
Abstract
This study aimed to compare the peri- and postoperative outcomes of patients treated with conventional versus robot-assisted laparoendoscopic single-site radical prostatectomy (C-LESS-RP vs. R-LESS-RP). Data of patients with prostate cancer (106 who underwent C-LESS-RP, 124 underwent R-LESS-RP) were retrospectively collected and analyzed. All operations were performed by the same surgeon from January 8, 2018, to January 6, 2021, in the same institution. Information on clinical characteristics and perioperative outcomes was obtained from records at the medical institution. Postoperative outcomes were acquired from follow-up. Intergroup differences were retrospectively analyzed and compared. All patients had similar clinical characteristics in meaningful aspects. The perioperative outcomes were better with R-LESS-RP than with C-LESS-RP in terms of operation time (120 min vs. 150 min, p < 0.05), estimated blood loss (17.68 ml vs. 33.68 ml, p < 0.05), and analgesic duration (0 days vs. 1 days, p < 0.05). The drainage tube duration and postoperative stay did not differ significantly between groups. However, R-LESS-RP was more expensive than C-LESS-RP (56559.510 CNY vs. 44818.27 CNY, p < 0.05). The patients who underwent R-LESS-RP had better urinary incontinence recovery and higher European quality of life visual analog scale scores than those who underwent C-LESS-RP. However, no significant intergroup difference was noted in biochemical recurrence. In conclusion, R-LESS-RP could achieve better perioperative outcomes, especially for those skilled surgeons who have mastered C-LESS-RP. Additionally, R-LESS-RP accelerated the recovery from urinary incontinence effectively and presented some benefits in health-related quality of life with additional costs.
Similar content being viewed by others


Introduction
Prostate cancer (PCa) is the fourth most common cancer worldwide accounting for approximately 1.4 million patients estimated to be diagnosed according to the GLOBOCAN 20201. Coincident with the widespread application of prostate specific antigen (PSA) testing, the incidence and early detection of preclinical PCa have increased2. In China, except for the broader utilization of diagnostic practices, a cumulatively westernized lifestyle and certain genetic polymorphism may collaboratively lead to the increase in the detection rate of PCa3,4. In the last 5 years, trends in incidence rates of PCa have remained stable in most Asian countries examined except an increasing trend observed in China5. Hence, although Chinese people are less affected by genetic inheritance than other races, the number of Chinese people diagnosed with PCa would continue to rise, especially in rural areas. Currently, the main treatments for PCa include radical prostatectomy, chemoradiotherapy and hormonal therapy, among which radical prostatectomy might serve as the only treatment strategy for treating the disease.
To date, laparoscopic radical prostatectomy has become the dominant treatment option for men with localized PCa. With the pursuit of minimally invasive treatment, many countries had a rapid adoption of conventional laparoendoscopic single-site radical prostatectomy (C-LESS-RP) or robot-assisted laparoendoscopic single-site radical prostatectomy (R-LESS-RP) such that the usage rate of robot assistance has increased to > 80% of all radical prostatectomies in the USA6. Although statistical data are lacking in China, increasing evident advantages have accelerated the rapid dissemination of R-LESS-RP in clinical practice.
Recently, several systematic reviews have suggested the superiority of robot-assisted radical prostatectomy (RARP) to open radical retropubic prostatectomy (ORP) in potency, urinary, positive surgical margin, biochemical recurrence (BCR), and complication rate7,8,9. By contrast, another study has reported that R-LESS-RP had similar outcomes in function to those of ORP and only provided benefits of a minimally invasive surgical approach to patients10.
The aforementioned studies mostly assessed and compared the benefits of RARP and ORP. However, few studies have compared the differences between RARP and laparoscopic radical prostatectomy (LRP), let alone the comparative study of C-LESS-RP and R-LESS-RP. A LAP-01 multicenter, patient-blinded, randomized controlled trial has demonstrated that the urinary incontinence recovery among patients with RARP was superior to patients with LRP after 3 months, although this difference diminished at the 12-month follow-up11. A prospective randomized trial has revealed significant differences in continence between patients who underwent RARP and those who underwent LRP 12 months postoperatively12. In total, 120 patients with PCa who received LRP demonstrated statistically significant differences 12 months postoperatively following RARP. However, the benefits of R-LESS-RP remain unclear despite having an increased surgery cost. For patients, the extra costs for R-LESS-RP might lead to their unwillingness to select such method. Meanwhile, because of the increased technical difficulty of R-LESS-RP, it failed to gain popularity among urologists. Moreover, whether this operating technique could achieve a high-level of evidence in perioperative and function outcomes was still unproven. Hence, we conducted a retrospective study to compare the differences in peri- and postoperative outcomes of patients with PCa treated with C-LESS-RP and R-LESS-RP.
