
Abstract
Knowledge about modifiable determinants of daily physical activity (PA) in patients with chronic obstructive pulmonary disease (COPD) is crucial to design effective PA interventions. The present study aimed to determine the contribution of quadriceps strength, power and endurance to daily PA in COPD. Additionally, for quadriceps endurance, we also aimed to determine to what extent the association varies according to the mode of movement (isotonic, isometric, or isokinetic). Using a multicentre cross-sectional trial design we determined the contribution of quadriceps function to daily PA (steps, sedentary time and time spent doing moderate-to-very-vigorous physical activity [MVPA]) using bivariate and partial Pearson correlation analysis (r) and multiple linear regression models (ΔR2). Pre-determined controlling factors were sex, age, body mass index (BMI), COPD-assessment test, forced expiratory volume in one second in percent of the predicted value (FEV1pred), and distance walked on the 6-minute walk test. Eighty-one patients with COPD (mean ± SD: age 67 ± 8 years, FEV1pred 57 ± 19%, daily steps 4968 ± 3319, daily sedentary time 1016 ± 305 min, and MVPA time 83 ± 45 min) were included. Small to moderate bivariate correlations (r = .225 to .452, p < .05) were found between quadriceps function and measures of PA. The best multiple linear regression models explained 38–49% of the variance in the data. Isotonic endurance was the only muscle contributor that improved all PA models; daily steps (ΔR2 = .04 [relative improvement 13%] p = .026), daily sedentary time (ΔR2 = .07 [23%], p = .005) and MVPA-minutes (ΔR2 = .08 [20%], p = .001). Isotonic endurance was also independently associated with most PA variables, even when controlling for strength, power or isometric-isokinetic endurance properties of the muscle (r = .246 to .384, p < .05). In contrast, neither strength, power, isometric-or isokinetic endurance properties of the muscle was independently associated with PA measures when controlling for isotonic endurance (r = .037 to .219, p > .05). To conclude, strength, power, and endurance properties of the quadriceps were low to moderately associated with PA in patients with COPD. Isotonic quadriceps endurance was the only quadriceps property that was independently associated with the different measures of PA after controlling for a basic set of known determinants of PA, quadriceps strength or power, or isometric or isokinetic quadriceps endurance. Future longitudinal studies should investigate its potential as a modifiable determinant of PA.
Similar content being viewed by others

Introduction
Physical activity (PA) is recognized as an essential feature in patients with chronic obstructive pulmonary disease (COPD)1, being amongst the strongest predictors of all-cause mortality and quality of life in the disease2,3,4,5. Importantly, PA levels can potentially be improved1, and over recent years, several modifiable determinants of PA in COPD have been identified3. Even so, there is still limited and inconsistent evidence on the effectiveness of interventions to enhance PA in COPD1. Considering that knowledge about determinants of PA in patients with COPD is crucial to design effective PA interventions3,6, these findings highlighting that other modifiable determinants of PA likely exists, even though they have yet to be identified1,3.
Quadriceps dysfunction, defined by reduced strength, power or endurance properties of the quadriceps is a common extrapulmonary manifestation of the disease, evident in over a third of the COPD-population7,8. Even though improving quadriceps function often is an integrated aim of exercise interventions1,7,9,10,11, information on the potential role of quadriceps function as a determinant of PA in COPD is sparse.
Other than quadriceps strength, shown not to be linked to PA in several different studies12,13,14, there is today limited knowledge on the impact of other potentially modifiable properties of the quadriceps on PA in COPD. Recently, quadriceps power has emerged as a more important predictor of PA than quadriceps strength, being positively associated with active time per day as well as light intensity PA in COPD13. However, to our knowledge, the role of quadriceps power to PA has only been investigated in this single study in which the sample size was small, and the study included only older men, highlighting a need for further investigation13.
Another potentially modifiable determinant of PA is quadriceps endurance. The endurance capacity of the quadriceps may be of particular interest to PA, considering that the muscle's ability to repeat a specific task over time15 indicates a similarity in PA task requirements based on the repetitive nature of quadriceps use in everyday daily activities such as walking. For example, quadriceps endurance has previously been found to be independently associated with walking distance on the 6-minute walk test (6MWT) even after controlling for quadriceps strength16. Considering the existing link between 6MWT and PA in COPD3,17, these findings indicate that quadriceps endurance could also be more closely associated with PA than other aspects of quadriceps function.
