
Abstract
The impact of 3-year change in glycemic state on the risk of hypertension among Tehranian adults aged ≥20 years was assessed. The study population included 1679 men and 2348 women who were non-diabetic normotensive at enrollment. The following categories were defined both at baseline visit and three years later (second visit): normoglycemia [normal fasting glucose (NFG) and normal glucose tolerance (NGT)] and prediabetes [impaired fasting glucose (IFG) or impaired glucose tolerance (IGT)]. Changes in the categories, i.e., regression to normoglycemia, remaining in previous status, and progression to diabetes were assessed. Changes in fasting plasma glucose (FPG) and 2-hour plasma glucose (2hPG) categories were also considered separately. We used the Cox models adjusted for traditional hypertension risk factors to estimate hazard ratios (HRs) with 95% confidence intervals (CIs). During a median follow-up of 9.4 years, 485 men and 589 women developed hypertension. Among men, considering both FPG and 2hPG, compared to individuals remaining normoglycemic, changing from prediabetes to normoglycemia had a HR of 1.30 (95% CI: 0.98–1.71; P-value: 0.064). Defining changes by 2hPG showed that compared to remaining NGT, incident IGT (progression from NGT to IGT) had a significant association with increased risk of hypertension development by a HR of 1.61 (1.13–2.30). Among women, on the other hand, change in glycemic state generally didn’t show a significant association with incident hypertension. To sum up, change in glycemic state hadn’t a significant association with hypertension development among women; however, compared to remaining NGT, men with incident IGT had a significant higher risk.
Similar content being viewed by others


Introduction
A great number of the world population have been suffering from non-communicable diseases (NCDs), especially type 2 diabetes mellitus (T2DM) and hypertension [1]. T2DM (in general term dysglycemic state) has been identified as a major issue due to the high burden worldly [2]. Prediabetes is defined as an intermediate glucose regulation state that prone person to NCDs development [3, 4]; it is characterized by elevated blood glucose concentrations, including those with impaired fasting glucose (IFG), impaired glucose tolerance (IGT), or elevated glycosylated hemoglobin A1C (HbA1C), but not in diabetic ranges [5, 6]. A national study has shown that about 11.4 and 14.6% of Iranian adults had T2DM and IFG, respectively, in 2011 [7]. Moreover, using oral glucose tolerance test and fasting plasma glucose (FPG) level, we reported the prevalence of prediabetes among Tehranian residents reached about 24.5% in 2008–2011 [8].
In addition to the high burden of dysglycemia, the World Health Organization (WHO) reported hypertension as being one of the main important risk factors for morbidity and mortality globally; more than one billion people are involved with hypertension, and it causes 9.4 million deaths yearly [9]. A systematic review and meta-analysis study has reported that the prevalence of hypertension in the Middle East and North Africa (MENA) region has been increasing in the past three decades [10]. Furthermore, nearly 2.7% of Tehranian adults (3% of men and 2.6% of women) develop hypertension annually [11].
Hypertension has a two-way relationship with dysglycemia [12] and is two times more common among diabetic patients [13]. Higher risk of hypertension was also found for adults with prediabetic state in some but not all studies; however, this higher risk may have been significant only for one of IFG, IGT, or elevated HbA1C or only for one gender [4, 11, 14,15,16,17,18,19,20]. In addition to the snapshot assessment of the glycemic state, change in glycemic state was shown to have associations with NCDs, especially cardiovascular disease (CVD) [21, 22]. To the best of our knowledge, there is only one cohort study that described the effect of change in glycemic state on hypertension development [18]; the researchers found the progression of glycemic state as a strong determinant of incident hypertension; however, different components of prediabetes were not considered [18]. Previously we reported that the presence of IFG was associated with more than 20% significantly higher risk of incident hypertension only for women but not men [4]. In the current study, we aim to extend our previous study by clarifying the association of 3-year change in glycemic state with the risk of incident hypertension among Tehranian men and women.
