
Abstract
Gene expression imbalances were measured for tyrosine kinase (TK) genes using Nanostring in 19 samples of inflammatory myofibroblastic tumor (IMT). All cases were immunohistochemically stained with anaplastic lymphoma kinase (ALK) and pan-tropomyosin-related-kinase (pan-Trk) antibodies. Five cases with imbalanced ALK expression, reported with Nanostring, were tested using fluorescence in situ hybridization (FISH); two cases with imbalanced neurotrophic tyrosine receptor kinase 3 (NTRK3) expression were tested using reverse transcription-polymerase chain reaction (RT-PCR). One case with imbalanced expression for ROS proto-oncogene 1 (ROS1) was tested using RNA sequencing and RT-PCR. TK fusions were detected in all cases with imbalanced TK expression. RNA sequencing detected a FN1–ROS1 fusion gene in an adult IMT case. IMT with ALK rearrangement showed myofibroblast-dominant features. IMT with ETV6–NTRK3 fusion showed prominent lymphoplasmacytic infiltration with scattered myofibroblasts. Pan-Trk IHC revealed only scattered positively stained cells in IMT with ETV6–NTRK3 fusion gene. ROS1-positive IMT showed myofibroblast-dominant features.
Similar content being viewed by others


Introduction
Inflammatory myofibroblastic tumor (IMT) is a rare mesenchymal tumor that can occur at any age; however, it is most common among the children and young adults1. Although IMT can occur at any anatomical site, the lungs, abdomen/pelvis, and retroperitoneum are frequently affected. The tumor is histologically characterized by spindle myofibroblastic cell proliferation with a lymphoplasmacytic inflammatory infiltrate2. The standard IMT treatment is surgical resection; however, treatment options are limited for patients with unresectable tumors or at advanced stage of the disease.
A clonal rearrangement of chromosome 2p23 involving the anaplastic lymphoma kinase (ALK) gene is detected in approximately 50% of the IMT cases, resulting in ALK overexpression and hyperactivation3. Furthermore, recent studies have reported novel fusion genes, such as ROS proto-oncogene 1 (ROS1)4, platelet-derived growth factor receptor beta (PDGFRB), and neurotrophic tyrosine receptor kinase 3 (NTRK3) in these tumors2,5,6. Identification of these fusion genes involving tyrosine kinases (TK) in IMT opened a new therapeutic option for IMT patients, especially for those with advanced-stage tumors.
However, given the histological diversity of IMT, even experienced pathologists face difficulty in reaching a definite diagnosis. Thus, identification of the histological cues using appropriate molecular pathology techniques holds significant importance in the correct diagnosis of IMT. Here, we comprehensively screened the imbalances of TK gene expression to identify the novel fusions in IMTs.
Materials and methods
Case selection
We collected information regarding cases diagnosed as either IMT or inflammatory pseudotumor (IPT) from the files at the Pathology Department at Juntendo University Hospital, from 2008 to 2018. IMTs were diagnosed based on the histological and immunohistochemical characteristics described in the WHO Classification of Tumours1. Immunoglobulin G4 (IgG4)-related sclerosing disease was excluded using immunoglobulin G (IgG) and IgG4 immunohistochemical staining, together with available serum IgG4 data. Infectious lesions, including granulomatous lesions, were also excluded. As a result, a total of 19 cases, including one pediatric case, were diagnosed with IMT. These cases were numbered as IMT#1–19. All patients provided informed consent before the surgeries in accordance with the institutional review board policy.
Immunohistochemistry (IHC)
IHC was performed for all cases using the antibodies described in Table 1. A pediatric soft tissue tumor with an LMNA-NTRK1 fusion7 and a case of salivary gland secretory carcinoma with ETV6-NTRK3 (formerly MASC)8 fusion were used as positive controls for pan-Trk IHC.
RNA extraction
RNA was extracted from formalin-fixed paraffin-embedded (FFPE) samples using the RNeasy FFPE Kit (QIAGEN, Hilden, Germany). The primary tumor sample was used in cases of recurrence.