The primary aim of the present study was, therefore, to determine and to compare the contribution of quadriceps strength, power and endurance to PA in patients with COPD. Furthermore, in recent studies, static (isometric) and dynamic (isotonic, isokinetic) endurance protocols have been found to reflect different aspects of quadriceps function in COPD16,18. Thus, a secondary objective was to determine to what extent the association varies according to the mode of movement (isotonic, isometric, isokinetic). Amongst the quadriceps muscle properties examined, the main hypothesis was that quadriceps muscle endurance would show the strongest association and contribution to the physical activity measures.
Method
Study design and participants
The present study was a multicentre cross-sectional study conducted in Sweden, Canada, and the Netherlands. Participants in this prospective study were continuously enrolled with convince sampling at each centre. Participants were included in every month of the year, thereby covering all seasons. Inclusion criteria were at least 40 years of age, and a confirmed diagnosis of mild to very severe COPD according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria19 controlled through medical records. Exclusion criteria’s consisted of recent COPD exacerbation (within 3 months), muscular-, rheumatic-, or cardiac disorders affecting testing procedures, and a daily dose of prednisone >10mg within 3 months, also controlled through medical records, and self-reported regular quadriceps strengthening exercises.
Procedure
All participants attended two visits, and PA was measured for seven days, from 2016 to 2019. On the first visit were anthropometrics including body mass index (BMI), and symptoms on the COPD assessment test (CAT) collected. After that were a 6MWT20, spirometry21, and an isometric quadriceps strength test performed. The second visit included the assessment of isokinetic quadriceps power as well as isometric, isokinetic and isotonic quadriceps endurance22 (Fig. 1).

Description of study procedure. CAT COPD assessment test, MRC Medical Research Council dyspnea scale, 6MWT 6-minute walking test, MVPA time spent in moderate to very vigorous intensity. *Randomized order, POWER, was obtained from the isokinetic protocol.
Quadriceps function
Quadriceps strength, power and endurance were measured with a computerized dynamometer (Biodex System Pro 3 or 4 Biodex Medical Systems, Shirley, New York, NY, USA) using test procedures that have been described in detail elsewhere22. Quadriceps strength was measured during a maximal voluntary contraction (MVC) using an isometric (static) protocol at a 90° knee angle22, performed in line with international recommendations and reported in Newton-meters (Nm)7. Quadriceps power, equivalent to energy output per unit of time, was obtained from the average power developed during 30 maximal isokinetic contractions; results were expressed in watt23,24.
Quadriceps endurance was assessed with three reliable protocols22, all performed with similar (1) starting position (sitting, 90° knee angle, straps over the thigh and pelvis), (2) direction of movement (restricted by the lever arm), and (3) duration of the test (~ 60 s). The three protocols differed regarding the mode of contraction/movement (isometric [static], isokinetic [dynamic, fixed speed], or isotonic [dynamic, fixed external loading]). The two dynamic protocols had identical range-of-motion (90° knee flexion to full individual knee extension − 5°), while the static protocol was performed at a 90° knee angle22. Standardized verbal encouragements were given in all tests.
The isometric protocol consisted of a static contraction at 60% of MVC at 90° knee angle using visual feedback (results: total work (load [Nm] × seconds until momentary failure)22. The isokinetic endurance protocol consisted of 30 maximal dynamic contractions at a fixed pace of 90°/s (results: total work in Joule [J])22. The isotonic endurance test protocol consisted of the maximal amount of dynamic leg extensions throughout the full range of motion, performed using a resistance of 30% of isometric MVC maintaining an externally set pace by a metronome at 60 beats per minute (i.e., 30 repetitions/minute) (results: total work (load [Nm] × repetitions)22.
PA
A tri-axial accelerometer (DynaPort MoveMonitor, McRoberts; Hague, the Netherlands) was used to measure PA. The accelerometer is considered valid for patients with COPD25 and is a small, light ambulant measurement device (106.6 x 58 x 11.5 mm, 55 g) worn with an elastic belt on the lower back. Since the sensors measure gravity (g) in static situations, the acceleration signal is expressed relative to g. The participants were instructed to wear the accelerometer for seven consecutive days, including a weekend day. The minimum wearing criteria was ≥ 4 days, with ≥ 8 h wearing time each day26,27. Daily steps, daily sedentary time in minutes, and daily time spent in moderate to very vigorous activity (MVPA) were selected as these are the three most commonly used measures of PA in COPD intervention studies1 and were considered to display different aspects of PA. PA measures were summarized for valid days by the manufacturer software. Thresholds for describing time spent at different intensity levels were; sedentary time < 1.5 metabolic equivalents (METs), and time spent in moderate to very vigorous activity ≥ 3 METs, as proposed by the American College of Sports Medicine28. To define each individual’s average value during the physical activity measurement was the median from valid days used in the main analysis. To compare levels of PA between week- and weekend days, the individual’s median value during the valid week and weekend days was used.
