
Abstract
Aims To examine the effect of the quality of root canal fillings and prosthetic restorations on the frequency of apical periodontitis (AP).
Methodology A total of 200 radiographs of 1,098 teeth with indirect restorations were selected. Each case was documented by age, sex, tooth location, tooth type, restoration type and presence of root canal treatment (RCT). Teeth were categorised as healthy or diseased considering periapical health. The quality of RCT and prosthetic restorations was categorised by radiographic and clinical examinations. Data were analysed using chi-squared test and logistic regression.
Results Inadequate prosthetic restorations were found to be less healthy than the adequate ones. Statistical significance was found in teeth with RCT, which had a higher rate of AP (15.8%). Root-filled teeth categorised as inadequately treated (24.1%) were significantly unhealthier than the adequately root-filled teeth. Teeth with inadequate prosthetic restorations and RCT had an increase in AP risk of 6.41 and 20.74 times, respectively (p <0.05).
Conclusions Results showed that AP risk was increased by both inadequate RCT and prosthetic restorations. Quality of RCT significantly affected periapical health more than the quality of prosthetic restorations. Not only radiographic but also clinical examination of restorations is required for successful evaluation.
Key points
-
Periapical health depends on both the quality of root canal fillings and prosthetic restorations.
-
Highlights that root canal filling quality has a greater effect on periapical health than prosthetic restoration quality.
-
Highlights the importance of clinical examination in addition to radiographic examination in the evaluation of prosthetic restoration quality.
Similar content being viewed by others



Introduction
Apical periodontitis (AP) is an inflammatory condition in the periradicular tissues that originates from diseases in the root canal system.1 This pathology has been noted to be widespread among societies of different countries.2,3 The results of longitudinal studies on root canal treatment (RCT) have been recorded with high success rates in teeth with no AP.4,5 As the prevalence of AP with an endodontic basis can create a public health issue in many countries, various epidemiological studies have been conducted to examine the prevalence and effect of endodontic treatments and the periapical status of endodontically treated teeth.6,7,8 The outcome of RCT is positively correlated with the root canal obturation quality, which maintains a hermetic seal against microbial ingress. However, coronal restoration quality may also affect the periapical status of endodontically treated teeth.7,8
Several studies examined the association between the type of restoration and periapical health.9,10,11 Previous studies found no statistically significant difference in the prevalence of AP in laboratory-fabricated crown restorations in comparison to direct restorations.10,12 Failure in the root canal obturation quality in teeth restored with indirect or direct restorations may contribute to the difference in the findings. In some studies, coronal restoration quality was not assessed.9,11,13
In recent years, the periapical index (PAI), which was introduced by Ørstavik,14 has been the most agreed upon method to determine the periapical status in cross-sectional7,11 and clinical studies.15,16 Periapical status is one of the key factors in evaluating treatment success. A radiograph provides only static information of a dynamic process and a periapical lesion may be either increasing in size or healing.17 Previous studies demonstrated approximately two years is required to observe periapical changes on radiography after RCT.18 The present study can help to evaluate the treatment outcome, as the radiographic quality of root canal obturation and the clinical and radiographic qualities of coronal restorations and their relation to periapical health have not been examined previously in a Turkish subpopulation. This evaluation can help to determine whether improvement is needed in endodontic and prosthetic applications by clinicians.
In this study, the clinical examination aimed to improve the quality of evaluation of prosthetic restoration, considering this is a major limitation in previously published studies as some of them did not evaluate coronal restoration clinically. This study evaluated the frequency of AP in both endodontically treated and untreated teeth from a selected Turkish patient group, and assessed the association between the quality of root canal fillings and prosthetic restorations and the periapical health of these teeth.
Methodology
This study was approved by the Ethics Committee of Biruni University Institutional Review Board (2019/29-39).
