
Abstract
Objectives To define an expert Delphi consensus on when to intervene in the caries process and existing carious lesions.
Methods Non-systematic literature synthesis, expert Delphi consensus process and expert panel conference.
Results Lesion activity, cavitation and cleansability determine intervention thresholds. Inactive lesions do not require treatment (in some cases, restorations may be placed for form, function, aesthetics); active lesions do. Non-cavitated carious lesions should be managed non- or micro-invasively, as should most cavitated lesions which are cleansable. Cavitated lesions which are not cleansable usually require minimally invasive management. In specific circumstances, mixed interventions may be applicable. Occlusally, cavitated lesions confined to enamel/non-cavitated lesions extending radiographically into deep dentine may be exceptions. Proximally, cavitation is hard to assess tactile-visually. Most lesions extending radiographically into the middle/inner third of dentine are assumed to be cavitated. Those restricted to the enamel are not cavitated. For lesions extending radiographically into the outer third of dentine, cavitation is unlikely. These lesions should be managed as if they were non-cavitated unless otherwise indicated. Individual decisions should consider factors modifying these thresholds.
Conclusions Comprehensive diagnosis is the basis for systematic decision-making on when to intervene in the caries process and existing lesions.
Key points
-
Provides much needed guidance for the primary care practitioner to help in their management of dental caries.
-
Considers the quality of the evidence available to provide pragmatic guidelines for caries management interventions.
-
Comprehensive diagnosis is the basis for systematic decision-making on when to intervene in the caries process and existing lesions
Similar content being viewed by others


This manuscript has been modified with permission from Schwendicke F, Splieth C, Breschi L et al. Consensus statement: When to intervene in the caries process? Clin Oral Invest 2019; 23: 3691-3703, Springer. https://doi.org/10.1007/s00784-019-03058-w
Building an expert Delphi consensus on caries intervention thresholds
There is an ever-increasing number of strategies available to manage the caries process and its outcome, the carious lesion (ranging from very early signs and symptoms through to extended cavitated lesions with pulp involvement). These strategies are applied to avoid pain, prevent loss of tooth tissues or entire teeth, retain functionality and aesthetics. Daily, oral health practitioners are faced with the decision of 'if and when' to intervene using one of the many approaches available. This decision should be based on the available evidence, the characteristics, needs and wishes of the specific patient, the features of the tooth or carious lesion to be managed (as will be discussed below) and the operator's experience.1
Expert consensus can also support decision-making, especially if existing systematic evidence is limited or of too narrow scope. There have been recent attempts in dentistry and specifically cariology, to assist clinical decision-making by expert consensus; for example, on minimum intervention dentistry and carious tissue removal.2,3,4,5 The presented paper describes the consensus reached by an expert consensus panel who met in July 2018 in London, UK and used a structured online Delphi process before and after the meeting to systematically collate expert opinion and come to an agreement. The consensus focused specifically on when to intervene in the caries process and on existing carious lesions, rather than caries prevention. A detailed description of the methods can be found in Appendix 1, also including the guidance on conducting and reporting Delphi studies (CREDES).6
Firstly, the contemporary understanding of the caries process and the characteristics of carious lesions will be described. Secondly, the different levels of interventions will be presented and brief examples given. Thirdly, factors determining the decision of when to intervene will be outlined. Finally, consensus recommendations, which emerged from a 2-round Delphi process and a consensus conference involving a panel of more than 20 international experts, will be presented. The panel comprised members of the European Organisation for Caries Research (ORCA) and delegates of the European Federation of Conservative Dentistry (EFCD) and international experts from around the world. Note that this document and the resulting consensus recommendations do not aim to update or replace existing (often broader) guidance. The consensus on minimum intervention dentistry, for example, discussed caries detection and risk assessment, remineralisation and other preventive measures, minimally invasive operative interventions and re-treatments.4 Instead, this document specifically aims to assist decision-making on when to intervene in the caries process and on existing carious lesions.
Dental caries and carious lesions
Dental caries is one of the most prevalent and ubiquitous non-communicable diseases affecting humankind today.7 It was first understood to be an infectious disease, requiring removal of all plaque (biofilm) from the teeth or from affected carious hard tissues (specific plaque hypothesis). This concept, whilst debated (that is, biofilm being cariogenic under certain conditions; non-specific plaque hypothesis), was later modified, suggesting that the mere presence of biofilm is not sufficient for the pathogenesis of caries, but that an overlapping interaction between the host/teeth, substrate and microbiota is needed. Despite being 'infected' (or contaminated) with cariogenic bacteria, a cavitated carious lesion will not develop without a cariogenic diet.8,9 Marsh [1994] introduced the ecological plaque theory. The microbial composition of the biofilm is stable unless 'environmental perturbations' occur which can affect microbial homeostasis, leading to dysbiosis.10,11 With respect to caries, diet (mainly free sugars), oral hygiene and salivary factors are the contributing drivers of dysbiosis, leading to a shift in the microbiota towards acidogenic and aciduric microorganisms. There are also wider influences on caries experience,12 but consideration of those is beyond our remit. The original composition of an individual's dental biofilm is influenced by both hereditary and environmental factors, but, as time goes on, the types and proportions of micro-organisms acquired early in life are modified by environmental influences.13 Currently, the extended ecological plaque hypothesis is accepted as an explanation of the pathogenesis of caries.14