Statistical analysis
A statistical software package was used for all calculations (Jamovi, version 1.6.7, Sydney, Australia), a p value of < .05 was considered to indicate statistical significance. Contribution of quadriceps function to PA (daily steps, daily sedentary time, and daily MVPA-minutes) was determined through Pearson’s bivariate and partial correlations, and multiple linear regression analyses. Levels of PA between week- and weekend was compared using paired t-tests and Pearson’s bivariate correlations. For bivariate analysis were correlation coefficients (r) values in the range of < .1 considered trivial, .1–.3 small, .3–.5 moderate, .5–.7 large, .7–.9 very large, and > .9 extremely large29. Partial correlations analyses were used to examine the correlation between PA and one quadriceps property while controlling for another quadriceps property (e.g., the correlation between MVPA-minutes and quadriceps endurance while controlling for quadriceps strength). In the multiple linear regression analysis, daily steps, daily sedentary time, and daily MVPA-minutes represented dependant variables. Based on previous literature3,13 and basic clinical characteristics7 were sex, age in years, BMI, CAT score, FEV1pred and 6MWT in meters selected as pre-determined independent variables and constituted the basic model30,31. A minimum of 75 participants was aimed to be included based on the general rule that 10 to 15 subjects per predictor are needed for a reliable equation32. To determine the contribution of various quadriceps properties to PA in COPD, isometric strength, isokinetic power, as well as isotonic, isometric and isokinetic quadriceps endurance measurements were entered independently to the basic model. The models were then again applied to the three dependent PA variables. Outcomes to evaluate the contribution to PA included the standardized estimated effect of included variables, the predicting ability of the model using R2, and absolute change (ΔR2) between the first and second models. Multicollinearity was evaluated with the tolerance and variance inflation factor (VIF) statistics with tolerance value > .1 and VIF < 10. The quality of the linear regression models was assessed using the Akaike information criterion (AIC) (lower score, better model)33.
Ethics approval and consent to participate
The study was conducted in accordance with the declaration of Helsinki and was approved by the respective local ethical boards (regional medical ethics committee of Umeå: DNR: 2015-426-31M, 2016-379-32M; Comité éthique du Centre de Recherche, Institut Universitaire de Cardiologie et de Pneumologie de Québec, Université Laval: CER: 21322; Committee on Research Involving Human Subjects (CMO) region Arnhem-Nijmegen: CMO: NL59926.091.16), all participants received written and verbal information about the study and gave their written informed consent before the study commenced.
Results
Eighty-one participants with COPD were included in the analysis, 4 participants were excluded from the analysis, either missing a valid isometric quadriceps muscle endurance measurement (n = 3) or isotonic quadriceps muscle endurance measurement (n = 1). The PA measurement covered both weekdays and weekends for all participants. Eighty participants had at least one valid weekend day. Table 1 display participant characteristics, PA measures, and quadriceps functions, Table 2 displays bivariate and partial correlation coefficients, Table 3 displays the R2, and ΔR2 of each multiple linear regression model, while Table 4 displays the standardized estimated effect of the models with the best coefficient of determination for daily steps, sedentary time, and MVPA-minutes. No multicollinearity was observed in the multiple analyses.
Pearson’s correlation and multiple linear regression analyses
Small to moderate significant correlations (r = .219 to .452) were found between different quadriceps function properties and all PA measures. Partial correlation analyses on strength, power and endurance properties of the quadriceps revealed that isotonic quadriceps endurance was independently associated with all PA measures after controlling for quadriceps strength as well as independently associated with sedentary time and MVPA-minutes but not daily steps (r = .201, p = .07) when controlling for quadriceps power. In contrast, neither strength nor quadriceps power was independently associated with PA measures when controlling for isotonic endurance. Similarly, other than daily steps when controlling for isokinetic endurance (r = .200, p = .08), isotonic quadriceps endurance was also independently associated with PA measures when controlling for isometric and isokinetic endurance. At the same time, no significant associations were seen between PA measures and isometric and isokinetic endurance when controlling for isotonic endurance (Table 2).
The basic multiple linear regression model, including the pre-determined variables sex, age in years, BMI, CAT score, FEV1pred and distance walked on the 6MWT explained 31–41% of the variance in the PA data (R2: daily steps .37, daily sedentary time .31 and MVPA-minutes .41). Isotonic quadriceps endurance was included in the best model to additionally explain variability of daily steps (ΔR2 = .04 [relative improvement of the model = 13%] p = .026), daily sedentary time (ΔR2 = .07 [23%], p = .005) and MVPA-minutes (ΔR2 = .08 [20%], p = .001), resulting in 38–49% of the variance in PA being explained (Tables 3 and 4). Quadriceps strength or power did not improve any model while isometric endurance improved the MVPA model (ΔR2 = .06 [10%], p = .006). The MVPA model also improved by isokinetic endurance (ΔR2 = .03 [8%], p = .048) (Table 3).