Materials and methods
Patients
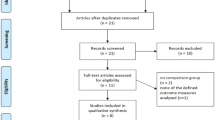
A consecutive cohort of PCa patients attending for surgery treatment was recruited thus limiting bias. Altogether, 230 patients who underwent single-site LRP performed by the same surgeon and pathologically diagnosed with PCa between January 8, 2018 and January 6, 2021 at Jiangsu Province Hospital of Chinese Medicine were enrolled in our study. The process, cost, risk, advantages, and disadvantages of the two surgical methods were discussed with the patients preoperatively. After detailed communication with patients, the surgical option for LESS-RP or R-LESS-RP was independently selected by each patient preoperatively. In total, 106 patients selected C-LESS-RP and 124 underwent R-LESS-RP with the Da Vinci IV robotic platform. Informed consent was obtained from all the participants. Data on sociodemographic and clinical characteristics including age, body mass index (BMI), PSA level, prostate volume, Gleason score, and the eighth edition American Joint Committee on Cancer tumor-nodes-metastasis (TNM) staging were retrieved from medical records. This study was approved by the Ethics Committee of the Affiliated Hospital of Nanjing University of Chinese Medicine (Institutional Ethics Committee ID: 2020NL-KS051). All procedures were conducted in accordance with relevant guidelines and regulations. The STROBE checklist of the study was presented in Table S1. The flow diagram for the study was shown in Fig. 1.

The flow chart of the study.
Perioperative outcomes measures
Perioperative data including operation time, estimated blood loss (EBL), analgesic duration, drainage tube duration, postoperative stay, and complications of all the patients were obtained from the institution’s health information system. The operation time referred to the duration of skin incision to skin suture. In R-LESS-RP, the operation time included the setup time. Considering that an analgesia pump is not routinely used in single-site surgery, the analgesic duration was defined as the number of days of postoperative use of analgesics which were mainly administered intravenously once a day. Additionally, information on total hospitalization costs of all the patients was also collected from the health information system.
Postoperative outcome measures
Postoperative outcomes including urinary incontinence and postoperative serum PSA levels and subsequent therapy were followed up regularly. Urinary incontinence recovery was evaluated according to the number of pads used daily, and those who used 0–1 pad daily were considered to have recovered from urinary incontinence13. Postoperative PSA levels were used to monitor for BCR, which was defined as postoperative PSA level of ≥ 0.2 ng/ml on two consecutive occasions during follow-up14. Additionally, a 5-level version of the European quality of life five-dimensional descriptive system (EQ-5D-5L) and EQ-VAS was used to evaluate whether the patients’ postoperative health-related quality of life after surgeries differed after the two surgical approaches15,16. EQ-5D-5L is an instrument comprising five dimensions (mobility, self-care, usual activities, pain or discomfort, and anxiety or depression). Each domain is divided into five levels of severity (none, slight, moderate, severe, extreme problems, or unable to). Patients were asked to rate their self-perceived health state from 0 (worst health) to 100 (best health) in the EQ-VAS14,17.
Statistical analyses
Data were analyzed using the SPSS 26.0 or R software (version 4.1.0). Group differences were assessed using t-test (normal distribution data) or Mann–Whitney test for continuous variables and χ2 or Fisher’s exact test for categorical variables at follow-up timepoints. BCR and urinary incontinence were estimated using Kaplan–Meier analysis and were compared using log-rank test. A two-sided p < 0.05 was considered statistically significant.
Results
Clinical characteristics
Altogether, 230 patients with PCa were enrolled in our study. After detailed communication with the patients, the surgical option was selected by the patients independently. On the principle of voluntary selection, 106 patients selected C-LESS-RP and 124 selected R-LESS-RP as their surgical modalities. As demonstrated in Table 1, the patients in the two groups had similar clinicopathologic data. At baseline, patient sociodemographic and clinical characteristics such as age, BMI, prostate volume, grade, and clinical stage were not significantly different between the two groups. However, the average preoperative PSA of patients who underwent C-LESS-RP was higher than those who underwent R-LESS-RP.