This pathogenesis involves organic acids, the by-product of microbial metabolism of dietary free sugars. As the pH of the biofilm decreases, it reaches a point where the biofilm fluid at the surface of the tooth is under-saturated with respect to tooth mineral, and dissolution occurs to maintain equilibrium.15 Initially, the dissolution occurs at the surface of the tooth, but, if conditions persist, and the lesion becomes more extensive, mineral from deeper in the enamel (and subsequently dentine) will be lost. Caries has an indirect genetic component, with influencing factors including enamel quality and quantity, immune response, dietary preferences and salivary characteristics.16,17 In summary, dental caries is a disease characterised by a process of demineralisation of the dental hard tissues, caused by frequent free sugars exposure to the dental biofilm, which shifts the ecological balance towards a cariogenic dysbiosis. For dentine and root caries, cleavage of collagen by bacterial or mainly dentine enzymes follows early mineral loss and contributes to the loss of the hard tissue.18,19
Management of the caries process/carious lesions
The former management of the caries process and carious lesions was influenced by an understanding that caries was a purely infectious disease and could be managed invasively/restoratively by removing all demineralised and 'contaminated'/infected tissue. This was grounded in (1) a lack of understanding that the caries process and carious lesions are separate, but related; (2) the incorrect assumption that once a lesion had established and the tooth was 'infected', eradication of microbiota was needed; (3) the erroneous concept that lesion progression was inevitable; and, (4) the fact that the majority of carious lesions dentists encountered in the past were truly 'decayed', that is, cavitated dentine lesions. Therefore, the professional education of dental surgeons concentrated on mechanistic surgical procedures instead of that of dental physicians who manage the disease and patient as a whole. Remuneration systems incentivised such invasive/restorative therapies.20,21 Notably, the shift away from this approach was initiated decades ago, but consistent updated data from all over the globe demonstrates that it has not been fully adopted.22
Building on the evidence accrued over several decades, it is clear that (1) the caries process can be controlled by modifying the patient's caries risk/susceptibility, depending on his/her adherence to behavioural modifications and not only by intervening operatively on carious lesions, yet success/understanding of behavioural interventions on caries control has been limited;23 (2) the caries process and carious lesions can be managed without removing microorganisms, but by rebalancing the dysbiosis within the tooth surface biofilm and arresting those within the depths of the tissues; (3) active (progressing) lesions can be inactivated;24 (4) in many high-income countries the spectrum of carious lesions has been and is shifting, especially in younger people, as there are now more non-cavitated lesions being detected;25,26 and, (5) while dental education in some countries now involves the contemporary understanding of caries and its subsequent carious lesions, remuneration systems for oral healthcare delivery have largely not been adjusted accordingly (there may be exceptions, and admittedly the uptake of a more contemporary approach towards caries and carious lesions has improved slowly over the last three decades or so).
Hence, the conventional restorative/invasive approach towards managing the caries process and carious lesions is not grounded in current understanding of the disease and it is also not appropriate for managing the broad spectrum of lesions found in many individuals (from very early to large cavitated lesions). It should also be considered that subsequent interventions on restored teeth are often necessary.27,28,29 This is classically known as the 'restorative death spiral'.30,31,32 Given these alternative arguments, there is consensus that invasive/restorative interventions alone are not beneficial for managing the caries process and lesions in all situations. Instead, invasive/restorative interventions represent a late step in the management puzzle, repairing the gross tissue damage and restoring form, function, aesthetics and cleansability, thereby allowing the control of risk of future loss of function. Invasive strategies may also be used to approach acute carious lesions.26 Invasive/restorative interventions are an important and relevant tool, but they should be complemented by other (non- or micro-invasive) management strategies. These 'other' strategies aim to control the caries process and the activity of carious lesions (as will be discussed below). If they are successfully implemented, the presence of bacteria is no longer a problem, since the cariogenic activity and the resulting mineral loss from dental hard tissues can be controlled concomitantly. In order to implement these alternative approaches successfully, there needs to be clear communication between the oral healthcare professional team and the patient, with the latter appreciating their role in valuing and respecting their own oral health.20
Intervention strategies: levels of invasiveness
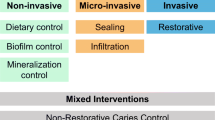
In the present document, we distinguish three levels of invasiveness to classify intervention strategies for 'treating' existing carious lesions. They are based on the degree of tissue removal associated with each strategy (Fig. 1):

Overview of different intervention levels and strategies. All strategies should be provided following the principles of minimally invasive dentistry
-
Non-invasive strategies do not remove dental hard tissue and involve, for example, fluorides and other chemical strategies for controlling mineral balance, biofilm control measures and dietary control
-
Micro-invasive strategies remove the dental hard tissue surface at the micrometre level, usually during an etching step, such as sealing or infiltration techniques
-
Minimally invasive strategies remove gross dental hard tissue, such as through use of hand excavators, rotary instruments or other devices. In most cases, this process is associated with the placement of restorations.
Note that some interventions can be regarded as 'mixed', not clearly falling into one of these categories. In the following sections, an overview of what falls into the three different levels of invasiveness will be offered. The individual details pertaining to each strategy will not be discussed, since the aim of this consensus paper was not to give recommendations on how to specifically intervene, but when.
Non-invasive interventions
To arrest existing lesions, several strategies are available, many of which have been developed originally for preventing the development of carious lesions and are now also applied for arresting lesions. These include diet control, biofilm control and mineralisation control.
Diet control
With free sugars being the driver of biofilm dysbiosis and cariogenic activity, both prevention and lesion arrest should, theoretically, be possible if sugar intake (mainly free sugars) is restricted/regulated.33 Sugar replacement may also be a valid option. Despite having biological plausibility, diet control measures, however, have been tested mainly for their preventive efficacy, as opposed to lesion arrest.
