
Abstract
Background
To describe the pattern of gestational weight gain (GWG), derive reference centiles for GWG specific to North Indian population, and to compare the weight gain across different periods of gestation with the INTERGROWTH–21st reference.
Methods
A prospective pregnancy (GARBH-Ini) cohort was initiated and followed between May 2015 and June 2019 in a district hospital, Gurguram, North India. GWG centile curves were modelled by Generalized Additive Models for Location, Scale and Shape method (n = 2844) and compared with INTERGROWTH-21st reference. The independent association of GWG with biological and social predictors was assessed using multivariable regression analysis.
Results
Percentiles (3rd, 10th, 50th, 90th and 97th) for each completed week from 18–40 weeks of gestation were derived from smoothed centile curves. The median GWG across pregnancy during specific antenatal visits was 1.29 at 18, 4.44 at 26, 5.8 at 30 and 9.06 kg at 40 weeks of gestation. Nearly 26% of participants had GWG < 10th centile at 18–20 weeks as per INTERGROWTH–21st reference and this increased to 45% at delivery. Significant predictors of GWG included maternal age, height, first trimester body mass index, parity, type of family, and use of clean fuel for cooking.
Conclusion
These GWG percentiles will serve as a useful reference, particularly during the WHO recommended antenatal visit schedule for optimum pregnancy outcomes, for clinicians and researchers. Multiple independent biological and social predictors of GWG suggest that single interventions are unlikely to bridge the gap between general Indian population and international references.
Similar content being viewed by others


Introduction
Maternal nutrition is a crucial determinant of foetal growth and can be quantified by body mass index (BMI) at conception and gestational weight gain. There is ambiguity in the interpretation of the term “gestational weight gain” in the current literature. It could be interpreted by purists as a change in gestational weight per unit time (e.g. per week of gestation) or velocity, or alternatively as an increase in maternal weight over and above the pre-pregnancy weight (distance charts). The latter is being used by several stakeholders including the Institute of Medicine guidelines [1,2,3]. While a consensus is needed to impart clarity to the definition and subsequent interpretation, we have followed the more widely used terminology to avoid confusion and to enable comparison with other references such as INTERGROWTH-21st. We have used the term “gestational weight gain” for the distance charts of gestational weight, and our use of the term “gestational weight velocity” refers to the growth or rate of change of weight over a period of time. The appositeness of GWG, in relation to international norms, can be evaluated through a comparison with Institute of Medicine-2009 (IOM-2009) or INTERGROWTH-21st references [2, 3]. IOM-2009 guidelines provide recommendations for adequate GWG for four different BMI categories but do not account for the variations due to the length of gestation. These guidelines apply to women from developed countries, and are not intended for use in low- and middle-income countries (LMICs), where women are substantially shorter or thinner, or adequate obstetric services are often not available [2]. Conventionally, in South Asian populations, GWG has been studied as total weight gain measured at the end of pregnancy and compared against IOM recommendations. This measure, while useful for comparing total GWG in a population, does not reflect the trajectories of GWG or the adequacy of weight gain during different periods of gestation, which would be possible with prospective longitudinal cohorts [4]. The INTERGROWTH–21st reference for GWG was developed recently using data from a population with nearly twenty exclusion criteria, namely no identifiable medical, nutritional, social or environmental risk factors associated with adverse maternal and perinatal outcomes during pregnancy; a subset (N ~448/3097 total subjects) of the study population was included from Central India [3]. This reference provides centiles for different periods of gestation, allowing an evaluation of GWG across different time points of pregnancy. There is a remarkable under-representation of information on how women from LMIC gain weight in comparison to global references and the predictors of GWG. Further, the centiles are applicable only to the subgroup of women with normal Body Mass Index (BMI).
We describe the GWG in a North Indian population of pregnant women visiting a district hospital and derive reference centiles. In addition, we compare the weight gain across different periods of gestation with INTERGROWTH–21st reference. We also identify and characterize the predictors of GWG in this population.
