
Abstract
Elevated serum uric acid (SUA) is associated with the incidence of hypertension, but whether relevant metabolic factors have mediating effects is not certain. Our study was based on a functional community cohort established in Beijing. In 2015, a total of 7482 individuals without hypertension were recruited and followed up until 2019. Multivariate logistic regression analysis was used to investigate the association between SUA and hypertension. Cross-lagged panel analysis and mediation analysis were used to explore the effects of metabolic factors on the association between SUA and incident hypertension. During the average 4-year follow-up, the cumulative incidence of hypertension was 10.9% (n = 580). SUA was an independent risk factor for hypertension, and the RRs (95% CI) for subjects with baseline SUA levels in quartile 2, quartile 3 and quartile 4 were 1.20 (0.88–1.63), 1.50 (1.10–2.05), and 1.57 (1.11–2.22) compared to those in quartile 1, respectively. The cross-lagged panel analysis showed that the increases in Cr, TG, LDL, ALT, AST and WBC occurred after SUA increased (P < 0.001). Among these factors, TG, WBC and ALT played an intermediary role in both men (TG: 14.76%; WBC: 11.61%; ALT: 15.93%) and women (TG: 14.55%; WBC: 8.55%; ALT: 6.89%). The elevated SUA concentration was an independent risk factor for hypertension in the Chinese population, and TG, WBC and ALT had important mediating effects on the association between SUA and hypertension.
Similar content being viewed by others

Introduction
Hypertension is a chronic disease characterized by elevated arterial blood pressure. Long-term hypertension is an important risk factor for cardiovascular diseases such as coronary artery disease and stroke [1, 2]. The number of people with hypertension has increased substantially due to population growth and aging [3]. Therefore, it is very important to optimize the hypertension risk stratification method to identify people at high risk of cardiovascular diseases and other complications.
Serum uric acid (SUA), the end-product of purine metabolism in humans, is excreted largely by the kidneys [4]. A large number of studies have shown that elevated SUA is a risk factor for hypertension [5, 6]. For example, a population-based cohort study in the United States showed that increasing quartiles of SUA were associated with the 10-year incidence of hypertension independent of smoking, alcohol intake and baseline kidney function [7]. Experimental studies have suggested that SUA may activate the renin angiotensin system and inhibit the release of endothelial nitric oxide, which is followed by a reduction in renal blood flow and elevation of systemic blood pressure [8].
In addition, many studies have reported that some metabolic indicators, such as body mass index (BMI) [9, 10], waist-hip ratio (WHR) [11], blood lipids [12, 13], fasting blood glucose (GLU) [12, 14], white blood cell [15], and alanine aminotransferase (ALT) [16], are significantly associated with hypertension and are closely related to the occurrence and development of hypertension. Moreover, these metabolic indicators have been found to be significantly correlated with SUA [17,18,19]. There may not be a direct correlation between SUA and hypertension, and their correlation may be partially or fully mediated by metabolic factors. For instance, the African-PREDICT study pointed out that the association between SUA and blood pressure is significant in young healthy women with increased adiposity but not in lean women or men [20]. A retrospective cohort study conducted in Japan by Kuwabara et al. reported that SUA is an independent risk factor for the onset of hypertension in lean subjects, and the risk of hypertension is significantly higher in lean subjects with metabolic syndrome than in lean subjects without metabolic syndrome [21].
However, the temporal relationship between SUA and these metabolic factors has not been elucidated by research. In this context, cross-lagged panel analysis has attracted extensive attention. It is an analytical strategy used to describe reciprocal relationships or directional influences between variables over time [22]. Mediation analysis could elucidate the association between two variables and quantify the effect of mediating variables [23]. Therefore, the purpose of our study was to revisit the association between elevated SUA concentrations and hypertension in our cohort, and then we further applied cross-lagged panel analysis and mediation analysis to explore the roles of relevant metabolic factors in the association of SUA with hypertension.
Methods
Study population
The present study was based on a functional community cohort established in 201024. The cohort was composed of 8671 current employees or retired employees (aged 30–65) of governments, schools, hospitals, factories, business, and service institutions in Xicheng District, representing most of the occupational population in urban Beijing. Those with somatic or psychiatric abnormalities were excluded at enrollment [24]. All the participants in the cohort underwent an annual physical examination at the health management center of Beijing Xuanwu Hospital, Capital Medical University. We collected relevant baseline data in 2015 and followed up the participants for 4 years. Each participant signed an informed consent form, and this study was approved by the Ethics Committee of Capital Medical University. Participants were excluded if they had hypertension, acute and chronic infectious diseases and severe liver and kidney diseases at baseline. Finally, 5330 subjects with normal blood pressure at baseline were included in our analyses (Fig. 1).

Flow diagram of participant recruitment
Data collection and clinical measurements
Data on general information such as age, sex, current smoking, alcohol consumption and physical exercise were collected by standard questionnaires. Current smoking was considered smoking more than one cigarette per day. Alcohol consumption was defined as the intake of wine/beer/cider/spirits 1 time per week or more. Physical exercise was defined as walking or bike riding more than 15 min daily, doing sports or physical exercise more than 2 h weekly, or lifting or carrying heavy objects at work daily [25].
