
Abstract
We aimed to investigate how underweight affects the incidence of fractures, as well as the influence of cumulative, longitudinal periods of low body mass index (BMI) and changes in body weight on fracture development. Data on adults aged 40-year and over who had three health screenings between January 1, 2007, and December 31, 2009 were used to determine the incidence of new fractures. The hazard ratios (HRs) for new fractures depending on BMI, total cumulative number of underweight, and weight change over time were calculated using Cox proportional hazard analysis. In this study, 15,955 (2.8%) of the 561,779 adults were diagnosed with fractures more than once over three health examinations. The fully adjusted HR for fractures in underweight individuals was 1.173 (95% Confidence interval [CI] 1.093–1.259). Underweight individuals diagnosed only once, twice, or three times had an adjusted HR of 1.227 (95%CI 1.130–1.332), 1.174 (95%CI 1.045–1.319), and 1.255 (95%CI 1.143–1.379), respectively. Although the adjusted HR was higher in adults who consistently had underweight (HR; 1.250 [95%CI 1.146–1.363]), those with underweight had an increased risk of fractures regardless of weight change (HR; 1.171 [95%CI 1.045–1.312], and 1.203[95%CI 1.075–1.346]). Underweight is a risk factor for fractures in adults over the age of 40 years, even if they returned to normal weight.
Similar content being viewed by others


Introduction
Fractures are one of the leading causes of morbidity and mortality among adults, particularly the elderly1. Fractures are also directly related with increased social expenses, as they can result in extended absences, substantial use of medical resources, and long-term impairment2. Age, gender, menopause, underweight, obesity, smoking, excessive alcohol use, and lack of physical activity are well-known risk factors associated with an increase in fractures3,4,5,6,7,8,9,10,11. Weight loss has been linked to osteoporosis and sarcopenia, and weight gain has been demonstrated to help maintain bone density12,13. Therefore, it may be assumed that weight loss affects bone density and raises the risk of fractures, whereas, weight gain maintains bone density and reduces the incidence of fractures.
Weight is a major determinant of health status, including metabolic, immunological, reproductive, and musculoskeletal functioning14. Being underweight can result in poor physical health, which is directly related with an increased risk of mortality and morbidity15,16. Additionally, being underweight may be linked to reduced bone density, soft tissue loss, and muscle weakness; hence, increasing the risk of fractures13. However, weight gain without an increase in muscle mass did not prevent fractures, but rather increased their incidence17. Due to unfavorable attitudes and discrimination against obesity, a greater proportion of adults, particularly women, are underweight in modern culture18. Therefore, it is crucial to examine the relationship between underweight and fractures. Consequently, we attempted to assess the risk of fracture resulting from an underweight using a database containing health examination results from the general Korean population. The purpose of this study was to investigate how being underweight affects the incidence of fractures, as well as the influence of cumulative numbers of low BMI on fracture development.
Methods
Data source, study design and population
The study protocol was approved by the Institutional Review Board of Korea University Ansan Hospital (Approval No. K2021-2601-001). The ethics committees of Korea University Ansan Hospital have waived the requirement to obtain informed consent as the register data analysed in this study are in anonymised and deidentified format. This study was performed in accordance with the tenets of the Declaration of Helsinki, and all research methods were carried out in accordance with appropriate regulations and guidelines.
The KNHIS database contains health information of the entire Korean population (approximately 50 million people), including diagnoses (ICD-10) and prescriptions as well as procedures19. All insured Koreans aged 40 years and older and all workers aged 20 years and older must undergo regular health screening examinations one or two years20. Among the information contained in these health-screening records include anthropometric measurements and lifestyle questionnaires, socioeconomic data and records of prescriptions and hospitalizations as well as outpatient records and death dates for the insured Korean population.
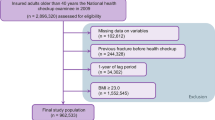
Data on adults over the age of 40 who had three consecutive general health tests between January 1, 2007, and December 31, 2009 was collected from this database and used to establish a long-term cohort study. Patients who previously suffered from osteoporotic fractures and with incomplete information were excluded from the study. The impact of being underweight was amplified by applying a one-year time lag after the screening process had been carried out. In total, this research included 561,779 participants (Fig. 1). Fracture cases were tracked in this cohort from the time of initial health assessment to the end of the cohort's designated follow-up period (December 2018) or the participant's death. Fractures were defined as any fracture that resulted in a claim for hospitalization or outpatient treatment after the index general health-screening date.

