
Abstract
Lymphocytic choriomeningitis virus (LCMV) is a prevalent pathogen, whose natural host and reservoir is the wild mouse. Humans can be infected when they contact the secretions of mice. Most infections of postnatal humans result in mild illness. However, the consequences can be severe when the infection occurs during pregnancy, as the virus crosses the placenta to infect the fetus. LCMV infection of the human fetus can lead to severe neuropathologic effects, including microencephaly, hydrocephalus, focal destructive lesions, and cerebellar hypoplasia. Outcomes among children with congenital LCMV are variable, but most are permanently and severely disabled. The neonatal rat inoculated with LCMV models human prenatal infection. The rat model has demonstrated that effects of LCMV depend on host age at the time of infection. Some effects, including encephalomalacia and neuronal migration disturbances, are immune-mediated and depend on the actions of T-lymphocytes. Other effects, including cerebellar hypoplasia, are virus-mediated and do not depend on T-lymphocytes. Cerebellar neuronal migration disturbances are caused by immune-mediated corruption of Bergmann glia structure. The rat pup inoculated with LCMV is a superb animal model for human congenital infection. All neuropathologic effects observed in human congenital LCMV infection can be recapitulated in the rat model.
Impact
-
Lymphocytic choriomeningitis virus (LCMV) is a prevalent human pathogen that can cause serious neurologic birth defects when the infection occurs during pregnancy.
-
The effects of the virus on the developing brain depend strongly on the age of the host at the time of infection.
-
Some of the pathologic effects of LCMV are immune-mediated and are driven by T-lymphocytes, while other pathologic effects are due to the virus itself.
Similar content being viewed by others


LCMV is a prevalent pathogen and an important cause of meningitis
Lymphocytic choriomeningitis virus (LCMV) is a prevalent human pathogen and an important cause of meningitis and neurologic birth defects. Yet, despite the importance of this virus, most pediatricians are unfamiliar with it.1
LCMV is a member of the Arenaviridae family of viruses. The arenaviruses are single-stranded, enveloped RNA viruses that acquired their name from arenosus, the Latin word for “sandy,” due to the fine granularities observed within the virion when viewed under an electron microscope.2
LCMV, like almost all arenaviruses, utilizes rodents as its principal reservoir. The common house mouse, Mus musculus, is the natural host and reservoir.3 In the mouse population, the virus is transferred vertically from one generation to the next by intrauterine infection. Although they may carry high viral loads, rodents that acquire LCMV trans-placentally often remain asymptomatic because the virus is not cytolytic and congenital infection provides the rodents with immunological tolerance for the virus. Mice infected with LCMV shed the virus in large quantities in all secretions, including urine, saliva, milk, semen, and feces throughout their lives.4,5
Humans acquire LCMV most often through direct contact with fomites contaminated with infectious virus or by inhaling aerosolized virus. In either case, the transmission occurs via human interaction with infected mice. Large numbers of humans are infected in this way. Epidemiologic studies have demonstrated that ~5% of people carry antibodies against LCMV, indicating prior infection.6,7 The virus is present across the globe, wherever wild mice are present, which is every continent except Antarctica.
In most cases, LCMV infection in children and adults is a mild febrile illness from which the patient fully recovers.8 Symptoms include fever, myalgia, malaise, headache, anorexia, nausea, and vomiting. In most cases, the illness is brief, self-limited, and never diagnosed.9 In as many as one-third of cases, the infection is asymptomatic. However, in some cases, the symptoms are far more severe, and fatalities from acquired LCMV infection do occur.10,11
People can also acquire LCMV via solid organ transplantation.12,13 Infections acquired in this way are always severe. Recipients of infected organs develop lethargy, leukopenia, and fever several weeks post-transplantation and rapidly progress to septic shock and multiorgan system failure. Virtually all cases of LCMV acquired by organ transplantation are fatal.12
The third way in which humans can be infected with LCMV is vertically. Congenital infection occurs when a woman acquires LCMV during pregnancy.14 The virus is passed to the fetus trans-placentally, presumably during maternal viremia. The first recognized case of congenital LCMV infection was reported in England in 1955.15 In subsequent decades, multiple cases of congenital LCMV infection were identified throughout Europe. However, the first cases of congenital LCMV were not identified in the US until 1993.16,17 The subsequent case reports have suggested that the virus causes severe injury to the developing brain and retinas.18,19,20,21
Congenital LCMV infection can induce a variety of pathologic effects and neurologic deficits
When we began studying congenital LCMV infection, little was known regarding the clinical manifestations of the disease or its epidemiology. Only sporadic case reports describing 1 or 2 patients at a time had been published. Therefore, we undertook a prospective study examining the presentation and outcome of congenital LCMV infection. We identified 20 newborns with congenital LCMV infection and followed them clinically for 6 months to 11 years.22 This was the largest cohort of children with congenital LCMV ever investigated. We asked the following three questions: 1) What are the presenting clinical signs? 2) What are the radiographic findings? and 3) What are the long-term outcomes?