Methods
The GARBH–Ini cohort (interdisciplinary Group for Advanced Research on BirtH outcomes- DBT India Initiative) is a prospective observational cohort of pregnant women initiated in May 2015 at Gurugram Civil Hospital (GCH), Haryana, India. Women in this ongoing cohort are enrolled within 20 weeks of gestation and followed three times during pregnancy (18–20, 26–28 and 30–32 weeks), at delivery and once postpartum. The objectives of this ongoing study are to identify clinical, epidemiologic, genomic, epigenomic, proteomic, and microbial correlates; discover molecular-risk markers by using an integrative -omics approach, and generate a risk-prediction algorithm for preterm birth. The strengths of the cohort are accurate dating of pregnancy based on an ultrasonographic evaluation, detailed phenotypic description including clinical, epidemiological characteristics and documented birthweight [5].
Data from all the participants (N = 8235), enrolled between May 2015 and December 2020 (study period) in the GARBH–Ini cohort was considered. We included women who were enrolled <14 weeks of gestation (N = 4831) to ensure the most accurate correlate of pre-pregnancy weight. Since our participants were enrolled after conception, the first trimester weight was considered a surrogate of the preconception weight. We excluded women who had early pregnancy loss (n = 192) and stillbirths (n = 87). We required increments in maternal weight across pregnancy to construct smoothed centile curves and therefore included 2844 participants with at least four documented weights (Fig. 1).

The figure describes the selection of participants from GARBH-Ini cohort for modelling gestational weight gain trajectories.
The gestational age was ascertained at the time of enrolment by a dating ultrasound performed by a qualified radiologist using GE Voluson E8 Expert (General Electric Healthcare, Chicago, Illinois). Maternal weight was measured at enrolment and at four time points (18–20w, 26–28w, 30–32w and just before delivery) to the nearest 0.1 kg using a periodically calibrated Seca 769 adult weighing scale (Seca, Hamburg, Germany). The same weighing scale was used for all weights taken at GCH while a similar calibrated instrument was used in the referral hospital (Safdarjung Hospital). Maternal height (cm) was measured once at the time of enrolment using a calibrated stadiometer (Seca, Hamburg, Germany). Socio-demographic and clinical information at the time of enrolment and during follow-up visits was collected using questionnaires that followed standard protocols. All data were collected by trained study nurses under the direct supervision of medically qualified research officers using the standard operating protocols. The details of the variables collected and the processes are described in detail elsewhere [5]. The measurement processes were evaluated periodically by quality control exercises and errors were within acceptable limits [6].
Statistical analysis
GWG for a given gestational age was calculated as a difference between weight measured at that gestational age and weight at the time of enrolment. Maternal weight (kg), height (cm), and the maternal BMI (weight in kg/height in m2) were considered as continuous variables. BMI was also categorized by severity as underweight (<18.5), normal weight (18.5–24.9), overweight (25–29.9), and obese (≥ 30). Sociodemographic, clinical characteristics at enrolment were summarized as median (interquartile range; IQR) for continuous and as number (percentage) for categorical variables.
Weight gain from 18 to 40 weeks of gestation was modelled as a nonlinear function of gestational age using GAMLSS – Generalized Additive Models for Location, Scale and Shape method [7]. Specifically, the mean weight gain, nu and sigma parameters of the Box-Cox Power Exponential distribution were modelled against gestational age using cubic splines with five degrees of freedom. Smoothed centiles of GWG by gestational age were constructed and the goodness of fit of each model was assessed using quantile–quantile plots of residuals, comparing empirical to the fitted centiles and plot of fitted z–scores across gestational ages (Fig. S1). The weight gain across different time periods of pregnancy was compared between the participants of this study and INTERGROWTH–21st reference by superimposing the smoothed centile curves of GARBH–Ini participants and the INTERGROWTH–21st reference. The maternal weight gain was also compared for a subset of participants without any obvious pregnancy complications who were selected using exclusion criteria similar to INTERGROWTH–21st selection criteria (identified as low-risk population) [8]. The proportions of participants who gained weight < 10th, 10–50th, and >90th centile at different periods of gestation were tabulated for the unselected and low-risk populations.