Weight and height were measured while the subjects were wearing light clothing and no shoes. BMI was computed as weight in kilograms divided by the square of height in meters. Waist circumstance (WC) and hip circumference were measured with a soft ruler while the subjects were standing upright, with their arms drooping naturally and their abdomen in a relaxed state. The waist and hip measurements were accurate to 0.01 cm. The WHR was equal to WC divided by hip circumference. Blood pressure was measured uniformly with a calibrated mercury sphygmomanometer. The participants rested in a quiet state for 5 min. The right elbow was exposed with the participant in a sitting position and placed at the same level as the heart. The space between the lower margin of the cuff and the space in front of the elbow was 2~3 cm, and systolic blood pressure (SBP) and diastolic blood pressure (DBP) were recorded. The average of the two blood pressure measurements was taken, and the result was accurate to 1 mmHg.
Biochemical index detection
Blood samples were collected in the morning from 7:00 to 8:30 after participants fasted for 1 night. After the subjects provided informed consent, 5 ml peripheral venous blood was collected from the cubital vein using EDTA (ethylene diamine tetra-acetic acid) for biochemical marker detection. A fully automatic biochemical analyzer (Hitachi, 7060) was used to detect GLU, total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL), low-density lipoprotein cholesterol (LDL), aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatinine (Cr), white blood cell count (WBC) and serum uric acid (SUA).
Definition of hypertension
Participants with SBP above 140 mmHg, DBP above 90 mmHg, or self-reported use of antihypertensive agents were diagnosed with hypertension according to the JNC-7 criteria [26].
Statistical analysis
We summarized subjects’ demographic and biochemical characteristics using descriptive statistics, reporting the mean and standard deviation (SD) for normally distributed data or median and interquartile ranges for nonnormally distributed continuous variables stratified by sex. A correlation bubble diagram was drawn to assess the correlations between the variables in this study. To determine seasonal differences, we used the following definitions of seasons: winter is December, January and February; spring is March, April and May; summer is June, July and August; and autumn is September, October and November. The seasonal differences in SUA at baseline were compared using the Kruskal–Wallis H test.
Restricted cubic splines (RCS) were drawn to understand the relationship between uric acid and hypertension in the population, adjusting for age, sex, BMI, WHR, current smoking, alcohol consumption and physical exercise. Multivariable logistic regression models were used to analyze the association between hypertension and baseline SUA. To further explore the association between the change in SUA and hypertension, latent class trajectory models (LCTMs) were used to identify trajectories of SUA from 2015 to 2019 [27]. This is a specialized form of finite mixture modeling. Our models used second-order polynomials. The best-fitting number of trajectories was based on the lowest value of Bayesian information criterion (BIC). According to the slope of each trajectory, we assigned labels to the trajectories to facilitate interpretability. Then, receiver operating characteristic (ROC) curves were generated to estimate the effects of SUA on hypertension [28].
The cross-lagged panel analysis was used to measure the time relationship between SUA and relevant metabolic factors (BMI, WHR, GLU, TC, TG, LDL, HDL, Cr, AST, ALT, WBC). Cross-lagged panel analysis is a form of path analysis [29, 30] that also examines the reciprocal, longitudinal relationships between a set of interrelated variables [31].
Once the temporal relationship between metabolic factors and SUA was established, mediation models were constructed to examine whether these selected factors played a mediating role in the association between SUA and hypertension in men and women. In this model, X was SUA (predictor), M was the mediator, and hypertension was the outcome; mediators were determined by the cross-lagged path that was changed after SUA. This statistical approach has been applied successfully in previous studies to demonstrate the role of mediators [32,33,34,35]. The path coefficients were the beta (β) coefficients of the multivariable regression models and represented the magnitude and direction of associations between variables included in the model. We included age as a covariate to adjust for the mediating effect of these indicators on the association between SUA level and hypertension. R 3.6.3, SPSS 24.0 and Mplus Version 7.3 were used for the statistical analyses. All statistical tests were two-sided, with P < 0.05 considered to indicate statistical significance.
Results
Baseline characteristics
A total of 5330 participants were included in the final analysis. The baseline characteristics of participants according to quintiles of SUA stratified by sex are shown in Table 1. The correlation between variables at baseline in our study is shown in Supplementary Fig. 1. There was a correlation between SUA and SBP (r = 0.30) and between SUA and DBP (r = 0.30). The seasonal difference in SUA is shown in Fig. 2a. SUA was significantly higher in autumn than in other seasons.