Perioperative outcomes
To compare the advantages and disadvantages of the two surgical methods, we mainly evaluated the perioperative data (Fig. 2 and Table 2). For operation time, the surgeon took longer time to complete C-LESS-RP than R-LESS-RP. The median operation time of R-LESS-RP was 120 ± 36.29 min, whereas that of C-LESS-RP was 150 ± 47.39 min (p < 0.01). It is worth mentioning that the average standby time for R-LESS-RP was 14.6 ± 3.2 min. Consistent with the operation time, a distinct difference of EBL during operations between two surgical approaches was identified (p < 0.01). The median EBL of R-LESS-RP was 17.68 ± 34.29 ml, whereas that of C-LESS-RP was 33.68 ± 38.81 ml. No patient required an intraoperative or postoperative blood transfusion in either group. Additionally, the analgesic duration of patients who underwent R-LESS-RP (0 ± 1.8 days) was apparently less than those of another surgical approach (1 ± 2.23 days, p = 0.033). Nevertheless, the drainage tube duration and postoperative stay did not significantly differ between the two surgical approaches. As predicted, total hospitalization costs were markedly different between the two surgical approaches. The median hospitalization cost of patients who underwent R-LESS-RP was 56,559.5 ± 14,991.99 CNY. Meanwhile, those who underwent C-LESS-RP spent a lower median cost of 44,818.27 ± 22,041.35 CNY (p < 0.01).

Comparison of perioperative outcomes between patients with the two different surgery approaches ((A) operation time; (B) blood loss; (C) analgesic duration; (D) drainage tube duration; (E) postoperative stay; (F) total hospitalization costs). According to t-test or Mann–Whitney test.
Additionally, postoperative complications were counted. As presented in Table 3, 16 patients experienced postoperative complications (seven who underwent C-LESS-RP versus nine who underwent R-LESS-RP). Five patients developed urinary fistula after C-LESS-RP, and six patients experienced the same situation with R-LESS-RP, although no significant intergroup difference was noted. One patient who underwent C-LESS-RP had a postoperative ileus that was treated using a second surgery. Two patients who underwent R-LESS-RP developed postoperative ileus; only one case was spontaneously resolved, and the other patient received a second surgery. One patient had urethral stenosis after R-LESS-RP. Besides, one patient in each group had chylous leakage. Most of the complications were minor, except for one case of postoperative ileus in each group.
Postoperative outcomes
Urinary incontinence recovery
Regardless of the type of operation received, the patients received the same postoperative care, and no additional rehabilitation training was performed. Anti-infection, pain relief, and other symptomatic treatment were provided postoperatively during hospitalization. Significant differences in duration to achieve urinary incontinence recovery following the operations were observed between the two surgical approaches. After excluding patients who were lost to follow-up, the data of 75 patients who underwent C-LESS-RP and 102 patients who underwent R-LESS-RP were retrospectively analyzed. None of the cases were severe that required surgery as a treatment method. The results suggested that the incontinence rate after R-LESS-RP was higher than that after C-LESS-RP. The patients who underwent R-LESS-RP significantly spent less time to achieve satisfactory urinary function (Fig. 3).

Difference in urinary incontinence recovery after operations with the two surgery approaches estimated with KM curves. According to the Kaplan–Meier methodology and compared using log-rank test.
Health-related quality of life
To access the postoperative health-related quality of life, EQ-5D-5L and EQ-VAS questionnaires were used to evaluate six aspects. The results of the EQ-5D-5L revealed no difference in the five aspects of mobility, self-care, usual activities, pain/discomfort, and anxiety/depression (Fig. 4A–E). The pain score did not differ between the two groups (p = 0.52). However, self-perceived health state was significantly better for patients following R-LESS-RP than for those who underwent C-LESS-RP (82.88 ± 11.58 vs. 78.84 ± 11.58, p = 0.014; Fig. 4F).

Comparison of postoperative health-related quality of life in patients with R-LESS-RP to those underwent C-LESS-RP ((A) mobility; (B) self-care; (C) usual activity; (D) pain; (E) anxiety; (F) self-perceived health state). According to t-test or Mann–Whitney test.