Flow chart of study population.
Evaluation of body weight
This information was taken from the general health screening results. BMI was calculated as: weight in kilograms divided by their height in meters squared (kg/m2). Underweight (< 18.5), normal (≥ 18.5 and < 23), overweight (≥ 23 and < 25), obesity (≥ 25 and < 30), and severely obesity (≥ 30) were defined by the WHO Asia–Pacific regional guidelines21,22. The cumulative number of underweight diagnosed at each health screening examinations (0 to 3 times) was counted and divided into four groups.
Each time a patient was screened, their body weight status was reported. The total number of people who were identified to be overweight or obese as a result of routine health examinations was used to calculate the number of people who were actually underweight. As part of our study, we evaluated the diagnoses of underweight status at the first and final health screenings to see how BMI changes over time could affect fractures. There were four groups of people in the study: underweight to underweight (U-to-U), underweight to non-underweight (U-to-N), non-underweight to underweight (N-to-U), and non-underweight to non-underweight (N-to-N).
Operational definitions of fractures
We utilized ICD-10, procedure, and radiographic study codes to search all the fracture cases from the insurance claim database1,23,24. ICD-10 codes for each fractures were the following: vertebral fracture [S22.0 (fracture of the thoracic spine), S22.1 (multiple fractures of the thoracic spine), S32.0 (fracture of the lumbar spine), S32.7 (multiple fractures of the lumbar spine), T080 (fracture of the spine), M48.4 (fatigue fracture of vertebra)], hip fracture [S72.0 (fracture of the femur neck) and S72.1 (trochanteric fracture)], humerus fracture [S42.2 (fracture of upper end of humerus), S42.3 (fractured shaft of humerus)], and radius fractures [S52.5 (fracture of lower end of radius) and S52.6 (fracture of lower end of both ulnar and radius)]23.
Covariates and measurements
In this study, baseline demographic data were defined as those from the most recent health screening. Socioeconomic data, laboratory results (cholesterol, fasting glucose, blood pressure, triglyceride), responses to lifestyle questionnaires (regular exercise, smoking, alcohol consumption), anthropometric measurements (height, weight, waist circumference), and medical histories, which included hypertension, diabetes, dyslipidemia, and chronic kidney disease (CKD), comprised these fundamental characteristics25. Regarding medical history, comorbidities were provided if a record at the health screening or past medical claim data indicated their presence.
Non-smokers, former smokers, and current smokers were distinguished by their smoking status. According to the amount of alcohol consumed daily, participants were categorized as non-drinkers, light drinkers (less than 30 g/day), or heavy drinkers (more than 30 g/day). Regular exercise was defined as at least 20 min of vigorous exercise on at least three days per week or 30 min of moderate to intense exercise on at least five days per week. The income was classified as low if it fell within the bottom 20 percent of the yearly income, or as normal otherwise. Appendix I is a listing of the ICD-10 codes utilized for this investigation.
Statistical analysis
According to the total number of underweight patients, baseline parameters of the study population are reported as mean (± standard deviation) or counts (percentages). The incidence rate (IR) per 1,000 person-years (PY) with 95% confidence intervals (95%CIs) was used to define the IR. We calculated the hazard ratios (HRs) with 95%CIs for the incidence of fractures by the BMI at the time of the index health screening examination (3rd exam; 2009) and the cumulative numbers of underweight using Cox’s regression analysis. The proportional-hazards assumption was assessed using the Schoenfeld residuals test, with a logarithm of the cumulative hazard functions based on Kaplan–Meier estimates26. Over time, there was no significant departure from proportionality in the hazards. To decrease covariate bias, we compared HRs for unadjusted and three adjusted models: Model 1 was adjusted for age and sex; Model 2 was adjusted for age, sex, and additional environmental factors including smoking, alcohol consumption, regular exercise, and low income; and Model 3 was fully adjusted for age, sex, additional environmental factors (smoking, alcohol consumption, regular exercise, and income), and comorbidities (diabetes, hypertension, dyslipidemia, and CKD). Statistical analysis was conducted with the SAS 9.3 program (SAS Institute, Cary, NC, USA). The analysis of variance for continuous variables and the chi-square test for categorical variables were utilized, and a two-sided p < 0.05 was regarded statistically significant.