Materials and methods
Study design and population
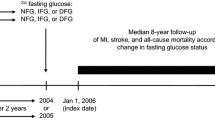
The Tehran Lipid and Glucose Study (TLGS) is a large population-based cohort study conducted on the Tehranian civilization in district No 13. It has been designed to determine the prevalence and incidence of NCDs. For this study, as shown in Fig. 1, we considered the second phase of TLGS as baseline recruitment (2001–2005). After about 3 years, the glycemic state of participants was reassessed at phase III (2005–2008) again. Then, participants have been followed for incident hypertension with approximately 3-year intervals (i.e., phase IV: 2008–2011, phase V: 2011–2014, and phase VI: 2015–2018). The details of the TLGS protocol and design have been described elsewhere [23].

Timeline of the study design: Tehran Lipid and Glucose Study, Iran, 2002–2018.
As presented in Supplementary Fig. 1, for this study, among a sum of 3891 male and 5036 female participants aged ≥20 years, 443 men and 623 women with prevalent T2DM at baseline were excluded. Moreover, we excluded 781 male and 861 female subjects because of prevalent hypertension at baseline or incident hypertension until the end of phase III. Among the remaining 2667 men and 3552 women, 929 male and 1015 female individuals were also eliminated, due to missing data on glycemic state or blood pressure at phase II or III. Other exclusion criterion was missing data on covariates (59 men and 189 women), leading to 1679 men and 2348 women remaining eligible for the analysis of the current study (response rate was 63 and 66% for men and women, respectively).
Clinical and laboratory measurements
At recruitment, a valid questionnaire was used to obtain the data on demographic identification, past medical/drugs history, family history, and smoking habits regarding the TLGS protocol [23]. Using the Modifiable Activity Questionnaire (MAQ), which measures all three forms of activities including leisure time, job and household activities over the past year, the level of physical activity was assessed [23, 24].
Weight was measured with a sensitive scale by 100 g error, and height was measured in a standing position without shoes. Then, body mass index (BMI) was calculated by weight in kilograms divided by the square of height in meters. An expert, who was not aware about the cardiometablolic profiles of participants, used a standardized mercury sphygmomanometer (calibrated by the Iranian Institute of Standards and Industrial Research) to measure the blood pressure (BP) of participants. Subsequent to 15 min of rest, two measurements were done on the right arm with a 30-s interval; the mean of these two office BP measurements was considered as the subject’s BP. Blood samples from all participants were taken after 12–14 h of fasting. Also, for those without a history of using glucose-lowering drugs, after taking 75 g glucose orally, 2-hour post-challenge plasma glucose (2hPG) was measured. Details for laboratory measurements, including FPG, 2hPG, high-density lipoprotein cholesterol (HDL-C), and triglycerides (TG), are published elsewhere [23].
Definition of the main exposures, confounding factors, and outcome
Based on the 2003 American Diabetes Association (ADA) guideline [25], we defined IFG as 5.6 ≤ FPG < 7 mmol/L and IGT as 7.8 ≤ 2hPG < 11 mmol/L. Prediabetes was defined as those with IFG and/or IGT. T2DM was also defined as FPG ≥ 7 mmol/L, or 2hPG ≥ 11.1 mmol/L, or using glucose-lowering drugs. Moreover, normal fasting glucose (NFG) was those with FPG < 5.6 mmol/L, and normal glucose tolerance (NGT) was those with 2hPG < 7.8 mmol/L. The normoglycemic participants were those with NFG and NGT.
Smoking status was divided into two groups; current smokers versus former/never smokers. Subjects with <1500 MET (metabolic equivalent task-minutes per week) were also in the low physical active group [23]. Furthermore, a positive family history of premature CVD has been defined as prior diagnosed CVD in female first-degree blood relatives aged below 65 years or male first-degree blood relatives who were below 55 years.
Regarding the seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high BP (the JNC 7 report) [26], hypertension was defined as the existence of one of continued parameters: (a) having systolic blood pressure (SBP) ≥ 140 mm Hg, (b) having diastolic blood pressure (DBP) ≥ 90 mm Hg, or (c) initiation of using anti-hypertensive medications.
Statistical analysis
Descriptive statistics were used to describe the baseline characteristics of the participants. Normally distributed continuous variables were reported as mean ± standard deviation (SD), and the highly skewed variables were reported as median (interquartile range: IQR). Number (%) was also used for reporting categorical variables. We compared the baseline characteristics of the respondents versus non-respondents (those with missing data on main exposure or covariates) and also normoglycemic versus prediabetic groups, using chi-square, ANOVA, and Kruskal–Wallis tests as appropriate.