Biochemical recurrence
Altogether, 204 patients were followed up to assess the effect of different surgery methods on BCR (92 underwent LESS-RP, 112 underwent R-LESS-RP). The data were composited PSA results of patients’ report during follow-up and records from medical situation. However, it revealed no evidence of interaction between surgical approaches and BCR after surgery (Fig. 5).

BCR survival of PCa patients according to the different surgery approaches. BCR biochemical recurrence. According to the Kaplan–Meier methodology and compared using log-rank test.
Discussion
Robot-assisted technology could facilitate the accomplishment of some important surgical steps of the procedure18. Since Binder has reported the first RARP in 2001, offering technical innovations including three-dimensional visualization, articulated instruments, and tremor filtration, it has immediately become popular among urologists19. The Da Vinci Xi surgical system released in 2014 has smaller and lighter operating arms, and the suspended mobile platform can allow adjusting the operating direction freely, thereby expanding the operative field exposure. Robotic surgery has gained increasing attention because of its advantages of clearer vision, more flexible operation angle, and more precise exposure anatomy. Surgeons advocating single-site surgery may prefer the Da Vinci single-port robotic system because of the principle of anterior pelvic support preservation and its touted early continence recovery20. However, whether the extra cost is worth it remains controversial.
This retrospective comparative analysis demonstrated the feasibility and preponderance of R-LESS-RP using the Da Vinci Xi system. The EBL and operation time were important for assessing a new surgical technique. The median operation time of R-LESS-RP was only 120 min (vs. 150 min for C-LESS-RP, p < 0.05). Slightly different from that of the previous study21, the EBL was less in the R-LESS-RP procedure than in the other prostatectomy procedure (17.68 ml vs. 33.68 ml, p < 0.05). As the EBL might be positively associated with the operation time, the surgeon could complete the surgery more quickly with less blood loss. The stabilizer of the Da Vinci system also helped to complete the surgeries more quickly with less blood loss. Moreover, as R-LESS-RP is minimally invasive, this could be the reason for the shorter analgesic duration (0 days vs. 1 days, p < 0.05) associated with it. The shorter analgesic duration might help with faster postoperative recovery. Otherwise, the results revealed that robot-assisted surgery did not reduce or increase the incidence of complications. The drainage tube duration and postoperative stay were not significantly different between the two surgical approaches. As expected, the hospitalization cost of patients who underwent R-LESS-RP was more expensive than that of the patients who underwent C-LESS-RP (44,818.27 CNY vs. 56,559.51 CNY, p < 0.05). Nevertheless, the difference in the cost was smaller than expected.
After prostatectomy, urinary incontinence recovery is one of a patient’s major concerns regardless of the type of surgical procedure performed. Because of the facilitated frozen section analysis, R-LESS-RP was considered a better approach for sparing the neurovascular bundle. Neurovascular bundle preservation was performed depending on the individual surgeon’s discretion based on clinical staging. A mature laparoscopic radical prostatectomy series revealed that the 12-month urinary continence recovery was 66–95%22. Another study has reported that the prevalence of urinary incontinence after RARP was 4–31%23. According to the statistical data of our institution, the 12-month continence rate after R-LESS-RP was higher than that after C-LESS-RP (74% vs. 50%, Table 4). A significant difference in urinary incontinent recovery was identified between both groups. The time of urinary incontinence recovery of patients who underwent R-LESS-RP was faster than that of patients who underwent C-LESS-RP. The traditional single-site laparoscopic surgery often lacks the “triangle” relationship of surgical operation, special instruments need to be used during the operation, and the operation space is relatively limited. The mutual interference between the lens and other instruments greatly increases the difficulty of the operation. The learning curve of the surgeon is long, especially in the aspects of exposure and suture. The advantages of the robot-assisted surgery system are reflected in its “wrist” device significantly expanding the scope of surgery, and its unique motion scaling and vibration control that effectively improves the flexibility and accuracy of surgery.
The data of neurovascular bundle tissue sparing on histology were lacking in both groups in this study. However, the preoperative PSA of the patients who underwent C-LESS-RP was higher, which might affect neurovascular bundle tissue sparing and urinary incontinence recovery. Furthermore, although erectile function is also a postoperative concern for patients, we did not analyze such data. As erectile function can continue to improve for up to 3 years postoperatively24, any difference in outcomes between these surgical techniques might not become apparent for some time.