Biofilm control
Dental caries results from dysbiosis in the dental biofilm on a susceptible tooth surface. Therefore, restoring balance within that biofilm (through the use of mechanical biofilm control, antimicrobials, probiotics, etc.) has been advocated.11 Regular toothbrushing, interdental hygiene and antimicrobial strategies (including chlorhexidine and polyols) are the most common examples. Toothbrushing in combination with regular provision of fluoride has been investigated specifically for arresting existing active lesions. Most other therapies have been tested mainly for their preventive effect, not necessarily to arrest existing carious lesions.34
Mineralisation control
Fluoride has been shown to reduce dental caries occurrence consistently in both the primary and permanent dentitions, with the most current evidence strongly suggesting that its effect is primarily topical (that is, post-eruptive). Examples include dentifrices with fluoride concentrations above 1,000 ppm,35,36,37 5,000 ppm fluoride dentifrices,38,39,40,41 and fluoride rinses.42 Professionally-applied fluoride products, such as gels and varnishes, as well as silver fluoride products (such as silver diamine fluoride) have also been tested for arresting non-cavitated lesions.35,38,43,44 Moreover, a variety of products containing calcium in different forms (for example, calcium stabilised by casein derivatives, calcium sodium phosphosilicate, etc) or self-assembling peptides45 have been introduced to aid remineralisation. The evidence supporting the clinical efficacy of these products is currently limited.34,46,47
Micro-invasive interventions
There are two main strategies falling into this level of invasiveness; sealing and infiltration.
Sealing
A sealant places a diffusion barrier on the susceptible tooth surface and, hence, impedes acid diffusion into and mineral loss from the tooth tissues. It can also help re-contour the surface so aiding mechanical biofilm control. Sealing non-cavitated carious lesions on proximal, occlusal or smooth surfaces has been assessed in a range of studies.48,49,50 There has been a limited assessment of the sealing of cavitated surfaces49,50,51 and the current data imply a greater risk of sealant failure due to fracture or loss of retention, but further research needs to be undertaken to enable definitive conclusions to be drawn.51,52,53 The relevance of sealant loss for lesion progression may further differ between different sealant materials (that is, resin versus glass-ionomer cement-based sealants).54
Infiltration
Lesion infiltration involves the penetration of incipient enamel carious lesions by low-viscosity resins after removal of the surface layer (by etching with hydrochloric acid) and drying (using ethanol and air).55 A diffusion barrier is created within the dental hard tissue sub-surface, impeding acid diffusion into and mineral loss from the tooth tissue, so inactivating the lesion. There is some evidence supporting infiltration of non-cavitated proximal lesions.34,48 However, there is currently only one product available on the market for caries infiltration and nearly all related studies have been sponsored by the manufacturer of that product, with the associated potential for bias in the reported findings.
Mixed interventions
Non-restorative cavity control
Non-restorative cavity control (NRCC) aims to reinstate the cleansability of cavitated lesions by chiselling, cutting or grinding away overhanging, biofilm-trapping enamel or dentine.56 Subsequently, patients are encouraged to clean the opened 'saucerised' cavity and apply fluoride toothpaste/products (in addition to professional fluoride varnish application). Currently, the technique has been applied only in primary teeth or root surface lesions. Under optimal conditions, NRCC seems to be a feasible option to manage cavitated lesions, especially in uncooperative children who may not tolerate other treatments57,58,59,60 or dependent and systemically compromised older adult patients.
Hall technique
The Hall technique involves 'sealing' of cavitated carious lesions in primary teeth using preformed metal crowns without any tooth preparation. It combines the biological management of carious lesions (via sealing bacteria and depriving them of nutrition) and the restorative advantages of preformed metal crowns.58,61,62
Minimally invasive interventions
Minimally invasive operative caries management involves placement of a restoration after selective removal of carious tissue, done to create conditions for long-lasting restorations and maintaining the tooth-restoration complex. Modern bio-interactive adhesive materials have allowed for minimally invasive restorations that provide a seal and focus on preserving healthy and repairable/remineralisable tissue and maintaining pulp health. An International Caries Consensus Collaboration presented recommendations on terminology and on carious tissue removal and restorative management of cavitated carious lesions. These recommendations support less invasive carious lesion management, delaying entry to, and slowing down, the restorative cycle by preserving tooth tissue, being selective on tissue removal and retaining teeth long-term.5
Factors affecting caries intervention thresholds
A number of key factors help to determine caries intervention thresholds. These are activity, cavitation, and cleansability of the lesion.
Activity
The term 'lesion activity' reflects the ongoing mineral loss or gain of a lesion. It indicates how likely a lesion is to progress. An inactive (arrested) lesion may be considered as a 'scar' and does not require any treatment. In some cases, restorations might be placed for reasons of form, function and/or aesthetics. As discussed, restorations may also be provided in cases of pain to reduce pulp stress and improve symptoms. Lesion activity is often determined visually; tactile assessment should only be performed gently so as to not damage the surface, using a rounded/ball-ended explorer (forceful probing with a sharp dental explorer is not recommended). For root surfaces, gentle probing may be undertaken to determine the texture.63
Since there is currently no technology available that allows an objective longitudinal measurement of lesion activity, the following clinical signs can be used to estimate lesion activity: (1) the presence of biofilm covering the lesion may indicate activity, especially, in the presence of high and frequent consumption of sugars; (2) the condition of the gingiva (local gingivitis in proximity to the lesion) can also serve as a proxy measure to determine whether biofilm has been present over time; (3) lesion characteristics, such as texture, hardness and appearance. A smooth enamel lesion surface indicates inactivity, while rough surfaces may indicate activity. Colour-wise, a white chalky matt lesion colour may indicate activity, but shiny or dark lesions may indicate inactivity.63,64,65,66
Notably, not all clinical criteria will be always available, for example, in proximal surfaces or for micro-cavitated lesions. However, in many circumstances, one criterion or more will be assessable and may be complemented with (4) longitudinal recall data, if available (for example, via repeated radiographs, or those from fluorescence-assisted systems, visual scales, or clinical photographs). These can also be used for activity assessment. Lesion activity is the first main factor to decide intervention thresholds, although such evidence is limited and more research is strongly advocated.