The time to event was described as the time of censoring or the outcome occurring, whichever firstly came. In the case of death, leaving the district, or being until the end of the study (April 2018) without any event, we censored participants. For individuals with incident hypertension, the event date was defined as the mid-time between the dates of the follow-up visit at which an individual developed hypertension and the last follow-up visit preceding incident hypertension.
We categorized participants into different glycemic change groups by three methods: (a) using both FPG and 2hPG [normoglycemia to normoglycemia (reference), normoglycemia to prediabetes, prediabetes to normoglycemia, prediabetes to prediabetes, and prediabetes to T2DM]. (b) using FPG [NFG to NFG (reference), NFG to IFG, IFG to NFG, IFG to IFG, and IFG to diabetic range of FPG]; (c) using 2hPG [NGT to NGT (reference), NGT to IGT, IGT to NGT, IGT to IGT, and IGT to diabetic range of 2hPG]. It should be noted that the frequency of normoglycemic participants that changed to diabetes was too low to include in our models.
The Cox proportional hazard models were applied to evaluate the sex-specific association of glycemic state change with incident hypertension. The hazard ratios (HRs) with 95% confidence intervals (CIs) were reported in three models: Model 1: adjusted for age; Model 2: adjusted for age, BMI, current smoking, low physical activity, history of CVD, and family history of premature CVD; Model 3: Model 2 + further adjusted for TG/HDL-C, as a surrogate of insulin resistance (IR) [27, 28].
Using the Schoenfeld residual test, the proportionality was assessed for the Cox models. All proportionality assumptions were appropriate in our analysis. STATA version 14 (StataCorp LP, College Station, TX, USA) statistical software was used for statistical analyses of this study, and a two-tailed p-value < 0.05 was considered significant.
Results
The study population included 1679 men with a mean age of 40.8 years and 2348 women with a mean age of 38.8 years. Baseline characteristics of the respondent and non-respondents are compared in Supplementary Table 1. Among men, respondents had lower HDL-C and were more physically inactive, but they smoked less. Among women, respondents were older and had higher level of BMI, FPG, and 2hPG. Moreover, female respondents were less educated, but they were more physically active and smoked less.
Baseline characteristics of the participants are shown in Table 1. Among continuous variables, generally, the cardiometabolic profile was worsened among prediabetic participants; they were older and had higher values for BMI, SBP, DBP (only among women), FPG, 2hPG, and triglycerides. Moreover, prediabetic women had lower HDL-C level. Among categorical variables, normoglycemic participants were more educated and with lower prevalent CVD, although they had a higher prevalence of low-physical activity.
During a median follow-up of 9.4 years (IQR: 8.4–10.2), 485 men and 589 women developed hypertension.
Multivariable HRs and 95% CI of incident hypertension according to glycemic state change are reported in Table 2 for male participants. Considering both FPG and 2hPG, compared to individuals remaining normoglycemic, those prediabetic individuals at baseline that changed to normoglycemia had a marginally significant higher risk of incident hypertension with a HR of 1.31 (95% CI: 0.99–1.72; P-value: 0.057) in model 2; the risk remained marginally significant even after adjustment for TG/HDL-C in model 3. Moreover, progression from normoglycemia to prediabetes and also prediabetes to T2DM had HRs of 1.25 (0.92–1.72) and 1.41 (0.70–2.86), respectively, in model 3. Considering FPG, different changes in glycemic state were not associated significantly with incident hypertension in model 3. On the other hand, defining changes by 2hPG showed that incident IGT (progression from NGT to IGT) had a significant association with increased risk of hypertension development by a HR of 1.61 (1.13–2.30) in model 2. It should be noted that the higher hypertension risk for newly-diagnosed IGT cases remained significant, even after adjustment for TG/HDL-C in model 3.
Results for female participants are presented in Table 3. Generally, change in glycemic state did not show a significant association with incident hypertension. Moreover, most of the effect sizes were located in the trivial zone.
