
Abstract
Background
Vegetable and fruit consumption may have a protective effect against several types of cancer. However, evidence suggesting that increased intake of vegetables and fruits, their subtypes, or the antioxidant nutrients they contain in abundance decreases the risk of bladder cancer is limited.
Methods
This study included 80,952 participants from the Japan Public Health Center-based Prospective Study, who responded to a food frequency questionnaire in a 5-year follow-up survey in 1995–1998 and were followed up until December 2015 to investigate the associations between intake of vegetables and fruits, their subtypes, or the antioxidant nutrients and bladder cancer risk using Cox proportional hazards regression models.
Results
Within 1,287,514 person-years of follow-up, 401 bladder cancer cases (307 men and 94 women) were diagnosed. No association was found between intake of total vegetable and fruit, total vegetable, total fruit, subtypes of vegetables and fruits, or antioxidant nutrients and bladder cancer risk in both men and women, even in the analyses conducted among men stratified by smoking status.
Conclusions
In this population, the consumption of vegetables and fruits was not associated with the risk of bladder cancer.
Similar content being viewed by others


Background
Bladder cancer is one of the top ten most common cancers worldwide, with ~550,000 new cases reported annually [1]. The global age-standardised incidence rate (ASR) is higher in men (9.6 per 100,000) than in women (2.4 per 100,000). The incidence of bladder cancer varies widely by region. The highest rates (ASR in men ≈ 20 per 100,000 per year and ASR in women ≈ 4.5 per 100,000 per year) were reported in Europe and North America, and approximately threefold lower rates were reported in Southeast Asia [1]. However, the incidence rates in Japan were higher than those in Southeast Asia (ASR in men 17.5 per 100,000 and ASR in women 3.7 per 100,000 in 2017) [2].
Given that some of the nutrients we take in from food are excreted in the urine, some foods and nutritional factors may contribute to bladder cancer risk [3]. Vegetables and fruits contain many antioxidants that potentially have anticarcinogenic properties, so consumption of vegetables and fruits may inhibit the development of several types of cancers. According to an expert panel of the World Cancer Research Fund (WCRF), the evidence suggesting that greater consumption of vegetables and fruits decreases the risk of bladder cancer is limited [4].
In particular, Japanese cohort studies have been conducted to investigate the association of intake of vegetables, fruits, or subtypes of vegetables or fruits with bladder cancer risk [5,6,7,8]. However, these studies showed inconsistent results and had several limitations. The food frequency questionnaire was fairly crude and simply assessed the food frequency to measure the dietary intake, without any information on portion size [5,6,7,8]. The reproducibility and validity of the questionnaire were not examined [5, 7]. Only the association of intakes of subtypes of vegetables or fruits with bladder cancer risk was examined, while that of total vegetables and fruits was not examined [6,7,8]. The Japan Public Health Center-based Prospective Study (JPHC Study) is a large-scale population-based prospective study in Japan to collect information on lifestyle habits from 140,420 people living in various parts of Japan and to clarify what lifestyle habits are related to the onset of diseases by tracking the onset of diseases for more than 20 years. Herein, we aimed to investigate the association between vegetable and fruit intake and bladder cancer risk in this large-scale population-based prospective study in Japan.
Methods
Study cohort and participants
The JPHC Study conducted a baseline survey in 140,420 registered residents aged 40–69 years in 11 public health centres (PHCs) (Cohort I; Iwate, Akita, Nagano, Tokyo, Okinawa–Chubu, Cohort II; Niigata, Ibaraki, Osaka, Kochi, Nagasaki and Okinawa–Miyako) from 1990 to 1993. Details regarding the study design are reported elsewhere [9].
