/10.3390/nu12071997 (2020).
Schauer, P. R. et al. Laparoscopic gastric bypass surgery: Current technique. J. Laparoendosc. Adv. Surg. Tech. A 13, 229–239. https://doi.org/10.1089/109264203322333557 (2003).
Roa, P. E. et al. Laparoscopic sleeve gastrectomy as treatment for morbid obesity: Technique and short-term outcome. Obes. Surg. 16, 1323–1326. https://doi.org/10.1381/096089206778663869 (2006).
Farup, P. G. & Hestad, K. The peripheral kynurenine pathway and psychosomatic comorbidity in subjects with morbid obesity undergoing bariatric surgery. Appl. Sci. Basel https://doi.org/10.3390/app12052648 (2022).
Salman, M. A. et al. Effects of gastric bypass and sleeve gastrectomy on bone mineral density and bone turnover markers: A systematic review and meta-analysis. World J. Surg. 46, 865–875. https://doi.org/10.1007/s00268-021-06429-1 (2022).
Hofso, D. et al. Bone mineral density and turnover after sleeve gastrectomy and gastric bypass: A randomized controlled trial (Oseberg). J. Clin. Endocrinol. Metab. 106, 501–511. https://doi.org/10.1210/clinem/dgaa808 (2021).
de Holanda, N. C. et al. Secondary hyperparathyroidism, bone density, and bone turnover after bariatric surgery: Differences between Roux-en-Y gastric bypass and sleeve gastrectomy. Obes. Surg. 31, 5367–5375. https://doi.org/10.1007/s11695-021-05739-6 (2021).
Bredella, M. A., Greenblatt, L. B., Eajazi, A., Torriani, M. & Yu, E. W. Effects of Roux-en-Y gastric bypass and sleeve gastrectomy on bone mineral density and marrow adipose tissue. Bone 95, 85–90. https://doi.org/10.1016/j.bone.2016.11.014 (2017).
Ahlin, S. et al. Fracture risk after three bariatric surgery procedures in Swedish obese subjects: Up to 26 years follow-up of a controlled intervention study. J. Intern. Med. 287, 546–557. https://doi.org/10.1111/joim.13020 (2020).
Niemeier, A., Schinke, T., Heeren, J. & Amling, M. The role of apolipoprotein E in bone metabolism. Bone 50, 518–524. https://doi.org/10.1016/j.bone.2011.07.015 (2012).
Noguchi, T. et al. Apolipoprotein E plays crucial roles in maintaining bone mass by promoting osteoblast differentiation via ERK1/2 pathway and by suppressing osteoclast differentiation via c-Fos, NFATc1, and NF-kappaB pathway. Biochem. Biophys. Res. Commun. 503, 644–650. https://doi.org/10.1016/j.bbrc.2018.06.055 (2018).
Lumsden, A. L., Mulugeta, A., Zhou, A. & Hypponen, E. Apolipoprotein E (APOE) genotype-associated disease risks: A phenome-wide, registry-based, case-control study utilising the UK Biobank. EBioMed. 59, 102954. https://doi.org/10.1016/j.ebiom.2020.102954 (2020).
Dieckmann, M. et al. Human apolipoprotein E isoforms differentially affect bone mass and turnover in vivo. J. Bone Miner. Res. 28, 236–245. https://doi.org/10.1002/jbmr.1757 (2013).
Johnston, J. M., Cauley, J. A. & Ganguli, M. APOE 4 and hip fracture risk in a community-based study of older adults. J. Am. Geriatr. Soc. 47, 1342–1345. https://doi.org/10.1111/j.1532-5415.1999.tb07436.x (1999).
Lee, S. I., Lee, S. Y. & Yoo, W. H. Association of apolipoprotein E polymorphism with bone mineral density in postmenopausal women with rheumatoid arthritis. Rheumatology 44, 1067–1068. https://doi.org/10.1093/rheumatology/keh675 (2005).
Souza, L. S. et al. Role of APOE gene in bone mineral density and incidence of bone fractures in brazilian postmenopausal women. J. Clin. Densitom. 21, 227–235. https://doi.org/10.1016/j.jocd.2017.03.005 (2018).
Gkastaris, K., Goulis, D. G., Potoupnis, M., Anastasilakis, A. D. & Kapetanos, G. Obesity, osteoporosis and bone metabolism. J. Musculoskelet. Neuronal. Interact. 20, 372–381 (2020).
Huang, J. et al. Change in adipokines and gastrointestinal hormones after bariatric surgery: A meta-analysis. Obes. Surg. 33, 789–806. https://doi.org/10.1007/s11695-022-06444-8 (2023).
Blom-Hogestol, I. K. et al. Bone metabolism, bone mineral density and low-energy fractures 10 years after Roux-en-Y gastric bypass. Bone 127, 436–445. https://doi.org/10.1016/j.bone.2019.07.014 (2019).
Hewitt, S. et al. Relationships of serum 25-hydroxyvitamin D, ionized calcium and parathyroid hormone after obesity surgery. Clin. Endocrinol. 88, 372–379. https://doi.org/10.1111/cen.13531 (2018).
Chen, X. X. & Yang, T. Roles of leptin in bone metabolism and bone diseases. J. Bone Miner. Metab. 33, 474–485. https://doi.org/10.1007/s00774-014-0569-7 (2015).
Dyrek, N., Wikarek, A., Niemiec, M. & Kocelak, P. Selected musculoskeletal disorders in patients with thyroid dysfunction, diabetes, and obesity. Reumatologia 61, 305–317. https://doi.org/10.5114/reum/170312 (2023).
Welan, R. Effect of vitamin B6 on osteoporosis fracture. J. Bone Metab. 30, 141–147. https://doi.org/10.11005/jbm.2023.30.2.141 (2023).
Rondanelli, M. et al. An update on magnesium and bone health. Biometals 34, 715–736. https://doi.org/10.1007/s10534-021-00305-0 (2021).
Weng, W., Li, H. & Zhu, S. An overlooked bone metabolic disorder: Cigarette smoking-induced osteoporosis. Genes https://doi.org/10.3390/genes13050806 (2022).
Aaseth, J. O. & Alexander, J. Postoperative osteoporosis in subjects with morbid obesity undergoing bariatric surgery with gastric bypass or sleeve gastrectomy. Nutrients https://doi.org/10.3390/nu15061302 (2023).
Lewis, C. A. et al. Monitoring for micronutrient deficiency after bariatric surgery-what is the risk?. Eur. J. Clin. Nutr. 77, 1071–1083. https://doi.org/10.1038/s41430-023-01318-3 (2023).
Acknowledgements
The author thanks Medical Laboratory Scientists at the Unit for Special Analyses, Department of Medical Biochemistry at Oslo University Hospital for APOE genotyping.
Funding
An unrestricted grant from Innlandet Hospital Trust, Brumunddal, Norway funded the work.
Author information
Authors and Affiliations
Contributions
PGF is the guarantor of the project. He designed the main study, was responsible for practical implementation, performed the statistical analyses, wrote the manuscript, is responsible for the integrity of the work, and approved the last version.
Corresponding author
Ethics declarations
Competing interests
The author declares no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Farup, P.G. Changes in bone turnover markers 6–12 months after bariatric surgery. Sci Rep 14, 14844 (2024). https://doi.org/10.1038/s41598-024-65952-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-65952-y
- Springer Nature Limited