Finally, after further adjustment for BMI change from phase II (baseline) to phase III, among men, the association of incident IGT with hypertension risk still remained significant with a HR of 1.68 (1.18–2.39; P-value: 0.004); moreover, changing from prediabetes to normoglycemia reached to a significant level [HR: 1.33 (1.00–1.75); P-value: 0.047]. Among women, on the other hand, results did not change.
Discussion
In this population-based prospective study, we examined the association of 3–year changes in glycemic state with incident hypertension during over 9 years of follow-up. We found that change in glycemic state had not a significant association with hypertension development among women. For men, on the other hand, although most of the effect sizes were at the trivial zone, incident IGT showed a significantly higher risk for hypertension development, compared to remaining NGT; this higher risk remained significant even after adjustment for TG/HDL-C and BMI change.
Among Tehranian adults, we previously found the prediabetes at the baseline as a hypertension risk factor in women, not men [11]. Moreover, by considering different components of dysglycemia [4], compared to FPG of <5.6 mmol/L, Tehranian female adults with FPG of 5.6–6.9 (IFG) and ≥7.0 mmol/L were at higher risk of hypertension in a multivariable model; however, this higher risk was not found for men. Considering 2hPG, we also showed that only women with 2hPG ≥ 11.0 mmol/L were at higher risk of hypertension development, and IGT did not increase the risk in either gender [4]. These findings mean that in our population, the effect of impaired glycemic state at baseline on hypertension risk is more prominent among women than men. Now, we found that change in glycemic state (especially NGT to IGT) can have association with hypertension development only among men. It can be suggested that among Tehranian men, the development of hypertension can be more influenced by the progression of glycemic state through 2hPG than the snapshot measurements of glycemic state at baseline. Similar to our results for men, among Korean adults, it was found that prediabetic participants were not significantly at higher risk of hypertension, in comparison with normoglycemia; however, compared to the maintaining glycemic state, the progression of normoglycemia to prediabetes, normoglycemia to T2DM, and prediabetes to T2DM significantly increased the risk of incident hypertension [18]; the authors suggested that the aggravation of IR may be an underlying mechanism. In our results, on the other hand, adjustment for TG/HDL-C, as a IR surrogate [27, 28], did not change the effect sizes prominently. It was suggested that the role of lipids (TG and HDL-C) in IR was more prominent in IFG than IGT [29]; therefore, it was expectable that adjustment for TG/HDL-C could not change the effect of incident IGT tangibly. Furthermore, the site of IR and type of beta-cell dysfunction differ between IFG and IGT [29]. Importantly, it is now clear that mainly due to the steroid hormones, many aspects of energy balance and glucose metabolism are regulated differently in men and women and influence their predisposition to cardiometabolic disorders. Premenopausal women are at lower risk of cardiometabolic disorders than men with the same age and BMI. This cardiometabolic advantage in women disappears after the menopause or when DM develops [30, 31]. About the higher risk for our male participants with reversion from prediabetes to normoglycemia, it could be a chance association.
The strengths of this study consist of standardized measurement techniques and assessment of sex-specific association by considering components of dysglycemia (IFG and IGT) separately.
A number of important limitations need to be considered. First, our sample size was limited, resulting in wide confidence intervals and insignificant P-values. In addition to our exploratory study, this relationship definitely should be reexamined in future confirmatory studies with larger sample sizes. However, most of our insignificant effect sizes were located in trivial zones (0.8–1.2), which were independent of sample size [32]. Second, more than 30% of our recruited participants were missed due to missing data. Although there were statistically significant differences between respondents and non-respondents, the values of differences were not clinically significant. Third, our study population included only urban residents of Tehran, and our findings may not be generalizable to rural areas. Fourth, TG/HDL-C was found as a predictor of IR among Tehranian residents [28]; however, TG/HDL-C has not been validated as a surrogate of IR among Iranian adults. Finally, data were not available for some potential hypertension predictors such as air pollution, dietary factors, and family history of hypertension.
Conclusion
To sum up, among Tehranian men, hypertension development was more influenced by the progression of dysglycemia (especially incident IGT) than snapshot assessment of glycemic state.
Summary
What is known about topic
-
It was suggested that prediabetes and diabetes increased the risk of incident hypertension.
-
However, the relation of change in glycemic state was not clearly investigated.
