
Abstract
Background/objectives
While beverages are an important dietary source of water and some essential nutrients, consumption of sweet beverages has increasingly been linked to adverse health outcomes. Currently there is a paucity of longitudinal consumption data on beverage consumption in Australian children.
Subjects/methods
The Longitudinal Study of Australian Children has run biennially since 2004. Twenty four-hour recall data collected over 6 waves from the birth cohort (aged 0–1 year at baseline) was analysed and demographics were assessed for associations.
Results
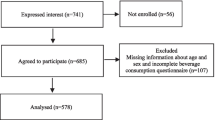
Five thousand one hundred and seven children participated at baseline, with a 71–90% retention of participants at each wave. Water consumption remained consistent with age over time, with more than 90% consuming more than one glass in the last 24-h. Proportions of fruit juice consumers decreased overall. Soft drink and cordial consumer proportions increased from 1% (0–1 year), to 28% (2 years) and 43% (10 years). Between 2 and 10 years, proportions of consumption of full-cream milk decreased by 8% and for skim milk this proportion increased by 51%. High proportions of consumers of soft drink/cordial was significantly associated with older children, males, children with a medical condition, living in a rural area, low socio-economic status and Indigenous Australians.
Conclusions
Water consumption remained consistently high across the ages, while fruit juice was commonly introduced into the diet early childhood. While proportions of fruit juice consumers decreased after the age of 2 years, proportions of soft drink consumers increased. The findings from this study should assist with surveillance data and inform policy and interventions aimed at reducing consumption of sweet beverages.
Similar content being viewed by others


Introduction
Sweet beverages have been linked to various adverse health outcomes and lack health benefits [1]. Consumption of sweet beverages (naturally sweet, sugar sweetened and artificially sweetened) is associated with overweight/obesity in Australian children, however the nature of this association is complex [2, 3]. A higher body mass index in Australian children has been associated with higher consumption of sweet beverages [4]. Sweet beverages consumption has been reported to increase risk for cardiometabolic conditions [5, 6] and for dental disease [7]. In Australia, the burden of disease attributed to sweet beverage consumption is unknown, although conditions such as obesity, diabetes and dental diseases contribute significant costs to Australian health care [8]. The Cancer Council Australia, Diabetes Australia and the National Heart Foundation of Australia recommend limiting consumption of sweet beverages to reduce their contribution to ill-health [9]. The Australian Dental Association also discourages sweet drink intake for prevention of oral ill-health [10].
In Australia, beverage sales data shows a decrease in sugar sweetened beverage sales and an increase in plain still water and artificially sweetened beverage sales over the past 15 years [11]. The per capita difference (in litres per person) between 1997 and 2011 was −10.8 for sugar sweetened beverages and +15.6 for non-sugar (including artificially sweetened) beverages [11]. Sales of artificially sweetened carbonated beverages, energy drinks, sports drinks, iced tea and still water all had a statistically significant increase [11]. While data from sales can be useful to show overall national population trends, it does not provide subgroup data such as consumption in children.
Currently, there is a lack of beverage consumption longitudinal data for Australian children. A critical element to inform any national nutrition policy is sufficient nationally representative dietary data to assist in setting policy directions, and to provide a feedback loop to show if policy actions are effective. For example, in the US, whole-of-population annual national surveys use comparable food composition data and collection methods, including multiple 24-h recalls [12] and two day food records [13]. Data from these surveys have shown trends in beverage consumption in US children aged 2–18 years with soft drink and fruit drinks increasing from 87.4 kcal (365kJ) per capita to 153.7 kcal (643kJ) per capita between 1977 and 2006 [13]. This study aimed to investigate consumption of beverages consumption in Australian children and to evaluate trends over time using the Longitudinal Study of Australian Children (LSAC).
Methods
Study participants
Growing up in Australia, the Longitudinal Study of Australian Children (LSAC) is a cross-sequential study that follows two cohorts of 5107 children initially aged 0–1 years (Birth cohort) and 4983 4–5 years olds (Kindergarten cohort) in 2004. Stratified sampling was used during recruitment to ensure representation of all Australian children and there is a 71–90% retention of participants at each wave. The LSAC is conducted every two years. Themes measured in the LSAC range and include demographics, relationships, learning and development, health and wellbeing [14]. The LSAC has been approved by the Australian Institute of Family Studies Ethics Committee, and all interviewers and researchers involved must comply with the Privacy Act 1988. All participants’ parent/guardians provided informed consent prior to participating.