Nanostring analysis
The Nanostring (NanoString Technologies, Inc., Seattle, WA, USA) procedure was performed (probe set described in Supplementary Table 1) to target 90 different TK and three serine/threonine kinases (BRAF, ARAF, and CRAF). At least two probes, spanning the exons and 100 bp in size were designed for each gene. One was designed against the 5′-terminal sequence and another against the 3′-terminal sequence. Briefly, 400 ng of ribonucleic acid (RNA) was hybridized to the probes (a reporter probe and a capture probe) at 65 °C for 18–24 h using a thermal cycler. Samples were inserted into the nCounter Prep Station to remove excess probes, purify, and immobilize the sample on the internal surface of a sample cartridge for 3 h. Finally, the sample cartridge was transferred to the nCounter Digital Analyzer, where color codes were counted and tabulated for each target molecule. The expression number for the base sequence of the probe part was analyzed using nSolver Analysis Software Version 4.0 (https://www.nanostring.com/products/analysis-software/nsolver). Raw data were statistically analyzed and plotted on graphs [X-axis: log2(5′-end expression), Y axis: log2(3′-end expression)] with 95% confidence interval (CI) lines. The case was deemed to have imbalanced gene expression if one end expression was more than tenfold higher than the other end expression or out of the 95% CI area of the graph.
RNA sequencing
Total RNA was extracted from FFPE samples using the RNeasy FFPE Kit (Qiagen, Hilden, Germany) before treatment with deoxyribonuclease 1 (DNase 1) (Thermo Fisher Scientific; Waltham, MA, USA). The RNA-Seq library was prepared using the NEBNext Ultra Directional RNA Library Prep Kit (New England Bio Labs Inc., Tokyo, Japan) and according to the manufacturer’s protocol. Next-generation sequencing (NGS) was carried out from both ends of each cluster using the HiSeq2500 platform (Illumina, San Diego, CA, USA).
Reverse transcription-polymerase chain reaction (RT-PCR)
We performed RT-PCR to confirm the fusion genes ETV6–NTRK3 or FN1–ROS1 using the PCR SuperMix (Thermo Fisher Scientific, Commonwealth, MA, USA). RNA quality was determined using a Nanodrop, and total RNA was reverse-transcribed to complementary DNA (cDNA) using the SuperScriptIV First-Strand Synthesis Kit (Invitrogen). RT-PCR was performed using the Platinum Green Hot Start PCR Master Mix (Invitrogen) for 40 cycles at 55 °C annealing temperature with the following primer pairs. The ETV6–NTRK3 primer sequences were 5′-ACCACATCATGGTCTCTGTCTCCC-3′ and 5′-CATCGTGCTGAAGCGAGAACTG-3′8. FN1–ROS1 primer sequences were 5′-CCATAAAGGGCAACCAAGAG-3′ and 5′-CAGTGGGAGAAAGCTGAAGAT-3′. Glyceraldehyde 3-phosphate dehydrogenase (GAPDH) expression was used as an RNA quality control using the following primers: 5-GAAGGTGAAGGTCGGAGTC-3 and 5- GAAGATGGTGATGGGATTT-3′.
Fluorescence in situ hybridization (FISH)
In cases of imbalanced ALK expression, FISH was performed on 4-μm-thick unstained tissue sections (Vysis LSI ALK Dual-Color, BreakApart Rearrangement Probe Kit.). The FISH signals were scored by evaluating 50 tumor cell nuclei per case. A split signal was defined by 5′ and 3′ signals at a distance greater than a single signal width, and signals separated by a distance less than a single signal width were regarded as fused signals. Tumor cells showing split signals or isolated 3′ signals were concluded to have ALK rearrangements. We interpreted the result as FISH-positive, if > 15% tumor cells showed gene rearrangement6.
Ethical standards
This study was reviewed and approved by the Juntendo University School of Medicine Institutional Review Board (#2019-034).
Results
Nanostring assays for TK fusion screening
The clinicopathological features, including IHC findings of 19 IMT cases, are summarized in Table 2. We created graphs with a scatter plot for each tyrosine kinase receptor (TKR) in these cases. The Nanostring result quantifies the number of expressions (Supplementary Table 2). Imbalanced expression was defined if 3′-end expression was more than tenfold higher than 5′-end expression or lying out of the 95% CI area of the graph. This definition revealed imbalanced TK gene expression in ALK, ROS1, and NTRK3, which had been previously reported, and we conducted subsequent analysis on these three genes. Finally, five ALK, one ROS1, and two NTRK3 cases were identified as imbalanced cases (Fig. 1).