We found that most mothers of affected babies had a known exposure to mice. Eleven of the 20 mothers lived in a rural setting; 7 lived in an urban setting, and only 2 lived in a suburban setting. This heavy weighting toward urban and rural dwellers over suburban dwellers probably reflects exposure to infected mice, since women living near corn cribs and other rural outbuildings and women living in urban apartment buildings are more likely to be exposed to mice than women living in suburban single-family houses.22,23
Of the 20 mothers, 12 had known exposure to wild mice during their pregnancies. One had been exposed to a sick pet hamster, which is also a competent host for LCMV.24 During their pregnancies, 12 of the 20 women experienced a “flu-like” illness, but eight of the women had no illness. This lack of illness on the part of the pregnant women reflects the fact that LCMV infections in adults can be asymptomatic.
Chorioretinitis and microcephaly are common presenting signs of congenital LCMV infection
The presenting signs of congenital LCMV infection in the newborns were variable. However, chorioretinitis was present in all 20 of the diagnosed babies. The next most common sign was microcephaly, present in 13 of the 20 (65%). Hydrocephalus, seizures, and jitteriness were also common presentations.
The clinical signs of congenital LCMV infection were largely confined to the nervous system. All 20 of the newborns had signs of nervous system dysfunction. However, only one affected baby had signs outside the nervous system, and this was a rash. None of the babies had hepatosplenomegaly, bone marrow suppression, cardiac defects, limb dysplasia, or vesicular rash, as are often seen in other congenital infections. In addition, the babies’ somatic growth was not substantially altered. Fourteen of the 20 babies (70%) had a birth weight appropriate for gestational age. Only six of the babies (30%) were small for gestational age. Thus, unlike many other congenital infections, such as toxoplasmosis and congenital cytomegalovirus (CMV) infection, congenital LCMV tends not to affect extra-neural tissues and does not interfere with somatic growth.22
Neuroimaging studies of the babies revealed a variety of abnormalities. The most common was microcephaly with periventricular calcifications. Other abnormalities included hydrocephalus, periventricular cysts, porencephalic cysts, encephalomalacia, parenchymal calcifications, cerebellar hypoplasia, and lissencephaly. This variety of neuroimaging findings suggests that LCMV infection induces pathology through a variety of mechanisms. In particular, microcephaly and hypoplasia suggest that the virus can interfere with brain growth; lissencephaly suggests that the virus can interfere with neuronal migration, while encephalomalacia suggests that the viral infection can induce destructive lesions. Indeed, as discussed below, the animal model verifies these various mechanisms of injury.
Children with congenital LCMV infection have vision loss and cognitive deficits
Among the 20 identified children, the long-term outcomes were diverse. All 20 had chorioretinitis and vision loss, and all 20 had cognitive deficits.21 However, the severity of the cognitive deficits varied widely. The cognitive deficits were profound in 5 of the children, and they were severe in 10. However, the cognitive deficits were only mild in 5 of the affected children. The severity of the cognitive deficits correlated with the neuroimaging findings. All children who had microcephaly and periventricular calcifications had profound or severe cognitive deficits, while all children with isolated cerebellar hypoplasia had only mild cognitive deficits.22
Additional long-term neurologic deficits were present in many of the children. Spastic quadriparesis and epilepsy were observed in most. Ataxia and hearing impairment were also common. However, none of the children showed evidence of regression over time. Thus, unlike congenital toxoplasmosis and CMV infections, congenital LCMV infection does not lead to progressive neurologic deterioration.
Congenital LCMV infection can induce isolated cerebellar hypoplasia
One noteworthy observation was that congenital LCMV infection can induce isolated cerebellar hypoplasia. These babies presented with jitteriness in the newborn period. Their long-term outcome was ataxia with mild cognitive deficits.22 While it has been hypothesized for many years that congenital viral infections may cause cerebellar hypoplasia, LCMV is one of the few viruses in which there is now evidence that this occurs.