Seasonal distribution of serum uric acid and trajectories of serum uric acid from 2015 to 2019. a seasonal distribution of serum uric acid; b trajectories of serum uric acid from 2015 to 2019; class 1: decreasing slowly and then increasing slowly at high concentration; class 2: maintaining a low concentration; class 3: maintaining a high concentration; class 4: rapidly rising and then falling at high concentration; and class 5: maintaining a moderate concentration
Cumulative incidence of hypertension
In 2019, the cumulative incidence of hypertension in the general population was 10.9% (n = 580), and there was a higher cumulative incidence of hypertension in men (12.2% (n = 299)) than in women (9.8% (n = 281)). As the SUA concentration increased, the incidence of hypertension gradually increased in men and women (P < 0.001) (Supplementary Figure 2).
The association between SUA and hypertension
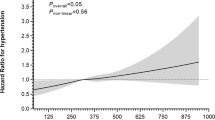
In the total population, we did not observe a nonlinear relationship between baseline SUA and incident hypertension after adjustment for age, sex, BMI, WHR, current smoking, alcohol consumption and physical exercise (P > 0.05) (Fig. 3a). In the sex-stratified analysis, we also did not identify nonlinear relationships between baseline SUA and incident hypertension after adjustment for age, BMI, WHR, current smoking, alcohol consumption and physical exercise (Fig. 3b, c).

Restricted cubic splines (RCS) and RRs between baseline SUA quartiles and hypertension in the study of the total population and stratified by sex. a RCS of total population; b RCS of men; c RCS of women; d RRs of total population; e RRs of men; f RRs of women. Model 1: adjusted for age and sex; Model 2: further adjusted for BMI, WHR, smoking, alcohol consumption, and physical activity; Model 3: further adjusted for SBP, DBP, GLU, TG, TC, HDL, LDL, Cr, AST, ALT, and WBC at baseline
The prospective association between baseline SUA concentration and the risk of developing hypertension in the longitudinal study is shown in Fig. 3d. In multivariable logistic regression analysis, SUA concentration quartiles were correlated with incident hypertension. After adjusting for age and sex (Model 1), using the lowest quartile as a reference, the relative risks (RRs) (95% CI) were 1.48 (1.11–1.97), 2.03 (1.53–2.71), and 2.41 (1.77–3.27) for quartiles 2–4, respectively. In Model 2, after additional adjustment for BMI, WHR, smoking, alcohol consumption, and physical exercise, the RRs (95% CI) were 1.34 (0.99–1.79), 1.70 (1.27–2.28), and 1.81 (1.32–2.48) for quartiles 2–4, respectively. Finally, after further adjusting for SBP, DBP, GLU, TG, TC, HDL, LDL, Cr, AST, ALT, and WBC at baseline in Model 3, the RRs (95% CI) were 1.20 (0.88–1.63), 1.50 (1.10–2.05), and 1.57 (1.11–2.22) for quartiles 2–4, respectively.
In the sex subgroup analysis, as Fig. 3e shows, the highest quartile of SUA compared with the lowest quartile was significantly associated with a 57% increased risk of hypertension (RR = 1.57 [1.07–2.33]) for men in Model 3. However, in women (Fig. 3f), we did not find a statistically significant association between SUA and hypertension (P = 0.092) in Model 3, which indicated elevated SUA in men had a higher risk of developing hypertension.
We identified five distinct trajectories of SUA in 5330 individuals (Fig. 2b), characterized by decreasing slowly and then increasing slowly at high concentrations (class 1; 187 [3.5%]); maintaining a low concentration (class 2; 1630 [30.6%]); maintaining a high concentration (class 3; 1497 [28.1%]); rapidly rising and then falling at high concentrations (class 4; 29 [0.5%]); and maintaining a moderate concentration (class 5; 1987 [37.7%]). Using the class 5 trajectory as the reference trajectory, the result of multiple logistic regression analysis showed that “decreasing slowly and then increasing slowly at high concentration” and “maintaining a high concentration” trajectories were associated with a higher risk of hypertension (Supplementary Table 1).
Predictive efficacy of serum uric acid for hypertension
According to the results of multivariable logistic regression analysis, SUA was an independent risk factor for hypertension in Model 3 after adjusting for all relevant variables in our study. Based on this, we take Model 3 as the prediction model. To assess the predictive efficacy of the prediction model, we assessed the ROC curve, for which the AUC was 0.725, and the 95% CI was 0.708–0.741 (Supplementary Table 2). In the analysis of male and female stratification, the AUC of women (0.769) was greater than that of men (0.674), indicating that the prediction model was even more effective in women. Supplementary Figure 3 shows the ROC curves for the prediction in the total population and stratified by sex.
Cross-lagged panel analysis of the association between SUA and BMI, WHR, Cr, GLU, TC, TG, HDL, LDL, ALT, AST, and WBC
Figure 4 shows the cross-lagged path analysis between BMI, WHR, Cr, GLU, TC, TG, HDL, LDL, ALT, AST, WBC and SUA in the total population, adjusted for age, sex and follow-up days. We can see that the changes in Cr, TG, LDL, ALT, AST and WBC occurred after the change in SUA, so we chose these indicators as potential mediators to analyze the association between SUA and hypertension. For these six indicators, both of the path coefficients ρ1 and ρ2 were significantly different from 0 (P < 0.001). ρ1 from baseline SUA to follow-up Cr (TG, LDL, ALT, AST and WBC) was greater than ρ2 from baseline Cr (TG, LDL, ALT, AST and WBC) to follow-up SUA (P < 0.001). The χ2 test for model fit showed a difference between the hypothesized model and the observed data (P < 0.001), which was probably related to the high sensitivity of the large sample size.