Study population
The cases in this study were the patients who visited the Dental School of Biruni University for routine dental care from January 2019 to June 2019. An informed consent form was obtained from each patient. All the examined radiographs were taken in the first half of the year 2019 at the patients' first visits. The 200 patients who were 24 to 79 years old and fulfilling the inclusion criteria were included in the study. Inclusion criteria for patient selection were the following:
-
Recently taken periapical radiographs from the section of prosthetic restorations (for further diagnosis or patient-reported problems) in addition to panoramic radiographs
-
Patients with at least one ceramic restoration (crown, post-crown, bridge abutment and post-bridge abutment), regardless of their substructure
-
Having no dental treatment (RCT and prosthetic restoration) for at least two years.
Exclusion criteria were the following:
-
Teeth with no or temporary restorations
-
Teeth with apical surgeries
-
Teeth with endodontic-periodontal combined lesions.
Each case was recorded by age, sex, tooth location, tooth type, indirect restoration type and presence of root canal filling.
Radiographic assessment
The 1,098 teeth included in the study were radiographically examined for the presence of RCT, quality of the indirect restoration and periapical health. The quality of root canal obturation was also evaluated in endodontically treated teeth. Panoramic and digital periapical radiographs were taken by a dental radiologist using a Sirona Galileos panoramic x-ray unit (Sirona, Bensheim, Germany) and a phosphor plate radiography system (Dürr Dental, Bietigheim-Bissingen, Germany) using the parallel technique for standardisation, respectively. One experienced endodontist and one experienced prosthodontist observed the radiographs using the Picture Archiving and Communication Systems software version (1.1.1.6) for Windows 10 (Microsoft Corporation, Redmont, WA, USA) displayed on a 28-inch Samsung LU28H750UQMXUF monitor (Samsung Electronics, Seoul, South Korea) with a 3,840 x 2,160-pixel resolution. Before the assessment of the radiographic images, each observer participated in calibration training which included a series of 25 images that were not related to the study sample for calibration between observers. Cohen's kappa was used for inter-observer consensus, which corresponded to a very good agreement with the value of 0.88. Any difference in the radiographic assessment was resolved through a discussion until a consensus between the two observers was reached.
Endodontic treatment assessment
The endodontically treated teeth were classified in accordance with the radiographic assessment of the root canal obturation. Multi-rooted teeth were grouped by the root canal with the most inadequate obturation. Root canal obturations were categorised as either adequate or inadequate based on the European Society of Endodontology guidelines19 and the following criteria by Barrieshi-Nusair et al.:20
-
1.
Adequate root canal obturation: root canal obturations ending within 2 mm from the radiological apex with no visible voids and consistent tapers from the coronal to the apical part of the filling, with a good reflection of the canal shape with no iatrogenic errors (Fig 1)
Fig. 1 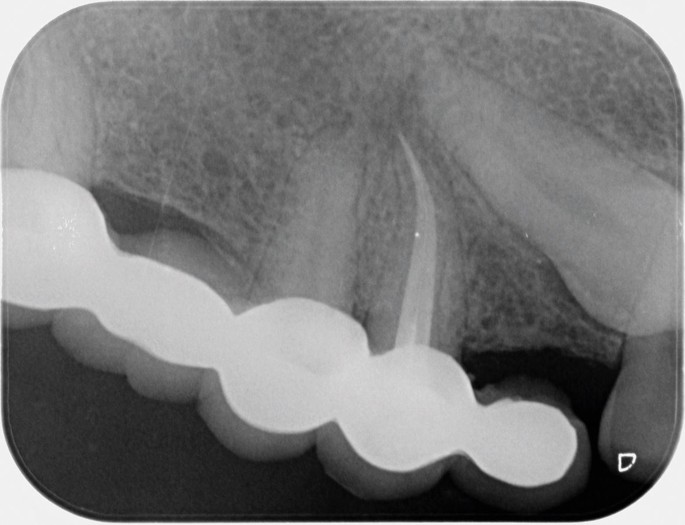
Maxillary first premolar with adequate RCT and adequate indirect restoration
-
2.
Inadequate root canal obturation: underfilled, overfilled, or poorly condensed root canal fillings and cases with inadequate preparation tapers and iatrogenic errors such as ledge, perforation and fractured instrument presence (Fig. 2).