The predictors of gestational weight gain were identified using a multivariable regression analysis with GWG as the dependent variable and candidate predictors as independent variables. The candidate predictors, their definitions and variable handling and coding are presented in Table S1. We compared the mean GWG in different categories of first trimester BMI using ANOVA as applicable. All analyses were performed in R programming language 3.6.3, version using the packages gamlss v5.1–6 for longitudinal modelling and R base packages for statistical analyses.
Written informed consent was obtained from all study participants. For an illiterate woman, details of the study were explained in the presence of a literate impartial witness; a verbal consent and a thumb impression were taken from her along with the signature of a witness. The study was approved by the Institutional Ethics Committees of Translational Health Science and Technology Institute, Faridabad; Civil Hospital, Gurugram; Safdarjung Hospital, New Delhi.
Results
The detailed sociodemographic and clinical characteristics of the included participants are summarized in Table S2. The median age of the participants was 23 years (IQR 21, 26), with 27% being underweight and 14% overweight or obese. The median height of the participants was 153 cm (IQR 149.1–156.7). The participants largely belonged to the lower socio-economic strata (44%) with less than 1% being classified as upper class [9]. More than half (51%) of the participants were primiparous. Exposure to second-hand tobacco smoke, documented on direct questioning, was prevalent in 20 and 8% were exposed to smoke from using biomass fuel for cooking. The median gestational age at enrolment into the study when the first measurement of weight was made was 10.1 weeks (IQR 8–12.1 weeks).
The distribution of GWG across different gestational ages is shown in Table S3. The smoothed centile curves showed that the median GWG (kg) across pregnancy during specific antenatal visits was 1.29 at 18, 4.44 at 26, 5.8 at 30 and 9.06 kg at 40 weeks of gestation. The variation in cumulative GWG between individual participants was less in early pregnancy (18 weeks: IQR 0.18–2.49) but widened as the pregnancy progressed (40 weeks: IQR 6.78–11.51) (Table S3 and Fig. 2). The longitudinal evaluation of GWG, described as gestational weight velocity estimates between the different gestational age windows were derived and tabulated in Table S4. As anticipated, the GWG was highest during the third trimester (mean GWG: 3.28 kg), followed by the second trimester (mean GWG: 3.04 kg). The GWG centiles across pregnancy were derived separately for the underweight, normal and overweight/obese categories of pregnant women. There was a trend of decreasing gestational weight gain from underweight category to normal to overweight/obese category (p < 0.001) across all gestational ages, which was more evident in early pregnancy than at later gestational ages. At 18 weeks, the median GWG for three categories was 1.86, 1.16 and 0.66 kg, respectively while at 40 weeks it was 10.13, 9.45 and 8.48 kg (Table 1, Fig. 3 and Table S5). The World Health Organization has recommended an eight-visit schedule during the antenatal period for optimum pregnancy outcomes [10]. To provide a population-specific reference for these recommended windows, we derived the 10th, 50th, and 90th centile cut-offs of GWG from our study population (Table S6).

A Smoothed centile curves at 3rd, 10th, 50th, 90th, and 97th centiles for gestational weight gain (maternal weight above pre-pregnancy weight) in the study population, GARBH-Ini cohort (n = 2844); B Comparison of patterns of gestational weight gain of the study population with INTERGROWTH-21st reference (n- 2844); C Smoothed centile curves at 3rd, 10th, 50th, 90th, and 97th centiles for gestational weight gain in the low-risk population, GARBH-Ini cohort (n = 200); D Comparison of patterns of gestational weight gain of the GARBH-Ini low-risk population with INTERGROWTH-21st reference (n = 200). The smoothed centiles for the unselected and the low-risk population of GARBH-Ini cohort (A and C) were constructed by Generalized Additive Models for Location, Scale and Shape method. These centile curves were superimposed on the curves generated using the INTERGROWTH-21st reference.