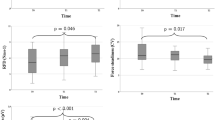
Group means of the individual’s average value using medians for valid week- and weekend days separately show higher daily steps and daily MVPA-minutes during weekdays than during weekends (mean ± standard deviation: weekday daily steps 5162 ± 3498 vs. weekend daily steps 4685 ± 3203, p = .029, weekday MVPA-minutes 86.6 ± 48.5 vs. weekend MVPA-minutes 80.8 ± 45.0, p = .040), sedentary time was not different (weekday sedentary minutes 1014 ± 300 vs. weekend sedentary minutes 1015 ± 302, p = .993). The correlations between weekday and weekend PA were very large (r = .84–.87, p < .001).
Discussion
The main findings of the present study are that strength, power and endurance properties of the quadriceps are significantly associated with PA in patients with COPD. Of the included measures of quadriceps function, quadriceps endurance was the only muscle property that was associated with daily steps, daily sedentary time and MVPA-minutes even after controlling for a basic set of known determinants of PA or when controlling for strength-power properties of the muscle. Our result also indicate that the mode of movement is of importance as isotonic quadriceps endurance was independently associated with PA in COPD even when controlling for isometric or isokinetic quadriceps endurance. In contrast, neither strength, power nor isometric and isokinetic endurance properties were independently associated with PA measures, when controlling for isotonic endurance.
Interpretation of study results
Quadriceps strength was associated with all PA measures, however, when added to a basic set of known determinants of PA (sex, age, BMI, FEV1pred, CAT, 6MWT) quadriceps strength was not a significant contributor to any of the models. These findings are in line with previous research12,13,34. However, considering the known link between BMI and quadriceps strength in COPD35, it should be noted that the lack of added predictive value of quadriceps strength to the basic set of variables, may, at least partly, be explained by that BMI was one of the basic variables. Furthermore, quadriceps power was recently found to be positively associated with light intensity PA, and active time per day (r = .37 to .51), but not daily steps in older men with COPD (r = .30, p > .05)13. In the present study, active time per day and light intensity PA was not explicitly investigated but isokinetic quadriceps power was associated with all included aspects of PA, even daily steps (r = .313, p < .01). About the latter, considering the similarity in the coefficient of correlation in the present study (r = .313) and in the study of Hernandez et al. (r = .300), the lack of statistical significance in the latter study was likely due to the lower sample size (n = 44 vs. n = 81)13. Nevertheless, even though quadriceps power has been highlighted as a more important predictor of PA than maximum strength13, the results from the present study indicate that it does not seem to add additional value when added to already known determinants of PA in COPD, or when compared to the endurance capacity of the quadriceps. It should be noted that the recognised link between isokinetic power and distance walked on the 6MWT18 likely contributed to why the basic models were not further improved by isokinetic power. However, in contrast, the endurance capacity of the quadriceps improved PA models when added to the basic models despite the known link to distance walked on the 6MWT16,36. Our observed findings are further supported by the results from the partial correlation analysis in which neither quadriceps strength nor power was independently associated with PA when controlling for isotonic quadriceps endurance. In contrast, isotonic quadriceps endurance was, except for steps per day when controlling for quadriceps power, independently associated with daily steps, sedentary time and MVPA-minutes even after controlling for strength and power properties of the quadriceps. Similarly, isotonic quadriceps endurance was independently associated with most PA measures even after controlling for isometric or isokinetic quadriceps endurance measurements.
Clinical relevance
As previously reported, FEV1pred, BMI, and distance walked on the 6MWT were significant contributors to the best models to determine PA. In fact, the distance walked on the 6MWT is consistently found associated with measures of PA in COPD, and often considered one of the best available determinants of PA in COPD3. The findings from the present study demonstrate that strength, power and endurance properties of the quadriceps are also low to moderately associated with PA in patients with COPD. Isotonic quadriceps endurance was the only significant muscle contributor to all PA models, resulting in an absolute improvement of the basic models with 4 to 8% (relative improvement 13 to 23%). Isotonic quadriceps endurance was also independently associated with PA in COPD even after controlling for strength/power or other modes (isometric/isokinetic). In contrast, neither strength/power nor other modes of quadriceps endurance was associated with any of the included PA measures when controlling for isotonic endurance. A possible explanation for these findings is that isotonic endurance measurements, in a similar way as many daily physical activities, e.g., going for a brief daily walk, consists of dynamic submaximal movements/contractions. In contrast, isometric measurements are static (i.e., no movement) while isokinetic power and endurance measurements consist of maximal, and not submaximal contractions8,22,23,24.