An animal model, utilizing neonatal rats, provides a means to study human congenital LCMV infection
We next sought to understand the mechanisms by which LCMV damages the developing brain. To explore these mechanisms, we turned to the neonatal rat model of the disease.25 Rat brains are immature at birth, relative to humans. Therefore, exposure of a neonatal rat to teratogens simulates human fetal exposure. By injecting the neonatal rat brain with LCMV, we can mimic prenatal human infection (Fig. 1). This model system has yielded substantial insight into the virology of LCMV in the developing brain.26

In this model system, 1000 plaque forming units of LCMV are injected into the right cerebral hemisphere of neonatal rats. The virus is suspended in 10 ul of Dulbecco’s modified Eagle’s medium (DMEM). Uninfected control littermates receive sham intracerebral injections of DMEM alone.
For the first experiment, we asked the following questions: 1) What are the cellular targets of LCMV within the developing brain? 2) Does the virus infect neurons? and 3) What forms of neuropathology does LCMV induce? We injected 1000 plaque forming units (pfu) of LCMV into the right hemisphere of neonatal rats on postnatal day (PD) 4. We killed the rats at a variety of ages post inoculation, from PD 6 to PD 120. We examined LCMV localization via immunohistochemistry and assessed the neuropathology histologically. To further assess the localization and quantification of virus, we measured viral concentration in tissues by plaque assay.
Astrocytes are the principal cellular target of LCMV
We found that the initial cellular targets of LCMV are astrocytes.27 Within several days of inoculation, large proportions of astrocytes throughout the brain contain LCMV. During the initial days following inoculation, while astrocytes were heavily infected, neurons were spared. For several days post inoculation, the virus swept across the brain via astrocytes. Thus, astrocytes are the portal of entry of the virus into the brain, the principal site of viral replication, and the conduit through which the virus migrates across the developing brain.
LCMV selectively infects neurons in regions containing mitotically active neuroblasts
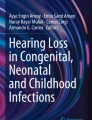
Several days after the virus infected astrocytes, neurons also became infected. However, not all neuronal populations were vulnerable. Indeed, neurons became infected in only four specific regions. These included the cerebellum, dentate gyrus, olfactory bulb, and septum. All neurons elsewhere in the brain remained uninfected, even when the astrocytes adjacent to them were heavily infected. These four infectable brain regions have a one-to-one correspondence with brain regions in which neurogenesis was occurring in the early postnatal rat (Fig. 2). All brain regions with infectable neurons had ongoing neurogenesis, and all brain regions with neurogenesis had infectable neurons (Fig. 2). This strongly suggests that dividing neuroblasts are a selective target of LCMV and that the virus utilizes the metabolic machinery of mitotically active neuroblasts to replicate.27

These are the olfactory bulb, septum, cerebellum, and dentate gyrus (red-colored areas in left panel). These are the same regions in which there is ongoing neurogenesis in the postnatal rat (green-colored areas in right panel). Thus, it is likely that LCMV utilizes the metabolic machinery of mitotically active neuroblasts to replicate.
For a brief period post inoculation, the virus resided within both astrocytes and neurons. However, after PD 18, the virus was abruptly cleared from astrocytes. The virus then persisted within neuronal populations for several months, until it was eventually cleared from all brain cells by PD 49.
Quantification of the virus, using plaque assays, showed that the virus replicates rapidly within the developing brain and reaches high titers. Following inoculation of 1000 plaque forming units into the brain on PD 4, viral titers rise to almost one billion plaque forming units per gram of tissue by PD 12 (Fig. 3). The viral titers remain high until PD 18, when the titers fall precipitously.

The y-axis denotes viral concentration (pfu per gram of tissue), while the x-axis denotes postnatal age (days). Note that the y-axis is a logarithmic scale. Following inoculation of 1000 pfu of LCMV on PD 4, viral titers rise to high levels by PD 18. This exponential rise in titers is due principally to a progressive infection of astrocytes. Between PD 12 and PD 18, viral titers plateau, during which both astrocytes and neurons are infected. After PD 18, viral titers abruptly decline, reflecting the clearance of virus from astrocytes. After PD 25, viral titers remain low, as the virus is confined to neurons, from which it is slowly cleared by PD 49.