Cavitation
Cavitated lesions are those with a surface breach that is clearly detectable to the naked eye or a rounded dental explorer. Often, this may also involve dentine exposure. Cavitation increases the likelihood of lesion progression,50,67 because the dental biofilm is protected from self-cleaning and oral hygiene procedures. Moreover, cavitation encourages a more rapid diffusion of acids and carbohydrates, as well as greater bacterial contamination of tissues. In cavitated lesions, the involved dentine is demineralised and the outer portion of the lesion is bacterially contaminated/infected.
A subgroup of cavitated lesions are the micro-cavitated lesions. Sometimes, magnification is needed to detect cavitation in these lesions. Micro-cavitated lesions can show enamel breakdown without visible dentine exposure.
Note that cavitation can be assessed tactile-visually on accessible smooth surfaces (buccal, lingual). Occlusally, their assessment is more complicated. Occlusal carious lesions which radiographically extend deep into the dentine (middle or inner dentine third, D2/3) are usually heavily bacterially contaminated and demineralised. These lesions may require a different management than lesions without such extensive dentine involvement.
On proximal surfaces, detecting cavitation using visual-tactile means is nearly impossible when adjacent teeth are present (except for clear cavitation in more extensive lesions). Orthodontic separators may be used to gain access over some days, but this is not practical in most settings. Hence, most clinicians will rely on further diagnostic aids, mainly bitewing radiography, to gauge the likelihood of cavitation. While radiographs seldom permit accurate detection of cavitation itself, the lesion depth serves as a proxy of how likely cavitation is; deeper radiographic lesions come with a higher chance of being cavitated. A number of studies have assessed the relationship between the radiographic lesion depth and the presence of cavitation. These have been summarised in a recent review.68 Lesions confined radiographically to the enamel (outer or inner enamel half, E1/E2) are seldom cavitated, while those into the middle or inner dentine third (D2/D3) are usually cavitated. Some of the lesions radiographically extending into the outer dentine third (D1) may be cavitated, others not. Further detection aids such as near-infrared light transillumination or fluorescence-based systems69 can be used to corroborate radiographic lesion depth assessment.
Cleansability
Cavitation is a major factor for deciding whether and how to intervene, because it serves as an indicator of cleansability and, as described, activity. Nevertheless, sometimes even cavitated lesions can be cleansable, for example in primary anterior teeth with open smooth surface lesions, or in root surface lesions.
There are further factors which can modify caries intervention thresholds: the patient's caries risk/susceptibility, age and the dentition.
Caries risk/susceptibility and behavioural adherence
The term caries risk/susceptibility refers to the chances of an individual developing new carious lesions in the future. There are a number of possible aspects to be integrated into caries susceptibility assessment, such as past caries experience (assuming past caries experience to be a robust indicator of risk factors on the behavioural and the genetic level) and factors directly or indirectly related to caries pathogenesis (diet, oral hygiene, saliva) or lesion development (fluoride intake). Past caries experience has been found to have a good predictive value,70 while most other factors have only moderate or low predictive value. Many further factors suggested for caries risk assessment (salivary buffering capacity, bacterial number/concentration in the saliva, to name but two) show limited predictive value.71 For root caries, the number of surfaces at risk (exposed roots) seems to be a useful robust parameter for risk assessment.72
There are some established caries risk/susceptibility assessment systems which integrate these factors and weight them. These systems have been found useful to predict coronal and root caries to some degree, but with limited generalisability.73,74,75
Caries susceptibility assessment helps to identify patient-specific factors, which are of value. These should be managed and re-evaluation performed regularly throughout any episode of care. If risk factor modification is not successful or longitudinal re-evaluation not possible, this should be taken into consideration in determining intervention thresholds.
Age
There are several unique considerations that are important in the oral health management of children's and older adults (or vulnerable groups with special needs).76 The oral health and behaviour of the carer has a marked influence on the oral health of younger children or other dependent individuals, such as the elderly and institutionalised individuals. The factors affecting patient behaviour in such groups, as in all patients, must be considered, that is capability, opportunity and motivation. Very young children may show only limited cooperation and behavioural adherence.77 In some of these individuals, sedation or general anaesthesia are needed to provide care. Interventional thresholds may be lowered and more invasive treatments chosen in some of these instances.
The dentition
The structure of primary teeth differs from that of permanent teeth. The enamel is thinner and slightly less mineralised. The pulp space is proportionally larger and the shape of the teeth is different. The contact areas of the molar teeth, especially between the mandibular molars, are flatter than permanent molars and premolars. This predisposes to carious lesions developing below the wider contact area, close to the gingival margin. Given this anatomy, conventional restorative approaches (including carious tissue removal and direct restorations) have higher risks of complications (more pulp exposure and restorative complications) in primary than permanent teeth.61,78 Moreover, visual-tactile lesion detection on proximal surfaces of primary teeth is difficult because of these wider contact areas.79 Also, and most importantly, primary teeth exfoliate. The time to exfoliation and the speed of progression of the carious lesion can influence the decision affecting treatment for a lesion. Pulp therapies for primary molars (especially those with necrotic pulp tissue) may be successful, but are technically demanding.80 In a few cases, removing primary molars and, if needed, maintaining the space may be a valid option to avoid pain or sepsis. In contrast, for permanent teeth, the overarching therapeutic aim is long-term retention of teeth in a functional, pain-free and depending on the location in the mouth, aesthetically acceptable condition. Any intervention threshold should consider these aspects on an individual patient basis.
When to intervene in the caries process?