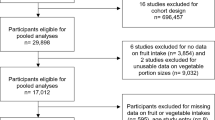
We enrolled participants who responded to a 5-year follow-up survey. We excluded participants registered in Tokyo (n = 7097) who did not have any information on cancer incidence and those registered in Osaka (n = 16,427) who had a different definition of the study population. Participants with foreign nationality (n = 52), who were relocated out of the study area before the date of response to the baseline survey (n = 171), with incorrect date of birth (n = 4), who were lost to follow-up (n = 17), and with duplicate registration (n = 12) were also excluded. After excluding those participants, 92,854 of 116,640 individuals (79.6%) aged 45 to 76 responded to the 5-year follow-up survey. We further excluded those who relocated out of the study areas before the follow-up start day (n = 1661) or with unknown relocation date (n = 32), who were diagnosed with any type of cancer before the start of follow-up (n = 1824) or had a history of cancer (n = 554), who had unknown (n = 1045) or extreme (lower and upper 2.5% percentile for each man and woman) intake of total energy (n = 4386), and who were ever smokers but did not indicate the number of cigarettes consumed per day (n = 2396). The final analytic cohort consisted of 37,061 men and 43,891 women.
Exposure definition
A self-administered food frequency questionnaire (FFQ) evaluated 138 food and beverage items consumed in the past year with three portion sizes (less than half, standard, and more than 1.5 times the standard portion size) and nine frequency categories (never, one to three times/month, one to two times/week, three to four times/week, five to six times/week, once/day, two to three times/day, four to six times/day and seven times/day). The frequency was multiplied by the relative portion size to calculate the daily consumption of each food items (g/day). The 30 vegetables and 16 fruits were categorised into total vegetables and fruits, total vegetables, green and yellow vegetables, cruciferous vegetables, green leafy vegetables, total fruits and citrus fruits. Details regarding the categories of vegetables and fruits are reported elsewhere [10, 11]. The daily consumption of antioxidant nutrients (retinol, α-carotene, β-carotene, lycopene, cryptoxanthin, vitamin C and vitamin E) was calculated using the Fifth Revised and Enlarged Edition of the Standard Tables of Food Composition in Japan [12].
To evaluate the validity and reproducibility of a self-administered FFQ, 215 participants (102 men and 113 women) from Cohort I and 350 participants (174 men and 176 women) from Cohort II participated in the validation studies voluntarily [13,14,15]. The validity of the FFQ was evaluated using 28- or 14-day dietary records as the gold standard. The FFQ was completed immediately or 3 months after the 28- or 14-day dietary records. The Spearman’s correlation coefficients between estimates based on the FFQ and dietary records in men of Cohort I, men of Cohort II, women of Cohort I, and women of Cohort II follow; 0.22, 0.44, 0.32 and 0.47 for total vegetables, 0.41, 0.55, 0.23 and 0.29 for total fruits, 0.37, 0.43, 0.39, and 0.49 for retinol, 0.51, 0.47, 0.48 and 0.53 for α-carotene, 0.40, 0.46, 0.33 and 0.48 for β-carotene, 0.43, 0.48, 0.29 and 0.31 for cryptoxanthin, 0.43, 0.48, 0.30 and 0.47 for vitamin C, respectively [13,14,15]. The reproducibility of the FFQ was evaluated by repeating the FFQ at a 1-year interval. The Spearman’s correlation coefficients in men of Cohort I, men of Cohort II, women of Cohort I and women of Cohort II follow; 0.62, 0.56, 0.53 and 0.59 for total vegetables, and 0.50, 0.57, 0.50 and 0.54 for total fruits [14, 16].
Follow-up and case identification
Participants were followed from the date of response to the 5-year follow-up survey until the date of any cancer diagnosis, death, emigration from Japan, or the end of follow-up (December 31, 2013, for Kochi and Nagasaki and December 31, 2015, for other PHC areas), whichever occurred first. Changes in residence status, including survival, were obtained annually through the residential registry in the municipality of each study area. In general, mortality data for residents included in the residential registry are sent to the Ministry of Health, Labour and Welfare and coded in the National Vital Statistics.