Outcome measure
Data from the birth cohort’s parent’s interview were used in this study. Using a computer-assisted face-to-face interview, parents were asked about their child’s beverage consumption frequency (none, once or more than once) in the last 24-h. Unflavoured beverages measured in the LSAC were water, full cream milk, skim milk (including low fat, skim or soy milk). Sweet beverages measured were fruit juice; soft drink and cordial; and diet soft drink and diet cordial. In wave 1, the birth (B) cohort was not asked about frequency of consumption of all beverages.
Demographics included in this study were gender, Australian statistical geography standard, birth country, language spoken at home, Aboriginal Torres Strait Islander status (ABTSI), socio-economic status and any medical conditions of the child at the time of the questionnaire. Medical conditions were not asked in wave 4 of the study. Socio-economic status of participants was measured according to the relative socio-economic advantage and disadvantage by the socio-economic index for areas (SEIFA) [15]. SEIFA advantage/disadvantage scores were coded into deciles using data from the Australian Bureau of Statistics, with one indicating the most disadvantaged 10% of postcodes and 10 the 10% of least disadvantaged postcodes [15].
Statistical analysis
Frequency distributions of the demographics and consumption results were tabulated using IBM SPSS (version 24). The total proportion of the consumption frequency for each drink was calculated at each wave and plotted in line graphs. Frequency data is presented for waves 2 to 6 as wave 1 only asked consumption (yes/no) and not frequency.
For all beverages those who in the last-24-h reported once or more than once consumption frequency were categorised as consumers and those who had none in the last 24-h were categorised as non-consumers. For the consumers, those who consumed no more than one drink in the last 24-h were defined as moderate consumers. Those who consumed more than one drink in the last 24-h were defined as high consumers. Proportions of consumers were tested against demographics using chi-squared test for significant difference.
Results
Demographics
A total of 5107 children in the birth cohort participated in the LSAC. The demographics at wave 1 are presented in Table 1. At baseline, 51.1% were male, 4.5% identified as Indigenous, 89.2% spoke English at home, 99.6% were born in Australia and 66.1% lived in a major urban population. The demographics of this cohort is comparable to the general Australian population and has been tested for representativeness elsewhere [14]. The demographics of the study population at each subsequent wave have been describe elsewhere [14]
.
Consumption frequency
The consumption frequency of sweet beverages over time is presented in Figs. 1a–c. The proportion of fruit juice consumers was high in toddlers (2 years) with 39.5% (n = 1813) moderate and 28.9% (n = 1327) high consumers (Fig. 1a). Overall the consumption of fruit juice decreased over time (Fig. 1a). Across the waves high consumption of fruit juice decreased, whereas moderate consumption remained similar (Fig. 1a).

a–f. Consumption frequency of sweet and unflavoured beverages in Australian children 2006–2014 (n = 5107)
Proportions of consumers of soft drink/cordial increased with age, with the highest increase in consumption occurring at 10 years (Fig. 1b). At 2 years and 4 years, 27.8% (n = 1280) and 31.7% (n = 1261) were consuming soft drinks/cordial (Fig. 1b). The majority of children were non-consumers of diet soft drink/cordial between 2 and 8 years (Fig. 1c). There was an increase of consumption of diet soft drink at 10 years, with moderate consumers increasing by 11.8% and high consumers by 5.1% from the previous wave (Fig. 1c).
Water consumption remained consistent with age over time, with more than 90% consuming more than one glass of water in the last 24-h (Fig. 1d). The consumption frequency of unflavoured full cream milk and skim milk over time is presented in Figs. 1e–f. Consumption of full cream milk decreased with age (Fig. 1e). Proportions of consumers of full cream milk decreased from 82.7% (n = 3804) to 74.8% (n = 2687) between ages 2 and 10 years (Fig. 1e). There was a shift in frequency of consumption of full cream milk at age 10 with the proportion of high consumers, dropping below the proportion of moderate consumers (Fig. 1e). While full cream milk consumption decreased with age, skim milk consumption increased (Fig. 1f). The largest change in consumption of skim milk occurred between 8 and 10 years, where the proportion of consumers increased from 28.5% (n = 1154) to 62.3% (n = 2238) (Fig. 1f).