Based on the contemporary understanding of the caries process, the available interventions and the factors determining or modifying intervention thresholds, all discussed in this article, the consensus group agreed on a number of recommendations for when to intervene non-invasively, micro-invasively or minimally invasively/restoratively in the caries process and for existing carious lesions. These recommendations were the subject of the Delphi process, with experts voting on the verbatim recommendations below.
The recommendations should be adapted to each individual patient and setting and need to be applied with each oral healthcare professional's individual expertise and practising context in mind. Also note that nearly all recommendations made are not based on strong empirical evidence, but mainly on expert opinion and experience. Hence, clinical judgment remains a key element in deciding the threshold for intervention. The recommendations are set out below, together with the level of agreement (mean values on a scale from 1 [do not agree at all] to 10 [fully agree] and standard deviations [SD]).
-
1.
Lesion activity should be assessed. An inactive (arrested) lesion is like a 'scar' and does not require any treatment, but should be reviewed. In some cases, restorations might be placed for reasons of form, function or aesthetics. An active lesion needs management (agreement 9.4, SD 1.1) (Fig. 2)
Fig. 2 
Factors involved in determining caries intervention thresholds. Activity, cavitation status and cleansability are the main factors determining intervention thresholds (whether and when to intervene). Thresholds need to be adapted to each individual patient and setting, and need to be applied with each dental professional's individual expertise in mind. There are specific scenarios (Fig. 3, note that as described, not all interventions are applicable in both dentitions or all patients)
-
2.
Cavitation increases the likelihood of activity and lesion progression, as the dental plaque biofilm is protected from self-cleaning and oral hygiene procedures. Moreover, cavitation encourages a more rapid diffusion of sugars and acids. Cavitation can be assessed on visible/accessible surfaces (9.2, SD 0.8)
-
3.
As a general principle:
-
1.
Inactive, non-cavitated and cavitated lesions do not require any treatment (except for reasons of form, function or aesthetics) (8.8, SD 1.4)
-
2.
Active, non-cavitated carious lesions should be managed non- or micro-invasively (9.1, SD 0.9) (Fig. 2)
-
3.
Cavitated carious lesions which are cleansable but active, can also be managed non- or micro-invasively (except for reasons of form, function or aesthetics) (8.8, SD 1.4) (Fig. 2)
-
4.
Cavitated carious lesions which are not cleansable and active, should be managed using minimally invasive/restorative strategies. In specific circumstances, mixed interventions may be applicable (9.1, SD 1.0) (Fig. 2).
-
1.
-
4.
On occlusal surfaces, two specific scenarios arise (Fig. 3):
Fig. 3 
Factors determining intervention thresholds for occlusal lesions. Activity and cavitation status are the main factors determining intervention thresholds. In addition, radiographic dentine involvement should be considered. Note that as described, not all interventions are applicable in both dentitions or all patients
-
A.
Micro-cavitated lesions extending only into enamel. These can be successfully managed using micro-invasive or mixed interventions (8.8, SD 1.5).
-
B.
Micro-cavitated lesions radiographically extending deep into dentine (middle or inner dentine third, D2/3). These are often bacterially contaminated/infected, demineralised and also cavitated, but the cavitation cannot be detected/accessed given the specific anatomy of the occlusal surface. Lesion arrest using non-invasive means may be unlikely here. Also, the stability of any kind of sealant material placed over these lesions appears to be limited. Hence, such lesions should be managed minimally invasively/restoratively in the majority of cases (9.1, SD 0.8).
-
A.
-
5.
On proximal surfaces, cavitation of early lesions is usually hard to assess tactile-visually. Orthodontic separators may be used to gain visible access, or lesion depth ascertained from bitewing radiography can be used as proxy to determine the likelihood of cavitation (Fig. 4). Lesions extending radiographically into the middle or inner third of the dentine (D2/3) can be assumed to be cavitated, whilst those restricted to the enamel (E1/2) are usually not cavitated. These lesions should be managed accordingly. For lesions radiographically extending into the outer third of the dentine (D1), a decision problem exists. If possible, these lesions should be managed as if they were non-cavitated, as they are likely to be non-cavitated (that is, non- or micro-invasively) (8.9, SD 1.1)
Fig. 4 
Factors determining intervention thresholds for proximal lesions. Activity and cavitation status are the main factors determining intervention thresholds. However, cavitation status is clinically often difficult to assess. Hence, radiographic lesion depth is usually used as a proxy to estimate the chances of cavitation. For lesions confined to enamel (E1, 2), cavitation is unlikely. For lesions extending into the middle or inner third of the dentine (D2, 3), cavitation is likely. Lesions extending into the outer third of the dentine (D1), are more likely non-cavitated than cavitated. If a cavitation cannot be detected clinically, dentists should prefer non- or micro-invasive means if possible. Only under specific circumstances, minimally invasive (or mixed) interventions should be applied. Note that as described, not all interventions are applicable in both dentitions or all patients
-
6.
The caries risk/susceptibility of a patient should be assessed. Identified patient-specific risk factors should be, if possible, managed, and re-evaluation performed regularly. If risk factor modification is not successful or longitudinal re-evaluation not possible, this should be taken into consideration and may influence subsequent interventional thresholds (9.0, SD 0.8)
-
7.
Interventional thresholds may be lowered and more invasive treatments chosen for treatment requiring sedation or general anaesthesia (for example, children, special care patients) (9.2, SD 1.1)
-
8.
In permanent teeth, the overarching therapeutic aim is retaining teeth in a functional, pain-free and - depending on the location in the mouth - aesthetically acceptable condition. In primary teeth, maintaining the space of primary molars and avoiding pain or sepsis is the overarching therapeutic aim. Intervention thresholds should consider these aims accordingly (9.0, SD 1.3).