According to the outcomes assessed using the self-reported EQ-5D-5L questionnaire, the EQ-VAS score was certainly connected with different surgical approaches (82.88 for patients who underwent R-LESS-RP vs. 78.84 for patients who underwent C-LESS-RP). Such outcomes might also be related to self-psychological status, urinary continence recovery, and advances in oncology which require further analysis. Different surgical approaches did not improve the patients’ health-related quality of life (mobility, self-care, usual activities, pain or discomfort, anxiety, or depression) postoperatively.
A previous study has demonstrated the lack of high quality evidence to support superiority of oncological outcomes, not only prostate cancer-specific survival in particular, but also biochemical and recurrence-free survival25. Similarly, we did not observe any short-term intergroup difference in biochemical recurrence. The dropout ratio of urinary incontinence recovery data for the patients who underwent C-LESS-RP was higher than for those who underwent R-LESS-RP (p = 0.039). For biochemical recurrence, no significant intergroup difference in dropout ratio was observed (p = 0.4). For each patient enrolled in our study, we all similarly followed the postoperative outcomes regardless of the specific surgery received by the patient. However, the patients who underwent R-LESS-RP were more likely to pay attention to their recovery status and share their information. Some patients also provided equivocal information that was excluded in our study. Some patients also changed or provided wrong contact information. For biochemical recurrence data, we definitely identified the PSA value from the patients from our hospital or presentation from local hospital for some patients. These might explain the differences in the dropout ratio between the two clinical outcomes. Although a slightly better trend was observed, further long-term clinical research is necessary.
Previously, the LAP-01 trial conducted by researchers from the University of Leipzig and other institutions in Germany proved that RARP was superior to the traditional LRP in terms of improving urinary continence after 3 months11. It is generally believed that patients who underwent RARP can continue to recover after 3 months, especially in terms of urinary continence. Therefore, functional and oncological data for 12 months are crucial for comparing the results of different surgical methods. In the former trial, further comparison on the urinary continence and oncology results between RARP and LRP during the 12-month follow-up indicated no significant difference. Similar to our outcomes, the postoperative recovery of urine continence in the short term was faster among patients after robot-assisted surgery. However, more differences between the two surgical methods were noted, which may be due to the high difficulty of traditional single-site laparoscopic surgery. Moreover, the application of robot-assisted technology can greatly reduce the difficulty of operation.
It is important to emphasize that all the operations were performed by the same surgeon who has engaged in urological single-port surgery for 10 years. As a surgeon who had mastered C-LESS-RP, robot-assisted technology could contribute to reserve energy and simultaneously achieve better perioperative outcomes.
In all the cases, R-LESS-RP demonstrated evident advantages of perioperative outcomes for patients with PCa and was conducive for recovery from urinary incontinence postoperatively. With the development of technology and economy, more patients would be willing to select robotic surgery.
Limitation
One limitation of this study is selection and treatment bias. The treatment method is mainly determined by the patient, and the different economic status among patients may have influenced postoperative recovery. Another limitation was that only one surgeon performed the surgeries as the study was conducted in a single institution study. Thus, these results might not be generalized to other settings. A prospective randomized trial with a larger sample size for repeated validation is required in the future.
Conclusions
R-LESS-RP had the following perioperative advantages: shorter operation time, less blood loss, and shorter analgesic duration. The recovery of urinary incontinence was significantly faster for patients who underwent R-LESS-RP than for those who underwent C-LESS-RP. The relatively extra cost remained a barrier to the popularity of R-LESS-RP which could be solved gradually.
Data availability
All data generated or analyzed during this study are included in this published article.
References:
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71(3), 209–249 (2021).
Rawla, P. Epidemiology of prostate cancer. World J. Oncol. 10(2), 63–89 (2019).
Chen, W. et al. Cancer statistics in China, 2015. CA Cancer J. Clin. 66(2), 115–132 (2016).
Wong, M. C. et al. Global incidence and mortality for prostate cancer: Analysis of temporal patterns and trends in 36 countries. Eur. Urol. 70(5), 862–874 (2016).
Culp, M. B., Soerjomataram, I., Efstathiou, J. A., Bray, F. & Jemal, A. Recent global patterns in prostate cancer incidence and mortality rates. Eur. Urol. 77(1), 38–52 (2020).
Oberlin, D. T., Flum, A. S., Lai, J. D. & Meeks, J. J. The effect of minimally invasive prostatectomy on practice patterns of American urologists. Urol. Oncol. 34(6), 255e1-5 (2016).