Cases of cancer were identified by active patient notification from the local major hospitals in the study areas and/or data linkage with the population-based cancer registries, with permission from each of the local governments. Death certificate information was used as a supplementary information source. Bladder cancer cases were defined by codes C67.0–67.9 of the International Classification of Diseases for Oncology, Third Edition. The morphology codes for the cases in the present study included 8000 (neoplasm), 8041 (small cell carcinoma), 8050 (papillary carcinoma), 8070 (squamous cell carcinoma), 8120 (transitional cell carcinoma), 8130 (papillary transitional cell carcinoma) and 8140 (adenocarcinoma). In all, 2.0% of bladder cancer cases in this study were ascertained from death certificates only. If two or more bladder cancers were diagnosed in one participant, the first bladder cancer was used for the analysis.
Statistical analysis
Cox proportional hazards model was used to calculate hazard ratios (HRs), 95% confidence intervals (CIs), and P trends for bladder cancer. Person-years of follow-up for each participant were calculated from the date of response to the 5-year follow-up survey and censored at the date of any cancer diagnosis, death, relocation out of the study area, or the end of follow-up (December 31, 2013, for Kochi and Nagasaki and December 31, 2015, for other PHC areas), whichever occurred first. The intake of vegetables, fruits and antioxidant nutrients was adjusted for total energy using the residual method, separately men and women [17], and categorised into quartiles with the lowest category as the reference. We conducted sex-specific evaluation because (1) there were sex differences in the intake of vegetables and fruits and the interaction between intake of vegetables and fruits and sex was significant (data not shown), (2) the incidence of bladder cancer differs greatly between males and females due to the large differences in the percentage of smokers and the amount of smoking in this cohort and (3) there is also substantial evidence that females present with more advanced disease stages at the primary diagnosis, which suggests that the development and detection of bladder cancer in males and females differs [18]. The multivariable analysis model was adjusted for age (continuous), study area (9 PHC areas), smoking status (never smoker, ever smoker, or unknown), duration of smoking (continuous), number of cigarettes per day (continuous), body mass index (<18.5, 18.5–25, 25–30 or >30 kg/m2), history of diabetes mellitus (yes/no), family history of any cancer (yes/no), alcohol intake (<1 day/month, 1–3 days/month, >1 day/week and <150 g/week, or >1 day/week and >150 g/week), coffee intake (0, <150, 150–300 or >300 ml/day), physical activity (quintile of metabolic equivalents), fish intake (quartile of energy-adjusted fish intake), red meat intake (quartile of energy-adjusted red meat intake) and supplement intake (yes/no). An analysis was also conducted stratified by smoking status (never smoker or ever smoker) among men to investigate whether vegetable and fruit intake affect the bladder cancer risk, which is a potential cause of oxidative stress and inflammation. In addition, a sensitivity analysis was performed by excluding participants diagnosed with bladder cancer within 3 years or 10 years after the date of response to the 5-year follow-up survey.
All P values reported were two-sided, and the significance level was set at P < 0.05. All statistical analyses were performed using Stata version 16.0 (Stata Corporation, College Station, TX, USA).
Results
Throughout the 1,287,514 person‐years (median; 17.1 years) of follow‐up, 401 participants (307 men and 94 women) were newly diagnosed with bladder cancer. The behaviour of neoplasms was determined in 399 participants, of whom 295 (74%) had malignant neoplasms and 104 (26%) had carcinoma in situ. Of the 401 participants, 352 (88%) had urothelial carcinoma, of whom 278 developed transitional cell carcinoma (M-8120) and 74 developed papillary transitional cell carcinoma (M-8130). In both men and women, participants who consumed more vegetables and fruits tended to be older and consume less red meat, alcohol, and coffee. They also have a lower prevalence of ever smokers, a lower number of cigarettes consumed per day, and a shorter duration of smoking. The prevalence of ever smokers among men was higher than that among women (Table 1).