Results
Baseline characteristics
Table 1 provides a summary of the baseline characteristics according to the cumulative number of underweight participants at each health screening examination. Of the total 561,779 participants, 545,824 (97.2%) had never been diagnosed as underweight. Regarding those who were underweight, 5,354 (1.0%) were diagnosed thrice, 3,672 (0.7%) were diagnosed twice, and 6,929 (1.2%) were diagnosed only once over the three health screenings. Except for age, the four groups of never-diagnosed, once-diagnosed, twice-diagnosed, and thrice-diagnosed individuals, indicated statistically significant differences in all categories investigated. Regardless of the duration of underweight status, those in the underweight group were more likely than those in the non-underweight group to be current smokers, to abstain from alcohol intake, to engage in regular exercise, and to have a low income.
The incidence and risk of fractures according to body mass index
The IRs per 1000PY of newly diagnosed fracture were 10.41 (95%CI; 9.70 – 11.12), 8.62 (95%CI; 8.48 – 8.77), 7.91 (95%CI; 7.76 – 8.07), 7.62 (95%CI; 7.48 – 7.77), and 7.80 (95%CI; 7.29 – 8.31) who were underweight, normal, overweight, obesity, and severe obesity, respectively (Table 2). Adjusted Cox’s proportional hazards regression analyses were performed to calculate adjusted HRs (model 3) for newly diagnosed fractures by the BMI at the index health screening examination. Underweight was associated with a significantly higher risk despite the adjustment for several potentially confounding variables (adjusted HR; 1.173 [95%CI; 1.093–1.259]).
Incidence and risk of fractures according to the cumulative number of underweight
A total of 36,580 fractures were detected (6.5%). The IR of fractures was 10.54 (95%CI 9.68–11.40) in the once-diagnosed underweight group, 9.88 (95%CI 8.74–11.03) in the twice-diagnosed underweight group, and 10.50 (95%CI 9.52–11.48) in the thrice-diagnosed underweight group, with the overall IR being higher in the underweight group. In contrast, there was no statistically significant serial increase in the number of fractures as the number of underweight diagnoses. The HRs were still statistically significant after adjusting for many variables. Underweight individuals diagnosed once, twice, or thrice had an adjusted HR (Model 3) for fractures of 1.227 (95%CI 1.130–1.332), 1.174 (95%CI 1.045–1.319), and 1.255 (95%CI 1.143–1.379), respectively (Table 3).
Risk of fracture according to temporal trends in body mass index changes
The IR was 8.06 (95%CI 7.98–8.15) in the N-to-N group, 10.25 (95%CI 9.09–11.41) in the N-to-U group, 10.01 (95%CI; 8.89–11.12) in the U-to-N group, and 10.49 (95%CI; 9.64–11.35) in the U-to-U group. Participants in the U-to-U, N-to-U, U-to-N group had a substantially increased risk of fractures after multivariate adjustment (HR; 1.250 [95%CI; 1.146–1.363], 1.171 [95%CI; 1.045–1.312], and 1.203[95%CI; 1.075–1.346], respectively). Adults over 40 years of age who have ever been underweight, even once, had a higher adjusted HR, and even if their weight changes, being underweight increased the risk of fracture (Table 4).
Discussion
Based on our knowledge, this is the first large population-based cohort study to establish the risk of fractures related with the cumulative burden of underweight. This study determined that underweight status increases the risk of fractures in people over 40 years of age, and increasing cumulative number in underweight does not enhance the risk of further fracture.