The relevance of the association of isotonic quadriceps endurance when estimating PA can be extrapolated to a clinical example. Based on the predictive models, an improvement of roughly 37% in isotonic quadriceps endurance would be needed to achieve a clinically relevant 600-daily step improvement in PA37, if all other factors remain constant. For the 6MWT, the corresponding change for a similar improvement in isotonic quadriceps endurance based on our data would be 63 m. Even though these estimations should be interpreted cautiously due to the cross-sectional nature of the data which prevent concluding on cause and effect, other research groups have found that trials with significant improvement in PA have also demonstrated considerable improvements in distance walked on the 6MWT (47 to 79 m)38,39,40. One of the studies also reports improvements of isometric quadriceps endurance of ~ 35% and isometric quadriceps strength of ~ 14% after an intervention with high-intensity interval training on stationary bicycles with significant improvements in several PA measures40. To our knowledge, isotonic quadriceps endurance has not been evaluated in trials that have demonstrated significant improvements in PA. Still, isotonic quadriceps endurance is repeatedly shown to be highly adaptable (+ 50 to 97%) by exercise interventions11,41,42.
Taken together with the observation that isotonic endurance also was independently associated with most PA measures even when controlling for strength, power, or isometric- and isokinetic endurance properties of the quadriceps, our results indicate that isotonic quadriceps endurance seems to be more closely associated with PA than other aspects of quadriceps function. Nevertheless, and as further described in the strengths and limitations of the study, only about half or less of the variation in PA is explained in our models, despite including a wide range of known determinants of PA among patients with COPD, and bivariate and partial correlations mainly demonstrated low to moderate associations for quadriceps muscle properties and PA in COPD.
Strengths and limitations
The international multicentre design with continuous data collection, the broad spectrum of disease severity and the direct comparison of several different aspects of quadriceps function are key strengths of the current study, increasing generalizability and facilitating the interpretation of the role of quadriceps function to PA in COPD. However, in line with the findings from the present study, it should be noted that strength, power and endurance properties of the quadriceps could be measured in various ways8,43,44,45. Thus, we cannot be certain that the results would have been similar if other strategies were also used. Nevertheless, isometric MVC was chosen as a measure of quadriceps strength since it, to date, is the recommended approach to assess quadriceps strength in COPD7. For quadriceps power, no such specific assessment recommendation exist44. However, other strategies such as the stair climb power test46, sit to stand47 or isotonic measures of power24 exist and may have provided other information, even though this needs to be further investigated. Furthermore, even though several different PA measures exist1,3, daily steps, sedentary time and MVPA-minutes were selected as these are the three most commonly used outcomes of PA in intervention studies targeting PA in COPD1. Steps and MVPA-minutes were lower during the weekend than during weekdays (− 476 steps/day and − 5.8 MVPA-minutes), but with very large correlations, as shown previously in COPD48. Inclusion of both week and weekend days resulted in more valid days in the main analysis, and the associations, therefore, reflect an average of valid days and not any specific part of the week. Lastly, an important notion is that only about half or less of the variation in PA is explained in our models, despite including known determinants of PA among patients with COPD3. The explanatory degree in the present study may have been further improved by the inclusion of more known factors than those selected3,49,50.
Firstly, have limitations in chest wall volume measurements, and central hemodynamic and peripheral muscle oxygenation been investigated and show that quadriceps muscle oxygen saturation and inspiratory reserve chest wall volume as the significant best contributors, explaining 77.7% of the variance in daily movement intensity49,50. However, movement intensity was not used as a dependent variable in this study, and movement intensity and movement amount (steps and time in activity) might reflect different aspects of PA6,48.
Secondly, in combination with the notion that included participants, even though representative in all GOLD stages, had a relatively well-preserved functional exercise capacity (only 22% walked < 350 m on the 6MWT). Factors other than pure physiological factors, such as motivation, social participation, meaningful interpersonal interactions, readiness to change and self-efficacy may have provided additional value and should be considered in future studies1,51. And thirdly, testing also other muscle groups, such as the calf-muscles, could also provide additional value considering the know link between the calf-muscles and walking ability in COPD52. Nevertheless, we do believe that this basic set of factors was sufficient for the present study's aim, that is, to determine and compare the association between different aspects of quadriceps function and PA in COPD.