Cross-lagged path analysis of SUA and BMI, WHR, GLU, HDL, LDL, TC, TGs, Cr, WBC, ALT and AST adjusted for age, sex and follow-up days. a cross-lagged path of SUA and BMI, b cross-lagged path of SUA and WHR, c cross-lagged path of SUA and GLU, d cross-lagged path of SUA and HDL, e cross-lagged path of SUA and LDL, f cross-lagged path of SUA and TC, g cross-lagged path of SUA and TG, h cross-lagged path of SUA and Cr, i cross-lagged path of SUA and WBC, j cross-lagged path of SUA and ALT, k cross-lagged path of SUA and AST. r1: synchronous correlations; r2 and r3: tracking correlations; ρ1, ρ2: cross-lagged path coefficients. *: represent coefficients different from 0, P < 0.001. #: P < 0.001 for difference between ρ1 and ρ2
Mediation analysis between SUA and hypertension
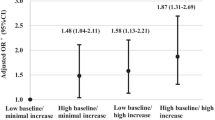
We tested Cr, TG, LDL, ALT, AST and WBC as potential mediators of the association between SUA and hypertension in men and women, with adjustment for age (Fig. 5 and Supplementary Table 3). TG, WBC and ALT played an intermediary role in both men and women, and the proportion of mediation in men was greater than that in women (TG: 14.76% > 14.55%; WBC: 11.61% > 8.55%; ALT: 15.93% > 6.89%). However, LDL and Cr did not play a mediating role in the relationship between SUA and hypertension in either men or women. Moreover, AST played a mediating role in men (AST: 11.17%) but not in women.

Mediation analysis of the association between SUA and hypertension. a men; b women
Discussion
In our study, we found a positive association between elevated SUA concentration and hypertension, and the hypertension prediction model had a good predictive ability. Through the cross-lagged panel analysis, we distinguished six indicators that changed after the SUA level changed, and then we analyzed their mediating effects on the association between SUA and hypertension. According to the results of mediation analysis, we found that TG, WBC and ALT played important mediating roles in the association between SUA and hypertension both in men and women.
Consistent with the Chinese Hypertension Guidelines [36], the incidence of hypertension was significantly higher in males than in females. Consistent with other studies, our study showed that elevated SUA was a risk factor for the incidence of hypertension. In a retrospective, single-center cohort study in Japan, increased SUA was a strong risk factor for developing hypertension in individuals with prehypertension [5]. Increasing levels of SUA were associated with elevated blood pressure in a cohort study in the US population [37]. Some studies in the US and Japan have shown that uric acid is associated with a U-shaped curve in the development of cardiovascular disease or cardiovascular mortality and that low levels of uric acid have some harmful effects on the cardiovascular system [38,39,40]. Unfortunately, low SUA levels did not show a deleterious effect on the development of hypertension in our study. This may be related to differences in the age, ethnicity, region and diet of the subjects in the different studies. Therefore, whether low SUA levels in the Chinese population have harmful effects on hypertension and the cardiovascular system needs to be further explored in other national studies.
Several pathogenetic mechanisms have been implicated in the association between SUA and hypertension. High SUA may lead to renal vasoconstriction through inhibition of the nitric oxide pathway and through activation of the renin–angiotensin system [41,42,43] and then to increased blood pressure. Moreover, SUA may cause oxidative stress by stimulating the activity of NADPH oxidase. This triggers activation of immune cells in the kidney, which results in renal vasoconstriction and increased blood pressure [44]. Uric acid can be produced by xanthine oxidase (XO) catalyzing the oxidation of hypoxanthine and xanthine [45]. Kario et al. found that topiroxostat, an XO inhibitor, significantly reduced plasma XO activity, resulting in a reduction in blood pressure and urinary albumin [46]. This finding also demonstrated that uric acid could have an effect on blood pressure. Therefore, in clinical practice, treatment can be used to reduce the activity of xanthine oxidase, thereby reducing uric acid levels and the influence of uric acid on blood pressure, ultimately reducing the risk of hypertension. To further explain the association between SUA and hypertension, we evaluated the mediation effect of the metabolic factors whose changes were induced by SUA changes. It was noteworthy that TG played the largest mediating role in this association, suggesting that TG is critical in the pathogenesis of hypertension. In a population-based cohort study, mediation analysis also showed that TG played an important mediating role in the pathway linking SUA and hypertension [47]. Unlike our study, that study also found that TC, HDL, BMI, and GLU had a mediating effect on the association. Renin–angiotensin system activation was induced not only by triglycerides but also by uric acid concentration, and the two factors had joint effects on blood pressure [47, 48]. Experimental studies have shown that SUA could increase TG accumulation [49, 50] and that hyperuricemia could also increase TG levels [51]. In general, many studies have suggested that SUA is independently related to TG [52, 53], and both are risk factors for hypertension. However, the chronological or causal relationship between them is not yet clear. The results of our prospective study showed that the elevation of SUA caused the elevation of TG. The important mediating role of TG also illustrated this point. Therefore, in the process of hypertension prevention and treatment in the future, attention should be given to whether there are abnormal TG levels.