The BMI of participants were categorised in to three classes using the 18.5 and 25 as cut-offs and the weight gain trajectories for these categories are plotted in panels a, b, and c. The smoothed centiles were constructed by Generalized Additive Models for Location, Scale and Shape.
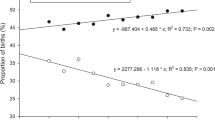
In comparison to the INTERGROWTH–21st reference, the study participants gained less weight during early pregnancy (mean difference in weight at 18 weeks: 1.41 kg (SD: 0.5)); this absolute difference increased as the pregnancy progressed (mean difference at 40 weeks: 4.57 kg (SD: 1.3)) (N = 2844) (Fig. 2). Thus 26% of study participants had GWG < 10th centile at 18–20 weeks as per INTERGROWTH–21st reference and this proportion increased progressively across pregnancy to reach 45% at parturition. Conversely, the proportion of women who gained weight more than 90th centile of INTERGROWTH–21st decreased from 5.2% to 0.6% across pregnancy (Table 2). Application of INTERGROWTH–21st selection criteria to identify women without evident pregnancy complications (low risk population) excluded 93.6% (2663/2844) participants (Table S7) in our cohort. The proportions of GWG < 10th centile at 18–20 weeks and at delivery were as high as the unselected population at 37 and 53%, respectively (Table 2, Fig. 2). Further, GWG in different windows of gestation in our unselected population was lower than that of the Indian subset of INTERGROWTH–21st participants with differences ranging between −0.22 (14–19 weeks) and 0.64 kg at 24–28 weeks of gestation. The GWG in the Indian subset of INTERGROWTH–21st was consistently lower than the total INTERGROWTH–21st population (Table 3).
The first trimester BMI (surrogate of preconception BMI) was independently associated with GWG (N = 2547). For every kg/m2 increase in first trimester BMI, there was 150 g reduction in GWG. Nulliparous women had the maximum GWG, which was 920 g lower for women with parity more than or equal to one. For every cm increase in height, the GWG increased by 60 g. GWG reduced by 70 grams for every year increase in maternal age. Women from nuclear families had 660 g higher weight gain across gestation than those from a joint or a three-generation family. Those who used safe fuel such as electricity or petroleum gas for cooking had 640 g higher GWG than those who used biomass fuel such as coal and wood (Table 4).
Discussion
Main findings and interpretation
We describe the GWG of pregnant women representing a semi-urban population visiting a district hospital in North India. We believe this data is novel because it is the first description of the weight gain of pregnant women across various gestations in an LMIC setting. Earlier studies have reported either total weight gain at the end of pregnancy or weight gain as cross-sectional observations at different time points of gestation [4]. The longitudinal nature of our data is well described by smoothed centile curves, that reflect weight gain during different periods of gestation. Documentation of reliable gestational age and rigorous quality control of anthropometry enhance confidence in the findings. INTERGROWTH–21st is the only description of GWG that includes, albeit small, Indian subset. Its purpose was to provide a standard derived from an apparently low-risk population, while our primary objective was to describe the distribution of GWG across pregnancy in an unselected population and present the centile cut-offs for different periods of gestation.
Pre-pregnancy BMI is a definitive determinant of GWG; we found that both total GWG and the trajectories are different in various categories of BMI. Although the pattern of decreasing GWG with increasing BMI categories has been reported, the differential between the underweight and normal BMI in our study is more than that reported in western datasets [11, 12]. This probably indicates better catchup in the underweight pregnant women in our setting. Considering this relationship of GWG with pre-pregnancy BMI, we customized the reference centiles for the three categories, namely, underweight, normal and overweight/obese. Further, from a practical clinical and public health perspective, we provide the centile cut-offs for the WHO recommended antenatal care visits for optimal care. These centile cut-offs will provide a reference to the healthcare provider to assess deviations in GWG across pregnancy for the women under their care.