Conclusion
In conclusion, this study found that strength, power and endurance properties of the quadriceps were low to moderately associated with PA in patients with COPD, but that isotonic quadriceps endurance was the best, and the only quadriceps property that was associated with all the different measures of PA (daily steps, daily sedentary time and MVPA-minutes) even after controlling for a basic set of known determinants of PA or when controlling for strength or power properties of the muscle. Thus, altogether these findings highlight that the endurance capacity of the quadriceps seems to be a new potentially modifiable determinant of PA in COPD that may be considered if the goal is to optimize the role of exercise training as a mean to improve PA in COPD, even though this needs to be confirmed in future longitudinal studies. Furthermore, when examining quadriceps endurance, the mode of movement seems to be important as isotonic quadriceps endurance was independently associated with most PA measures even when controlling for isometric and isokinetic endurance properties of the quadriceps.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Burge, A. T., Cox, N. S., Abramson, M. J. & Holland, A. E. Interventions for promoting physical activity in people with chronic obstructive pulmonary disease (COPD). Cochrane Database Syst. Rev. 4, Cd012626. https://doi.org/10.1002/14651858.CD012626.pub2 (2020).
Waschki, B. et al. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohort study. Chest 140, 331–342. https://doi.org/10.1378/chest.10-2521 (2011).
Gimeno-Santos, E. et al. Determinants and outcomes of physical activity in patients with COPD: a systematic review. Thorax 69, 731–739. https://doi.org/10.1136/thoraxjnl-2013-204763 (2014).
Esteban, C. et al. Predictive factors over time of health-related quality of life in COPD patients. Respir. Res. 21, 138. https://doi.org/10.1186/s12931-020-01395-z (2020).
Vaes, A. W. et al. Changes in physical activity and all-cause mortality in COPD. Eur. Respir. J. 44, 1199–1209. https://doi.org/10.1183/09031936.00023214 (2014).
Vorrink, S. N., Kort, H. S., Troosters, T. & Lammers, J. W. Level of daily physical activity in individuals with COPD compared with healthy controls. Respir. Res. 12, 33. https://doi.org/10.1186/1465-9921-12-33 (2011).
Maltais, F. et al. An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 189, e15-62. https://doi.org/10.1164/rccm.201402-0373ST (2014).
Evans, R. A. et al. Is quadriceps endurance reduced in COPD?: a systematic review. Chest 147, 673–684. https://doi.org/10.1378/chest.14-1079 (2015).
Spruit, M. A. et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 188, e13-64. https://doi.org/10.1164/rccm.201309-1634ST (2013).
De Brandt, J. et al. Changes in structural and metabolic muscle characteristics following exercise-based interventions in patients with COPD: a systematic review. Expert Rev. Respir. Med. 10, 521–545. https://doi.org/10.1586/17476348.2016.1157472 (2016).
De Brandt, J. et al. Changes in lower limb muscle function and muscle mass following exercise-based interventions in patients with chronic obstructive pulmonary disease: a review of the English-language literature. Chron. Respir. Dis. 15, 182–219. https://doi.org/10.1177/1479972317709642 (2018).
Rausch-Osthoff, A. K., Kohler, M., Sievi, N. A., Clarenbach, C. F. & van Gestel, A. J. Association between peripheral muscle strength, exercise performance, and physical activity in daily life in patients with chronic obstructive pulmonary disease. Multidiscip. Respir. Med. 9, 37. https://doi.org/10.1186/2049-6958-9-37 (2014).
Hernandez, M. et al. The relationships between muscle power and physical activity in older men with chronic obstructive pulmonary disease. J. Aging Phys. Act. 25, 360–366. https://doi.org/10.1123/japa.2016-0144 (2017).
Boutou, A. K. et al. Progression of physical inactivity in COPD patients: the effect of time and climate conditions—a multicenter prospective cohort study. Int. J. Chron. Obstruct. Pulmon. Dis. 14, 1979–1992. https://doi.org/10.2147/copd.S208826 (2019).
Caspersen, C. J., Powell, K. E. & Christenson, G. M. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. (Washington, D.C.: 1974) 100, 126–131 (1985).
Nyberg, A., Tornberg, A. & Wadell, K. Correlation between limb muscle endurance, strength, and functional capacity in people with chronic obstructive pulmonary disease. Physiother. Can. 68, 46–53. https://doi.org/10.3138/ptc.2014-93 (2016).
Singh, S. J. et al. An official systematic review of the European Respiratory Society/American Thoracic Society: measurement properties of field walking tests in chronic respiratory disease. Eur. Respir. J. 44, 1447–1478. https://doi.org/10.1183/09031936.00150414 (2014).
Gephine, S. et al. Specific contribution of quadriceps muscle strength, endurance, and power to functional exercise capacity in people with chronic obstructive pulmonary disease: a multicenter study. Phys. Ther. https://doi.org/10.1093/ptj/pzab052 (2021).
Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of COPD (2020 Report). Fontana, WI: Global Initiative for Chronic Obstructive Lung Disease (GOLD). https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-03Dec19_WMV.pdf. Accessed 11 December 2020.
Holland, A. E. et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur. Respir. J. 44, 1428. https://doi.org/10.1183/09031936.00150314 (2014).
Standardization of Spirometry, 1994 Update. American Thoracic Society. Am J Respir Crit Care Med 152, 1107-1136 https://doi.org/10.1164/ajrccm.152.3.7663792 (1995).
Frykholm, E. et al. Inter-day test–retest reliability and feasibility of isokinetic, isometric, and isotonic measurements to assess quadriceps endurance in people with chronic obstructive pulmonary disease: a multicenter study. Chron. Respir. Dis. 16, 1479973118816497. https://doi.org/10.1177/1479973118816497 (2019).
Reid, K. F. & Fielding, R. A. Skeletal muscle power: a critical determinant of physical functioning in older adults. Exerc. Sport Sci. Rev. 40, 4–12. https://doi.org/10.1097/JES.0b013e31823b5f13 (2012).
Bui, K. L. et al. Reliability of quadriceps muscle power and explosive force, and relationship to physical function in people with chronic obstructive pulmonary disease: an observational prospective multicenter study. Physiother. Theory Pract. https://doi.org/10.1080/09593985.2019.1669233 (2019).
Gore, S., Blackwood, J., Guyette, M. & Alsalaheen, B. Validity and reliability of accelerometers in patients with COPD: a systematic review. J. Cardiopulm. Rehabil. Prev. https://doi.org/10.1097/HCR.0000000000000284 (2017).
Demeyer, H. et al. Standardizing the analysis of physical activity in patients with COPD following a pulmonary rehabilitation program. Chest 146, 318–327. https://doi.org/10.1378/chest.13-1968 (2014).
Wang, T., Tan, J. Y., Xiao, L. D. & Deng, R. Effectiveness of disease-specific self-management education on health outcomes in patients with chronic obstructive pulmonary disease: an updated systematic review and meta-analysis. Patient Educ. Couns. https://doi.org/10.1016/j.pec.2017.02.026 (2017).
Riebe, D., Ehrman, J. K., Liguori, G. & Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription 10th edn. (Wolters Kluwer, 2018).
Hopkins, W. G., Marshall, S. W., Batterham, A. M. & Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 41, 3–13. https://doi.org/10.1249/MSS.0b013e31818cb278 (2009).
Sun, G. W., Shook, T. L. & Kay, G. L. Inappropriate use of bivariable analysis to screen risk factors for use in multivariable analysis. J. Clin. Epidemiol. 49, 907–916. https://doi.org/10.1016/0895-4356(96)00025-x (1996).
Smith, G. Step away from stepwise. J. Big Data 5, 32. https://doi.org/10.1186/s40537-018-0143-6 (2018).
Tabachnick, B. G. & Fidell, L. S. Using Multivariate Statistics 6th edn. (Pearson, Boston, 2013).
Burnham, K. P. & Anderson, D. R. Multimodel inference: understanding AIC and BIC in model selection. Sociol. Methods Res. 33, 261–304. https://doi.org/10.1177/0049124104268644 (2004).
Pitta, F. et al. Potential consequences for stable chronic obstructive pulmonary disease patients who do not get the recommended minimum daily amount of physical activity. J. Bras. Pneumol. 32, 301–308. https://doi.org/10.1590/s1806-37132006001100008 (2006).
Kharbanda, S., Ramakrishna, A. & Krishnan, S. Prevalence of quadriceps muscle weakness in patients with COPD and its association with disease severity. Int. J. Chron. Obstruct. Pulmon. Dis. 10, 1727–1735. https://doi.org/10.2147/copd.S87791 (2015).
McNamara, R. J. et al. Determinants of functional, peak and endurance exercise capacity in people with chronic obstructive pulmonary disease. Respir. Med. 138, 81–87. https://doi.org/10.1016/j.rmed.2018.03.032 (2018).
Demeyer, H. et al. The minimal important difference in physical activity in patients with COPD (report). PLoS ONE 11, e0154587. https://doi.org/10.1371/journal.pone.0154587 (2016).
Breyer, M. K. et al. Nordic walking improves daily physical activities in COPD: a randomised controlled trial. Respir. Res. 11, 112. https://doi.org/10.1186/1465-9921-11-112 (2010).
Pleguezuelos, E. et al. Improving physical activity in patients with COPD with urban walking circuits. Respir. Med. 107, 1948–1956. https://doi.org/10.1016/j.rmed.2013.07.008 (2013).