If one combines the plaque assay data with the immunohistochemistry data, one can appreciate the relative roles of astrocytes and neurons in the sequential migration of infection. As shown in Fig. 3, the rising titers of LCMV between PD 4 and PD 12 represent the progressive infection of astrocytes. The plateau in LCMV titers between PD 12 and PD 18 represents the concomitant infection of neurons and glia. The precipitous decline in viral titer between PD 18 and PD 25 represents clearance of the virus from the glia, and the slowly declining titers after PD 25 represent the persistent infection of neurons.27
LCMV induces acute-onset and late-onset neuropathology
We found that pathologic changes were observed only in the four regions in which neurons were infectable and not in the regions in which the infection was confined to astrocytes. Furthermore, the type and time course of pathology differed markedly among the four regions. 1) In the cerebellum, LCMV infection induced an acute destructive process, driven by T-lymphocytes, that obliterated much of the cerebellum and left the animals markedly ataxic. 2) In the olfactory bulb, LCMV induced hypoplasia, which temporarily reduced the size of the olfactory bulb, due to a reversible reduction in granule cell number. 3) In the dentate gyrus, LCMV initially induced no evident pathology. However, weeks later, the infection led to a delayed-onset loss of granule cells, which was often accompanied by the onset of seizures. 4) In the septum, LCMV induced no early pathology or late pathology, despite a heavy infection of that brain region. Thus, LCMV infected neurons within four brain regions and induced a different form of pathology in all four regions.27 Why four brain regions simultaneously infected with the same virus would have such different neuropathologic effects is unknown.
Capacity of LCMV to replicate depends on host age at the time of infection
Our clinical observation that children with congenital LCMV infection have a wide variety of neuroimaging abnormalities and outcomes led us to wonder why this would occur. We hypothesized that the differences in outcome might be due to differences in the gestational timing of infection. We could not answer this question using our patient cohort because many of the women were asymptomatic during the infection or could not recall the timing of their illness. Thus, to determine the importance of gestational timing, we again turned to the animal model. We infected rat pups at a variety of ages and asked the following questions: Does the timing of infection (a) affect the infectability of the brain? (b) determine the cellular targets of infection? (c) determine the pathologic effects?
We found that brain infectability depended strongly on age of the animal at the time of inoculation.28 As shown in Fig. 4, peak viral titers in all brain regions examined were far higher when the infection occurred during the first days of postnatal life than when the infection occurred at later ages. In the cerebral cortex, for example, peak viral titers were a thousand-fold higher when the infection occurred on PD 1 than when it occurred on PD 6. By PD 21, the cerebral cortex was uninfectable. Thus, over the course of just several days, the infectability of the developing brain by LCMV declined substantially (Fig. 4).

Shown here are peak viral titers attained in three brain regions (cerebral cortex, cerebellum, and olfactory bulb) as a function of age at the time of inoculation. Note that the y-axis is a logarithmic scale. In all brain regions, higher peak viral titers were achieved when the infection occurred at early postnatal ages. Over the course of just several days, the infectability of the brain declines dramatically. Between PD 1 and PD 10, there is a 10,000-fold decline in peak viral titers achieved in the cerebral cortex. After PD 21, only the olfactory bulb remains infectable and only at relatively low levels.
The cellular targets of LCMV in the developing brain depend on host age at the time of infection
The cellular targets of infection also changed with development. This fact was most evident in the cerebral cortex. When the inoculation occurred on PD 1, virtually all neurons and astrocytes of the cerebral cortex were heavily infected. However, when the infection occurred just three days later, on PD 4, no neurons were infectable within the cerebral cortex, and the infection was limited exclusively to astrocytes. By PD 21, no cells—neither neurons nor astrocytes—were infectable. Thus, over the course of just several days, the cellular targets of infection changed dramatically.28
The neuropathologic effects of LCMV depend on host age at the time of infection
The pathologic changes induced by LCMV depended strongly on the age of the host at the time of infection. This fact was most evident in the cerebellum. When the infection occurred on PD 1, the cerebellum was hypoplastic. The cerebellum was greatly reduced in size, due to a reduction in granule cell number but was histologically intact and had no areas of destruction. In contrast, when the infection occurred just three days later, on PD 4, the cerebellum underwent a destructive process that obliterated large portions of the cerebellum. Furthermore, infection on PD 4 or PD 6 led to neuronal migration disturbances within the cerebellum, such that clumps of granule cells were permanently ectopically located within the molecular layer. This neuronal migration disturbance did not occur with infection on PD 1 or at any time after PD 6. When the infection occurred on PD 21, the cerebellum was left completely intact, with no hypoplasia, destruction, or ectopia. Thus, the type and severity of neuropathology depended on host age at the time of infection.28
The immune response to LCMV infection also depended on the age of the animal at the time of inoculation. When the inoculation occurred on PD 1, very few lymphocytes infiltrated the cerebellum, despite a heavy infection of that brain region. However, if the infection occurred just three days later, on PD 4, then large numbers of lymphocytes infiltrated the cerebellum, and the structure underwent an acute destructive process. Thus, the immune response to LCMV was heavily influenced by host age and changed dramatically within several days.28 The window of PD 4–6, marked by lymphocytic infiltration, tissue destruction, and neuronal migration disturbances is probably due to a combination of high viral titer and immune system maturation.