Conclusions
A consensus on when to intervene in the caries process and for existing carious lesions using non- or micro-invasive, minimally invasive/restorative or mixed interventions has been presented. Lesion activity, cavitation and cleansability are the key factors to be considered to determine intervention thresholds. Inactive lesions do not usually require any treatment (in some cases, restorations might be placed for reasons of form, function, aesthetics); active lesions do. Non-cavitated carious lesions should be managed non- or micro-invasively, as should cavitated carious lesions which are cleansable. Cavitated carious lesions which are not cleansable usually require minimally invasive/restorative management, also to restore form, function and aesthetics of the tooth. In specific circumstances, mixed interventions may be applicable. On occlusal surfaces, cavitated lesions confined to enamel and non-cavitated lesions radiographically extending deep into dentine (middle or inner dentine third, D2/3) may be exceptions to that rule. On proximal surfaces, cavitation is usually hard to assess tactile-visually. Hence, radiographic lesion depth is used to determine the likelihood of cavitation. Lesions extending radiographically into the middle or inner third of the dentine (D2/3) can be assumed to be cavitated, while those restricted to the enamel (E1/2) are usually not cavitated. For lesions extending radiographically into the outer third of the dentine (D1), cavitation status remains unclear. These lesions should be managed as if they were non-cavitated unless otherwise indicated. Individual decisions and clinical judgment should consider factors modifying the described intervention thresholds. Comprehensive diagnosis is the basis for systematic decision-making on when to intervene in the caries process and on existing carious lesions. Patients should be informed fully about treatment options and should provide informed consent accordingly and thorough, contemporaneous records maintained.
References
Sackett D L, Rosenberg W M C, Gray J A M, Haynes R B, Richardson W S. Evidence based medicine: what it is and what it isn't. BMJ 1996; 312: 71-72.
Frencken J E, Innes N P, Schwendicke F. Managing Carious Lesions: Why Do We Need Consensus on Terminology and Clinical Recommendations on Carious Tissue Removal? Adv Dent Res 2016; 28: 46-48.
Innes N P, Frencken J E, Schwendicke F. Don't Know, Can't Do, Won't Change: Barriers to Moving Knowledge to Action in Managing the Carious Lesion. J Dent Res 2016; 95: 485-486.
Frencken J E, Peters M C, Manton D J, Leal S C, Gordan V V, Eden E. Minimal intervention dentistry for managing dental caries - a review: report of a FDI task group. Int Dent J 2012; 62: 223-243.
Schwendicke F, Frencken J E, Bjorndal L et al. Managing Carious Lesions: Consensus Recommendations on Carious Tissue Removal. Adv Dent Res 2016; 28: 58-67.
Junger S, Payne S A, Brine J, Radbruch L, Brearley S G. Guidance on Conducting and Reporting Delphi Studies (CREDES) in palliative care: Recommendations based on a methodological systematic review. Palliative Medicine 2017: 31: 684-706.
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019; 393: e44.
Keyes PH. The infectious and transmissible nature of experimental dental caries. Findings and implications. Arch Oral Biol 1960; 1: 304-320.
Keyes P H, Fitzgerald R J. Dental caries in the Syrian hamster. IX. Arch Oral Biol 1962; 7: 267-277.
Marsh PD. Dental plaque as a biofilm and a microbial community - implications for health and disease. BMC Oral Health 2006; 6: S14.
Marsh PD. In Sickness and in Health - What Does the Oral Microbiome Mean to Us? An Ecological Perspective. Adv Dent Res 2018; 29: 60-65.
Fisher-Owens S A, Gansky S A, Platt L J et al. Influences on children's oral health: a conceptual model. Pediatrics 2007; 120: e510-520.
Gomez A, Espinoza J L, Harkins D M et al. Host Genetic Control of the Oral Microbiome in Health and Disease. Cell Host Microbe 2017; 22: 269-278.
Takahashi N, Nyvad B. The role of bacteria in the caries process: ecological perspectives. J Dent Res 2011; 90: 294-303.
Dawes C. What is the critical pH and why does a tooth dissolve in acid? J Can Dent Assoc 2003; 69: 722-724.
Vieira A R, Gibson C W, Deeley K, Xue H, Li Y. Weaker dental enamel explains dental decay. PloS One 2015; 10: e0124236.
Weber M, Bogstad Sovik J, Mulic A et al. Redefining the Phenotype of Dental Caries. Caries Res 2018; 52: 263-271.
Valdebenito B, Tullume-Vergara P O, Gonzalez W, Kreth J, Giacaman R A. In silico analysis of the competition between Streptococcus sanguinis and Streptococcus mutans in the dental biofilm. Mol Oral Microbiol 2018; 33: 168-180.
Takahashi N, Nyvad B. Ecological Hypothesis of Dentin and Root Caries. Caries Res 2016; 50: 422-431.
Banerjee A. 'Minimum intervention' - MI inspiring future oral healthcare? Br Dent J 2017; 223: 133-135.
Schwendicke F, Gostemeyer G. Understanding dentists' management of deep carious lesions in permanent teeth: a systematic review and meta-analysis. Implementation Sci 2016: IS 11: 142.
Innes N, Schwendicke F. Restorative Thresholds for Carious Lesions: Systematic Review and Meta-analysis. J Dent Res 2017; 96: 501-508.
Albino J, Tiwari T. Preventing Childhood Caries: A Review of Recent Behavioral Research. J Dent Res 2016; 95: 35-42.
Domejean S, Banerjee A, Featherstone J D B. Caries risk/susceptibility assessment: its value in minimum intervention oral healthcare. Br Dent J 2017; 223: 191-197.
Ismail A. Diagnostic levels in dental public health planning. Caries Res 2004; 38: 199-203.
Kassebaum N J, Bernabe E, Dahiya M, Bhandari B, Murray C J, Marcenes W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res 2015; 94: 650-658.