Louvaris, Z. et al. Interval training induces clinically meaningful effects in daily activity levels in COPD. Eur. Respir. J. 48, 567–570. https://doi.org/10.1183/13993003.00679-2016 (2016).
Vivodtzev, I. et al. Significant improvement in arterial stiffness after endurance training in patients with COPD. Chest 137, 585–592. https://doi.org/10.1378/chest.09-1437 (2010).
Covey, M. K., Collins, E. G., Reynertson, S. I. & Dilling, D. F. Resistance training as a preconditioning strategy for enhancing aerobic exercise training outcomes in COPD. Respir. Med. 108, 1141–1152. https://doi.org/10.1016/j.rmed.2014.06.001 (2014).
Nyberg, A., Saey, D. & Maltais, F. Why and how limb muscle mass and function should be measured in patients with chronic obstructive pulmonary disease. Ann. Am. Thorac. Soc. 12, 1269–1277. https://doi.org/10.1513/AnnalsATS.201505-278PS (2015).
Marklund, S., Bui, K. L. & Nyberg, A. Measuring and monitoring skeletal muscle function in COPD: current perspectives. Int. J. Chron. Obstruct. Pulmon. Dis. 14, 1825–1838. https://doi.org/10.2147/copd.S178948 (2019).
Massierer, D., Alsowayan, W., Lima, V. P., Bourbeau, J. & Janaudis-Ferreira, T. Prognostic value of simple measures of physical function and muscle strength in COPD: a systematic review. Respir. Med. 161, 105856. https://doi.org/10.1016/j.rmed.2019.105856 (2020).
Roig, M., Eng, J. J., MacIntyre, D. L., Road, J. D. & Reid, W. D. Associations of the Stair Climb Power Test with muscle strength and functional performance in people with chronic obstructive pulmonary disease: a cross-sectional study. Phys. Ther. 90, 1774–1782. https://doi.org/10.2522/ptj.20100091 (2010).
Alcazar, J. et al. The sit-to-stand muscle power test: an easy, inexpensive and portable procedure to assess muscle power in older people. Exp. Gerontol. 112, 38–43. https://doi.org/10.1016/j.exger.2018.08.006 (2018).
Mesquita, R. et al. Physical activity patterns and clusters in 1001 patients with COPD. Chron. Respir. Dis. 14, 256–269. https://doi.org/10.1177/1479972316687207 (2017).
Louvaris, Z. et al. Intensity of daily physical activity is associated with central hemodynamic and leg muscle oxygen availability in COPD. J. Appl. Physiol. 1985(115), 794–802. https://doi.org/10.1152/japplphysiol.00379.2013 (2013).
Kortianou, E. A. et al. Limitation in tidal volume expansion partially determines the intensity of physical activity in COPD. J. Appl. Physiol. 1985(118), 107–114. https://doi.org/10.1152/japplphysiol.00301.2014 (2015).
Philip, K. E. J., Polkey, M. I., Hopkinson, N. S., Steptoe, A. & Fancourt, D. Social isolation, loneliness and physical performance in older-adults: fixed effects analyses of a cohort study. Sci. Rep. 10, 13908. https://doi.org/10.1038/s41598-020-70483-3 (2020).
Ho, S. C. et al. The relationship between anthropometric indicators and walking distance in patients with chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 10, 1857–1862. https://doi.org/10.2147/copd.s87714 (2015).
Funding
Open access funding provided by Umea University. The study was funded with support from The Swedish Research Council, The Swedish Heart, and Lung Association, The Canadian Lung Association, and Stichting Gooiskinderziekenhuis Huizen, the Netherlands. The funders had no role in the design or reporting of results from this study.
Author information
Authors and Affiliations
Contributions
E.F., D.S., H.W.V.H., P.K., F.M. and A.N. have contributed to the design and planning of the study, E.F., S.G., and A.L. performed data collection, A.N. and E.F. performed statistical analyses and wrote the manuscript. S.G., D.S., H.W.V.H., P.K., E.V., and F.M. critically revised the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
FM reports grants and lecture fees from Boehringer Ingelheim, GSK and Novartis. FM holds a CIHR/GSK research Chair on COPD at Université Laval. AN reports lecture fees from AstraZeneca. EF, SG, DS, AL, PK, EV, and H.W VH declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Frykholm, E., Gephine, S., Saey, D. et al. Isotonic quadriceps endurance is better associated with daily physical activity than quadriceps strength and power in COPD: an international multicentre cross-sectional trial. Sci Rep 11, 11557 (2021). https://doi.org/10.1038/s41598-021-90758-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-90758-7
- Springer Nature Limited