The HRs and 95% CIs of bladder cancer incidence according to the quartiles of intake of vegetables and fruits, total vegetables, total fruits, and subgroups of vegetables or fruits are shown in Table 2. The crude incidence rate in men was 4.2 times higher than that in women (54.6 vs. 13.0 per 100,000 person-years). In the multivariable models, no significant association was observed in both men and women. In women, there was some evidence of a positive association when comparing the second quartile with the lowest quartile for vegetables [HR = 2.59 (95% CI: 1.36–4.93)], green-yellow vegetables [HR = 2.13 (95% CI: 1.13–4.03)], and cruciferous vegetables [HR = 2.08 (95% CI: 1.07–4.04)], although there was no association for the highest vs. the lowest and the trend were not significant. Excluding cases diagnosed with bladder cancer during the first 3 years or 10 years of follow-up did not change the results of the multivariable models.
Vegetables and fruits contain numerous antioxidants with potentially anticarcinogenic properties. We investigated the association of carotenoids, vitamin C, and vitamin E concentrated in vegetables and fruits with bladder cancer risk. The HRs and 95% CIs of bladder cancer incidence according to the quartiles of the antioxidants are shown in Table 3. In multivariable models, no significant association was observed in both men and women. In women, there was some evidence of a positive association when comparing the third quartile with the lowest quartile [HR = 1.86 (95% CI: 1.05–3.30)] for α-carotene and the second [HR = 2.54 (95% CI: 1.30–4.99)] and the third quartile [HR = 2.12 (95% CI: 1.06-4.24)] with the lowest quartile for β-carotene although the association for the highest vs. the lowest and the trend were not significant. Excluding cases diagnosed with bladder cancer during the first 3 years of follow-up did not change the results of the multivariable models. In the sensitivity analysis excluding cases diagnosed with bladder cancer during the first 10 years, there was a positive association when comparing the highest quartile with the lowest quartile for retinol [HR = 1.73 (95% CI: 1.11–2.69), P trend = 0.02] in men but no association in women [HR = 1.42 (95% CI: 0.72–2.82), P trend = 0.65].
To examine the potential residual confounding and effect modification of smoking, we conducted stratified analysis by smoking status in men. The crude incidence rate in ever smokers was 1.7 times higher than that in never smokers (61.5 vs. 35.3 per 100,000 person-years). In multivariable models, the trend for green leafy vegetables for never smokers was marginally significant although there was no association for the highest vs. the lowest [HR = 2.17 (95% CI: 0.95–4.92)]. No significant associations were observed in total vegetables and fruits, vegetables, fruits, or subtypes of vegetables or fruit except green leafy vegetables with bladder cancer risk in either never or ever male smokers. We did not detect an interaction between each of the vegetables, fruits, and smoking status (Table 4). There was also no association between intake of carotenoids such as α-carotene and β-carotene and incidence of bladder cancer in a stratified analysis by smoking status (Supplemental Table 1).
Discussion
This population-based prospective cohort study in Japan found no association between intake of total vegetable and fruit, total vegetable, total fruit, subtypes of vegetables and fruits, or antioxidant nutrients and bladder cancer risk in both men and women. To our knowledge, this is the first study of a large general Japanese population to assess the association between vegetable and fruit consumption and bladder cancer risk by estimating the food and nutrient intake using a detailed and validated food frequency questionnaire. The major strengths of this study are its large general population of participants and prospective study design. A high response rate to the survey and a high follow‐up rate are also strengths in minimising selection bias.
In the most recent report of WCRF/AICR, there was limited evidence to suggest that a high intake of fruits and vegetables reduces the risk of bladder cancer [4]. In previous studies, two meta-analyses of observational studies concluded that intake of vegetables and fruits was associated with a reduced risk of bladder cancer [19, 20]. However, other meta-analyses based on cohorts found no association between vegetable and fruit intake and bladder cancer risk [21, 22]. In a meta-analysis of cohort and case-control studies, there was an inverse association between fruit intake and the risk of bladder cancer. However, the association was not significant when the meta-analysis was restricted to cohort studies [23]. In this study, no association was found between the intake of vegetables and fruits and the risk of bladder cancer. This result is similar to that of previous cohort studies and meta-analyses [21, 22].
