
Abstract
Nonadherence to antihypertensive drugs is a primary reason for suboptimal clinical outcomes among hypertensive patients. We assessed adherence to newly initiated antihypertensive medications in non-elderly Japanese patients and examined which patient and facility characteristics were associated with low adherence. We selected new oral antihypertensive drug users, aged 30–74 years, between 2014 and 2016 from a large administrative claims database. We measured adherence as the proportion of days covered (PDC) during a 1-year follow-up and divided patients into three groups of low (PDC < 40%), intermediate (PDC ≥ 40% to <80%), and high (PDC ≥ 80%) adherence. Factors associated with low adherence were assessed by logistic regression analysis with generalized estimating equations. Among 31,592 patients (mean age, 51.7 years; 41.2% female), the median 1-year PDC was 88.5% (IQR: 41.9–98.1%). In total, 59.2%, 16.6%, and 24.2% of patients were categorized as having high, intermediate, and low adherence, respectively. Female sex (odds ratio [OR] 1.15, 95% confidential interval [95% CI] 1.08–1.22), younger age, and the initiation of angiotensin-converting enzyme inhibitors (OR 1.37, 95% CI 1.12–1.66), beta-blockers and thiazide diuretics (OR 4.82, 95% CI 4.34–5.36 and OR 3.91, 95% CI 2.79–5.46, respectively; compared with angiotensin II receptor blockers) were associated with low adherence. Patients initiating antihypertensives at larger hospitals (≥200 beds) were more likely to be adherent. While adherence to antihypertensive drugs in non-elderly Japanese patients was relatively high compared with that reported in previous studies in Western countries, patients with intermediate-low adherence may benefit from targeted interventions.
Similar content being viewed by others


Introduction
Hypertension is a common chronic disease and is associated with major cardiovascular disease (CVD) and mortality [1]. Previous studies have shown that better control of hypertension improves the clinical outcomes [1] and that better adherence to antihypertensive drugs is a key factor in its successful treatment, resulting in lower CVD mortality [2,3,4,5,6]. Nonadherence to prescribed drugs is one of the primary reasons for suboptimal clinical outcomes in these patients [7,8,9]. The identification of the predictors of nonadherence is important in the development of interventions to improve adherence because it will allow interventions to be targeted at patients at high risk of nonadherence. In previous studies, various factors have been associated with patient adherence, including patient demographics, chronic conditions, drug type, social issues, and healthcare systems [10,11,12].
Although hypertension is a common disease in Japan, with an estimated 43 million affected individuals in 2010 [13], few studies have reported adherence to antihypertensive drugs, especially on a nationwide level. There are many reports on adherence to antihypertensive drugs from different regions of Europe [14,15,16], North America [17,18,19], and Asia [20, 21], and adherence was shown to vary widely across countries. Therefore, a study of the adherence pattern in Japan and how the predictors of adherence compare with those from other countries is required. We thus sought to assess the adherence pattern of new users of antihypertensive drugs in a large Japanese administrative database and to evaluate whether patient and facility characteristics were associated with low adherence.
Methods
Data source
In this study, we used the administrative claims database of JMDC Inc., Japan. This database collects data from health insurance societies whose enrollees are employees of major corporations throughout Japan and their family members [22]. This database does not include people aged ≥75 years because their health insurance is covered by a public insurance system for older people. The database contains inpatient and outpatient claims data (for diagnoses, procedures, and prescriptions), demographic data, laboratory and measurement data from health check-ups, and facility information. The diagnostic information is coded according to the International Classification of Disease (ICD), 10th version, and the details of the prescribed drugs are coded according to the Anatomical Therapeutic Chemical (ATC) Classification System. The study was approved by the Institutional Review Board of the University of Tokyo, Tokyo, Japan.
Study cohort
Using the database, we identified new users of oral antihypertensive drugs aged ≥30 years who initiated monotherapy or combination therapy (i.e., treatment with two drugs) between January 2014 and June 2016 (Fig. 1). The target oral antihypertensive drugs included angiotensin II receptor blockers (ARBs; ATC codes: C09, C10BX03), angiotensin-converting enzyme inhibitors (ACEIs; ATC code: C09), beta-blockers (BBs; ATC code: C07, excluding metoprolol [C07AS02]), calcium channel blockers (CCBs; ATC code: C08, excluding selective calcium channel blockers with direct cardiac effects [C08D] and phenylalkylamine derivatives [C08EA]), and thiazides (ATC code: C03A).