Consumption of beverages by demographics
The proportion of consumers of sweet beverages (fruit juice, soft drink/cordial and diet soft drink/cordial) by demographics over time is presented in Tables 2–4. Overall, consumption of fruit juice increased significantly from 38.1% (n = 1942) at 0–1 year to 60.5% (n = 2777) at age 2 years (Table 2). There was no significant difference in consumption proportions between genders, whereas at 0–1 year there were significantly higher proportions of consumers of fruit juice in areas outside of major urban populations, low SEIFA areas and those with a medical condition. In older children (8 and 10 years), proportions of consumers were higher for those born overseas. The proportion of fruit juice consumers was also greater for those who spoke another language at home and Indigenous Australians at 0–1, 2 and 6 years.
The proportions of soft drink/cordial consumers was higher in males (4, 8 and 10 years), children with medical conditions (0–1, 4 and 10 years), children born in Australia (8 years) and participants who spoke another language at home (8 and 10 years) (Table 3). Soft drink/cordial consumer proportions were significantly higher at all time points in participants who lived in areas outside of major urban populations, lived in low SEIFA areas or were Indigenous.
The proportions of diet soft drink/cordial consumers was were higher in males (10 years), children who lived in areas outside of major urban populations (6 and 10 years) or spoke another language at home (10 years) (Table 4). Indigenous Australians had significantly higher proportions of diet soft drink and cordial consumers across all ages except 6 years. Low and middle SEIFA areas had higher diet beverage consumer proportions than did high SEIFA areas at all ages.
The proportion of children consuming water was significantly higher in females (4, 6, 8 and 10 years), children without a medical condition (6 years), living in higher SEIFA areas (0–1, 2, 6 and 8 years) and non-Indigenous Australians (2, 4, 6, 8 and 10 years) (Supplementary Table 1).
Proportions of full cream milk consumers was significantly higher in males (6 years), rural areas (8 years), children without a medical condition (10 years), born in another country (8 and 10 years) and Indigenous (6 years) (Supplementary Table 2). Children who spoke another language other than English (2, 4, 6 and 8 years) and those living in low SEIFA areas (2, 6 and 8 years) had higher proportions of full cream milk consumers (Supplementary Table 2).
From ages 2 to 8 years, there were consistently higher proportion of skim milk consumers in females, children living in urban areas, high SEIFA areas, children who spoke English, and non-Indigenous Australians (Supplementary Table 3). Proportions of skim milk consumers were higher in children without a medical condition at age 4 and children born in Australia at age 8 (Supplementary Table 3).
Discussion
This study describes beverage consumption for a large national sample of Australian children. Water consumption remained consistent with age over time, with over 90% consumers. With increasing age, proportions of consumers of full cream milk decreased from 83 to 75% and skim milk increased from 29 to 62%. Fruit juice was introduced into the diet in infancy and toddler years for the majority of children with proportions of consumers increasing from 38 to 61% between 0–1 and 2 years. Proportions of consumers of fruit juice then decreased over time. Soft drink and cordial consumption was introduced into children’s diet at 2 years when proportions of consumers increased from 1 to 28%. More children began consuming diet beverages after 10 years.
In this study, sub-groups within Australian children had lower proportions of consumers of water and skim milk and higher sweet beverages. Exploring why these differences exist can inform policy and interventions to improve consumption behaviours in these groups. Currently in Australia, a range of implemented and proposed public health measures have been explored which aim to curb consumption of sweet beverages [16,17,18]. Factors such as access, price, portion size, social marketing and nutritional labelling have been identified as important influences on consumption and can be targeted to reduce intake in children [19, 20]. Being the main purchaser/supplier, parent/guardians are an important influence on children’s consumptions behaviours [2]. In this study, consumption of fruit juice and soft drink and cordial was occurring in early childhood [2 years] and previously implemented interventions such as beverage bans in schools would not have an impact on consumption in these children [21]. Lower levels of parental education have been shown previously to be an indicator of lower consumption of water and higher consumption of sweet beverages [7, 22, 23]. Dietary guidance for parents and guardians of Australian children through targeted education and interventions is needed to reduce frequency of consumption of beverages (with no or minimal nutritional value) and increase water consumption to reduce the associated burden of disease.