Contrary to our expectations, there was some evidence of an increased risk in the group with near median intakes of total vegetables, green-yellow vegetables, and cruciferous vegetables compared with the group with the lowest intake in women, although the P value for trend was not significant in this study. Each of these associations could be due to the confounding of unknown factors or measurement errors or a chance due to the small number of female bladder cancer cases. However, some results similar to ours have been reported. Park et al. [24] reported that total vegetables and yellow-orange vegetables (highest vs. lowest quartile) were inversely associated with the risk of invasive bladder cancer among women in the Multiethnic Cohort Study. However, the risk of invasive bladder cancer in the second quartile vs. the lowest quartile of intake of total vegetables, light green vegetables, dark green vegetables and cruciferous vegetables was slightly higher in women.
In a meta-analysis of cohort studies to assess the relationships of vegetable and fruit intake and bladder cancer risk [22], there was a slight increase in the risk of bladder cancer as total vegetable intake increased from 1 serving (80 g) to 2 servings (160 g) per day, and a nonlinear association was observed between a decrease in bladder cancer risk and total vegetable intake of more than 4 servings (320 g) per day in the nonlinear dose-response analysis. This trend was also observed for cruciferous vegetables, in which the risk of bladder cancer slightly increased as the intake of cruciferous vegetables increased from 1 to 3 servings per week (approximately 11.4–34.3 g per day) [22]. In this study, the median (interquartile range) intakes of total vegetables, green-yellow vegetables, or cruciferous vegetables for the lowest and second quartiles in women were 104 (79–123) and 170 (155–185), 36 (26–45) and 69 (61–76), or 26 (18–33) and 50 (44–55) g per day, respectively, which was close to the intake at which the increased risk was observed in the systematic review.
In this study, there was some evidence of an increased bladder cancer risk in the group with near median intakes of α-carotene and β-carotene. β-carotene is the most well-known carotenoid, known to quench singlet oxygen and a potent antioxidant [25]. Therefore, it was proposed that β-carotene may reduce the risk of cancer. A meta-analysis of cohort and case-control studies showed that a high intake of β-carotene was associated with a significantly lower risk of bladder cancer [26]. However, previous clinical trials failed to support these findings, and on the contrary, β-carotene supplementation marginally increased the risk of bladder cancer as reported in a meta-analysis of randomised controlled trials although the function of synthetic antioxidants may be different from that of natural antioxidants obtained from the diet [27].
Several studies have explained the biological mechanism underlying the harmful effects of beta-carotene [25, 27,28,29,30,31]. β-carotene has been reported to function as either an antioxidant or a prooxidant, depending on the environment in which it is present [31]. In the presence of chronic oxidative stress, such as smoking, it induces oxidative stress by generating reactive oxygen species or inhibiting the antioxidant system, which induces DNA damage [29]. In this study, the positive association found in women, but not in men, may be partially explained by the difference in bladder environment. There are sex differences in the anatomy of the bladder, urinary habits, hormone factors, and incidence of urinary tract infection and resultant cystitis [18, 32,33,34]. These differences in the bladder environment may alter an antioxidant or a prooxidant property of β-carotene, causing differences in its effects on the incidence of bladder cancer.
Smoking is a predominant risk factor for bladder cancer development. Since smokers suffer more oxidative damage from smoking than non-smokers, it can be hypothesised that antioxidants that reduce oxidative stress may derive more benefit from consuming fruits and vegetables [24, 35]. However, the effect of vegetables and fruits on bladder cancer risk among never and ever smokers was not consistent in previous cohort studies [24, 35,36,37,38,39]. In this study, we found no association between intake of vegetables and fruits and bladder cancer risk among never and ever male smokers and no significant interaction between smoking status and intake of vegetables and fruit.