Graphs for ALK, NTRK3, and ROS1 expression after normalization using nSolver Analysis software Version 4.0 in all cases. X-axis: gene expression measured by a probe located on the 5′-end, Y-axis: gene expression measured by a probe located on the 3′-end. The red reference line represents twofold standard deviation (SD). The expression data was analyzed using the nSolver Analysis Software Version 4.0 (https://www.nanostring.com/products/analysis-software/nsolver).
Confirmatory studies
Further analyses (FISH, RT-PCR, IHC, and RNA sequencing) were performed for cases showing imbalanced gene expression based on Nanostring results.
FISH
We found ALK rearrangement in all five ALK imbalanced cases. One case occurred in the ileum, and the remaining four cases occurred in the lungs. ALK rearrangements were detected in all five cases (Fig. 2).

FISH for ALK rearrangement. The majority of tumor cells show a split signal pattern of one green signal (ALK 5′-end) and one red signal (ALK 3′-end).
IHC
ALK IHC staining was performed in all cases and revealed five positive cases (Fig. 3A,B). All five cases showed imbalanced ALK expression based on Nanostring data and were FISH-positive. Pan-Trk staining was also performed in all cases, including the two cases in which the NTRK3 fusion gene was confirmed using RT-PCR. Only scattered positively stained cells within lymphoplasmacytic backgrounds were observed in two IMTs with NTRK3 fusion (Fig. 3C–F). Smooth muscle actin (SMA) IHC staining also highlighted the scattered positively stained spindle-shaped cells (Fig. 3G,H). A pediatric soft tissue tumor with LMNA–NTRK1 showed diffuse and strong cytoplasmic staining for pan-Trk (Supplementary Fig. 1A). In contrast, a salivary gland secretory carcinoma with ETV6–NTRK3 fusion primarily exhibited typical nuclear staining with weak cytoplasmic staining for pan-Trk (Supplementary Fig. 1B).

Immunohistochemistry for ALK and pan-Trk. Strong ALK expression was observed. (A: IMT#2, B: IMT#3). Only scattered positively stained cells within lymphoplasmacytic backgrounds were observed in two IMTs with NTRK3 fusion (C: IMT#10, D: IMT#17). Spindle-shaped cells also showed positive staining for pan-Trk IHC (E: IMT#10, F: IMT#17). SMA IHC staining showed scattered positively stained cells among morphologically indistinguishable lymphoplasmacytic cells in addition to the spindle-shaped cells (G: IMT#10, H: IMT#17). (A–H): 400 × magnification.
RNA sequencing
RNA was sequenced in the single case with ROS1 imbalance. As a result, a FN1-ROS1 fusion gene was discovered.
RT-PCR
ETV6–NTRK3 fusion was detected using RT-PCR in two IMT cases with imbalanced NTRK3 expression. Both cases had the same fusion gene with ETV6 exon 5 fused to NTRK3 exon 15 based on Sanger sequencing (Fig. 4A,B). The first case was reported in a 41-year-old woman with IMT occurring in the right lung (IMT#10). Another example is of a 56-year-old man with IMT occurring in the left lung (IMT#17). FN1–ROS1 fusion was confirmed by RT-PCR and direct sequencing in the ROS1 imbalance case (Fig. 4C,D).

RT-PCR and Sanger sequencing. (A) A 110 bp RT-PCR product was detected using the ETV6–NTRK3 fusion primer pair. (B) Sanger sequencing demonstrates that exon 5 of ETV6 is fused to exon 15 of NTRK3 in IMT#10. (C) A 131 bp PCR product was detected using the FN1–ROS1 fusion primer pair. (D) Sanger sequencing demonstrates that exon 20 of FN1 is fused to exon 32 of ROS1 in IMT#16. Neg.: Negative control without template cDNA.
Histology of IMT with TK fusion
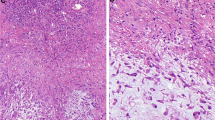
The dominant histological features are described in Table 2. Among the seven cases originally diagnosed as IMT, tumors in six cases were mainly composed of proliferating spindle cells with inflammatory infiltrates. Only one of the seven cases showed prominent lymphoplasmacytic infiltration with myofibroblastic cells. Four out of five IMT with ALK rearrangements were originally diagnosed as IMT. In contrast, among the 12 cases originally diagnosed as IPT, only two cases showed spindle cell predominant features, but both cases had TK fusion/rearrangement. One case with ALK rearrangement showed hypocellular proliferation of the spindle-shaped cells with prominent nucleoli in the myxoid background. In another case, ROS-1 positive IMT showed a histological admixture of spindle-shaped cells with prominent nucleoli and lymphoplasmacytic inflammatory cells within the collagenous background (Fig. 5A,B). Two cases with NTRK3 fusion showed prominent lymphoplasmacytic infiltration with scattered spindle-shaped myofibroblasts (Fig. 5C,D).