-
There is only one cohort study about this issue that found the progression of glycemic state as a strong determinant of hypertension.
What this study adds
-
In this population-based prospective study, we examined the association between 3–year changes in glycemic state with incident hypertension.
-
During over 9 years of follow-up, we found that change in glycemic state had not a significant association with hypertension development among women.
-
For men, incident IGT showed a significant higher risk, compared to remaining NGT.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Organization WH. Global status report on noncommunicable diseases 2014. World Health Organization; 2014.
Ogurtsova K, da Rocha Fernandes J, Huang Y, Linnenkamp U, Guariguata L, Cho NH, et al. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40–50.
Schlesinger S, Neuenschwander M, Barbaresko J, Lang A, Maalmi H, Rathmann W, et al. Prediabetes and risk of mortality, diabetes-related complications and comorbidities: umbrella review of meta-analyses of prospective studies. Diabetologia. 2021:1–11.
Parizadeh D, Rahimian N, Akbarpour S, Azizi F, Hadaegh F. Sex-specific clinical outcomes of impaired glucose status: a long follow-up from the Tehran Lipid and Glucose Study. Eur J Preventive Cardiol. 2019;26:1080–91.
Association AD. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2020. Diabetes Care. 2020;43:S14–31.
Nandhini LP, Kamalanathan S, Sahoo J. Definition, diagnostic criteria, screening, diagnosis, and classification of diabetes and categories of glucose intolerance. In: The Diabetes Textbook. Springer, 2019, pp 71–85.
Esteghamati A, Etemad K, Koohpayehzadeh J, Abbasi M, Meysamie A, Noshad S, et al. Trends in the prevalence of diabetes and impaired fasting glucose in association with obesity in Iran: 2005–2011. Diabetes Res Clin Pr. 2014;103:319–27.
Moazzeni SS, Ghafelehbashi H, Hasheminia M, Parizadeh D, Ghanbarian A, Azizi F, et al. Sex-specific prevalence of coronary heart disease among Tehranian adult population across different glycemic status: Tehran lipid and glucose study, 2008–2011. BMC Public Health. 2020;20:1510.
Organization WH. A global brief on hypertension: silent killer, global public health crisis: World Health Day 2013. World Health Organization, 2013.
Mohammadian Khonsari N, Shahrestanaki E, Ejtahed HS, Djalalinia S, Sheidaei A, Hakak-Zargar B, et al. Long-term trends in hypertension prevalence, awareness, treatment, and control rate in the Middle East and North Africa: a systematic review and meta-analysis of 178 population-based studies. Curr Hypertens Rep. 2021;23:41.
Asgari S, Moazzeni SS, Azizi F, Abdi H, Khalili D, Hakemi MS, et al. Sex-specific incidence rates and risk factors for hypertension during 13 years of follow-up: the tehran lipid and glucose study. Glob Heart. 2020;15:29–29.
Ferrannini E, Cushman WC. Diabetes and hypertension: the bad companions. Lancet. 2012;380:601–10.
De Boer IH, Bangalore S, Benetos A, Davis AM, Michos ED, Muntner P, et al. Diabetes and hypertension: a position statement by the American Diabetes Association. Diabetes Care. 2017;40:1273–84.
Bjørnholt JV, Erikssen G, Kjeldsen SE, Bodegård J, Thaulow E, Erikssen J. Fasting blood glucose is independently associated with resting and exercise blood pressures and development of elevated blood pressure. J Hypertension. 2003;21:1383–9.
Cheung BM, Wat NM, Tso AW, Tam S, Thomas GN, Leung GM, et al. Association between raised blood pressure and dysglycemia in Hong Kong Chinese. Diabetes Care. 2008;31:1889–91.
Geva M, Shlomai G, Berkovich A, Maor E, Leibowitz A, Tenenbaum A, et al. The association between fasting plasma glucose and glycated hemoglobin in the prediabetes range and future development of hypertension. Cardiovasc Diabetol. 2019;18:53.
Kuwabara M, Chintaluru Y, Kanbay M, Niwa K, Hisatome I, Andres-Hernando A, et al. Fasting blood glucose is predictive of hypertension in a general Japanese population. J Hypertension. 2019;37:167–74.