Athymic rats provide a means to study the role of T-lymphocytes in LCMV-induced pathology
Within the cerebellum, LCMV infection induces a robust infiltration of T-lymphocytes. This led us to wonder whether the pathology in congenital LCMV infection is immune-mediated or virus-mediated.29 We asked the questions: What role do T-lymphocytes play in the cerebellar pathology? Are lymphocytes responsible for the destructive lesions? For the hypoplasia? For the disturbed neuronal migration?
To address these issues, we compared the effects of infection in wild-type rats with the effects in athymic (nude) rats. While wild-type rats have an intact immune system, athymic rats have a congenital absence of T-lymphocytes.
We found that the cellular targets of infection and peak viral titers were identical in the two rat strains. Thus, the presence or absence of T-lymphocytes does not influence infectability of the brain. However, while viral titers fell rapidly in the wild-type rats, they fell much more slowly in the athymic rats, and clearance of the virus from astrocytes was impaired in the athymic rats. Therefore, T-lymphocytes play a crucial role in the clearance of LCMV from the developing brain.29
The destructive lesions and neuronal migration disturbances are immune-mediated, while the hypoplastic effects are likely virus-mediated
LCMV infection led to a robust infiltration of T-lymphocytes in the wild-type rats, while, predictably, this lymphocytic response was absent in the athymic rats. Furthermore, while the infection induced hypoplasia, destructive lesions, and neuronal migration disturbances in the wild-type rats, the infection produced hypoplasia alone in the athymic rats. Thus, the destructive lesions and neuronal migration disturbances depend on T-lymphocytes, while the hypoplasia does not. This finding suggests that the destructive lesions and neuronal migration disturbances are immune-mediated, while the hypoplasia is virus-mediated.29 Likely, hypoplasia is due to the viral load impairing neurogenesis.30 However, it is possible that the hypoplasia is also immune-mediated, and due to some component of the immune system other than T-lymphocytes.
To confirm the role of T-lymphocytes in the destructive lesions and neuronal migration disturbances, we conducted an adoptive transfer experiment. We injected LCMV-competent splenocytes into athymic rat pups that had been infected one day earlier with LCMV. We found that the athymic rats that did not receive the splenocytes had cerebellar hypoplasia alone. However, when athymic rats received splenocytes, destructive lesions and neuronal migration disturbances also occurred. These results demonstrate that the destructive lesions and neuronal migration disturbances are immune-mediated and depend on lymphocytes, while the hypoplasia is not immune-mediated and is probably a direct effect of the virus.29
LCMV infection disturbs neuronal migration by disrupting the structure of Bergmann glia
We next explored the mechanism by which the neuronal migration disturbance occurs. Within the developing cerebellum, Bergmann glial cells are the scaffolding along which granule cells migrate from the external granule cell layer to the internal granule cell layer. The fibers of Bergmann glia are normally arranged in a “tram-trac” parallel formation (Fig. 5). In the developing cerebellum, this configuration guides the granule cells in a straight pathway across the molecular layer. We hypothesized that LCMV infection induces neuronal migration disturbances by corrupting the configuration of Bergmann glia. To investigate this, we infected wild-type and athymic rats with LCMV and examined the structure of Bergmann glia by immunostaining them with an antibody for glial fibrillary acidic protein (GFAP). We found that, in wild-type rats, LCMV infection substantially altered the structure of Bergmann glia cells and caused a neuronal migration disturbance. In contrast, in the athymic rats, LCMV infection did not alter Bergmann glia structure and did not cause a neuronal migration disturbance (Fig. 5).