Fig. 2 
Mandibular first premolar with inadequate RCT and inadequate indirect restoration


Indirect coronal restoration assessment
The quality of ceramic restorations was evaluated radiographically and clinically. The radiographic and clinical assessments were accomplished in accordance with the criteria by Tronstad et al.8 and Lundegren et al.,21 respectively. Intraoral evaluation was reported as follows:
-
1.
Adequate indirect restoration: radiographically intact ceramic restoration without any commentary on the clinical assessment record8,21 (Figures 1 and 3)
Fig. 3 
Intraoral image of adequate maxillary posterior bridge restoration and inadequate mandibular posterior bridge restoration
-
2.
Inadequate indirect restoration: ceramic restoration with overhangs, open margins or caries detected on radiograph or commentary on the clinical assessment record8,21 (Figures 2 and 3).

Periapical status assessment
Periapical status was assessed using the PAI introduced by Ørstavik et al.14The appearance of the apical third and periradicular tissues on radiographs was examined and the classification was made according to Strindberg22 as follows:
-
1.
Healthy teeth (PAI 1, 2): normal contour and width of the periodontal ligament space or widened periodontal ligament space in case of overfilled obturation22 (Fig. 2)
-
2.
Diseased teeth (PAI 3, 4, 5): any recognisable periapical radiolucency22 (Fig. 3).
Teeth with multiple roots were categorised with regards to the root with the worst assessment.
Statistical analysis
The data were analysed with the IBM SPSS Statistics 22 (IBM SPSS, Turkey) programme. Chi-squared test, Fisher's exact chi-squared test and continuity (Yates's) correction were used to analyse the differences between the data groups. Logistic regression analysis was performed for the multivariate analysis. The level of statistical significance was set to 5% (p <0.05).
Results
The 1,098 teeth of the 200 patients were examined in this study. Among the patients, 110 (55%) were women and 90 (45%) were men. The age range was 24-79 years and the average age band was 47.67 + 11.68. The study parameters according to sex, age, tooth location, tooth type, restoration type, quality of prosthetic restoration, presence of RCT, quality of RCT and periapical health status are shown in Table 1.
In terms of sex, the presence of AP was not found to be statistically significant (p >0.05). With regards to age groups, periapical pathosis (13.5%) was significantly higher in the cases of the 40-49 age range (p = 0.002; p <0.05), with an increased AP risk of 1.94 times. In the 60-69 and 70-79 age groups, periapical pathosis was found to be statistically lower than that in the other age groups (p <0.05). Regarding the effect of types of restorations on periapical health, there was no statistical significance between both crowns and bridge abutments and restorations with posts and no posts (p >0.05). Considering quality of restoration on periapical health, the inadequate prosthetic restorations were found to be less healthy than the adequate ones (p = 0.003; p <0.05), with an increased AP risk of 2.21 times. Teeth with RCT had a statistically higher rate of AP (15.8%), with an increased AP risk of 2.59 times (p <0.001) (Table 1). In terms of quality of RCT, inadequately root-filled teeth (24.1%) were significantly unhealthier than the adequately root-filled teeth (p <0.001), with an increased AP risk of 15.55 times (Table 1).
The results of the backward stepwise logistic regression analysis are presented in Table 2. According to this analysis, teeth with inadequate prosthetic restorations and RCT had an increase in AP risk of 6.41 and 20.74 times, respectively.
Restoration quality in teeth with adequate RCT had no statistical significance on AP (p >0.05) (Table 3). On the other hand, endodontically treated teeth with bridge abutment (15.8%) (OR = 2.44) were found to have significantly higher rates of AP than those without endodontic treatment (7.1%) (p <0.001) (Table 4).