Raedel M, Hartmann A, Bohm S et al. Four-year outcomes of restored posterior tooth surfacesa massive data analysis. Clin Oral Invest 2017; 21: 2819-2825.
Burke F J, Lucarotti P S, Holder R L. Outcome of direct restorations placed within the general dental services in England and Wales (Part 2): variation by patients' characteristics. J Dent 2005; 33: 817-826.
Schwendicke F, Gostemeyer G, Blunck U, Paris S, Hsu L Y, Tu Y K. Directly Placed Restorative Materials: Review and Network Meta-analysis. J Dent Res 2016; 95: 613-622.
Elderton RJ. Clinical studies concerning re-restoration of teeth. Adv Dent Res 1990; 4: 4-9.
Brantley C, Bader J, Shugars D, Nesbit S. Does the cycle of rerestoration lead to larger restorations? J Am Dent Assoc 1995; 126: 1407-1413.
Tyas M J, Anusavice K J, Frencken J E, Mount G J. Minimal intervention dentistry - a review. FDI Commission Project 1-97. Int Dent J 2000; 50: 1-12.
Moynihan P J, Kelly S A M. Effect on Caries of Restricting Sugars Intake: Systematic Review to Inform WHO Guidelines. J Dent Res 2014; 93: 8-18.
Slayton R L, Urquhart O, Araujo MW B et al. Evidence-based clinical practice guideline on nonrestorative treatments for carious lesions: A report from the American Dental Association. J Am Dent Assoc 2018; 149: 837-849.
Marinho V C, Worthington H V, Walsh T, Clarkson J E. Fluoride varnishes for preventing dental caries in children and adolescents. The Cochrane database of systematic reviews 2013;7: Cd002279.
Walsh T, Worthington H V, Glenny A M et al. Fluoride toothpastes of different concentrations for preventing dental caries in children and adolescents. The Cochrane database of systematic reviews 2010: Cd007868.
Wolff M S, Schenkel A B. The Anticaries Efficacy of a 1.5% Arginine and Fluoride Toothpaste. Adv Dent Res 2018; 29: 93-97.
Wierichs R J, Meyer-Lueckel H. Systematic Review on Noninvasive Treatment of Root Caries Lesions. J Dent Res 2015; 94: 261-271.
Baysan A, Lynch E, Ellwood R et al. Reversal of primary root caries using dentifrices containing 5,000 and 1,100 ppm fluoride. Caries Res 2001; 35: 41-46.
Ekstrand K, Martignon S, Holm-Pedersen P. Development and evaluation of two root caries controlling programmes for home-based frail people older than 75 years. Gerodontology 2008; 25: 67-75.
Ekstrand K R, Poulsen J E, Hede B et al. A randomized clinical trial of the anti-caries efficacy of 5,000 compared to 1,450 ppm fluoridated toothpaste on root caries lesions in elderly disabled nursing home residents. Caries Res 2013; 47: 391-398.
Marinho V C, Chong L Y, Worthington H V, Walsh T. Fluoride mouthrinses for preventing dental caries in children and adolescents. Cochrane Database Syst Rev 2016; 7: Cd002284.
Gao S S, Zhang S, Mei M L, Lo E C, Chu C H. Caries remineralisation and arresting effect in children by professionally applied fluoride treatment - a systematic review. BMC Oral Health 2016; 16: 12.
Fung M H T, Duangthip D, Wong M C M, Lo E C M, Chu C H. Randomized Clinical Trial of 12% and 38% Silver Diamine Fluoride Treatment. J Dent Res 2018; 97: 171-178.
Alkilzy M, Santamaria R M, Schmoeckel J, Splieth C H. Treatment of Carious Lesions Using Self-Assembling Peptides. Adv Dent Res 2018; 29: 42-47.
Fontana M. Enhancing Fluoride: Clinical Human Studies of Alternatives or Boosters for Caries Management. Caries Res 2016; 50 Suppl 1: 22-37.
Alkilzy M, Tarabaih A, Santamaria R M, Splieth C H. Self-assembling Peptide P11-4 and Fluoride for Regenerating Enamel. J Dent Res 2018; 97: 148-154.
Krois J, Gostemeyer G, Reda S, Schwendicke F. Sealing or infiltrating proximal carious lesions. J Dent 2018; 74: 15-22.
Schwendicke F, Jager A M, Paris S, Hsu L Y, Tu Y K. Treating pit-and-fissure caries: a systematic review and network meta-analysis. J Dent Res 2015; 94: 522-533.
Griffin S O, Oong E, Kohn W et al. The Effectiveness of Sealants in Managing Caries Lesions. J Dent Res 2008; 87: 169-174.
Fontana M, Platt J A, Eckert G J et al. Monitoring of sound and carious surfaces under sealants over 44 months. J Dent Res 2014; 93: 1070-1075.
Hesse D, Bonifacio C C, Mendes F M et al. Sealing versus partial caries removal in primary molars: a randomized clinical trial. BMC Oral Health 2014; 14: 58.
Bakhshandeh A, Qvist V, Ekstrand K. Sealing occlusal caries lesions in adults referred for restorative treatment: 2-3 years of follow-up. Clin Oral Invest 2012; 16: 521-529.
Mickenautsch S, Yengopal V. Validity of sealant retention as surrogate for caries prevention - a systematic review. PloS One 2013; 8: e77103.
Paris S, Hopfenmuller W, Meyer-Lueckel H. Resin Infiltration of Caries Lesions. J Dent Res 2010; 89: 823-826.
Gruythuysen R. Non-Restorative Cavity Treatment. Managing rather than masking caries activity. Nederlands tijdschrift voor tandheelkunde 2010; 117: 173-180.