Notably, pregnant women from our population gained less weight when compared with the INTERGROWTH–21st reference; this deficit increased as the pregnancy advanced with nearly 50% gaining less than 10th centile at 40 weeks. The slope of maternal weight curves seemed to be lower throughout the range of gestational age. There was no specific point in pregnancy where there was a distinct deviation in our population. Studies from other regions of our country, have reported prevalence of inadequate weight gain ranging from 66 to 82% but they had smaller sample sizes and used IOM-2009 reference for comparison [13,14,15,16,17]. The INTERGROWTH–21st uniquely provides centile cut-offs for all gestational ages from 14 to 40 weeks. Yet, it is not without limitation; the INTERGROWTH–21st reference was developed from normal BMI women with twenty other exclusions, making its direct application and interpretation to an unselected population challenging. We, therefore, identified a low-risk group in our cohort to make it similar to the INTERGROWTH–21st population and performed sub-analyses to understand the comparison better. Interestingly, the proportion of GWG < 10th centile was similar in both the low-risk and the unselected population. The observed difference in GWG between INTERGROWTH–21st population and ours may be attributed to multiple factors: disparities in the sociodemographic profile, differences in the baseline characteristics of the two populations such as height, and BMI, nutritional deficit, or inherent differences in our population from that of the western countries. We attempted to account for some of these differences by comparing the GWG in our unselected population with that of the Indian subset of INTERGROWTH–21st population. The differences noted in this analysis are interesting with a higher first trimester weight gain in our unselected population as compared to the INTERGROWTH–21st population. The reasons for these differences are worth exploring and would yield insights into the multifactorial nature of GWG.
Prominent independent determinants of GWG included maternal age, height, first trimester BMI, parity, type of family of the participant and cooking fuel. While maternal age, height, first trimester BMI and parity are well documented, our finding of type of family and cooking fuel as determinants of GWG is novel [18]. GWG was higher among women from nuclear families than those from a joint or three-generation family. This could indicate a possible constraint of resources in a large family. Use of biomass fuel has been shown to be associated with low birthweight [19, 20]. The association that we report between biomass fuel use and GWG may be an indication of its role in mediating the relationship between biomass fuel and birthweight. This needs to be evaluated in a separate analysis. One could also posit that biomass fuel usage is a surrogate for socioeconomic status and the association represented by biomass fuel with GWG could actually be the residual effect missed by traditional definitions like Modified Kuppuswamy Scale [9]. Social constructs like type of family are generally adjusted for in traditional GWG analyses and hence their association with GWG aren’t evaluated [21]. These social factors have their unique importance in public health outcomes, particularly those that are as multifactorial as GWG. Systematic evaluation is needed to understand how these social factors could influence GWG. Further, there is a need to identify women who are at risk of inadequate GWG due to nutritional deficits, through precise nutritional biomarkers. While improving nutrition by dietary interventions (ranging from simple dietary advice to energy-dense supplements) is an attractive proposition, randomized controlled trials must simultaneously evaluate the benefits and adverse effects (like gestational diabetes) of such nutritional interventions.
Limitations
The following limitations merit consideration while interpreting the results. The first trimester weight was considered as the surrogate for pre-pregnancy weight, as the GARBH–Ini cohort enrols participants during the antenatal period. Participants enrolled below 14 weeks of gestation (median GA at enrolment of 10.1 weeks) were included in this study. The sociodemographic and clinical characteristics were comparable between them and those who were excluded (Table S8) from this analysis. We believe that there will be no changes in the centile curves due to these limitations. Clinical outcomes such as neonatal anthropometry, perinatal morbidity and morbidity during infancy need to be evaluated for their association with GWG. We did not have enough sample size to assess the latter outcome as we could follow-up only a small subset of babies.