Discussion
According to the radiographic evaluation of the prevalence of AP, 8.9% of the examined indirectly restored teeth were unhealthy regardless of RCT. Various studies from different countries showed a similar AP prevalence to that in this study, ranging from 2% to 18.9%.7,14,23 Conversely, Üreyen Kaya et al.16 found the prevalence of AP to be 1.2% in their study, which examined all the present teeth in the oral cavity independent from any restorations or RCT, thus explaining the lower AP prevalence. The patients who were within the age range of 40-49 years were found to have the most percentage of AP, and those in the age range of 60-69 years and 70-79 years were found to have a healthier periapex in our study. Although various studies found the highest AP prevalence in different age groups, the age of 40 and upwards had the highest risk of AP.12,24,25 The differences in the results of the studies can be explained by the variations in population selection, dental care habits and examination parameters.
Studies on coronal restoration quality and periapical health in teeth with RCT examined only radiographs to assess the quality of coronal restoration.7,11 The present study considered radiographic examination to be fundamental but not sufficient alone, as clinical examination was also performed to eliminate the constraint of the two-dimensional vision of radiographs. The radiographic and clinical qualities of coronal restorations and RCT affect periapical health.7,9,26 In the present study, the clinical status of indirect restorations was also examined to eliminate the limitations of radiographic analysis for the evaluation of marginal adaptation and coronal leakage. According to our results, inadequate restoration quality was statistically significant on AP by increasing the risk 2.21 times. Tronstad et al.8 reported that the coronal leakage caused by inadequate restorations was significantly related to the failure of RCT. According to a previous study, the quality of coronal restoration was more important in periapical health than the radiographic quality of RCT.9 However, recent studies noted that if the RCT was inadequate regardless of the adequacy of the coronal restoration, the risk of AP would still be high.3,4,22
The findings of the present study showed that both the quality of prosthetic restoration and RCT affect the periapical status of root canal-treated teeth. However, the risk of AP was approximately three times greater based on quality of RCT than the quality of prosthetic restoration. Moreover, the results were found to be similar to those of other studies:8,27,28 quality of RCT was the main factor in periapical health as the coronal restoration quality of teeth with adequate RCT had no statistical significance on AP. Song et al.29 reported that the qualities of both RCT and coronal restorations were equally effective on AP. The difference between these studies is that we examined only the indirect restorations in all types of teeth, whereas Song et al. examined both direct and indirect restorations in teeth with RCT. Thus, to prevent AP, a sufficiently sealed coronal restoration should be performed instantly after a quality RCT.
Many studies showed that AP could be underestimated when taking panoramic radiographs compared with periapical radiographs30,31 and this condition could have limited these studies. Thus, we observed both panoramic and periapical radiographs in the present study for a more detailed examination. Even though there are studies32,33 using cone beam computed tomography (CBCT) as an evaluation parameter, regarding artefacts in the imaging of CBCT with the presence of prosthetic restorations, we observed both panoramic and periapical radiographs and considered the most suitable evaluation method.
This study revealed the percentage of teeth with adequate root canal fillings to be 37.6%, whereas Segura-Egea et al.34 found that 34% of the RCT was adequate. Likewise, previous studies found the adequate root canal filling rate to be 30-40%.6,27 In the present study, the percentage of AP in teeth with inadequate fillings (24.1%) was statistically higher than that of AP in teeth with adequate fillings (2%) (p = 0.000; p <0.05), consistent with previous studies.34,35,36
In the present study, the frequency of AP in teeth with RCT was 2.59 times higher than that in teeth without RCT. Similarly, Kalender et al.15 showed that the percentage of AP with endodontic treatment was approximately four times higher than that without endodontic treatment. This finding can be explained by the higher percentage of the examined root canal fillings being inadequate.
The results demonstrated that root canal-filled teeth restored with bridge abutments tended to be 2.44 times more at risk of AP. Accordingly, the AP percentage in the present study was 15.8% in the bridge abutment teeth with RCT, whereas Gumru et al.7 found the AP percentage to be 46.5% given the same criteria. This difference can be explained by the sample size and study designs; the former used a prospective design and the latter a retrospective design.
One of the limitations of this study is that it is impossible to determine whether a periapical lesion is healing or not.10 In this manner, one of the inclusion criteria of the present study was patients who had no RCT for at least two years in order to assess periapical health more accurately. Considering that over half of the coronal restorations and RCTs were classified as inadequate, the operating dentist may be a contributing factor. Due to the fact that there was no solid information about the previous practitioners of the study patients, this may be considered as another limitation of the present study.