Histological features of IMT with TK fusion/rearrangement. ROS-1-positive IMT showing admixture of spindle-shaped cells with prominent nucleoli and lymphoplasmacytic inflammatory cells within collagenous background (A,B). Two cases with NTRK3 fusion showing prominent lymphoplasmacytic infiltration with scattered spindle-shaped myofibroblasts (C: IMT#10, D: IMT#17). (A): 100 × , (B–D): 200 × magnification.
Discussion
IMT is currently classified as an intermediate and rarely metastasizing neoplasm composed of myofibroblasts accompanied by an inflammatory infiltrate containing plasma cells, lymphocytes, and eosinophils in varying proportions. Most patients with IMT are children, adolescents, or young adults, but the tumor can occur throughout life. IMT was regarded as an inflammatory tumor-like lesion under the name IPT, which showed histological diversity. The concept of IMT was proposed because of its invasive and metastatic nature. Since the introduction of IMT, various gene fusion studies have been conducted. Approximately 50%–70% of IMT have been reported to harbor ALK gene rearrangement, leading to a chimeric fusion protein formation detectable by IHC or FISH2,9. However, this frequency varies from study to study, probably due to histological diversity. In IMT, more than 10 different genes have been identified as ALK fusion partners that provide a strong promoter and an oligomerization domain, resulting in oncogenic activation of the ALK kinase2. Furthermore, recent studies in IMT have described novel fusions involving ROS1, PDGFRB, and NTRK3 genes2,4,5,6. A recent study has demonstrated that all thoracic IMTs harbor TK abnormalities including ALK, ROS1, NTRK3, and rearranged during transfection (RET) TK fusions, and only one case had alternative ALK transcription initiation10.
We investigated the frequency of TK fusions in order to report a novel fusion in IMT. The Nanostring screening system employed in the study was based on the theory that a 5′-end/3′-end imbalance should be observed if fusion genes involving TKR were formed and maintained11. We found eight imbalanced cases using Nanostring and detected gene fusions/rearrangements in all of them. The imbalance criterion is a key factor in this assay. A previous study used 5′/3′ ratio below -4 on a log2 scale, which is consistent with the 5′/3′ ratio > 16-fold11. Another study used a 3′/5′ ratio > fivefold for ALK probes10. One of our two criteria was a 3′/5′ ratio > tenfold for each probe. We also employed another standard that used our accumulated Nanostring data set composed of more than 1000 sample data obtained using the same probe set. For this criterion, samples plotted out of the 95% CI area were considered significant, and all of these samples showed a 3′/5′ ratio > tenfold for the corresponding probe. Furthermore, the remaining cases lying within the 95% CI area showed 3′/5′ ratio < threefold. All the eight cases with TK fusions tested positive for both the criteria. Demonstrating the sensitivity of the scoring based on these two criteria, we detected only one case lying out of the 95% CI but negative for ALK IHC and FISH among all the collected samples. This case was not found positive upon screening with the tenfold increase criterion. Therefore, we believe that screening for a tenfold increase in case of 3′/5′ ratio would be more reliable. Regarding the correlation between IHC and Nanostring analysis, IHC was performed for all cases using ALK and pan-Trk antibodies, and all cases positive for either ALK or pan-Trk IHC showed imbalanced expression for ALK or NTRK3 by Nanostring, respectively. It is well known that the IHC staining pattern and intensity highly depends on the staining conditions, such as antibody dilution, antigen retrieval method, and the incubation time. Here, IHC titration could be considered ideal because none of the cases negative for imbalance showed positive results for pan-Trk and ALK IHC.