Most importantly, there is a need to have clarity on the terminology associated with gestational weight gain. What is traditionally referred to as GWG (the accrued weight gain over and above the pre-conceptional weight) may in fact should conceptually be termed as gestational weight and gestational weight gain be used for the weight velocity curves. Such a shift in terminology should keep in mind the challenges of interpretation, particularly in the clinical world, with respect to gestational weight gain and should emerge as a consensus. In order to make our data more meaningful, practical and have greater acceptance, we have retained the concept of accrued weight gain over and above the pre-conceptional weight as gestational weight gain (as defined elsewhere [3]). However, accepting the importance of weight velocity curves we have added a table of week-wise weight gain velocity. (Table S4)
Conclusion
From public health perspective, this study comprehensively describes GWG for the first time in a low-middle income population, provides population-specific reference centiles across pregnancy for different categories of pre-pregnancy BMI, and evaluates GWG trajectories in comparison to an international reference. The GWG distribution, described for the WHO recommended antenatal visit schedule for optimum pregnancy outcomes, provides an important reference for healthcare workers while assessing GWG of pregnant women under their care. Multiple independent biological and social predictors of GWG suggest that single interventions are unlikely to bridge the gap between general Indian population and international references.
Data availability
Data described in the manuscript will be made available upon request pending approval.
Code availability
Analysis code will be made available upon request with the objective of use.
References
Kominiarek MA, Peaceman AM. Gestational weight gain. Am J Obstet Gynecol. 2017;217(Dec):642–51.
Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines. Weight Gain During Pregnancy: Reexamining the Guidelines [Internet]. Rasmussen KM, Yaktine AL, editors. Washington (DC): National Academies Press (US); 2009 [cited 2019 Jul 25]. (The National Academies Collection: Reports funded by National Institutes of Health). Available from: http://www.ncbi.nlm.nih.gov/books/NBK32813/.
Cheikh Ismail L, Bishop DC, Pang R, Ohuma EO, Kac G, Abrams B, et al. Gestational weight gain standards based on women enrolled in the Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project: a prospective longitudinal cohort study. BMJ. 2016;i555.
Arora P, Tamber Aeri B. Gestational Weight Gain among Healthy Pregnant Women from Asia in Comparison with Institute of Medicine (IOM) Guidelines-2009: A Systematic Review. J Pregnancy. 2019;2019(Mar):1–10.
Bhatnagar S, Majumder PP, Salunke DM. A pregnancy cohort to study multidimensional correlates of preterm birth in india: study design, implementation, and baseline characteristics of the participants. Am J Epidemiol. 2019;188(Apr):621–31.
WHO MULTICENTRE GROWTH REFERENCE STUDY GROUP, Onis M. Reliability of anthropometric measurements in the WHO Multicentre Growth Reference Study: WHO Multicentre Growth Reference Study Group. Acta Paediatrica. 2007;95(Jan):38–46.
Stasinopoulos MD, Rigby RA, Heller GZ, Voudouris V, Bastiani FD. Flexible regression and smoothing: Using GAMLSS in R (1st ed.) 2017. Chapman and Hall/CRC, Boca Raton. p. 572. https://doi.org/10.1201/b21973.
Villar J, Altman D, Purwar M, Noble J, Knight H, Ruyan P, et al. The objectives, design and implementation of the INTERGROWTH-21st Project: The INTERGROWTH-21st Project. BJOG: Int J Obstet Gynaecol. 2013;120(Sep):9–26.
Mohd Saleem S. Modified Kuppuswamy socioeconomic scale updated for the year 2019. Indian J Forensic Community Med. 2019;6:1–3.
World Health Organization, editor. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: World Health Organization; 2016. 152 p.
[Standard values for the weight gain in pregnancy according to maternal height and weight] - PubMed [Internet]. [cited 2021 Feb 16]. Available from: https://pubmed.ncbi.nlm.nih.gov/17960517/.
Hutcheon JA, Platt RW, Abrams B, Himes KP, Simhan HN, Bodnar LM. A weight-gain-for-gestational-age z score chart for the assessment of maternal weight gain in pregnancy. Am J Clin Nutr. 2013;97:1062–7.
Bhavadharini B, Anjana R, Deepa M, Jayashree G, Nrutya S, Shobana M, et al. Gestational weight gain and pregnancy outcomes in relation to body mass index in Asian Indian women. Indian J Endocrinol Metab. 2017;21:588.
Mahanta L, Choudhury M, Devi A, Bhattacharya A. On the study of pre-pregnancy Body Mass Index (BMI) and weight gain as indicators of nutritional status of pregnant women belonging to low socio-economic category: a study from Assam. Indian J Community Med. 2015;40:198.