Conclusion
In conclusion, the results showed that AP risk was increased by both inadequate RCT and prosthetic restorations, and that the quality of RCT had significantly greater effect on periapical health than the quality of prosthetic restorations. Considerable effort must be spent to enhance the treatment quality to maintain apical health.
References
Chala S, Abouqal R, Abdallaoui F. Prevalence of apical periodontitis and factors associated with the periradicular status. Acta Odontol Scand 2011; 69: 355-359.
Hülsmann M. Epidemiology of post-treatment disease. Endod Topics 2016; 34: 42-63.
Pak J G, Fayazi S, White S N. Prevalence of periapical radiolucency and root canal treatment: a systematic review of cross-sectional studies. J Endod 2012; 38: 1170-1176.
Friedman S. Considerations and concepts of case selection in the management of post-treatment endodontic disease (treatment failure). Endod Topics 2002; 1: 54-78.
Ricucci D, Russo J, Rutberg M et al. A prospective cohort study of endodontic treatments of 1359 root canals: results after 5 years. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011; 112: 825-842.
Dugas N N, Lawrence H P, Teplitsky P E, Pharoah M J, Friedman S. Periapical health and treatment quality assessment of root-filled teeth in two Canadian populations. Int Endod J 2003; 36: 181-192.
Gumru B, Tarcin B, Iriboz E, Turkaydin D E, Unver T, Ovecoglu H S. Assessment of the periapical health of abutment teeth: A retrospective radiological study. Niger J Clin Pract 2015; 18: 472-476.
Tronstad L, Asbjørnsen K, Doving L, Paedersen I, Eriksen H M. Influence of coronal restorations on the periapical health of endodontically treated teeth. Endod Dent Traumatol 2000; 16: 218-221.
Dawson V S, Petersson K, Wolf E, Åkerman S. Periapical Status of Root-filled Teeth Restored with Composite, Amalgam, or Full Crown Restorations: A Cross-sectional Study of a Swedish Adult Population. J Endod 2016; 42: 1326-1333.
Hommez G M, Coppens C R, De Moor R J. Periapical health related to the quality of coronal restorations and root fillings. Int Endod J 2002; 35: 680-689.
Thampibul P, Jantarat J, Arayasantiparb R. Post-treatment apical periodontitis related to the technical quality of root fillings and restorations in Thai population. Aust Endod J 2019; 45: 163-170.
De Moor R J, Hommez G M, De Boever J G et al. Periapical health related to the quality of root canal treatment in a Belgian population. Int Endod J 2000; 33: 113-120.
Stassen I G, Hommez G M, De Bruyn H, De Moor R J. The relation between apical periodontitis and root-filled teeth in patients with periodontal treatment need. Int Endod J 2006; 39: 299-308.
Ørstavik D, Kerekes K, Eriksen H M. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endod Dent Traumatol 1986; 2: 20-34.
Kalender A, Orhan K, Aksoy U, Basmaci F, Er F, Alankus A. Influence of the quality of endodontic treatment and coronal restorations on the prevalence of apical periodontitis in a Turkish Cypriot population. Med Princ Pract 2013; 22: 173-177.
Ureyen Kaya B, Kececi A D, Guldas H E, Orhan H. A retrospective radiographic study of coronal-periapical status and root canal filling quality in a selected adult Turkish population. Med Princ Pract 2013; 22: 334-339.
Lupi-Pegurier L, Bertrand M-F, Muller-Bolla M, Rocca J P, Bolla M. Periapical status, prevalence and quality of endodontic treatment in an adult French population. Int Endod J 2002; 35: 690-697.
Alaçam T. Periapikal doku iyileşmesi ve başarı değerlendirmesi. In Alaçam T (ed) Endodonti. pp 865-878. Ankara: Tayfun Alaçam, 2012.
European Society of Endodontology. Consensus report of the European Society of Endodontology on quality guidelines for endodontic treatment. Int Endod J 1994; 27: 115-124.