Shown here are sections of cerebellum immunostained for GFAP (green, which labels Bergmann glia), NeuN (red, which labels granule cells), and DAPI (blue, a nuclear counterstain). The white arrows point to Bergmann glia. Left panel: In the normal, uninfected cerebellum of wild type (Lewis) rats, the radial processes of Bergmann glia are arranged in a parallel “tram-trac” fashion, which guides the migrating granule cells across the molecular layer. Middle panel: In the LCMV-infected cerebellum of wild type rats, Bergmann glia structure is dramatically altered. The normal parallel configuration is lost, and the processes, instead, have a knotted “spaghetti-like” arrangement. As a result, some granule cells (white arrowheads) have failed to migrate to the granule cell layer and remain ectopically located in the molecular layer. Right panel: In the LCMV-infected cerebellum of athymic rats, the normal configuration of Bergmann glia cells is preserved, and all granule cells have properly migrated to their position in the granule cell layer. Thus, LCMV induces a neuronal migration disturbance in the cerebellum by corrupting the structure of Bergmann glia, and this effect is immune-mediated and depends on the actions of T-lymphocytes.
This finding strongly suggested that the neuronal migration disturbance is immune-mediated and due to the actions of lymphocytes. To confirm this notion, we conducted another adoptive transfer experiment in which we again transplanted LCMV-competent lymphocytes into LCMV-infected athymic rats. In these lymphocyte recipients, the corruption of Bergmann glia structure and the neuronal migration disturbance, which had been absent in the athymic rats, were restored. These results show that the neuronal migration disturbance is immune-mediated and that it is due to lymphocyte-induced alteration in Bergmann glia structure.29
Different strains of LCMV have different cellular targets, immune responses, and pathologic effects
In nature, several strains of LCMV exist.31 We hypothesized that some of the variability in outcome among humans with congenital LCMV may be due to infection with different viral strains. To investigate this possibility, we infected neonatal rats with one of three different strains: E350, Clone 13, and WE2.2. These strains were chosen for comparison because they differ in receptor binding affinities, immune response, and virulence. We conducted behavioral tests, immunohistochemistry to identify cellular targets of infection, viral quantification to measure viral burdens, gene expression studies to measure cytokine responses, and histologic analyses to assess neuropathology. We found that the different viral strains induced markedly different effects in all of these parameters. For example, the E350 strain initially targeted astrocytes, while WE2.2 and Clone 13 targeted neurons. The E350 strain induced focal destructive lesions, while the other two induced global microencephaly. All three strains induced olfactory bulb pathology, but the form and severity of pathology differed markedly among the strains and produced different olfactory discrimination deficits.32 We discovered that different LCMV strains have different patterns of infection, neuropathology, immune responses, and disease symptoms.31 These findings suggest that the different outcomes among children with congenital LCMV infection are due, at least in part, to infection with different viral strains.
Summary and conclusions
-
Lymphocytic choriomeningitis virus (LCMV) is a prevalent human pathogen. Spread principally through the secretions of wild mice, the virus infects large numbers of people.33 Humans can be infected in three ways: by contacting the secretions of infected mice, through organ transplantation, or via mother-to-fetus vertical transmission.8
-
In most cases of postnatally acquired infection, the disease consists of a mild febrile illness from which the patient fully recovers. In contrast, when the infection occurs prenatally, the fetus can be severely and permanently injured.14 The virus is highly neurotropic, and most fetal injuries occur in the brain.9
-
LCMV induces a variety of neurologic effects, but virtually all children with congenital infection have chorioretinitis and cognitive impairment. Epilepsy, cerebral palsy, and ataxia are also common outcomes.22
-
The neonatal rat model has provided valuable insight into the virology of congenital LCMV infection.26 This model system has shown that astrocytes are the principal cellular target of LCMV in the developing brain. Neuroblasts are also important target cells. In the developing brain, LCMV infection leads to destructive lesions, hypoplasia, neuronal migration disturbances, and delayed-onset mortality of infected neurons.27 Some of these effects are immune-mediated, while others are virus-mediated.29
-
Developmental age at the time of infection plays a key role in determining the cellular targets, viral titers, immune responses, pathologic effects, and disease symptoms.28
-
Different strains of LCMV have different patterns of infection, forms of pathology, and disease symptoms.32
-
The neonatal rat infected with LCMV is a powerful model system for the study of human congenital LCMV disease. All pathologic effects in humans with congenital LCMV can be recapitulated in the rat model by injecting the rat pup with a specific LCMV strain at a specific age (Table 1). As a result, the rat pup infected with LCMV is one of the best model systems for the study of congenital brain infections.26
Table 1 With LCMV infection on different postnatal ages and with different strains, the rat model recapitulates all pathologic effects observed in humans with congenital LCMV infection. -
The infected neonatal rat is not a perfect model system of congenital LCMV because it lacks the mother’s immune system and the placenta, both of which are affected by LCMV infection and likely play a role in the infection’s effect on the fetus.34 Thus, additional model systems should be developed for the study of this important disease.