WBC is a marker of subclinical or low-grade inflammation, and its five subtypes play various roles in the inflammatory response and host immunity [54, 55]. Accumulating evidence suggests that inflammation contributes to the development and progression of hypertension [56]. Our study found that WBC played a certain mediating role in the association between SUA and hypertension, suggesting that SUA may lead to increased blood pressure by inducing inflammation. Recent studies have found that SUA may cause inflammation by activating both mitogen-activated protein kinases (MAPKs) as well as stimulating NADPH oxidase [44]. In this study, we also found that the elevation of both AST and ALT occurred after the elevation of SUA. ALT played a mediating role in both genders, but AST only had a mediating effect in men. This difference may be related to age differences between men and women and differences in liver function due to men drinking more alcohol. Both ALT and AST are markers of liver dysfunction, and studies have shown that ALT is strongly correlated with the onset of hypertension in the Chinese population [57, 58]. In addition, studies have shown that serum ALT is closely related to insulin resistance [59], excessive inflammation and oxidative stress [60]. Thus, SUA may affect liver function through certain pathways, resulting in abnormal liver metabolism and elevated AST, which in turn affects the occurrence and development of hypertension. However, there are currently no studies showing a significant association between AST and hypertension [61]; therefore, the mediating effect of AST needs to be further studied.
In addition, it is worth noting that the mediating proportions of all the metabolic factors that play an intermediary role in this study are greater in males than in females, suggesting that the pathogenesis of hypertension in males and females may be different due to sex, lifestyle habits, sex hormones [62] and physical activity, which needs further research. Additionally, sex stratification should be carried out in the future for the prevention and control of hypertension.
Our study had several strengths. First, this study was a 4-year longitudinal study, which allowed for better verification of the causal relationship between SUA and hypertension. Second, we added the cross-lagged panel analysis to analyze the time sequence relationship between the variables in the study. This study had some limitations. First, we did not quantitatively investigate alcohol intake, and there was a lack of lifestyle variables such as dietary habits [63], which may affect the relationship between uric acid and hypertension. Second, the fact that our study is a single-center analysis and the included subjects may be more concerned about health issues than the general population may lead to selection bias. Third, most of the population in this study was composed of residents in the Beijing area, which resulted in certain regional limitations and limited the generalizability of the research results.
Perspective of Asia
Although uric acid is an independent risk factor for hypertension that has been confirmed by many studies, it has been reported that there are some differences in the strength of the correlation between different races [64]. Therefore, further studies are needed to confirm the roles of metabolic factors (TG, WBC, ALT) in mediating the association between uric acid and hypertension in other ethnic groups.
Conclusions
In conclusion, elevated SUA concentration was an independent risk factor for hypertension in the Chinese population. Moreover, TG, WBC and ALT played important mediating effects on this association. The findings of our cross-lagged panel analysis and mediation effect analysis of SUA and hypertension development may further strengthen our understanding of the pathogenesis of hypertension, emphasizing the combined effect of serum uric acid and metabolic factors and providing a new direction and thinking for the prevention of hypertension.
Data availability
The data are available from the corresponding author upon reasonable request.
References
Manosroi W, Williams GH. Genetics of human primary hypertension: focus on hormonal mechanisms. Endocr Rev. 2019;40:825–56.
Furie K. Epidemiology and primary prevention of stroke. Contin (Minneap Minn). 2020;26:260–7.
Collaboration NCDRF. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398:957–80
Gaubert M, Bardin T, Cohen-Solal A, Dievart F, Fauvel JP, Guieu R, et al. Hyperuricemia and hypertension, coronary artery disease, kidney disease: from concept to practice. Int J Mol Sci. 2020;21:4066.
Kuwabara M, Hisatome I, Niwa K, Hara S, Roncal-Jimenez CA, Bjornstad P, et al. Uric acid is a strong risk marker for developing hypertension from prehypertension: a 5-year Japanese cohort study. Hypertension. 2018;71:78–86.
Ali N, Mahmood S, Islam F, Rahman S, Haque T, Islam S, et al. Relationship between serum uric acid and hypertension: a cross-sectional study in Bangladeshi adults. Sci Rep. 2019;9:9061.
Shankar A, Klein R, Klein BE, Nieto FJ. The association between serum uric acid level and long-term incidence of hypertension: Population-based cohort study. J Hum Hypertens. 2006;20:937–45.
Mazzali M, Kanbay M, Segal MS, Shafiu M, Jalal D, Feig DI, et al. Uric acid and hypertension: cause or effect? Curr Rheumatol Rep. 2010;12:108–17.