Jung JY, Oh C-M, Choi J-M, Ryoo J-H, Park SK. Long-term risk of hypertension in normoglycemia and prediabetes, and their relation to the change of glycemic state. Am J Hypertension. 2018;31:1042–8.
Britton KA, Pradhan AD, Gaziano JM, Manson JE, Ridker PM, Buring JE, et al. Hemoglobin A1c, body mass index, and the risk of hypertension in women. Am J Hypertension. 2011;24:328–34.
Mohan V, Anjana RM, Unnikrishnan R, Venkatesan U, Sankari GU, Rahulashankiruthiyayan T, et al. Incidence of hypertension among Asian Indians: 10 year follow up of the Chennai Urban Rural Epidemiology Study (CURES-153). J Diabetes Complications. 2020;34:107652.
Kabootari M, Hasheminia M, Azizi F, Mirbolouk M, Hadaegh F. Change in glucose intolerance status and risk of incident cardiovascular disease: Tehran Lipid and Glucose Study. Cardiovascular Diabetol. 2020;19:1–11.
Lee G, Kim SM, Choi S, Kim K, Jeong S-M, Son JS, et al. The effect of change in fasting glucose on the risk of myocardial infarction, stroke, and all-cause mortality: a nationwide cohort study. Cardiovascular Diabetol. 2018;17:1–10.
Azizi F, Ghanbarian A, Momenan AA, Hadaegh F, Mirmiran P, Hedayati M, et al. Prevention of non-communicable disease in a population in nutrition transition: Tehran Lipid and Glucose Study phase II. Trials. 2009;10:1–15.
Momenan AA, Delshad M, Sarbazi N, Rezaei Ghaleh N, Ghanbarian A, Azizi F. Reliability and validity of the Modifiable Activity Questionnaire (MAQ) in an Iranian urban adult population. Arch Iran Med. 2012;15:279–82.
Diagnosis ECot. Mellitus* CoD. Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care. 2003;26:3160–7.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr., et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289:2560–71.
Cordero A, Alegria-Ezquerra E. TG/HDL ratio as surrogate marker for insulin resistance. EJ Cardiol Pr [Internet]. 2009;8:16.
Derakhshan A, Tohidi M, Hajebrahimi M, Saadat N, Azizi F, Hadaegh F. Sex‐specific incidence rates and risk factors of insulin resistance and β–cell dysfunction: a decade follow‐up in a Middle Eastern population. Diabet Med. 2017;34:245–52.
Perreault L. Prediabetes. In: Feingold KR, Anawalt B, Boyce A, Chrousos G, de Herder WW, Dhatariya K, et al. (eds). Endotext. South Dartmouth (MA): MDText.com, Inc. Copyright © 2000-2022; 2000.
Tramunt B, Smati S, Grandgeorge N, Lenfant F, Arnal JF, Montagner A, et al. Sex differences in metabolic regulation and diabetes susceptibility. Diabetologia. 2020;63:453–61.
Goossens GH, Jocken JW, Blaak EE. Sexual dimorphism in cardiometabolic health: the role of adipose tissue, muscle and liver. Nat Rev Endocrinol. 2021;17:47–66.
Sullivan GM, Feinn R. Using effect size-or why the P value is not enough. J Grad Med Educ. 2012;4:279–82.
Acknowledgements
The authors would like to express their appreciation to the TLGS participants and staff for their kind cooperation.
Author information
Authors and Affiliations
Contributions
Study conception and design: SSM and FH. Analysis and interpretation of data: MH and FH. Drafting of the manuscript: SSM, SD and FH. Critical revision: RHA, FA and FH. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The ethics committee of the Research Institute for Endocrine Sciences of the Shahid Beheshti University of Medical Sciences approved the study proposal (IR.SBMU.ENDOCRINE.REC.1400.138).
Informed consent
Written informed consent was also obtained from all participants.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Moazzeni, S.S., Dehghani, S., Hasheminia, M. et al. Three-year change in glycemic state and the future risk of incident hypertension among Iranian adults: Tehran Lipid and Glucose Study. J Hum Hypertens 37, 944–949 (2023). https://doi.org/10.1038/s41371-022-00788-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41371-022-00788-5
- Springer Nature Limited