There are many variations for fusion genes in terms of partners and junctions, so it is difficult to cover all the possible fusion genes using RT-PCR. We have set all the 3′-end probes based on the sequences after the tyrosine kinase domain (TKD) for each TKR, allowing us to efficiently detect the functioning imbalance. These probes were also designed to target the exon–exon boundaries, to reduce the risk of interfering signals from genomic deoxyribonucleic acid (DNA) and correctly reflect the gene expression status. Our series showed that only 42% of the IMT cases harbored gene fusion/rearrangement involving either ALK, NTRK3, and ROS1, but it has been shown that approximately 50%–70% of the IMTs harbor ALK fusion/rearrangement2,9. A racial difference might have influenced the frequency of fusion genes involving TKRs in the study IMT samples. A recent study has demonstrated that 82.5% of the Japanese IMT cases had rearrangements involving either ALK, NTRK3, or ROS112, indicating that racial differences might be less likely to cause the low frequency of gene fusion/rearrangement. However, it has also been reported that pediatric cases frequently harbor TK fusions3,13,14. Our samples contained only one pediatric case, but one-third of the cases in a previous Japanese study were pediatric cases12. Therefore, the age difference might have affected the frequency of TK fusion/gene rearrangements. Furthermore, there also remains the possibility that IgG4-related sclerosing disease has not been completely excluded from the samples, since laboratory data on serum IgG4 levels were not available for most of the cases, although IgG and IgG4 IHC were performed for all cases. Interestingly, a recent study demonstrated that all thoracic IMTs harbor TK abnormalities, most of which are TK fusions10. In this study, TK fusions were detected in six of nine thoracic and two out of ten non-thoracic IMTs, respectively. We observed the same trend as that observed in the previous study10, and this difference was nearly statistically significant (p = 0.07).
Among the 19 IMT cases originally diagnosed as either IMT or IPT in this study, 7 cases were of IMT. FISH detected ALK gene rearrangements in four of these IMT cases (57.1%), which is consistent with the reported frequency of ALK fusion/rearrangements. The remaining 12 cases that have been originally diagnosed as IPT but revised as IMT by retrospective reviews, showed relatively few myofibroblasts with prominent inflammatory cells, including lymphocytes and plasma cells with hyalinized stroma. Only 4 of the 12 IPT cases harbored TK fusions (33.3%); however, interestingly, only one out of these four cases with TK fusions had ALK fusion/rearrangements. Thus, the relatively low frequency of TK fusions in our IMT samples may reflect the histological diversity in the lesions, and genetically unrelated histological mimics, especially in adults, that might have been included in the study samples, diluting the TK fusion frequency. Although a novel FN1–ROS1 fusion gene was recently discovered in an infantile IMT case4, we found, for the first time, FN1–ROS1 fusion in an adult IMT case, indicating that this fusion gene exists in both infant and adult patients. Although the practical scope of employing the Nanostring-based screening system in most hospitals is limited, the information is helpful for detecting ROS1 fusion in IMT with routine molecular tests using RT-PCR. This could lead to a potential molecular target therapy. In the near future, IMT might be defined and reclassified based on molecular pathological information concerning TK fusion/alteration10. The imbalanced TK expression detection by Nanostring or even quantitative PCR (qPCR) can be useful for not just identifying true IMT but also in the future molecular classification of IMT, keeping aside the concerns related to the histological diversity within IMT.
IMT with ETV6–NTRK3 fusion might have characteristic histological features. SMA staining confirmed that both the cases with ETV6–NTRK3 fusion were histologically composed of prominent lymphoplasmacytic infiltration with scattered myofibroblasts. The observation is closely related to the finding that only focal staining was observed using pan-Trk IHC in the two IMT cases with ETV6–NTRK3 fusion. In this regard, Alassiri et al. reported that IMT with ETV6-NTRK3 fusion can show a wide variety of histological features such as loose fascicles of spindle cells with prominent plasmacytic infiltrate, myxoid background, and ganglion-like cells5. It has been reported that pan-Trk IHC is highly sensitive and specific for NTRK3 fusion-positive tumor detection15,16. However, in comparison to NTRK1- and NTRK2-positive tumors, NTRK3 fusion-positive tumors are less sensitive to pan-Trk IHC17. Here, pan-Trk IHC was also performed on ETV6–NTRK3-positive secretory carcinoma (formerly MASC) under the same IHC staining conditions, but mainly nuclear rather than cytoplasmic staining was observed. However, an NTRK1 fusion tumor showed strong and diffuse cytoplasmic staining under the similar conditions (Supplementary Fig. 1). Although a recent study has demonstrated that nuclear and cytoplasmic staining patterns can be observed by pan-Trk IHC in NTRK3 fusion-positive IMT12, it is important to know that NTRK3 fusion-positive IMTs could also show a scattered nuclear/cytoplasmic staining pattern. This pattern is different from the diffused nuclear and poor cytoplasmic staining pattern of ETV6–NTRK3-positive secretory carcinoma (formerly MASC). Therefore, we shall conduct further studies based on this IHC finding, including RT-PCR and RNA sequencing. In addition, IMT cells with scattered staining pattern for pan-Trk IHC showed lymphoplasmacytic features, raising the possibility of being considered as a true IMT with NTRK3 fusion. Most of these positively stained cells for pan-Trk IHC had oval nuclei, and could not be morphologically distinguished from lymphoplasmacytic cells, and seemed not to display myofibroblastic characteristics. However, small amounts of spindle-shaped cells also exhibited positive staining for pan-Trk IHC though less frequent. In addition, SMA IHC staining also highlighted scattered positively stained cells with myofibroblastic nature among cells with oval nuclei.