Rahman M, Zaman MM, Islam JY, Chowdhury J, Ahsan HN, Rahman R, et al. Prevalence, treatment patterns, and risk factors of hypertension and pre-hypertension among Bangladeshi adults. J Hum Hypertens. 2018;32:334–48.
Ondimu DO, Kikuvi GM, Otieno WN. Risk factors for hypertension among young adults (18-35) years attending in Tenwek Mission Hospital, Bomet County, Kenya in 2018. Pan Afr Med J. 2019;33:210.
Walekhwa SN, Kisa A. Tobacco use and risk factors for hypertensive individuals in Kenya. Healthcare (Basel). 2021;9:591.
van Oort S, Beulens JWJ, van Ballegooijen AJ, Grobbee DE, Larsson SC. Association of cardiovascular risk factors and lifestyle behaviors with hypertension: a mendelian randomization study. Hypertension. 2020;76:1971–9.
Yao Y, He L, Jin Y, Chen Y, Tang H, Song X, et al. The relationship between serum calcium level, blood lipids, and blood pressure in hypertensive and normotensive subjects who come from a normal university in east of China. Biol Trace Elem Res. 2013;153:35–40.
Kuwabara M, Chintaluru Y, Kanbay M, Niwa K, Hisatome I, Andres-Hernando A, et al. Fasting blood glucose is predictive of hypertension in a general Japanese population. J Hypertens. 2019;37:167–74.
Sun YT, Gong Y, Zhu R, Liu X, Zhu Y, Wang Y, et al. Relationship between white blood cells and hypertension in Chinese adults: the Cardiometabolic Risk in Chinese (CRC) study. Clin Exp Hypertens. 2015;37:594–8.
Zhu L, Fang Z, Jin Y, Chang W, Huang M, He L, et al. Association between serum alanine and aspartate aminotransferase and blood pressure: a cross-sectional study of Chinese freshmen. BMC Cardiovasc Disord. 2021;21:472.
Nejatinamini S, Ataie-Jafari A, Qorbani M, Nikoohemat S, Kelishadi R, Asayesh H, et al. Association between serum uric acid level and metabolic syndrome components. J Diabetes Metab Disord. 2015;14:70.
Zong J, Sun Y, Zhang Y, Yuan J, Wang X, Zhang R, et al. Correlation between serum uric acid level and central body fat distribution in patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2020;13:2521–31.
Mukhopadhyay P, Ghosh S, Pandit K, Chatterjee P, Majhi B, Chowdhury S. Uric acid and its correlation with various metabolic parameters: a population-based study. Indian J Endocrinol Metab. 2019;23:134–9.
Du Toit WL, Schutte AE, Mels CMC. The relationship of blood pressure with uric acid and bilirubin in young lean and overweight/obese men and women: the African-PREDICT study. J Hum Hypertens. 2020;34:648–56.
Kuwabara M, Kuwabara R, Hisatome I, Niwa K, Roncal-Jimenez CA, Bjornstad P, et al. “Metabolically Healthy” Obesity and Hyperuricemia Increase Risk for Hypertension and Diabetes: 5-year Japanese Cohort Study. Obes (Silver Spring). 2017;25:1997–2008.
KM. Cross-Lagged Panel Analysis. (2017).
Dregan A, Rayner L, Davis KAS, Bakolis I, Arias de la Torre J, Das-Munshi J, et al. Associations between depression, arterial stiffness, and metabolic syndrome among adults in the uk biobank population study: a mediation analysis. JAMA Psychiatry. 2020;77:598–606.
Yan YX, Dong J, Liu YQ, Yang XH, Li M, Shia G, et al. Association of suboptimal health status and cardiovascular risk factors in urban Chinese workers. J Urban Health. 2012;89:329–38.
Yan YX, Dong J, Zhang J, Liu F, Wang W, Zhang L, et al. Polymorphisms in NR3C1 gene associated with risk of metabolic syndrome in a Chinese population. Endocrine 2014;47:740–8.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr., et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA 2003;289:2560–72.
Mirza SS, Wolters FJ, Swanson SA, Koudstaal PJ, Hofman A, Tiemeier H, et al. 10-year trajectories of depressive symptoms and risk of dementia: a population-based study. Lancet Psychiatry. 2016;3:628–35.
Churpek MM, Yuen TC, Winslow C, Meltzer DO, Kattan MW, Edelson DP. Multicenter comparison of machine learning methods and conventional regression for predicting clinical deterioration on the wards. Crit Care Med. 2016;44:368–74.
von Salisch M, Zeman JL. Pathways to reciprocated friendships: a cross-lagged panel study on young adolescents’ anger regulation towards friends. J Youth Adolesc. 2018;47:673–87.
Haga SM, Lisoy C, Drozd F, Valla L, Slinning K. A population-based study of the relationship between perinatal depressive symptoms and breastfeeding: a cross-lagged panel study. Arch Women’s Ment Health. 2018;21:235–42.