Sooriakumaran, P. et al. Erectile function and oncologic outcomes following open retropubic and robot-assisted radical prostatectomy: Results from the LAParoscopic prostatectomy robot open trial. Eur. Urol. 73(4), 618–627 (2018).
Tewari, A., Srivasatava, A., Menon, M., Members of the, V. I. P. T. A prospective comparison of radical retropubic and robot-assisted prostatectomy: experience in one institution. BJU Int. 92(3), 205–210 (2003).
Hu, J. C. et al. Perioperative complications of laparoscopic and robotic assisted laparoscopic radical prostatectomy. J. Urol. 175(2), 541–6 (2006).
Yaxley, J. W. et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: Early outcomes from a randomised controlled phase 3 study. Lancet 388(10049), 1057–1066 (2016).
Stolzenburg, J. U. et al. Robotic-assisted versus laparoscopic radical prostatectomy: 12-month outcomes of the multicentre randomised controlled LAP-01 trial. Eur. Urol. Focus 8(6), 1583–1590 (2022).
Porpiglia, F. et al. Randomised controlled trial comparing laparoscopic and robot-assisted radical prostatectomy. Eur. Urol. 63(4), 606–614 (2013).
Sandhu, J. S. et al. Incontinence after prostate treatment: AUA/SUFU guideline. J. Urol. 202(2), 369–378 (2019).
Tan, N. et al. Pathological and 3 tesla volumetric magnetic resonance imaging predictors of biochemical recurrence after robotic assisted radical prostatectomy: Correlation with whole mount histopathology. J. Urol. 199(5), 1218–1223 (2018).
van Hout, B. et al. Interim scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health 15(5), 708–715 (2012).
Murasawa, H. et al. Health utility and health-related quality of life of Japanese prostate cancer patients according to progression status measured using EQ-5D-5L and FACT-P. Qual. Life Res. 28(9), 2383–2391 (2019).
Sanders, G. D. et al. Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: Second panel on cost-effectiveness in health and medicine. JAMA 316(10), 1093–1103 (2016).
Checcucci, E. et al. Retzius-sparing robot-assisted radical prostatectomy vs. the standard approach: A systematic review and analysis of comparative outcomes. BJU Int. 125(1), 8–16 (2020).
Binder, J. & Kramer, W. Robotically-assisted laparoscopic radical prostatectomy. BJU Int. 87(4), 408–410 (2001).
Dalela, D. et al. A pragmatic randomized controlled trial examining the impact of the Retzius-sparing approach on early urinary continence recovery after robot-assisted radical prostatectomy. Eur. Urol. 72(5), 677–685 (2017).
Yilmazel, F. K. et al. Comparison of perioperative, oncological, and functional outcomes of three-dimensional versus robot-assisted laparoscopic radical prostatectomy: A preliminary study. J. Laparoendosc. Adv. Surg. Tech. A 32(3), 304–309 (2021).
Ficarra, V. et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: A systematic review and cumulative analysis of comparative studies. Eur. Urol. 55(5), 1037–1063 (2009).
Ficarra, V. et al. Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy. Eur. Urol. 62(3), 405–417 (2012).
Isgoren, A. E., Saitz, T. R. & Serefoglu, E. C. Erectile function outcomes after robot-assisted radical prostatectomy: Is it superior to open retropubic or laparoscopic approach?. Sex Med. Rev. 2(1), 10–23 (2014).
Ilic, D. et al. Laparoscopic and robotic-assisted versus open radical prostatectomy for the treatment of localised prostate cancer. Cochrane Database Syst. Rev. 9, CD009625 (2017).
Acknowledgements
This work was supported by the National Natural Science Foundation of China [Grant number: 81772732; 81702364] and the Natural Science Foundation of Jiangsu Province [Grant number: BK20171085].
Author information
Authors and Affiliations
Contributions
Y.W.: project development, data collection, manuscript writing. Q.J.: data management, manuscript writing. X.Z.: project development, manuscript revising. L.S., X.W., C.Z. and J.S.: manuscript revising. Q.Z.: project administration, manuscript writing and revising.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wei, Y., Ji, Q., Zhou, X. et al. R-LESS-RP versus C-LESS-RP: a single-institution retrospective comparative study. Sci Rep 13, 3844 (2023). https://doi.org/10.1038/s41598-023-31021-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-31021-z
- Springer Nature Limited