Mijan M, de Amorim R G, Leal S C et al. The 3.5-year survival rates of primary molars treated according to three treatment protocols: a controlled clinical trial. Clin Oral Invest 2014; 18: 1061-1069.
Santamaria R M, Innes N P T, Machiulskiene V et al. Alternative Caries Management Options for Primary Molars: 2.5-Year Outcomes of a Randomised Clinical Trial. Caries Res 2017; 51: 605-614.
Hansen N V, Nyvad B. Non-operative control of cavitated approximal caries lesions in primary molars: a prospective evaluation of cases. J Oral Rehab 2017; 44: 537-544.
Lo E C, Schwarz E, Wong M C. Arresting dentine caries in Chinese preschool children. Int J Paed Dent 1998; 8: 253-260.
Hickel R, Kaaden C, Paschos E et al. Longevity of occlusally-stressed restorations in posterior primary teeth. Am J Dent 2005; 18: 198-211.
Innes N P, Evans D J, Stirrups D R. Sealing caries in primary molars: randomized control trial, 5-year results. J Dent Res 2011; 90: 1405-1410.
Nyvad B, Machiulskiene V, Baelum V. Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions. Caries Res 1999; 33: 252-260.
Braga M, Mendes F, Martignon S, Ricketts D, Ekstrand K. In vitro comparison of Nyvad's system and ICDAS-II with lesion activity assessment for evaluation of severity and activity of occlusal caries lesions in primary teeth. Caries Res 2009; 43: 405-412.
Braga M M, Martignon S, Ekstrand K R, Ricketts D N, Imparato J C, Mendes F M. Parameters associated with active caries lesions assessed by two different visual scoring systems on occlusal surfaces of primary molars - a multilevel approach. Comm Dent Oral Epidemiol 2010; 38: 549-558.
Nyvad B, Fejerskov O. Assessing the stage of caries lesion activity on the basis of clinical and microbiological examination. Comm Dent Oral Epidemiol 1997; 25: 69-75.
Ferreira Zandona A, Santiago E, Eckert G J et al. The natural history of dental caries lesions: a 4-year observational study. J Dent Res 2012; 91: 841-846.
Wenzel A. Radiographic display of carious lesions and cavitation in approximal surfaces: Advantages and drawbacks of conventional and advanced modalities. Acta Odontol Scand 2014; 72: 251-264.
Tassery H, Levallois B, Terrer E et al. Use of new minimum intervention dentistry technologies in caries management. Aust Dent J 2013; 58: 40-59.
Broadbent J M, Foster Page L A, Thomson W M, Poulton R. Permanent dentition caries through the first half of life. Br Dent J 2013; 215: E12. https://doi.org/10.1038/sj.bdj.2013.991.
Mejare I, Axelsson S, Dahlen G et al. Caries risk assessment. A systematic review. Acta Odontol Scand 2013; 72: 81-91.
Lopez R, Smith P C, Gostemeyer G, Schwendicke F. Ageing, dental caries and periodontal diseases. J Clin Perio 2017; 44: S145-S152.
Bratthall D, Hansel Petersson G. Cariograma multifactorial risk assessment model for a multifactorial disease. Comm Dent Oral Epidemiol 2005; 33: 256-264.
Hayes M, Da Mata C, McKenna G, Burke F M, Allen P F. Evaluation of the Cariogram for root caries prediction. J Dent 2017; 62: 25-30.
Domejean S, White J M, Featherstone J D. Validation of the CDA CAMBRA caries risk assessment - a six-year retrospective study. J Calif Dent Assoc 2011; 39: 709-715.
Innes N P, Manton D J. Minimum intervention children's dentistry - the starting point for a lifetime of oral health. Br Dent J 2017; 223: 205-213.
Leal S C. Minimal intervention dentistry in the management of the paediatric patient. Br Dent J 2014; 216: 623-627.
Manhart J, Chen H, Hamm G, Hickel R. Buonocore Memorial Lecture. Review of the clinical survival of direct and indirect restorations in posterior teeth of the permanent dentition. Oper Dent 2004; 29: 481-508.
Ribeiro A A, Purger F, Rodrigues J A et al. Influence of contact points on the performance of caries detection methods in approximal surfaces of primary molars: an in vivo study. Caries Res 2015; 49: 99-108.
Smail-Faugeron V, Glenny A M, Courson F, Durieux P, Muller-Bolla M, Fron Chabouis H. Pulp treatment for extensive decay in primary teeth. Cochrane Database Syst Rev 2018; 5: Cd003220.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The corresponding author formally requested a declaration of possible conflicts of interest from each of the consensus panel members. No relevant conflicts of interest at the organisational and individual levels related to this consensus document were identified.
Funding
The conference was kindly sponsored by DMG (Hamburg, Germany). This included travel, accommodation and conference costs for panel members. The sponsor had no role in design or conduct of the conference or the content of this manuscript and were not present during the conference. No honoraria were given to any of the panel members.
Rights and permissions
About this article

Cite this article
Banerjee, A., Splieth, C., Breschi, L. et al. When to intervene in the caries process? A Delphi consensus statement. Br Dent J 229, 474–482 (2020). https://doi.org/10.1038/s41415-020-2220-4
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-020-2220-4
- Springer Nature Limited
This article is cited by
-
In vitro remineralization of adjacent interproximal enamel carious lesions in primary molars using a bioactive bulk-fill composite
BMC Oral Health (2024)
-
Preventive management of carious lesions: from non-invasive to micro-invasive operative interventions
British Dental Journal (2024)
-
Recommended procedures for managing carious lesions in primary teeth with pulp involvement—a scoping review
BDJ Open (2024)
-
Increasing awareness of risk literacy
British Dental Journal (2023)
-
Top tips for minimally invasive dentistry in primary care
British Dental Journal (2023)