Chen W, Li S, Fernandez C, Sun D, Lai CC, Zhang T, et al. Temporal relationship between elevated blood pressure and arterial stiffening among middle-aged black and white adults: the bogalusa heart study. Am J Epidemiol. 2016;183:599–608.
Yang W, Guo Y, Ni W, Tian T, Jin L, Liu J, et al. Hypermethylation of WNT3A gene and non-syndromic cleft lip and/or palate in association with in utero exposure to lead: A mediation analysis. Ecotoxicol Environ Saf. 2021;208:111415.
Taverner D, Paredes S, Ferre R, Masana L, Castro A, Vallve JC. Assessment of arterial stiffness variables in patients with rheumatoid arthritis: A mediation analysis. Sci Rep. 2019;9:4543.
Gray HL, Contento IR, Koch PA, Noia JD. Mediating mechanisms of theory-based psychosocial determinants on behavioral changes in a middle school obesity risk reduction curriculum intervention, choice, control, and change. Child Obes. 2016;12:348–59.
Guo J, Naimi AI, Brooks MM, Muldoon MF, Orchard TJ, Costacou T. Mediation analysis for estimating cardioprotection of longitudinal RAS inhibition beyond lowering blood pressure and albuminuria in type 1 diabetes. Ann Epidemiol. 2020;41:7–13 e11.
Wang Z, Chen Z, Zhang L, Wang X, Hao G, Zhang Z, et al. Status of hypertension in China: results from the china hypertension survey, 2012-5. Circulation 2018;137:2344–56.
Loeffler LF, Navas-Acien A, Brady TM, Miller ER 3rd, Fadrowski JJ. Uric acid level and elevated blood pressure in US adolescents: National Health and Nutrition Examination Survey, 1999-2006. Hypertension. 2012;59:811–7.
Tseng WC, Chen YT, Ou SM, Shih CJ, Tarng DC, Taiwan Geriatric Kidney Disease Research G. U-Shaped association between serum uric acid levels with cardiovascular and all-cause mortality in the elderly: the role of malnourishment. J Am Heart Assoc. 2018;7:e007523.
Odden MC, Amadu AR, Smit E, Lo L, Peralta CA. Uric acid levels, kidney function, and cardiovascular mortality in US adults: National Health and Nutrition Examination Survey (NHANES) 1988-94 and 1999-2002. Am J Kidney Dis 2014;64:550–7.
Verdecchia P, Schillaci G, Reboldi G, Santeusanio F, Porcellati C, Brunetti P. Relation between serum uric acid and risk of cardiovascular disease in essential hypertension. The PIUMA study. Hypertension 2000;36:1072–8.
Kanbay M, Jensen T, Solak Y, Le M, Roncal-Jimenez C, Rivard C, et al. Uric acid in metabolic syndrome: From an innocent bystander to a central player. Eur J Intern Med. 2016;29:3–8.
Bjornstad P, Laffel L, Lynch J, El Ghormli L, Weinstock RS, Tollefsen SE, et al. Elevated serum uric acid is associated with greater risk for hypertension and diabetic kidney diseases in obese adolescents with type 2 diabetes: an observational analysis from the treatment options for type 2 diabetes in adolescents and youth (TODAY) study. Diabetes Care. 2019;42:1120–8.
Shih-Wei Lai K-CN. Which anthropometric indices best predict metabolic disorders in Taiwan? South Med J. 2004;97:578–82.
Sanchez-Lozada LG, Rodriguez-Iturbe B, Kelley EE, Nakagawa T, Madero M, Feig DI, et al. Uric acid and hypertension: an update with recommendations. Am J Hypertens. 2020;33:583–94.
Fukunari A, Okamoto K, Nishino T, Eger BT, Pai EF, Kamezawa M. et al. Y-700[1-[3-Cyano-4-(2,2-dimethylpropoxy)phenyl]-1H-pyrazole-4-carboxylic acid]: apotent xanthine oxidoreductase inhibitor with hepatic excretion. J Pharmacol Exp Ther. 2004;311:519–28.
Kario K, Nishizawa M, Kiuchi M, Kiyosue A, Tomita F, Ohtani H, et al. Comparative effects of topiroxostat and febuxostat on arterial properties in hypertensive patients with hyperuricemia. J Clin Hypertens (Greenwich). 2021;23:334–44.
Cao Z, Cheng Y, Li S, Yang H, Sun L, Gao Y, et al. Mediation of the effect of serum uric acid on the risk of developing hypertension: a population-based cohort study. J Transl Med. 2019;17:202.
Mazzali M, Hughes J, Kim YG, Jefferson JA, Kang DH, Gordon KL, et al. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension. 2001;38:1101–6.
Lanaspa MAS-LL, Choi YJ, Cicerchi C, Kanbay M, Roncal-Jimenez CA. Uric acid induces hepatic steatosis by generation of mitochondrial oxidative stress: potential role in fructose-dependent and -independent fatty liver. J Biol Chem. 2012;287:40732–44.