Flowchart of patient selection
We defined the date of the first antihypertensive prescription on record for each patient as the index date and the previous 365 days as the baseline period. We defined new users as patients who were newly prescribed an antihypertensive drug without a prescription for any other antihypertensive drug in the preceding 365 days, excluding any patients who were not enrolled in the for ≥365 days before and ≥365 days after the index date. We also excluded patients who were prescribed only a single dosage (e.g., one tablet) of an antihypertensive drug on the index date, assuming that these were prescribed to treat transient conditions and were not intended for long-term use. In addition, we excluded patients with a recorded diagnosis of angina pectoris (ICD10 code: I20), myocardial infarction (ICD10 codes: I21–I23), ischemic heart disease (ICD10 codes: I24, I25), or heart failure (ICD10 code: I50) during the baseline period to generate a cohort of patients who were prescribed antihypertensive drugs for primary prevention of cardiovascular events rather than for secondary prevention.
Medication adherence
Adherence to antihypertensive medication was measured as the proportion of days covered (PDC), which is an interval-based measurement widely used among researchers to evaluate adherence based on administrative claims databases [23]. The PDC was calculated as the number of days covered by the prescription divided by the duration of follow-up [23]. We measured adherence for 365 days after the index date. If the drug class was switched between different antihypertensives or if there was an additional antihypertensive prescription, we counted the days covered by the drugs without duplication. We categorized the patients into three adherence groups based on their PDC as low adherence (<40%), intermediate adherence (≥40% to <80%), and high adherence (≥80%), considering the categories used in prior studies [2, 3, 14, 20, 24,25,26].
Baseline characteristics
We extracted information on the patients’ ages and sex from the database. The patient characteristics, including their medication use, previous diagnoses, and comorbidities, were defined using the claims recorded during the baseline period. Information on the facility that prescribed the initial antihypertensive medication was also extracted from the database.
The baseline medications included antidiabetic drugs (ATC code: A10), anxiolytics or hypnotic sedatives (ATC codes: N05B, N05C), H2 blockers (ATC code: A02BA), lipid-modifying agents (ATC code: C10), nonsteroidal anti-inflammatory drugs (NSAIDs; ATC code: M01A), and selective serotonin reuptake inhibitors (SSRIs)/serotonin and norepinephrine reuptake inhibitors (SNRIs) (ATC codes: N06AB, N06AX) because these are chronically or frequently used by some antihypertensive users (Supplementary table) [25]. Comorbidities included cancer (a history of inpatient care and ICD10 codes: C00–D48), cerebrovascular disease (a history of inpatient care and ICD10 codes: G45, I60–I69), chronic renal failure (ICD10 code: N18), chronic respiratory disease (ICD10 codes: J42–J45), hyperuricemia or gout (ICD10 codes: E790, M10), liver disease (ICD10 codes: K72–K75), obesity (ICD10 code: E66), and peripheral vascular disease (ICD10 code: I73). We did not include a diagnosis of diabetes mellitus, hyperlipidemia, or depression in the baseline comorbidities because prescriptions for these diseases were more specific. We defined patients with no record of the comorbidities or chronic conditions listed above and no drug record for diabetes or hyperlipidemia during the baseline period as ‘absent of comorbid conditions.’ We also assessed three surrogate measures of the patients’ overall health status: a history of hospitalization, defined as the presence of at least one inpatient claim; the number of drugs dispensed during the baseline period; and the number of concurrently prescribed drugs on the index date [25]. Finally, we categorized the facilities prescribing the initial antihypertensive drugs based on their number of beds: 0–19, 20–199 and ≥200. Facilities having 0–19 beds were defined as clinics, and the others were defined as hospitals based on the classification by the medical care law.
Statistical analysis
We first tabulated the characteristics of the patients in the whole cohort and evaluated the distribution of the PDC measurements. We also tabulated and compared the patient characteristics according to the PDC adherence groups using Pearson’s χ2 test for categorical variables and an analysis of variance for continuous variables.