-
Many fundamental questions remain regarding the pathophysiology of congenital LCMV infection. Among the most interesting are: Why does LCMV principally target astrocytes? Through what mechanism does LCMV induce the late-onset mortality of dentate granule cells? How does LCMV infection lead to cerebellar and olfactory bulb hypoplasia? Why do different strains of LCMV induce different patterns of infection and pathology? Answers to these questions will shed light on the biology of congenital LCMV and elucidate novel virus–host interactions.
References
Vilibic-Cavlek, T. et al. Lymphocytic choriomeningitis-emerging trends of a neglected virus: a narrative review. Trop. Med. Infect. Dis. 6, 88 (2021).
Olivieri, N. R., Othman, L., Flannery, D. D. & Gordon, S. M. Transmission, seroprevalence, and maternal-fetal impact of lymphocytic choriomeningitis virus. Pediatr. Res. https://doi.org/10.1038/s41390-023-02859-w (2023).
Castellar, A. et al. First evidence of lymphocytic choriomeningitis virus (arenavirus) infection in Mus musculus rodents captured in the urban area of the municipality of Sincelejo, Sucre, Colombia. Biomedica 37, 75–85 (2017).
Childs, J. E., Glass, G. E., Korch, G. W., Ksiazek, T. G. & Leduc, J. W. Lymphocytic choriomeningitis virus infection and house mouse (mus musculus) distribution in urban Baltimore. Am. J. Trop. Med. Hyg. 47, 27–34 (1992).
Talley, P., Holzbauer, S., Smith, K. & Pomputius, W. Notes from the field: lymphocytic choriomeningitis virus meningoencephalitis from a household rodent infestation – Minnesota, 2015. Morb. Mortal. Wkly Rep. 65, 248–249 (2016).
Ambrosio, A. M., Feuillade, M. R., Gamboa, G. S. & Maiztegui, J. I. Prevalence of lymphocytic choriomeningitis virus infection in a human population of Argentina. Am. J. Trop. Med. Hyg. 50, 381–386 (1994).
Stephensen, C. B. et al. Prevalence of serum antibodies against lymphocytic choriomeningitis virus in selected populations from two U.S. cities. J. Med. Virol. 38, 27–31 (1992).
Bonthius, D. J. Lymphocytic choriomeningitis virus: a prenatal and postnatal threat. Adv. Pediatr. 56, 75–86 (2009).
Bonthius, D. J. & Karacay, B. Meningitis and encephalitis in children: an update. Neurol. Clin. 20, 1013–1038 (2002).
Armstrong, C. & Lillie, R. D. Experimental lymphocytic choriomeningitis of monkeys and mice produced by a virus encountered in studies of the 1933 St. Louis encephalitis epidemic. Public Health Rep. 49, 1019–1022 (1934).
Folk, S. et al. Lymphocytic choriomeningitis with severe manifestations, Missouri, USA. Emerg. Infect. Dis. 17, 1973–1974 (2011).
Fischer, S. A. et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N. Engl. J. Med. 354, 2235–2249 (2006).
Centers for Disease Control and Prevention. Lymphocytic choriomeningitis virus transmitted through solid organ transplantation—Massachusetts, 2008. Morb. Mortal. Wkly Rep. 57, 799–801 (2008).
Bonthius, D. J. Lymphocytic choriomeningitis virus: an underrecognized cause of neurologic disease in the fetus, child and adult. Semin. Pediatr. Neurol. 19, 89–95 (2012).
Komrower, G. M., Williams, B. L. & Stones, P. B. Lymphocytic choriomeningitis in the newborn. Probable transplacental infection. Lancet 1, 697–698 (1955).
Barton, L. L. et al. Congenital lymphocytic choriomeningitis virus infection in twins. Pediatr. Infect. Dis. J. 12, 942–946 (1993).
Larsen, P. D., Chartrand, S. A., Tomashek, K. M., Hauser, L. G. & Ksiazek, T. G. Hydrocephalus complicating lymphocytic choriomeningitis virus infection. Pediatr. Infect. Dis. J. 12, 528–531 (1993).