Barrieshi-Nusair K M, Al-Omari M A, Al-Hiyasat A S. Radiographic technical quality of root canal treatment performed by dental students at the DentalTeaching Centre in Jordan. J Dent 2004; 32: 301-307.
Lundegren N, Axtelius B, Akerman S. Oral health in the adult population of Skane, Sweden: a clinical study. Acta Odontol Scand 2012; 70: 511-519.
Strindberg I Z. The dependence of the results of pulp therapy on certain factors. Acta Odontol Scand 1956; 14: 1-175.
De Moor R, Hommez G. The importance of apical and coronal leakage in the success or failure of endodontic treatment. Rev Belge Med Dent 2000; 55: 334-344.
Connert T, Truckenmüller M, ElAyouti A et al. Changes in periapical status, quality of root fillings and estimated endodontic treatment need in a similar urban German population 20 years later. Clin Oral Investig 2019; 23: 1373-1382.
Vengerfeldt V, Mandar R, Nguyen M S, Saukas S, Saag M. Apical periodontitis in southern Estonian population: prevalence and associations with quality of root canal fillings and coronal restorations. BMC Oral Health 2017; 17: 147-157.
Ricucci D, Grondahl K, Bergenholtz G. Periapical status of root-filled teeth exposed to the oral environment by loss of restoration or caries. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000; 90: 354-359.
Alkis H T, Kustarci A. Radiographic assessment of the relationship between root canal treatment quality, coronal restoration quality, and periapical status. Niger J Clin Pract 2019; 22: 1126-1131.
Siquera Jr J F, Rocas I N, Debelian G J et al. Profiling of root canal bacterial communities associated with chronic apical periodontitis from Brazilian and Norwegian subjects. J Endod 2008; 34: 1457-1461.
Song M, Park M, Lee C Y, Kim E. Periapical status related to the quality of coronal restorations and root fillings in a Korean population. J Endod 2014; 40: 182-186.
Takeshita W M, Chicarelli M, Iwaki L C. Comparison of diagnostic accuracy of root perforation, external resorption and fractures using cone-beam computed tomography, panoramic radiography and conventional & digital periapical radiography. Indian J Dent Res 2015; 26: 619-626.
Estrela C, Bueno M R, Leles C R et al. Accuracy of cone beam computed tomography and panoramic and periapical radiography for detection of apical periodontitis. J Endod 2008; 34: 273-279.
Nur B G, Ok E, Altunsoy M, Çolak M, Güngör E. Evaluation of technical quality and periapical health of root-filled teeth by using cone-beam CT. J App Oral Sci 2014; 22: 502-508.
Gomes A C, Nejaim Y, Amaro I V et al. Influence of Endodontic Treatment and Coronal Restoration on Status of Periapical Tissues: A Cone-beam Computed Tomographic Study. J Endod 2015; 41: 1614-1618.
Segura-Egea J J, Jiménez-Pinzón A, Poyato-Ferrera M, Velasco-Ortega E, Ríos-Santos J V. Periapical status and quality of root fillings and coronal restorations in an adult Spanish population. Int Endod J 2004; 37: 525-530.
Dugas N N, Lawrence H P, Teplitsky P E, Pharoah M J, Friedan S. Periapical health and treatment quality assessment of root-filled teeth in two Canadian populations. Int Endod J 2003; 36: 181-192.
Gündüz K, Avsever H, Orhan K, Demirkaya K. Cross-sectional evaluation of the periapical status as related to quality of root canal fillings and coronal restorations in a rural adult male population of Turkey. BMC Oral Health 2011; 20: 11-20.
Acknowledgements
This study received no financial support.
Author information
Authors and Affiliations
Contributions
All authors contributed equally to this work.
Corresponding author
Ethics declarations
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Sezgin, G., Kaplan, S., Kaplan, T. et al. Effect of prosthetic restorations and root canal fillings on periapical health in a selected patient group. Br Dent J 231, 127–132 (2021). https://doi.org/10.1038/s41415-021-3221-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-021-3221-7
- Springer Nature Limited