We then evaluated the associations between the baseline characteristics, including first-line medications and classification in the low adherence group (defined as a PDC < 40%), by building univariable and multivariable logistic regression models. In the multivariable model, we included all of the variables described above. Generalized estimating equations (GEEs) were used to estimate the standard errors considering the possibility of correlations among patients treated at the same facility [27]. All statistical tests were two sided, and p < 0.05 was regarded as indicating statistical significance. All analyses were performed with SAS 9.4 (SAS Institute, Cary, NC).
Results
Participant characteristics and adherence to antihypertensive medication
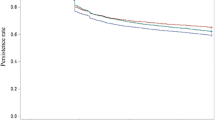
We identified 31,592 new users of antihypertensive therapy between January 2014 and June 2016. In the overall cohort, the mean PDC and its standard deviation (SD) were 70.2% and 34.6%, respectively, with a median of 88.5% and 25th and 75th percentiles of 41.9% and 98.1%, respectively (Fig. 2). The mean (SD) age of the analysis cohort was 51.7 (8.6) years (Table 1). In general, the prevalence of comorbidities was low, and the most frequent comorbidities were hyperuricemia or gout (13.5%) and chronic respiratory disease (10.9%). No comorbid conditions were diagnosed during the baseline period in 55.2% of patients. NSAIDs (37.8%), lipid-modifying agents (18.0%), and anxiolytics or hypnotic sedatives (14.3%) were frequently prescribed to the patients. Antihypertensives were predominantly prescribed as a single drug (95.4%), with CCBs (43.7%) and ARBs (42.1%) being the most frequently prescribed drugs, followed by BBs (7.0%), ACEIs (2.1%), and thiazides (0.5%). A few patients were prescribed combination therapies as their initial treatment (4.6%). For the vast majority of the patients (79.7%), these medications were prescribed by clinics rather than by hospitals.

Distribution of the PDC during the 365-day follow-up period
Factors associated with medication adherence
Table 2 shows the patient characteristics according to their adherence level. During the follow-up period of 365 days, 18,701 (59.2%), 5240 (16.6%), and 7651 (24.2%) patients were categorized as showing high adherence (PDC ≥ 80%), intermediate adherence (PDC ≥ 40–80%), or low adherence (PDC < 40%), respectively. Older patients were more likely to be adherent than younger patients, and females were less likely to be adherent than males. Patients who initiated combination therapy, ARB monotherapy, or CCB monotherapy were most likely to be adherent, whereas those who initiated BBs or thiazides tended to show low adherence during the follow-up period. Patients with hyperuricemia or gout, those prescribed antidiabetic drugs or lipid-modifying agents, and those attending a hospital were most likely to be adherent.
The univariable logistic regression analysis showed that most of the factors were significantly associated with low adherence, except for baseline comorbidities, the number of concurrently prescribed drugs and types of medical institutions. After adjustment for other factors using multivariable logistic regression analysis, the predictors associated with low adherence were indicated. Female sex (odds ratio [OR] 1.15, 95% confidence interval [CI] 1.08–1.22), a history of liver disease (OR 1.19, 95% CI 1.09–1.29), a history of peripheral vascular disease (OR 1.38, 95% CI 1.03–1.85), the absence of a chronic condition during the baseline period (OR 1.13, 95% CI 1.03–1.25), the use of anxiolytics or hypnotic sedatives (OR 1.23, 95% CI 1.13–1.34), the use of NSAIDs (OR 1.28, 95% CI 1.20–1.36), the prescription of multiple concurrent drugs on the index date (1–2 drugs: OR 1.29, 95% CI 1.20–1.38; ≥3 drugs: OR 1.33, 95% CI 1.21–1.45; compared with no prescriptions of concurrent drugs) and a history of hospitalization during the baseline period (OR 1.28, 95% CI 1.20–1.36) were significantly associated with low adherence (Table 3). Patients who initiated BBs (OR 4.82, 95% CI 4.34–5.36), thiazides (OR 3.91, 95% CI 2.79–5.46), or ACEIs (OR 1.37, 95% CI 1.12–1.66) were more likely to display low adherence than those who initiated ARBs. Patients who initiated combination therapy had a lower risk of low adherence than those who initiated a single therapy (OR 0.64, 95% CI 0.54–0.76). Age, the number of drug dispensations during the baseline period, and the use of antidiabetics were strong predictors of adherence. Higher age (50–59 years: OR 0.69, 95% CI 0.65–0.73; 60–74 years: OR 0.62, 95% CI 0.57–0.67; compared with 30–49 years), a history of hyperuricemia or gout (OR 0.86, 95% CI 0.78–0.94), more frequent drug dispensation (1–6 times: OR 0.90, 95% CI 0.84–0.97; ≥7 times: OR 0.59, 95% CI 0.53–0.64; compared with a history of no drug supply), the use of antidiabetics (OR 0.52, 95% CI 0.45–0.60) and the use of lipid-modifying agents (OR 0.78, 95% CI 0.71–0.85) were associated with a decreased risk of low adherence. Compared with patients prescribed antihypertensive drugs at a clinic, patients prescribed their drugs at larger hospitals (≥200 beds) had a decreased risk of low adherence (OR 0.81, 95% CI 0.73–0.89).