There are several limitations to our study. First, although our study included a large population and had a long follow-up period, the statistical power was limited due to the small number of bladder cancer cases (307 men and 94 women). The limited sample size also made it difficult to look at tumour subtypes separately. Second, the intake of vegetables, fruits, and antioxidant nutrients was determined using a single point of self‐administered FFQ, and the correlation coefficients to assess validity were moderate, which may have resulted in misclassification of exposure categories. Third, the possibility of residual confounding by smoking cannot be ruled out, and further adjustment for smoking may be necessary. Smoking is a predominant risk factor for bladder cancer development. In this study, there was a difference in smoking status, amount of smoking, and duration of smoking between participants with low and high vegetable and fruit intake. Fourth, some potential confounders were not adjusted in the multivariable analysis model. Although occupational carcinogen exposure is a risk factor for bladder cancer [1], this information was not collected in this study and not adjusted in the multivariable analysis model.
In conclusion, we found no evidence that the consumption of total vegetables and fruits, vegetables, and fruits reduces the risk of bladder cancer in this population.
Data availability
For information on how to submit an application for gaining access to JPHC data and/or biospecimens, please follow the instructions at https://epi.ncc.go.jp/en/jphc/805/8155.html.
References
Richters A, Aben KKH, Kiemeney L. The global burden of urinary bladder cancer: an update. World J Urol. 2020;38:1895–904.
National Cancer Registry (Ministry of Health, Labour and Welfare), tabulated by Cancer Information Service, National Cancer Center. Japan National Cancer Registry in Japan (2016–2018). 2021. https://ganjoho.jp/reg_stat/statistics/data/dl/en.html.
Piyathilake C. Dietary factors associated with bladder cancer. Investig Clin Urol. 2016;57:S14–25.
Research WCRF/AICR. Continuous Update Project Report: Diet, Nutrition, Physical Activity and Bladder Cancer. Washington, DC: WCRF/AICR; 2018.
Grant EJ, Ozasa K, Preston DL, Suyama A, Shimizu Y, Sakata R, et al. Effects of radiation and lifestyle factors on risks of urothelial carcinoma in the life span study of atomic bomb survivors. Radiat Res. 2012;178:86–98.
Li WQ, Kuriyama S, Li Q, Nagai M, Hozawa A, Nishino Y, et al. Citrus consumption and cancer incidence: the Ohsaki cohort study. Int J Cancer. 2010;127:1913–22.
Nagano J, Kono S, Preston DL, Moriwaki H, Sharp GB, Koyama K, et al. Bladder-cancer incidence in relation to vegetable and fruit consumption: a prospective study of atomic-bomb survivors. Int J Cancer. 2000;86:132–8.
Sakauchi F, Mori M, Washio M, Watanabe Y, Ozasa K, Hayashi K, et al. Dietary habits and risk of urothelial cancer incidence in the JACC Study. J Epidemiol. 2005;15:S190–5.
Tsugane S, Sawada N. The JPHC study: design and some findings on the typical Japanese diet. Jpn J Clin Oncol. 2014;44:777–82.
Takachi R, Inoue M, Ishihara J, Kurahashi N, Iwasaki M, Sasazuki S, et al. Fruit and vegetable intake and risk of total cancer and cardiovascular disease: Japan Public Health Center-Based Prospective Study. Am J Epidemiol. 2008;167:59–70.
Makiuchi T, Sobue T, Kitamura T, Ishihara J, Sawada N, Iwasaki M, et al. The relationship between vegetable/fruit consumption and gallbladder/bile duct cancer: a population-based cohort study in Japan. Int J Cancer. 2017;140:1009–19.
The Council for Science and Technology MoE, Sports, Science and Technology, Japan. Standard tables of food composition in Japan, 5th revised and enlarged edn. Tokyo: National Printing Bureau; 2005.
Sasaki S, Kobayashi M, Tsugane S. Validity of a self-administered food frequency questionnaire used in the 5-year follow-up survey of the JPHC Study Cohort I: comparison with dietary records for food groups. J Epidemiol. 2003;13:S57–63.