It is widely acknowledged in the public health literature that action beyond education campaigns is necessary in order to achieve the desired changes in consumption [24]. Australia is recognised as a leader in public health legislation and policy on tobacco control and parallels have been drawn between the challenges faced by tobacco and sugar control [25]. While there are a number of public health agencies and advocacy groups advocating for a broad range of strategies to reduce consumption of sweet beverages, action to date has been slow [26, 27]. Similar to the tobacco tax, a sugar tax is one proposed public health measure to reduce consumption of sweet beverages [28]. Economic modelling and online experimental data show that a tax would reduce consumption, and increasing community support and coverage in the media indicate there is growing public acceptance for a sugar tax in Australia [29,30,31,32].
The prevalence of consumption of all sweet beverages measured in this study was higher in children living in rural/remote areas and low socio-economic areas, which is in line with previous literature [4, 7, 33, 34]. The correlation between higher consumption rates in low SES and rural areas is perhaps due to easier access, availability or affordability of sweet beverages in these areas [35]. Additionally, poorer water quality and unreliable power to water pumping facilities has been cited as reasons for increased consumption of ready-to-drink sweet beverages [36, 37]. With higher incidence of obesity and dental diseases in low SES and rural/remote areas [38], targeted interventions to limit consumption in these vulnerable groups is essential.
Another group with health disparities and higher proportions of sweet beverages and full cream milk consumption are Indigenous Australians. Consumption rates were consistently higher across all ages measured in this sample of Australian children. Additionally, proportions of skim milk consumption was lower and full milk consumption higher. The current Australian Dietary Guidelines recommend limiting sweet beverage consumption, 2 serves of dairy daily and choosing reduced fat milk variations for children over 2 [39]. This highlights a lack of culturally appropriate information, nutrition knowledge and the low cost of sweet beverages in this population may influence consumption [37, 40]. Similarly, this study and the extant literature has observed a gender difference in consumption of sweet beverages, skim milk and water; and it might be plausible to also relate this outcome with knowledge differences between genders [41].
This study has a number of strengths and limitations. Strengths of this study include the large nationally representative and stratified random sample of Australian children. Another strength is the high (71–90%) retention of participants over the 10 years of data collection. Although this study has a number of strengths, it is not without limitations. First, the use of a parental report 24-h recall. Parents and carers often struggle with the estimation of quantities and usual patterns of beverage consumption in their children [40], and consumption may be underestimated if consumption is occurring away from parents’/guardians’ supervision or if the beverage is consumed less frequently than daily. Second, the use of broad beverage categories also meant that it was not possible to differentiate between soft drink and cordial consumption as these beverages was measured together in the 24-h recall. Third, the methods adopted in the LSAC allowed for neither the daily frequency nor quantities of beverages to be captured.
Monitoring consumption of beverages is crucial to inform nutrition policy including intervention strategies to curb consumption of beverages with no or minimal nutritional value and reduce the associated burden of disease. The quality of the available beverage consumption data would be strengthened by the use of a valid and reliable beverage assessment method like the BEVQ-15. The beverage questionnaire (BEVQ-15) is a beverage assessment method that has been recommended to assess adult population beverage consumption [42]. This questionnaire includes a range of non-alcoholic and alcoholic beverages and includes both the frequency and quantity of drink [42]. This questionnaire is also validated and reliable for use in children with simple modifications of this questionnaire including wording to suit parents and removal of alcoholic and uncommonly consumed beverages by children [43].
Conclusions
This study describes beverage consumption for a large national sample of Australian children. Water consumption remained consistently high amongst all ages of children, but was lowest in sub-groups who also had the highest proportions of sweet beverage consumption. Fruit juice was commonly introduced into the diet in infancy and toddlers with proportions of consumers increasing from 38 to 61% between 0–1 and 2 years. While proportions of fruit juice consumers decreased after the age of 2 years, proportions of soft drink consumers steadily increased after this age. Higher proportions of consumers of sweet beverages was significantly associated with older children, males, children with a medical condition, living in a rural area, living in a low socio-economic index area and Indigenous Australians. Monitoring consumption of beverages is crucial to inform nutrition policy including intervention strategies to curb consumption of beverages with no or minimal nutritional value and encourage water and skim milk consumption. The quality of the available beverage consumption data would be strengthened by the use of a valid and reliable beverage assessment methods which includes both the frequency and quantity of drink.
References
Curhan GC, Forman JP. Sugar-sweetened beverages and chronic disease. Kidney Int. 2010;77(7):569–70.