Finally, our screening system also detected imbalanced gene expression for the following TK genes, other than ALK, ROS1, and NTRK3: CSK in IMT#1 and 9, LMTK3 in IMT#4, LTK in IMT#11 and 17, MUSTK in IMT#13, and EPHA4 in IMT#18. We searched for TK fusion genes involving the above listed TK genes in PubMed. Since the previous studies including those employing NGS failed to identify fusion genes involving these TKR genes, we excluded CSK, EPHA4, LMTK3, LTK, and MUSTK from the targets. However, it remains to be proven whether the 11 cases deemed negative for TK fusion in this study were really fusion-negative.
In summary, all ALK rearranged cases were positive for ALK IHC, and all cases other than ALK rearranged/NTRK3 fusion-positive cases were negative for pan-Trk and ALK IHC. Thus, this Nanostring-based screening system was both 100% sensitive and specific. Out of the 19 IMT cases, we identified 8 cases (42%) with TK fusions. We found FN1–ROS1 in adult patients with IMT. We must keep in mind that NTRK3 fusion-positive IMTs frequently show scattered cytoplasmic staining pattern for pan-Trk IHC, which at times may be difficult to interpret. The Nanostring-based screening system is useful for detecting TK fusions, especially NTRK3 fusions.
References
Fletcher CDM, Bridge JA, Hogendoorn PCW & Mertens F. World Health Organization Classification of Tumours of Soft Tissue and Bone. IARC 2013 4th Edition, 83–84 (2013).
Lovly, C. M. et al. Inflammatory myofibroblastic tumors harbor multiple potentially actionable kinase fusions. Cancer Discov. 4, 889–895. https://doi.org/10.1158/2159-8290.CD-14-0377 (2014).
Coffin, C. M. et al. ALK1 and p80 expression and chromosomal rearrangements involving 2p23 in inflammatory myofibroblastic tumor. Mod. Pathol. 14, 569–576. https://doi.org/10.1038/modpathol.3880352 (2001).
Lopez-Nunez, O. et al. Infantile inflammatory myofibroblastic tumors: Clinicopathological and molecular characterization of 12 cases. Mod. Pathol. https://doi.org/10.1038/s41379-019-0406-6 (2019).
Alassiri, A. H. et al. ETV6-NTRK3 is expressed in a subset of ALK-negative inflammatory myofibroblastic tumors. Am. J. Surg. Pathol. 40, 1051–1061. https://doi.org/10.1097/Pas.0000000000000677 (2016).
Yamamoto, H. et al. ALK, ROS1 and NTRK3 gene rearrangements in inflammatory myofibroblastic tumours. Histopathology 69, 72–83. https://doi.org/10.1111/his.12910 (2016).
Kohsaka, S. et al. Pediatric soft tissue tumor of the upper arm with LMNA-NTRK1 fusion. Hum. Pathol. 72, 167–173. https://doi.org/10.1016/j.humpath.2017.08.017 (2018).
Inaba, T. et al. Cytological features of mammary analogue secretory carcinoma of the parotid gland in a 15-year-old girl: A case report with review of the literature. Case Rep. Pathol. 2015, 656107. https://doi.org/10.1155/2015/656107 (2015).
Griffin, C. A. et al. Recurrent involvement of 2p23 in inflammatory myofibroblastic tumors. Cancer Res. 59, 2776–2780 (1999).
