
Abstract
Design Prospective cohort study with seven years of follow-up.
Cohort selection All children aged under six years, who attended one of 15 randomly selected health centres in the municipality of Santa Maria, a city in Southern Brazil on National Children's Vaccination Day in 2010.
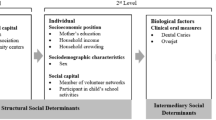
Exposure measurement Individual social support was measured by a questionnaire which asked parents if they had attended a volunteer group in the previous 12 months and if they participated in any groups related to the child's school. Neighbourhood social capital was measured for each of the 15 neighbourhoods, by indicating the presence or absence of each of the following three types of community assets: social-class associations; workers associations; and cultural community centres.
Outcome measurement Oral health-related quality of life (OHRQofL) was assessed using the Brazilian version of the Child Perception Questionnaire, for 8-10-year-olds (CPQ8-10). This includes a 5-point Likert score across 25 questions relating to oral symptoms, functional limitations, emotional well-being, and social well-being. The total mean score for each exposure group was calculated, ranging from 0-100, where higher scores indicate poorer OHRQofL.
Data analysis The association between individual and neighbourhood social capital at baseline and oral health-related quality of life at follow-up was assessed using a multi-level Poisson regression model to create incidence-rate-ratios where a ratio greater than 1 indicates poorer OHRQofL. Other variables included in the model were: sex; household income; household crowding; dental attendance behavior; presence of dental caries; and presence of increased maxillary overjet.
Results Of the 639 children originally enrolled in the study, 449 children were included at follow up (70.3%). Children who lived in a community that had a social-class association (IRR 0.79, 95% CI 0.67-0.93) or workers association (IRR 0.79, 95% CI 0.78-0.93) at baseline had lower oral health impact scores (better oral health-related quality of life) seven years later. The presence of cultural community centres was not associated with OHRQofL. Parental involvement with school activities at baseline was also associated with better OHRQofL at follow up (IRR 1.23, 95% CI 1.14-1.34), but participation in a voluntary network was not. Other variables that had a significant association with OHRQofL were: sex; household income; household crowding; dental attendance pattern; caries incidence; and increased maxillary overjet.
Conclusions Oral health-related quality of life was influenced by individual and neighbourhood social capital.
Similar content being viewed by others


A Commentary on
Knorst J K, Menegazzo G R, Emmanuelli B, Mendes F M, Ardenghi T M.
Effect of neighborhood and individual social capital in early childhood on oral health-related quality of life: a 7-year cohort study. Qual Life Res 2019; DOI:10.1007/s11136-019-02138-4.

GRADE rating
Commentary
Social capital can be defined as 'networks together with shared norms, values and understandings that facilitate co-operation within or among groups'.1 Health may be improved by social capital in a number of ways. 'Bonding' social capital refers to close ties that can help mitigate the strains of life.2 An example might be a family member bringing an older relative to a dental appointment. These close relationships can reduce stress and loneliness, which are in themselves health damaging, but may also increase the likelihood of adverse coping behaviours, such as smoking and drinking. Looser ties between groups from different backgrounds is known as 'bridging' social capital.2 This can promote trust and aid beneficial transfer of information, such as job opportunities. An example might be between members of a voluntary group. 'Linking' social capital refers to links between individuals and groups at different levels in the social or power hierarchy; opening up resources and opportunities to less powerful or excluded groups.3 Examples include relationships between funders and community interest groups, or formal mentorship arrangements.
A recent systematic review and meta-analysis found a 'modest positive relationship' between social capital and self-reported 'good health' and mortality outcomes.4 There is a growing body of literature investigating links between social capital and oral health, which have so far shown mixed results.5 One of the key difficulties faced by investigators is how to accurately measure such a complex social concept.4,5 Additionally, many previous studies have not accounted for important confounders, and there has been a lack of longitudinal studies.4 Longitudinal studies are needed because it is impossible to say from cross-sectional studies which direction any relationship is operating in; that is, it could be that poor health reduces social participation, rather than the other way around. This study adds to the literature and benefits from a prospective design with a population-based sample, relatively long duration of follow-up and good retention rates. The analysis also accounted for the confounding effect of socio-economic factors and reason for last dental attendance. The results are interesting and provide some evidence of an association between social capital and oral health in Brazilian children.
In the UK context, a recent prospective cohort study found that lower social capital at baseline was associated with greater deterioration in OHRQofL in older adults after five years.6 However, as with all observational studies, it must be remembered that association does not necessarily mean causation. It may be possible that measures of social capital correlate with other important but unmeasured confounders. Well-controlled intervention studies aimed at increasing neighbourhood or individual social capital are needed to provide stronger evidence of causation. Recent initiatives underpinned by theory and research on social capital include the 'social prescribing' movement, whereby general medical practices create formal links with community and voluntary organisations for the benefit of their patients.7,8 This is an area of growing interest and shows the potential for dental practices to link into such networks in an exciting, but relatively unexplored area.
References
Healy T, Côté S. The Well-Being of Nations - The Role of Human and Social Capital. Organisation for Economic Cooperation and Development. OECD Publications, 2001.
Putnam R. Bowling alone: the collapse and revival of American community. Simon and Schuster, 2000.
Szreter S, Woolcock M. Health by association? Social capital, social theory, and the political economy of public health. Int J Epidemiol 2004; 33: 650-667.
Gilbert K, Quinn S, Goodman R, Butler J, Wallace J. A meta-analysis of social capital and health: A case for needed research. J Health Psychol 2013; 18: 1385-1399.
Rouxel P L, Heilmann A, Aida J, Tsakos G, Watt R G. Social capital: Theory, evidence, and implications for oral health. Community Dent Oral Epidemiol 2015; 43: 97-105.
Rouxel P, Tsakos G, Demakakos P, Zaninotto P, Chandola T, Watt R G. Is Social Capital a Determinant of Oral Health among Older Adults? Findings from the English Longitudinal Study of Ageing. PLoS One 2015; 10: e0125557.
NHS. The NHS Long Term Plan. (2019). Available at https://www.longtermplan.nhs.uk/publication/nhs-long-term-plan/ (accessed July 2019).
Local Government Association. Just what the doctor ordered: Social prescribing - a guide for local authorities. 2016.
Author information
Authors and Affiliations
Rights and permissions
About this article

Cite this article
Moore, D. Does individual and neighbourhood social capital in early childhood influence oral health-related quality of life?. Evid Based Dent 20, 90–91 (2019). https://doi.org/10.1038/s41432-019-0050-5
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41432-019-0050-5
- Springer Nature Limited