Ambrosini GL, Oddy WH, Huang RC, Mori TA, Beilin LJ, Jebb SA. Prospective associations between sugar-sweetened beverage intakes and cardiometabolic risk factors in adolescents. Am J Clin Nutr. 2013;98(2):327–34.
Millar L, Rowland B, Nichols M, Swinburn B, Bennett C, Skouteris H, et al. Relationship between raised BMI and sugar sweetened beverage and high fat food consumption among children. Obesity. 2014;22(5):E96–E103.
Clifton PM, Chan L, Moss CL, Miller MD, Cobiac L. Beverage intake and obesity in Australian children. Nutr Metab. 2011;8:87.
Wang M, Yu M, Fang L, Hu RY. Association between sugar‐sweetened beverages and type 2 diabetes: A meta‐analysis. J Diabetes Investig. 2015;6(3):360–6.
Levy-Marchal C, Arslanian S, Cutfield W, Sinaiko A, Druet C, Marcovecchio ML, et al. Insulin resistance in children: consensus, perspective, and future directions. J Clin Endo Meta. 2010;95(12):5189–98.
Armfield JM, Spencer JA, Roberts-Thomson KF, Plastow K. Water fluoridation and the association of sugar-sweetened beverage consumption and dental caries in Australian children. Am J Public Health. 2013;103(3):494–500.
Hector D, Rangan A, Louie J, Flood V, Gill T. Soft drinks, weight status and health: a review. Sydney: A NSW Centre for Public Health Nutrition (now known as Cluster of Public Health Nutrition, Prevention Research Collaboration, University of Sydney) Project for NSW Health; 2009.
Heart Foundation Cancer Council. Sugar-sweetened beverages consumption in Australia: The problem and what needs to be done. Cancer Council DA, Heart Foundation; 2012.
Australian Dental Association. Policy Statement 2.2.2-Community Oral Health Promotion: Diet & Nutrition; 2013.
Levy GS, Shrapnel WS. Quenching Australia’s thirst: a trend analysis of water‐based beverage sales from 1997 to 2011. Nutr Diet. 2014;71(3):193–200.
Centers for Disease Control and Prevention. Measuring Guides for the Dietary Recall Interview 2010. http://www.cdc.gov/nchs/nhanes/measuring_guides_dri/measuringguides.htm.
Popkin BM. Patterns of beverage use across the lifecycle. Physiol Behav. 2010;100(1):4–9.
Australian Institute of Family Studies. The longitudinal study of Australian Children Annual Statistical Report 2015. Melbourne: AIFS; 2016.
Australian Bureau of Statistics. Census of population and housing: Socio-Economic Indexes for Areas (SEIFA). Australia; 2011.
Capewell S. Sugar sweetened drinks should carry obesity warnings. BMJ. 2014;348:g3428.
Couch KA. Introduction: health policy and sugar-sweetened beverages. J Policy Anal Manage. 2011;30(3):644.
Mytton OT, Clarke D, Rayner M. Taxing unhealthy food and drinks to improve health. BMJ. 2012;344(7857):e2931.
Joint WHO/FAO Expert Consultation. Diet, Nutrition and the Prevention of Chronic Diseases. Geneva: WHO; 2003.
World Health Organization Europe. The challenge of obesity in the WHO European region and the strategies for response. In: Francesco Branca NHaLT, editor. Copenhagen, WHO Europe, 2007.
Education Queensland. Healthy Food and Drink Supply Strategy for Queensland Schools. Smart Choices. Brisbane: Queensland; 2007.2004
Orr N, Milat AJ, Lin M, Neville L, Develin L. Evaluation of the 2008 NSW water campaign. Health Promot J Austr. 2010;21(2):114–9.
Rangan AM, Flood VM, Denyer G, Webb K, Marks GB, Gill TP. Dairy consumption and diet quality in a sample of australian children. J Am Coll Nutr. 2012;31(3):185–93.
The World Health Organisation. The Ottawa Charter for Health Promotion. Ottawa: First International Conference on Health Promotion; 1986.
Moodie R, Stuckler D, Monteiro C, Sheron N, Neal B, Thamarangsi T, et al. Profits and pandemics: prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries. Lancet. 2013;381(9867):670–9.
Australian Government. National Tobacco Strategy 2012–2018. In: Intergovernmental Committee onDrugs TDoHaA, editor. Canberra; 2012.