Discussion
In this population-based study, we found that 59.2% of new antihypertensive drug users in Japan displayed high adherence (PDC ≥ 80%) during the first 365 days of treatment. Low adherence was more frequent in females, younger patients, those with comorbidities, such as liver disease or peripheral vascular disease, those using anxiolytics and hypnotic sedatives, those prescribed multiple concurrent drugs and those who had a history of hospitalization. Patients who initiated BBs, thiazides, or ACEIs showed lower adherence than those who initiated CCBs or ARBs. Patients who were prescribed their drugs at small medical institutions were less likely to be adherent than those who received their prescriptions at larger hospitals.
A number of prior studies have evaluated adherence to antihypertensive drugs for the primary prevention of cardiovascular events. A meta-analysis of 11 studies, including 275,233 patients, reported that 50% of patients were categorized as adherent to the primary prevention regimen, although different metrics of adherence were used across the studies [28]. A study of an Italian population, including 31,306 patients initiating treatment with antihypertensive drugs, reported an adherence rate of 41.5% during the median follow-up of 1.9 years (maximum 3.5 years) [2]. Another large-scale study in the United Kingdom, which included 176,835 patients, found that the adherence rate was 80% for any antihypertensive drug during the median follow-up of 5.3 years [29]. A study that included 242,822 patients in the United States reported 1-year adherence rates of 24.2–38.5% [19]. When the longer follow-up periods and older age distributions in those studies are considered [14, 30], the adherence among Japanese non-elderly patients is relatively high, at least compared with previous reports from Western countries [19, 28, 31,32,33,34].
In a previous study based on a claims database, Wong et al. [20] reported that low adherence was associated with younger age, female sex, and a lack of comorbidities. In contrast, the use of combination therapies, ACEIs, and ARBs was associated with high adherence. Mazzaglia et al. [14] found that elderly and female patients were less likely to show good adherence, although cardiovascular risk factors were significantly associated with high adherence. Calderón-Larrañaga et al. [16] reported that younger age, female sex, and the presence of a mental comorbidity were positively associated with low adherence, whereas diabetes mellitus, hyperlipidemia, obesity, and risk factors for CVD were negatively associated with low adherence. Our findings are consistent with those of these earlier studies and demonstrate that predictors of low adherence include younger age, female sex, first prescription, and the type of medical institution. The association between sex and adherence has also been reported in studies of chronic conditions other than hypertension [7, 35, 36]. A study by Thunander et al. [37] showed that females were more likely than males to report their experiences and concerns about side effects to explain their nonadherence to any prescribed drug. Ong et al. [38] also reported that among atrial fibrillation patients, women tended to score lower for physical quality of life (QOL) than men and suggested that depression was a significant factor affecting the relationship between sex and QOL measures. These factors may contribute to the high likelihood of nonadherence to antihypertensive drugs among women.