Chang, J. C. et al. Expanding the molecular characterization of thoracic inflammatory myofibroblastic tumors beyond ALK gene rearrangements. J. Thorac. Oncol. 14, 825–834. https://doi.org/10.1016/j.jtho.2018.12.003 (2019).
Suehara, Y. et al. Identification of KIF5B-RET and GOPC-ROS1 fusions in lung adenocarcinomas through a comprehensive mRNA-based screen for tyrosine kinase fusions. Clin. Cancer Res. 18, 6599–6608. https://doi.org/10.1158/1078-0432.CCR-12-0838 (2012).
Yamamoto, H. et al. Diagnostic utility of pan-Trk immunohistochemistry for inflammatory myofibroblastic tumors. Histopathology 76, 774–778. https://doi.org/10.1111/his.14010 (2010).
Antonescu, C. R. et al. Molecular characterization of inflammatory myofibroblastic tumors with frequent ALK and ROS1 gene fusions and rare novel RET rearrangement. Am. J. Surg. Pathol. 39, 957–967. https://doi.org/10.1097/PAS.0000000000000404 (2015).
Chan, J. K., Cheuk, W. & Shimizu, M. Anaplastic lymphoma kinase expression in inflammatory pseudotumors. Am. J. Surg. Pathol. 25, 761–768. https://doi.org/10.1097/00000478-200106000-00007 (2001).
Hechtman, J. F. et al. Pan-Trk immunohistochemistry is an efficient and reliable screen for the detection of NTRK fusions. Am. J. Surg. Pathol. 41, 1547–1551 (2017).
Rudzinski, E. R. et al. Pan-Trk immunohistochemistry identifies NTRK rearrangements in pediatric mesenchymal tumors. Am. J. Surg. Pathol. 42, 927–935. https://doi.org/10.1097/PAS.0000000000001062 (2018).
Gatalica, Z., Xiu, J., Swensen, J. & Vranic, S. Molecular characterization of cancers with NTRK gene fusions. Mod. Pathol. 32, 147–153. https://doi.org/10.1038/s41379-018-0118-3 (2019).
Acknowledgements
We thank Ms. Keiko Mitani, Mr. Koji Sonoue, Ms. Noriko Sasahara, Ms. Chisato Kohara, and Ms. Satomi Saito for their assistance with these studies. We also thank Dr. Shigeo Yamaguchi and Dr. Kaoru Mogushi for data analysis. We thank the Laboratory of Molecular and Biochemical Research, Research Support Center, Juntendo University Graduate School of Medicine for technical assistance.
Funding
This study was supported by a Grant-in-Aid from the Japan Society for the Promotion of Science (Grant Number #15H04964, #16K15670, and #15KK0353 to YS; #17K08730 and #20K07415 to TS; #17K10987 to KK; #18K15329 to TO; #18K16634 to YK). This study was financially supported in part through grants from Leading Advanced Projects for Medical Innovation (LEAP) (Grant Number #JP18am0001009) and the Practical Research for Innovative Cancer Control (Grant Number #JP18ck0106252) from the Japan Agency for Medical Research and Development.
Author information
Authors and Affiliations
Contributions
T.S., Y.S., T.H., K.A., Y.K., T.T., T.O. and K.K. designed the study. T.S., T.H. and T.Y. made pathological diagnosis of the cases. T.K. performed main part of the experiments and K.S. performed experiments of RT-PCR and sequencing part. S.K., T.U., N.H., H.M. performed RNA sequence and analyzed data. T.K., Y.S. and T.S. wrote the main part of the manuscriptv.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kurihara, T., Suehara, Y., Akaike, K. et al. Nanostring-based screening for tyrosine kinase fusions in inflammatory myofibroblastic tumors. Sci Rep 10, 18724 (2020). https://doi.org/10.1038/s41598-020-75596-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-75596-3
- Springer Nature Limited
This article is cited by
-
NTRK2 expression in gastrointestinal stromal tumors with a special emphasis on the clinicopathological and prognostic impacts
Scientific Reports (2024)
-
Low-grade tracheal adenocarcinoma with ETV6::NTRK3 fusion: unique morphology akin to subsets of sinonasal low-grade non-intestinal-type adenocarcinoma
Virchows Archiv (2022)
-
Distinct properties of pure- and mixed-type high-grade fetal lung adenocarcinomas by genetic profiling and transcription factor expression
Virchows Archiv (2022)
-
NTRK fusion in Japanese colorectal adenocarcinomas
Scientific Reports (2021)