Despite the fact that the mechanism by which underweight increases the incidence of fractures is unknown, this study discovered that underweight is a risk factor for increased fractures27. Hypothesized to cause osteoporosis, being underweight in humans is frequently related with malnutrition. Malnutrition leads to bone deterioration and osteoporosis28,29. In addition, a low BMI is strongly associated with sarcopenia development. Previous research has demonstrated that malnourished people are more susceptible to sarcopenia30. Sarcopenia diminishes physical strength and muscular performance, leading to injuries that increase the probability of fracture31,32. Therefore, a lower BMI correlates with decreased BMD levels and diminished muscle strength. However, because this was a population-based cohort study utilizing the ICD-10 diagnostic, procedure and radiographic codes, actual skeletal muscle index and BMD scores were not available. Although this study cannot definitively explain the association between low BMI, BMD, and skeletal muscle index, the vast population database confirmed that low BMI is associated with fractures.
After adjusting for a number of factors, the association between underweight and fractures was analyzed. Compared to individuals who never had underweight, those who had been underweight at least once had an increased risk of fracture. In other words, the risk of fracture remained to increase regardless of the duration of underweight or the status of underweight; however, the risk of fracture does not increase if an individual consistently maintains a weight above the normal range. Individuals who have shifted from underweight to normal weight or normal weight to underweight are considered to have a normal weight but close to being underweight. It is believed that these people had low bone density and diminished muscle function, which raises the risk for fractures. Even if body weight is regained to a non-underweight status, adults over the age of 40 who have been underweight may have a loss in bone density or muscular strength due to an increase in fat mass relative to muscle mass33,34. Thus, adults who have ever been underweight may be at a higher risk for fractures than adults with a normal or higher body weight.
This is the only study to our knowledge that used a national database to analyze the risk of fracture in the general underweight population over 40 years. All citizens were enrolled in the national health insurance system, which is a substantial quantity of data. Furthermore, the database is regularly updated; hence, it yields substantial results that may be applied to the general population.
This study has some limitations. First, the BMD T-scores could not be directly validated. Underweight had an effect on the BMD score; however the exact effect was unknown in this investigation. Second, determining the precise number of fractures was difficult. Unlike other fractures, vertebral fractures are often asymptomatic and are more likely to be underestimated than actual fractures. Third, this study utilized a national database from one nation's national health insurance services, making it difficult to adapt to multiple ethnic groups. Because fractures were identified using the fracture diagnostic code in this analysis, we were unable to validate that all fractures were appropriately diagnosed. The best way to confirm the suggested algorithm of diagnostic codes is through validation studies. In order to identify fractures, the same operational definitions established in previous studies were utilized in this study4,23. To diagnose fractures as precisely as possible, we excluded individuals with previous fractures and employed a one-year lag time period after underweight diagnosis. It is highly probable that the incidence rate of fractures was significantly underestimated due to the implementation of the most conservative methodology in this study. Finally, we tried to analyze as many factors as possible. While analyzing and adjusting for confounding factors is an important to increase the reliability of a study, no study is ideal and there is always a possibility of unmeasured or unanalyzed confounding factors. Therefore, while efforts were made to adjust for confounding factors in this study to obtain more accurate results, future research is needed for better understanding, and its limitations should be taken into account.
In conclusion, this study investigated whether being underweight is an important factor that increases the risk of fracture in the Korean population over 40-year-old individuals using a nationwide population-based cohort. Adults over the age of 40 who were underweight had an increased risk of fractures, even if they returned to normal weight.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Park, S. M. et al. Incidence and mortality of subsequent vertebral fractures: Analysis of claims data of the Korea National Health Insurance Service from 2007 to 2016. Spine J. 20, 225–233. https://doi.org/10.1016/j.spinee.2019.09.025 (2020).
Han, S. et al. Changes in physical activity and risk of fracture: A Korean nationwide population-based cohort study. Sci. Rep. 10, 16266. https://doi.org/10.1038/s41598-020-73495-1 (2020).
Unnanuntana, A., Gladnick, B. P., Donnelly, E. & Lane, J. M. The assessment of fracture risk. J. Bone Joint Surg. Am. 92, 743–753. https://doi.org/10.2106/JBJS.I.00919 (2010).