Our findings on the association between drug class and adherence are similar to those reported previously. Ishida et al. [26] showed that adherence was the highest when ARBs were initiated, and there were no significant differences between adherence to ARBs and CCBs. The meta-analysis by Kronish et al. [39] also showed comparable results except for those on ACEIs. In an analysis of 15 previous publications, they reported that adherence was highest among patients who initiated treatment with ARBs or ACEIs, followed by those treated with CCBs, diuretics, or BBs. Although ACEIs are widely used as the primary treatment drug for hypertension in Western countries [15, 29, 34, 40], they were infrequently prescribed in our cohort [41]. East Asians reportedly suffer higher rates of adverse effects to ACEIs, including cough thanWhites [42]. Similarly, the side effects of BBs and thiazides (dizziness [43] and frequent urination [44], respectively) are widely reported. These factors may explain why the prescribing physicians were disinclined to prescribe these drugs and the patients’ low adherence to medications involving these drugs.
In this study, we found that patients who were prescribed antihypertensive drugs by doctors at larger hospitals had higher adherence rates than those who initiated treatment at clinics. Only ~20% of the patients who began treatment at hospitals received prescriptions from clinics at a later date, and the others continued receiving prescriptions from the hospital during the adherence measurement period (data not shown). This may be in part explained by the backgrounds of patients treated at these more specialized hospitals, including their comorbidities. While we do not know the exact mechanism of the pattern for certain, from a health economics perspective, most patients requiring continuous and long-term antihypertensive therapy should be treated by clinics rather than at acute-care hospitals. Further investigation on the mechanism underlying this phenomenon is warranted.
Strengths and limitations
The present study is the first to report adherence to newly initiated drug treatments for the primary prevention of hypertension based on a large-scale claims-based database in Japan. The size of the database allowed the robust assessment of patient adherence to antihypertensive drugs and the distribution of adherence in the cohort. However, several limitations of the study should be considered when interpreting the results. First, this was a claims-based study with limited information on patients’ clinical status. Although the prescriptions are expected to be recorded with high accuracy for claim purposes, diagnoses may be less accurate. Therefore, predictors related to baseline comorbid conditions may be interpreted as past records of potential diagnosis rather than definite comorbid conditions. We were also unable to assess the severity of the patients’ hypertension or the effectiveness of these drugs during the follow-up period. Second, because adherence was measured with prescription records, it may have differed from the patient’s actual drug-taking behavior. However, the PDC is known to be a conservative measure of adherence [45], and a strong association between adherence measured with claims and the patients’ actual blood concentrations of the drug prescribed has been reported [46]. Third, the generalizability of our results to the overall Japanese population might be limited in terms of age, sex, and socioeconomic status. The distribution of demographics, including age and sex, provided by JMDC Inc., is known to differ from national statistics for the same age group in Japan [47]. The database included few elderly enrollees, more males, and relatively healthier and wealthier patients than are present in the overall Japanese population because the database includes employees of major companies and their families.
Conclusions
Our objective evaluation of administrative claims data shows that adherence to newly initiated antihypertensive drugs in the Japanese population was relatively high compared with previous reports from Western countries. Factors associated with low adherence included younger age, female sex, drug class (including BBs, ACEIs, and thiazides), comorbid conditions, and the prescribing institution. These predictors may assist in the identification of candidates for interventions that effectively improve adherence to antihypertensive drug regimens.
References
World Health Organization. Global action plan for the prevention and cntrol of noncommunicable disease 2013–2020. http://www.who.int/iris/handle/10665/94384. Accessed 12 June 2019.
Esposti LD, Saragoni S, Benemei S, Batacchi P, Geppetti P, di Bari M, et al. Adherence to antihypertensive medications and health outcomes among newly treated hypertensive patients. Clin Outcomes Res. 2011;3:47–54. https://doi.org/10.2147/CEOR.S15619
Yang Q, Chang A, Ritchey MD, Loustalot F. Antihypertensive medication adherence and risk of cardiovascular disease among older adults: a population-based cohort study. J Am Heart Assoc. 2017;6. https://doi.org/10.1161/JAHA.117.006056
Tinetti ME, Han L, McAvay GJ, Lee DSH, Peduzzi P, Dodson JA, et al. Anti-hypertensive medications and cardiovascular events in older adults with multiple chronic conditions. PLoS ONE. 2014;9. https://doi.org/10.1371/journal.pone.0090733
Kim S, Shin DW, Yun JM, Hwang Y, Park SK, Ko YJ, et al. Medication adherence and the risk of cardiovascular mortality and hospitalization among patients with newly prescribed antihypertensive medications. Hypertension. 2016;67:506–12. https://doi.org/10.1161/HYPERTENSIONAHA.115.06731
Lee HJ, Jang SI, Park EC. Effect of adherence to antihypertensive medication on stroke incidence in patients with hypertension: a population-based retrospective cohort study. BMJ Open. 2017;7:1–8. https://doi.org/10.1136/bmjopen-2016-014486
Rodriguez F, Maron DJ, Knowles JW, Virani SS, Lin S, Heidenreich PA. Association of statin adherence with mortality in patients with atherosclerotic cardiovascular disease. JAMA Cardiol. 2019;4:206–13. https://doi.org/10.1001/jamacardio.2018.4936
Simard P, Presse N, Roy L, Dorais M, White-Guay B, Räkel A, et al. Association between metformin adherence and all-cause mortality among new users of metformin: a nested case-control study. Ann Pharmacother. 2018;52:305–13. https://doi.org/10.1177/1060028017743517
World Health Organization. Adherence to long-term therapies: evidence for action; 2015. https://www.who.int/chp/knowledge/publications/adherence_report/en/. Accessed 3 April 2019.
Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:1–12. https://doi.org/10.1155/2015/217047
Hamdidouche I, Jullien V, Boutouyrie P, Billaud E, Azizi M, Laurent S. Drug adherence in hypertension: Frommethodological issues to cardiovascular outcomes. J Hypertens. 2017;35:1133–44. https://doi.org/10.1097/HJH.0000000000001299
Osterberg L, Blaschke T. Adherence to medication dosage schedules. Control Clin Trials. 2005;10:333–4. https://doi.org/10.1016/0197-2456(89)90126-8
Miura K, Nagai M, Ohkubo T. Epidemiology of hypertension in Japan. Circ J. 2013;77:2226–31. https://doi.org/10.1253/circj.CJ-13-0847
Mazzaglia G, Ambrosioni E, Alacqua M, Filippi A, Sessa E, Immordino V, et al. Adherence to antihypertensive medications and cardiovascular morbidity among newly diagnosed hypertensive patients. Circulation. 2009;120:1598–605. https://doi.org/10.1161/CIRCULATIONAHA.108.830299
Schulz M, Krueger K, Schuessel K, Friedland K, Laufs U, Mueller WE, et al. Medication adherence and persistence according to different antihypertensive drug classes: a retrospective cohort study of 255,500 patients. Int J Cardiol. 2016;220:668–76. https://doi.org/10.1016/j.ijcard.2016.06.263
Calderón-Larrañaga A, Diaz E, Poblador-Plou B, Gimeno-Feliu LA, Abad-Díez JM, Prados-Torres A. Non-adherence to antihypertensive medication: the role of mental and physical comorbidity. Int J Cardiol. 2016;207:310–6. https://doi.org/10.1016/j.ijcard.2016.01.069
Friedman O, McAlister FA, Yun L, Campbell NRC, Tu K. Antihypertensive drug persistence and compliance among newly treated elderly hypertensives in Ontario. Am J Med. 2010;123:173–81. https://doi.org/10.1016/j.amjmed.2009.08.008
Ishisaka DY, Jukes T, Romanelli RJ, Wong KS, Schiro TA. Disparities in adherence to and persistence with antihypertensive regimens: an exploratory analysis from a community-based provider network. J Am Soc Hypertens. 2012;6:201–9. https://doi.org/10.1016/j.jash.2012.02.004
Patel BV, Remigio-Baker RA, Mehta D, Thiebaud P, Frech-Tamas F, Preblick R. Effects of initial antihypertensive drug class on patient persistence and compliance in a usual-care setting in the United States. J Clin Hypertens. 2007;9:692–700. https://doi.org/10.1111/j.1524-6175.2007.07194.x
Wong MCS, Tam WWS, Cheung CSK, Tong ELH, Sek ACH, Cheung NT, et al. Medication adherence to first-line antihypertensive drug class in a large Chinese population. Int J Cardiol. 2012;167:1438–42. https://doi.org/10.1016/j.ijcard.2012.04.060
Liu KQL, Griffiths SM, Wong MCS, Kang CD, Wang HHX, Li WTL, et al. Determinants of medication adherence and blood pressure control among hypertensive patients in Hong Kong: a cross-sectional study. Int J Cardiol. 2014;182:250–7. https://doi.org/10.1016/j.ijcard.2014.12.064
Sakamoto H, Rahman M, Nomura S, Okamoto E, Koike S, Yasunaga H, et al. Japan health system review. World Health Organization. New Delhi, India: Regional Office for South-East Asia; 2018;8. p. 55.