Ansari, N., Demmler-Harrison, G., Coats, D. K. & Paysse, E. A. Severe congenital chorioretinitis caused by congenital lymphocytic choriomeningitis virus infection. Am. J. Ophthalmol. Case Rep. 22, 101094 (2021).
Barton, L. L., Peters, C. J. & Ksiazek, T. G. Lymphocytic choriomeningitis virus: an unrecognized teratogenic pathogen. Emerg. Inf. Dis. 1, 152–153 (1995).
Barton, L. L. & Mets, M. B. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin. Infect. Dis. 33, 370–374 (2001).
Wright, R. et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics 100, 1–6 (1997).
Bonthius, D. J. et al. Congenital lymphocytic choriomeningitis virus infection: spectrum of disease. Ann. Neurol. 62, 347–355 (2007b).
Olivieri, N. R., Othman, L. & Gordon, S. M. Health disparities revealed in a case of congenital LCMV. Pediatr. Res https://doi.org/10.1038/s41390-023-02772-2 (2023).
Biggar, R., Woodall, J., Walter, P. & Haughie, G. Lymphocytic choriomeningitis outbreak associated with pet hamsters: fifty-seven cases from New York state. JAMA 232, 494 (1975).
Monjan A. A., Cole G. A. & Nathanson N. Pathogenesis of LCM disease in the rat. In: Lymphocytic choriomeningitis Virus and Other Arenaviruses (Lehmann F., ed) 195–206 (Springer-Verlag, New York, 1973).
Bonthius, D. J. & Perlman, S. Congenital viral infections of the brain: lessons learned from lymphocytic choriomeningitis virus in the neonatal rat. PLoS Pathog. 3, 1541–1550 (2007).
Bonthius, D. J., Mahoney, J. C., Buchmeier, M. J. & Taggard, D. A. Critical role for glial cells in the propagation and spread of lymphocytic choriomeningitis virus in the developing rat brain. J. Virol. 76, 6618–6635 (2002).
Bonthius, D. J., Nichols, B., Harb, H., Mahoney, J. & Karacay, B. Lymphocytic choriomeningitis virus infection of the developing brain: critical role of host age. Ann. Neurol. 62, 356–374 (2007a).
Klein, H., Rabe, G. K., Karacay, B. & Bonthius, D. J. T-cells underlie some, but not all, of the cerebellar pathology in a neonatal rat model of congenital lymphocytic choriomeningitis virus infection. J. Neuropathol. Exp. Neurol. 75, 1031–1047 (2016).
Sun, T., Vasek, M. J. & Klein, R. S. Congenitally acquired persistent lymphocytic choriomeningitis viral infection reduces neuronal progenitor pools in the adult hippocampus and subventricular zone. PLoS One 9, e96442 (2014).
Albarino, C. G. et al. High diversity and ancient common ancestry of lymphocytic choriomeningitis virus. Emerg. Inf. Dis. 16, 1093–1110 (2010).
Plume, J. M., Todd, D. & Bonthius, D. J. Viral strain determines disease symptoms, pathology, and immune response in neonatal rats with lymphocytic choriomeningitis virus infection. Viruses 11, 1–22 (2019).
Bonthius, D. J. Diagnosed cases of congenital LCMV infection: tip of the iceberg. Ann. Neurol. 64, 356 (2008).
Tevaearai, F., Moser, L. & Pomar, L. Prenatal diagnosis of congenital lymphocytic choriomeningitis virus infection: a case report. Viruses 14, 1–9 (2022).
Acknowledgements
Supported by grants from the NIH (K08-NS02007, T32-HD041922, F31-NS051161), March of Dimes Birth Defects Foundation (MOD-1-FY01-217), Child Neurology Society Young Investigator Award, and the Atrium Health Research Foundation. The author thanks Jo Mahoney, Glenda Rabe, Hannah Klein, and Jeffrey Plume for their technical and intellectual contributions.
Author information
Authors and Affiliations
Contributions
D.J.B. conceived the work reported here, wrote the manuscript, and produced the figures.
Corresponding author
Ethics declarations
Competing interests
The author declares no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bonthius, D.J. Lymphocytic choriomeningitis virus injures the developing brain: effects and mechanisms. Pediatr Res 95, 551–557 (2024). https://doi.org/10.1038/s41390-023-02985-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-023-02985-5
- Springer Nature America, Inc.