Misra A, Ray S, Patrikar S. A longitudinal study to determine association of various maternal factors with neonatal birth weight at a tertiary care hospital. Med J Armed Forces India. 2015;71:270–3.
Pal R, Maiti M, Roychoudhury B, Sanyal P, Chowdhury B. Association of pregestational BMI and antenatal weight gain with pregnancy outcome: a prospective observational cohort study. Int J Women’s Health Reprod Sci. 2017;5:37–40.
Radhakrishnan U, Kolar G, Nirmalan PK. Cross-sectional study of gestational weight gain and perinatal outcomes in pregnant women at a tertiary care center in southern India: Gestational weight gain. J Obstet Gynaecol Res. 2014;40:25–31.
Deputy NP, Sharma AJ, Kim SY, Hinkle SN. Prevalence and characteristics associated with gestational weight gain adequacy. Obstet Gynecol. 2015;125(Apr):773–81.
Amegah AK, Quansah R, Jaakkola JJK. Household air pollution from solid fuel use and risk of adverse pregnancy outcomes: a systematic review and meta-analysis of the empirical evidence. PLoS ONE. 2014;9:e113920. https://doi.org/10.1371/journal.pone.0113920.
Li X, Huang S, Jiao A, Yang X, Yun J, Wang Y, et al. Association between ambient fine particulate matter and preterm birth or term low birth weight: an updated systematic review and meta-analysis. Environ Pollut. 2017;227:596–605.
Siega-Riz AM, Bodnar LM, Stotland NE, Stang J. The Current Understanding of Gestational Weight Gain Among Women with Obesity and the Need for Future Research. NAM Perspectives [Internet]. 2020 Jan [cited 2020 Jul 16]; Available from: https://nam.edu/the-current-understanding-of-gestational-weight-gain-among-women-with-obesity-and-the-need-for-future-research.
Acknowledgements
Prof. MK Bhan will always be remembered reverently for his critical scientific and technical feedback. We greatly appreciate the extraordinary efforts from Drs. A Gambhir and S Sinha from DBT-India for supporting the GARBH–Ini program. We recognize the efforts of the research physicians, study nurses, clinical and laboratory technicians, field workers, internal quality improvement team, project and the data management team of GARBH–Ini cohort. This work was funded by the Department of Biotechnology, Ministry of Science and Technology, Govt. of India (BT/PR9983/MED/97/194/2013) and for some components of the biorepository by the Grand Challenges India – All Children Thriving Program (supported by the Programme Management Unit), Biotechnology Industry Research Assistance Council (BIRAC/GCI/0114/03/14–ACT).
Author information
Authors and Affiliations
Consortia
Contributions
SB, UCMN, NW, RT, KS, SM, NP, MJ, RB, PM, RT, and GARBH-Ini study team: conducted the GARBH–Ini cohort study and acquired the data; SB, RT, and BKD conceived the research questions and designed the analysis; BKD and RT analyzed data; SB, UCMN, HSS, SR, and RT guided and provided feedback on the analysis and interpretation of results; SB, RT, and BKD wrote the paper. All authors critically reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Thiruvengadam, R., Desiraju, B.K., Natchu, U.C.M. et al. Gestational weight gain trajectories in GARBH–Ini pregnancy cohort in North India and a comparative analysis with global references. Eur J Clin Nutr 76, 855–862 (2022). https://doi.org/10.1038/s41430-021-01040-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41430-021-01040-y
- Springer Nature Limited
This article is cited by
-
Should local references or global standards be used to assess gestational weight gain?
European Journal of Clinical Nutrition (2023)
-
The challenges in gestational weight gain monitoring in low and middle income settings
European Journal of Clinical Nutrition (2023)
-
Maternal weight latent trajectories and associations with adverse pregnancy outcomes using a smoothing mixture model
Scientific Reports (2023)
-
Pregnant women need local references for gestational weight gain – an editorial
European Journal of Clinical Nutrition (2022)