Han, S. et al. Severity of underweight and risk of fracture: A Korean nationwide population-based cohort study. Sci. Rep. 12, 10153. https://doi.org/10.1038/s41598-022-14267-x (2022).
Han, S. et al. Changes in underweight status and risk of hip fracture: A Korean nationwide population-based cohort study. J. Clin. Med. 11, 1913. https://doi.org/10.3390/jcm11071913 (2022).
Han, S. et al. Incidence of hip fracture in underweight individuals: A nationwide population-based cohort study in Korea. J. Cachexia Sarcopenia Muscle 13, 2473–2479. https://doi.org/10.1002/jcsm.13046 (2022).
Umehara, T. et al. Physical functions and comorbidity affecting collapse at 4 or more weeks after admission in patients with osteoporotic vertebral fractures: A prospective cohort study. Asian Spine J. 16, 419–431. https://doi.org/10.31616/asj.2020.0285 (2022).
Cho, M. J., Moon, S. H., Lee, J. H. & Lee, J. H. Association between osteoporotic vertebral compression fractures and age, bone mineral density, and European quality of life-5 dimensions in Korean postmenopausal women: A nationwide cross-sectional observational study. Clin. Orthop. Surg. 13, 207–215. https://doi.org/10.4055/cios20209 (2021).
Jang, H. D. et al. Management of osteoporotic vertebral fracture: Review update 2022. Asian Spine J. 16, 934–946. https://doi.org/10.31616/asj.2022.0441 (2022).
Choi, J. Y., Park, S. M., Kim, H. J. & Yeom, J. S. Recent updates on minimally invasive spine surgery: Techniques, technologies, and indications. Asian Spine J. 16, 1013–1021. https://doi.org/10.31616/asj.2022.0436 (2022).
Lee, S. Y., Seo, M.-S. & Yoo, J.-I. Effectiveness of weekly teriparatide injection in postmenopausal patients with hip fractures. Clin. Orthop. Surg. https://doi.org/10.4055/cios22280 (2023).
Gariballa, S. & Alessa, A. Sarcopenia: Prevalence and prognostic significance in hospitalized patients. Clin. Nutr. 32, 772–776. https://doi.org/10.1016/j.clnu.2013.01.010 (2013).
Nielson, C. M., Srikanth, P. & Orwoll, E. S. Obesity and fracture in men and women: An epidemiologic perspective. J. Bone Miner. Res. 27, 1–10. https://doi.org/10.1002/jbmr.1486 (2012).
Lim, J. & Park, H. S. Relationship between underweight, bone mineral density and skeletal muscle index in premenopausal Korean women. Int. J. Clin. Pract. 70, 462–468. https://doi.org/10.1111/ijcp.12801 (2016).
Suastika, K. et al. Underweight is an important risk factor for coronary heart disease in the population of Ceningan Island. Bali. Diab. Vasc. Dis. Res. 9, 75–77. https://doi.org/10.1177/1479164111422828 (2012).
Tamakoshi, A. et al. BMI and all-cause mortality among Japanese older adults: Findings from the Japan collaborative cohort study. Obesity (Silver Spring) 18, 362–369. https://doi.org/10.1038/oby.2009.190 (2010).
Kim, J. et al. Association between body mass index and fragility fracture in postmenopausal women: A cross-sectional study using Korean National Health and Nutrition Examination Survey 2008–2009 (KNHANES IV). BMC Womens Health 21, 60. https://doi.org/10.1186/s12905-021-01209-4 (2021).
Buhlmann, U. et al. Updates on the prevalence of body dysmorphic disorder: A population-based survey. Psychiatry Res. 178, 171–175. https://doi.org/10.1016/j.psychres.2009.05.002 (2010).
Kwon, S. Payment system reform for health care providers in Korea. Health Policy Plan. 18, 84–92. https://doi.org/10.1093/heapol/18.1.84 (2003).
Choi, E. K. Cardiovascular research using the Korean National Health Information Database. Korean Circ. J. 50, 754–772. https://doi.org/10.4070/kcj.2020.0171 (2020).
Organization, W. H. The Asia-Pacific perspective: redefining obesity and its treatment. (2000).