Choi YJ, Shin H-S, Choi HS, Park JW, Jo I, Oh E-S. Uric acid induces fat accumulation via generation of endoplasmic reticulum stress and SREBP-1c activation in hepatocytes. Lab Invest. 2014;94:1114–25.
Tapia ECM, Garcia-Arroyo FE, Soto V, Monroy-Sanchez F, Pacheco U, et al. Synergistic effect of uricase blockade plus physiological amounts of fructose–glucose on glomerular hypertension and oxidative stress in rats. Am J Physiol Ren Physiol. 2013;304:F727–F736.
Ali N, Rahman S, Islam S, Haque T, Molla NH, Sumon AH, et al. The relationship between serum uric acid and lipid profile in Bangladeshi adults. BMC Cardiovasc Disord. 2019;19:42.
Li F, Chen S, Qiu X, Wu J, Tan M, Wang M. Serum uric acid levels and metabolic indices in an obese population: a cross-sectional study. Diabetes Metab Syndr Obes. 2021;14:627–35.
Kim JH, Lee YJ, Park B. Higher monocyte count with normal white blood cell count is positively associated with 10-year cardiovascular disease risk determined by Framingham risk score among community-dwelling Korean individuals. Med (Baltim). 2019;98:e15340.
Pecht T, Gutman-Tirosh A, Bashan N, Rudich A. Peripheral blood leucocyte subclasses as potential biomarkers of adipose tissue inflammation and obesity subphenotypes in humans. Obes Rev. 2014;15:322–37.
Xiao L, Harrison DG. Inflammation in Hypertension. Can J Cardiol. 2020;36:635–47.
Jia J, Yang Y, Liu F, Zhang M, Xu Q, Guo T, et al. The association between serum alanine aminotransferase and hypertension: A national based cross-sectional analysis among over 21 million Chinese adults. BMC Cardiovasc Disord. 2021;21:145.
Huang G, Zhou H, Shen C, Sheng Y, Xue R, Dong C, et al. Bi-directional and temporal relationship between elevated alanine aminotransferase and hypertension in a longitudinal study of Chinese adults. Clin Exp Hypertens. 2021;43:750–7.
Liu X, Hamnvik OP, Chamberland JP, Petrou M, Gong H, Christophi CA, et al. Circulating alanine transaminase (ALT) and gamma-glutamyl transferase (GGT), but not fetuin-A, are associated with metabolic risk factors, at baseline and at two-year follow-up: the prospective Cyprus Metabolism Study. Metabolism 2014;63:773–82.
Kerner A, Avizohar O, Sella R, Bartha P, Zinder O, Markiewicz W, et al. Association between elevated liver enzymes and C-reactive protein: possible hepatic contribution to systemic inflammation in the metabolic syndrome. Arterioscler Thromb Vasc Biol. 2005;25:193–7.
Wu L, He Y, Jiang B, Liu M, Yang S, Wang Y, et al. Gender difference in the association between aminotransferase levels and hypertension in a Chinese elderly population. Med (Baltim). 2017;96:e6996.
Song JJ, Ma Z, Wang J, Chen LX, Zhong JC. Gender differences in hypertension. J Cardiovasc Transl Res. 2020;13:47–54.
Yoo TW, Sung KC, Shin HS, Kim BJ, Kim BS, Kang JH, et al. Relationship between serum uric acid concentration and insulin resistance and metabolic syndrome. Circ J. 2005;69:928–33.
DeBoer MD, Dong L, Gurka MJ. Racial/ethnic and sex differences in the relationship between uric acid and metabolic syndrome in adolescents: an analysis of national health and nutrition survey 1999-2006. Metabolism. 2012;61:554–61.
Acknowledgements
The authors thank Xuanwu Hospital of Capital Medical University for their support and assistance in this study. The authors thank the National Natural Science Foundation of China.
Funding
This work was supported by grants from the National Natural Science Foundation of China (81773511, 81573214).
Author information
Authors and Affiliations
Contributions
Yu-Xiang Yan and Xi Chu conceived the topic and designed the research. Jing Dong, Li-Kun Hu, Ya-Ke Lu, and Yu-Hong Liu carried out the data cleaning and collation. Jing Dong and Li-Kun Hu undertook the data analysis and drafted the manuscript. Yu-Xiang Yan, Xi Chu, Ya-Ke Lu, and Yu-Hong Liu provided guidance and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Capital Medical University, and informed consent was obtained from all individual participants included in the study.
Consent for publication
The authors affirm that human research participants provided informed consent for publication.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Dong, J., Hu, LK., Lu, YK. et al. Association of serum uric acid with the risk of developing hypertension: A prospective cohort study with mediation analysis. Hypertens Res 46, 345–356 (2023). https://doi.org/10.1038/s41440-022-01081-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-022-01081-1
- Springer Nature Singapore Pte Ltd.
Keywords
This article is cited by
-
2023 update and perspectives
Hypertension Research (2024)
-
Preface—this month’s Asian perspectives
Hypertension Research (2023)