Studdert DM, Flanders J, Mello MM. Searching for public health law’s sweet spot: the regulation of sugar-sweetened beverages. PLoS Med. 2015;12(7):e1001848.
MJA InSight. Put tax on sugared drinks on table Strawberry Hills, NSW: MJA; 2016. https://www.mja.com.au/insight/2016/13/put-tax-sugared-drinks-table.
Moretto N, Kendall E, Whitty J, Byrnes J, Hills AP, Gordon L, et al. Yes, the government should tax soft drinks: findings from a citizens’ jury in Australia. Int J Environ Res Public Health. 2014;11(3):2456–71.
Brownell KD, Farley T, Willett WC, Popkin BM, Chaloupka FJ, Thompson JW, et al. The public health and economic benefits of taxing sugar-sweetened beverages. N Engl J Med. 2009;361(16):1599–605.
Waterlander WE, Ni Mhurchu C, Steenhuis IH. Effects of a price increase on purchases of sugar sweetened beverages results randomized controlled trial appetite. Appetite. 2014;78:32–9.
Bollard T, Maubach N, Walker N, Ni Mhurchu C. Effects of plain packaging, warning labels, and taxes on young people’s predicted sugar-sweetened beverage preferences: an experimental study. Int J Behav Nutr Phys Act. 2016;13(1):95.
Riddell L, Beckford K, Grimes C. Australian children’s consumption of caffeinated-formulated beverages. Obes Rev. 2014;15:183.
Brimblecombe JK, Ferguson MM, Liberato SC, O’Dea K. Characteristics of the community-level diet of Aboriginal people in remote northern Australia. AMJ. 2013;198(7):380–4.
Han E, Powell LM. Consumption patterns of sugar sweetened beverages in the united states. J Acad Nutr Diet. 2013;113(1):43–53.
Bailie RS, Carson BE, McDonald EL. Water supply and sanitation in remote Indigenous communities‐priorities for health development. Aust NZJ Public Health. 2004;28(5):409–14.
Yuen E. Water consumption patterns in Australian Aboriginal communities: Murdoch University; 2005. Thesis published online: http://researchrepository.murdoch.edu.au/id/eprint/419/2/02Whole.pdf (Accessed: 01/02/2017)
Zander A, Sivaneswaran S, Skinner J, Byun R, Jalaludin B. Risk factors for dental caries in small rural and regional Australian communities. Rural Remote Health. 2013;13(3):2492.
National Health and Medical Research Council. Australian dietary guidelines. In: Australia Co, editor. Eat For Health. Canberra; 2013.
Jamieson LM, Bailie RS, Beneforti M, Koster CR, Spencer AJ. Dental self-care and dietary characteristics of remote-living Indigenous children. Rural Remote Health. 2006;6(2):503.
Commonwealth of Australia. Australian national children’s nutrition and physical activity survey. In: Department of Health and Ageing, editor; 2007.
Hedrick VE, Comber DL, Flack KD, Estabrooks PA, Savla J, Davy BM. Development of a brief questionnaire to assess habitual beverage intake: sugar-sweetened beverages and total beverage energy intake. J Am Diet Assoc. 2010;110(9):A26.
Lora KR, Davy B, Hedrick V, Ferris AM, Anderson MP, Wakefield D. Assessing initial validity and reliability of a beverage intake questionnaire in hispanic preschool-aged children. J Acad Nutr Diet. 2016;116(12):1951–60.
Acknowledgements
This study uses data from Growing Up in Australia, the Longitudinal Study of Australian Children (LSAC). The LSAC is conducted in partnership between the Department of Families, Housing, Community Services and Indigenous Affairs (FaHCSIA), the Australian Institute of Family Studies (AIFS) and the Australian Bureau of Statistics (ABS). The findings and views reported in this paper are those of the authors and should not be attributed to FaHCSIA, AIFS or the ABS.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Cockburn, N., Lalloo, R., Schubert, L. et al. Beverage consumption in Australian children. Eur J Clin Nutr 72, 401–409 (2018). https://doi.org/10.1038/s41430-017-0021-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41430-017-0021-x
- Springer Nature Limited
This article is cited by
-
Salivary characteristics and dental caries experience in remote Indigenous children in Australia: a cross-sectional study
BMC Oral Health (2019)
-
Factors associated with water consumption among children: a systematic review
International Journal of Behavioral Nutrition and Physical Activity (2019)