Al Jawaldeh, A., Osman, D., Tawfik, A. & Organization, W. H. Food and nutrition surveillance systems: A manual for policy-makers and programme managers (2014)
Ahn, S. H. et al. Osteoporosis and osteoporotic fracture fact sheet in Korea. J. Bone Metab. 27, 281–290. https://doi.org/10.11005/jbm.2020.27.4.281 (2020).
Yu, M. H. et al. Operational definition identifying osteoporotic vertebral fractures in the claims database. J. Korean Med. Sci. 37, e249. https://doi.org/10.3346/jkms.2022.37.e249 (2022).
Kwon, H. et al. Incidence of cardiovascular disease and mortality in underweight individuals. J. Cachexia Sarcopenia Muscle 12, 331–338. https://doi.org/10.1002/jcsm.12682 (2021).
Schoenfeld, D. Partial residuals for the proportional hazards regression model. Biometrika 69, 239–241 (1982).
Xue, S. et al. Age at attainment of peak bone mineral density and its associated factors: The National Health and Nutrition Examination Survey 2005–2014. Bone 131, 115163. https://doi.org/10.1016/j.bone.2019.115163 (2020).
Tanaka, S., Kuroda, T., Saito, M. & Shiraki, M. Overweight/obesity and underweight are both risk factors for osteoporotic fractures at different sites in Japanese postmenopausal women. Osteoporos. Int. 24, 69–76. https://doi.org/10.1007/s00198-012-2209-1 (2013).
Nevitt, M. C. et al. Risk factors for a first-incident radiographic vertebral fracture in women > or = 65 years of age: The study of osteoporotic fractures. J. Bone Miner. Res. 20, 131–140. https://doi.org/10.1359/JBMR.041003 (2005).
Sieber, C. C. Malnutrition and sarcopenia. Aging Clin. Exp. Res. 31, 793–798. https://doi.org/10.1007/s40520-019-01170-1 (2019).
Landi, F. et al. Sarcopenia as a risk factor for falls in elderly individuals: Results from the ilSIRENTE study. Clin. Nutr. 31, 652–658. https://doi.org/10.1016/j.clnu.2012.02.007 (2012).
Tokeshi, S. et al. Relationship between skeletal muscle mass, bone mineral density, and trabecular bone score in osteoporotic vertebral compression fractures. Asian Spine J. 15, 365–372. https://doi.org/10.31616/asj.2020.0045 (2021).
Schwartz, A. V. et al. Intensive glycemic control is not associated with fractures or falls in the ACCORD randomized trial. Diabetes Care 35, 1525–1531. https://doi.org/10.2337/dc11-2184 (2012).
Leanza, G. et al. Risk factors for fragility fractures in type 1 diabetes. Bone 125, 194–199. https://doi.org/10.1016/j.bone.2019.04.017 (2019).
Acknowledgements
We would like to thank Editage (www.editage.co.kr) for English language editing.
Funding
This work was Supported by Grant No. 09-2020-0008 from the SNUBH Research Fund.
Author information
Authors and Affiliations
Contributions
Conceptualization: S.M.P., J.P., K.H., J.Y.H. Data curation: K.H., J.Y.H. Formal analysis: K.H., J.Y.H. Funding acquisition: S.M.P. Investigation: S.M.P., J.P.. Methodology: S.H., H.D.J. Software: K.H., J.Y.H. Validation: H.J.K., J.S.Y. Visualization: S.M.P. Writing—original draft: S.M.P. Writing—review & editing: J.P., H.J.K., J.S.Y.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Park, SM., Park, J., Han, S. et al. Underweight and risk of fractures in adults over 40 years using the nationwide claims database. Sci Rep 13, 8013 (2023). https://doi.org/10.1038/s41598-023-34828-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-34828-y
- Springer Nature Limited
This article is cited by
-
Prevalence of osteoporosis and associated factors among people aged 50 years and older in the Madhesh province of Nepal: a community-based cross-sectional study
Journal of Health, Population and Nutrition (2024)
-
Effect of immunology biomarkers associated with hip fracture and fracture risk in older adults
Immunity & Ageing (2023)