Ishihara J, Sobue T, Yamamoto S, Yoshimi I, Sasaki S, Kobayashi M, et al. Validity and reproducibility of a self-administered food frequency questionnaire in the JPHC Study Cohort II: study design, participant profile and results in comparison with Cohort I. J Epidemiol. 2003;13:S134–47.
Ishihara J, Inoue M, Kobayashi M, Tanaka S, Yamamoto S, Iso H, et al. Impact of the revision of a nutrient database on the validity of a self-administered food frequency questionnaire (FFQ). J Epidemiol. 2006;16:107–16.
Sasaki S, Ishihara J, Tsugane S. Reproducibility of a self-administered food frequency questionnaire used in the 5-year follow-up survey of the JPHC Study Cohort I to assess food and nutrient intake. J Epidemiol. 2003;13:S115–24.
WC W. Nutritional epidemiology, 2nd edn. New York, NY: Oxford University Press; 1998.
Marks P, Soave A, Shariat SF, Fajkovic H, Fisch M, Rink M. Female with bladder cancer: what and why is there a difference? Transl Androl Urol. 2016;5:668–82.
Liu H, Wang XC, Hu GH, Guo ZF, Lai P, Xu L, et al. Fruit and vegetable consumption and risk of bladder cancer: an updated meta-analysis of observational studies. Eur J Cancer Prev. 2015;24:508–16.
Yao B, Yan Y, Ye X, Fang H, Xu H, Liu Y, et al. Intake of fruit and vegetables and risk of bladder cancer: a dose-response meta-analysis of observational studies. Cancer Causes Control. 2014;25:1645–58.
Xu C, Zeng XT, Liu TZ, Zhang C, Yang ZH, Li S, et al. Fruits and vegetables intake and risk of bladder cancer: a PRISMA-compliant systematic review and dose-response meta-analysis of prospective cohort studies. Medicine. 2015;94:e759.
Vieira AR, Vingeliene S, Chan DS, Aune D, Abar L, Navarro Rosenblatt D, et al. Fruits, vegetables, and bladder cancer risk: a systematic review and meta-analysis. Cancer Med. 2015;4:136–46.
Steinmaus CM, Nuñez S, Smith AH. Diet and bladder cancer: a meta-analysis of six dietary variables. Am J Epidemiol. 2000;151:693–702.
Park SY, Ollberding NJ, Woolcott CG, Wilkens LR, Henderson BE, Kolonel LN. Fruit and vegetable intakes are associated with lower risk of bladder cancer among women in the Multiethnic Cohort Study. J Nutr. 2013;143:1283–92.
Black HS, Boehm F, Edge R, Truscott TG. The Benefits and risks of certain dietary carotenoids that exhibit both anti- and pro-oxidative mechanisms-a comprehensive review. Antioxidants. 2020;9:264.
Jian-er, Tang, R-J, Wang, H Zhong, B Yu, Yu Chen. Vitamin A and risk of bladder cancer: a meta-analysis of epidemiological studies. World J Surg Oncol. 2014;12:1–9.
Park SJ, Myung SK, Lee Y, Lee YJ. Effects of vitamin and antioxidant supplements in prevention of bladder cancer: a meta-analysis of randomized controlled trials. J Korean Med Sci. 2017;32:628–35.
Palozza P. Prooxidant actions of carotenoids in biologic systems. Nutr Rev. 1998;56:257–65.
Palozza P. Can beta-carotene regulate cell growth by a redox mechanism? An answer from cultured cells. Biochim Biophys Acta. 2005;1740:215–21.
Carpenter KL. Beta-carotene: a colorful killer of cancer cells? A commentary on “ROS-triggered caspase 2 activation and feedback amplification loop in beta-carotene-induced apoptosis”. Free Radic Biol Med. 2006;41:418–21.