Pednekar PP, Ágh T, Malmenäs M, Raval AD, Bennett BM, Borah BJ, et al. Methods for measuring multiple medication adherence: a systematic review–Report of the ISPOR Medication Adherence and Persistence Special Interest Group. Value Heal. 2019;22:139–56. https://doi.org/10.1016/j.jval.2018.08.006
Ho PM, Bryson CL, Rumsfeld JS. Medication adherence. Circulation. 2009;119:3028–35. https://doi.org/10.1161/CIRCULATIONAHA.108.768986
Kumamaru H, Lee MP, Choudhry NK, Dong Y-H, Krumme AA, Khan N, et al. Using previous medication adherence to predict future adherence. J Manag Care Spec Pharm. 2018;24:1146–55. https://doi.org/10.18553/jmcp.2018.24.11.1146
Ishida T, Oh A, Hiroi S, Shimasaki Y, Nishigaki N, Tsuchihashi T. Treatment patterns and adherence to antihypertensive combination therapies in Japan using a claims database. Hypertens Res. 2018;42:249–56. https://doi.org/10.1038/s41440-018-0127-0
Hanley JA, Negassa A, Edwardes MDdB, Forrester JE. Statistical analysis of correlated data using generalized estimating equations: an orientation. Am J Epidemiol. 2003;157:364–75. https://doi.org/10.1093/aje/kwf215
Naderi SH, Bestwick JP, Wald DS. Adherence to drugs that prevent cardiovascular disease: meta-analysis on 376,162 patients. Am J Med. 2012;125:882–7.e1. https://doi.org/10.1016/j.amjmed.2011.12.013
Kurdi AI, Chen LC, Elliott RA. Exploring factors associated with patients’ adherence to antihypertensive drugs among people with primary hypertension in the United Kingdom. J Hypertens. 2017;35:1881–90. https://doi.org/10.1097/HJH.0000000000001382
Ho PM, Bryson CL, Rumsfeld JS. Medication adherence: its importance in cardiovascular outcomes. Circulation. 2009;119:3028–35. https://doi.org/10.1161/CIRCULATIONAHA.108.768986
Degli Esposti L, Esposti ED, Valpiani G, Di Martino M, Saragoni S, Buda S, et al. A retrospective, population-based analysis of persistence with antihypertensive drug therapy in primary care practice in Italy. Clin Ther. 2002;24:1347–57. https://doi.org/10.1016/S0149-2918(02)80039-X
Yang Z, Howard DH, Loustalot F, Ritchey M, Roy K, Will J. Association of antihypertensive medication adherence with healthcare use and medicaid expenditures for acute cardiovascular events. Med Care. 2016;54:504–11.
Ferrario CM, Panjabi S, Buzinec P, Swindle JP. Clinical and economic outcomes associated with amlodipine/renin–angiotensin system blocker combinations. Ther Adv Cardiovasc Dis. 2013;7:27–39. https://doi.org/10.1177/1753944712470979
Elliott WJ, Plauschinat CA, Skrepnek GH, Gause D. Persistence, adherence, and risk of discontinuation associated with commonly prescribed antihypertensive drug monotherapies. J Am Board Fam Med. 2007;20:72–80. https://doi.org/10.3122/jabfm.2007.01.060094
Granger BB, Ekman I, Granger CB, Ostergren J, Olofsson B, Michelson E, et al. Adherence to medication according to sex and age in the CHARM programme. Eur J Heart Fail. 2009;11:1092–8. https://doi.org/10.1093/eurjhf/hfp142
Kim J, Lee E, Park BJ, Bang JH, Lee JY. Adherence to antiretroviral therapy and factors affecting low medication adherence among incident HIV-infected individuals during 2009-2016: a nationwide study. Sci Rep. 2018;8:1–8. https://doi.org/10.1038/s41598-018-21081-x
Thunander Sundbom L, Bingefors K. Women and men report different behaviours in, and reasons for medication non-adherence: a nationwide Swedish survey. Pharm Pract. 2012;10:207–21.