Cui Y, Lu Z, Bai L, Shi Z, Zhao WE, Zhao B. Beta-carotene induces apoptosis and up-regulates peroxisome proliferator-activated receptor gamma expression and reactive oxygen species production in MCF-7 cancer cells. Eur J Cancer. 2007;43:2590–601.
Dobruch J, Daneshmand S, Fisch M, Lotan Y, Noon AP, Resnick MJ, et al. Gender and bladder cancer: a collaborative review of etiology, biology, and outcomes. Eur Urol. 2016;69:300–10.
Aoe J, Ito Y, Fukui K, Nakayama M, Morishima T, Miyashiro I, et al. Long-term trends in sex difference in bladder cancer survival 1975-2009: a population-based study in Osaka, Japan. Cancer Med. 2020;9:7330–40.
Zaitsu M, Toyokawa S, Tonooka A, Nakamura F, Takeuchi T, Homma Y, et al. Sex differences in bladder cancer pathology and survival: analysis of a population-based cancer registry. Cancer Med. 2015;4:363–70.
Ros MM, Bueno-de-Mesquita HB, Kampman E, Büchner FL, Aben KK, Egevad L, et al. Fruit and vegetable consumption and risk of aggressive and non-aggressive urothelial cell carcinomas in the European Prospective Investigation into Cancer and Nutrition. Eur J Cancer. 2012;48:3267–77.
Zeegers MP, Goldbohm RA, van den Brandt PA. Consumption of vegetables and fruits and urothelial cancer incidence: a prospective study. Cancer Epidemiol Biomark Prev. 2001;10:1121–8.
Michaud DS, Pietinen P, Taylor PR, Virtanen M, Virtamo J, Albanes D. Intakes of fruits and vegetables, carotenoids and vitamins A, E, C in relation to the risk of bladder cancer in the ATBC cohort study. Br J Cancer. 2002;87:960–5.
Michaud DS, Spiegelman D, Clinton SK, Rimm EB, Willett WC, Giovannucci EL. Fruit and vegetable intake and incidence of bladder cancer in a male prospective cohort. J Natl Cancer Inst. 1999;91:605–13.
Büchner FL, Bueno-de-Mesquita HB, Ros MM, Kampman E, Egevad L, Overvad K, et al. Consumption of vegetables and fruit and the risk of bladder cancer in the European Prospective Investigation into Cancer and Nutrition. Int J Cancer. 2009;125:2643–51.
Acknowledgements
The members of the Japan Public Health Center-based Prospective Study are listed at the following site (as of April 2020): https://epi.ncc.go.jp/en/jphc/781/8510.html. We would like to thank the Akita, Iwate, Nagano and Okinawa Cancer Registries for providing their incidence data.
Funding
This study was supported by the National Cancer Center Research and Development Fund (since 2010), a Grant-in-Aid for Cancer Research from the Ministry of Health, Labor and Welfare of Japan (from 1989 to 2010) and MAFF Commissioned project study (JPJ009842).
Author information
Authors and Affiliations
Contributions
NN, TS and LZ designed the work that led to the submission. NS and TS acquired the data. All authors participated in the interpretation of data. NN carried out the statistical analyses and drafted the manuscript. TS, LZ, TK, NS, M Iwasaki, M Inoue, TY and ST critically revised the manuscript. ST is the principal investigator of the JPHC Study. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was conducted in compliance with the provisions of the Declaration of Helsinki. The study protocol was approved by the institutional review board of the National Cancer Center, Tokyo, Japan and by the Ethical Review Board of Osaka University, Osaka, Japan. The participants were informed of the study objectives, and those who completed the survey questionnaire were regarded as consenting to participation.
Consent to publish
Not applicable.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Narii, N., Sobue, T., Zha, L. et al. Vegetable and fruit intake and the risk of bladder cancer: Japan Public Health Center-based prospective study. Br J Cancer 126, 1647–1658 (2022). https://doi.org/10.1038/s41416-022-01739-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-022-01739-0
- Springer Nature Limited