Ong L, Irvine J, Nolan R, Cribbie R, Harris L, Newman D, et al. Gender differences and quality of life in atrial fibrillation: the mediating role of depression. J Psychosom Res. 2006;61:769–74. https://doi.org/10.1016/j.jpsychores.2006.08.003
Kronish IM, Woodward M, Sergie Z, Ogedegbe G, Falzon L, Mann DM. Meta-Analysis. Circulation. 2011;123:1611–21. https://doi.org/10.1161/CIRCULATIONAHA.110.983874
Mancia G, Soranna D, Rea F, Ghirardi A, Corrao G, Merlino L. Adherence with antihypertensive drug therapy and the risk of heart failure in clinical practice. Hypertension. 2015;66:742–9. https://doi.org/10.1161/hypertensionaha.115.05463
Ishida T, Oh A, Hiroi S, Shimasaki Y, Tsuchihashi T. Current prescription status of antihypertensive drugs in Japanese patients with hypertension: analysis by type of comorbidities. Clin Exp Hypertens. 2018;00:1–8. https://doi.org/10.1080/10641963.2018.1465074
McDowell SE, Coleman JJ, Ferner RE. Systematic review and meta-analysis of ethnic differences in risks of adverse reactions to drugs used in cardiovascular medicine. Br Med J. 2006;332:1177–80. https://doi.org/10.1136/bmj.38803.528113.55
NHS. Beta blockers—NHS. https://www.nhs.uk/conditions/beta-blockers/. Accessed 24 June 2019.
Harvard Health Publishing. Tips for taking diuretic medications—Harvard Health. https://www.health.harvard.edu/heart-health/tips-for-taking-diuretic-medications. Accessed 24 June 2019.
Raebel MA, Schmittdiel J, Karter AJ, Konieczny JL, Steiner JF. Standardizing terminology and definitions of medication adherence and persistence in research employing electronic databases. Med Care. 2013;51:S11–21. https://doi.org/10.1097/MLR.0b013e31829b1d2a
Steiner JF, Prochazka AV. The assessment of refill compliance using pharmacy records: methods, validity, and applications. J Clin Epidemiol. 1997;50:105–16. https://doi.org/10.1016/S0895-4356(96)00268-5
Ohisa M, Kimura Y, Matsuo J, Akita T, Sato T, Matsuoka T, et al. Estimated numbers of patients with liver disease related to hepatitis B or C virus infection based on the database reconstructed from medical claims from 2008 to 2010 in Japan. Hepatol Res. 2015;45:1228–40. https://doi.org/10.1111/hepr.12497
Acknowledgements
This study was funded, in part, by the Japan Agency for Medical Research and Development (grant number 17lk1010010h0002).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
HK, SK, and HM are affiliated with the Department of Healthcare Quality Assessment at the University of Tokyo. The department is a social collaboration department supported by the National Clinical Database, Johnson & Johnson K.K., and Nipro Corporation. SK reports investigator-initiated grant funding from Bayer and Daiichi Sankyo, and personal fees from AstraZeneca, Bayer, Bristol-Myers Squibb, Daiichi Sankyo, Pfizer, Teikoku Seiyaku, and Boehringer Ingelheim, outside the submitted work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Nishimura, S., Kumamaru, H., Shoji, S. et al. Adherence to antihypertensive medication and its predictors among non-elderly adults in Japan. Hypertens Res 43, 705–714 (2020). https://doi.org/10.1038/s41440-020-0440-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-020-0440-2
- Springer Nature Singapore Pte Ltd.
Keywords
This article is cited by
-
The impact of clinical inertia on uncontrolled blood pressure in treated hypertension: real-world, longitudinal data from Japan
Hypertension Research (2024)
-
Do Orally Disintegrating Tablets Facilitate Medical Adherence and Clinical Outcomes in Patients with Post-stroke Dysphagia?
Dysphagia (2024)
-
Treatment and adherence to antihypertensive therapy in France: the roles of socioeconomic factors and primary care medicine in the ESTEBAN survey
Hypertension Research (2021)
-
Improving patient adherence: the last obstacle to achieving hypertension control
Hypertension Research (2021)