
Abstract
Childhood lead exposure has been shown to have a significant effect on neurodevelopment. Many of the biokinetics involved with lead biomarkers in children still remain unknown. Two hundred fifty (157 in the exposed group and 93 controls) children were enrolled in our study and lead exposed children returned for multiple visits for measurement of blood and bone lead and chelation treatment. We demonstrated that the correlation between blood and bone lead increased with subsequent visits. We calculated the blood lead half-life for 50 patients, and found a significant (p-value < 0.001) positive correlation with age. For ages 1–3 years (N = 17), the blood lead half-life was found to be 6.9 ± 4.0 days and for 3+ years it was found to be (N = 33) 19.3 ± 14.1 days. In conclusion, the turnover of lead in children is faster than in adults. Our results indicate that blood lead is a more acute biomarker of exposure than previously thought, which will impact studies of children’s health using blood lead as a biomarker.
Similar content being viewed by others


Introduction
Childhood lead (Pb) exposure has been linked with numerous adverse health impacts that have important implications throughout life. These include developmental neurological health disorders [1,2,3], among them effects on IQ and behavioral changes such as hyperactivity [4, 5], as well as hypertension, reproductive issues, and criminal activity [6,7,8,9,10,11]. For children in particular, it is important to understand the risks of Pb exposure, and for children already exposed, we need to identify the best methods for treatment or reducing exposure levels. In order to do this, the biokinetics of Pb in children needs to be understood. There is a significant gap in understanding of the action of Pb in the body for children, and we demonstrated in our previous work the significant differences and similarities children have in comparison to some adult biokinetic mechanisms [12].
This work expands on the previous findings, identifying the impact of age on biokinetic parameters and reevaluating the body burden of Pb. In this work, we identify the relationships between bone and blood Pb after removal of exposure sources. We use this as justification for our assumptions to determine the blood Pb half-life in children. Adult studies typically agree on a blood Pb half-life of ~20–30 days [13,14,15]. The literature has previously been unclear and limited for the identification of differences in the blood Pb half-life observed in children [16, 17]. In this study, we present more evidence to support our initial claims of a lower blood Pb half-life in children and present relationships of this data with age [12].
In addition to these primary goals, this work evaluates the use of portable x-ray fluorescence (pXRF) in comparison to K-shell x-ray fluorescence (KXRF) as a measure of bone Pb. This data was included in a previous manuscript, but additional results and analyses are presented here. The pXRF is a new measure of bone Pb, which is still being validated for use in large-scale studies. We provide some insight into the relationship observed between this measure of bone Pb, and the KXRF measured bone Pb and blood Pb in this study. We also evaluate the ability of the pXRF data to distinguish between exposed and unexposed individuals. These relationships will help to identify the ability of the pXRF for future studies of cumulative Pb exposure.
Methods
Study population
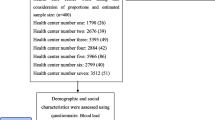
Both Pb-poisoned and non-Pb-poisoned children were recruited through Xinhua Hospital, Shanghai Jiaotong University, China. The study methods were detailed in our previous manuscript, but will be discussed briefly. Pb-poisoned children were recruited from children who were diagnosed as Pb poisoned, which means a blood Pb concentration >25 µg/dL at the time of the poisoning diagnosis. The primary source of Pb exposure for these children was identified and removed in most cases at point 1 in Fig. 1. For example, many of the children’s exposure was related to traditional medicines, the delivery of which were ceased at the visit prior to the first chelation. The process of source removal was different for each subject. The controls were recruited from children who visited the clinic for non-Pb-related reasons. All children had blood samples taken for Pb measurement and bone measured for Pb concentration using an advanced cloverleaf Cd-109 KXRF as well as a pXRF system. Control children had Pb measures taken only once. Pb-poisoned children had Pb measures taken multiple times each one following a chelation treatment using ethylenediaminetetraacetic acid (EDTA). Four of these children had chelation treatments prior to our first Pb measurements. Figure 1 shows the exposed group and number of chelation therapy visits before follow-up bone and blood Pb measurements in this group. Everyone in the original exposed group had their bone and blood Pb measured, but only twenty-four exposed patients had their bone and blood Pb measured prior to their third chelation treatment.

Number of exposed subjects with bone and blood Pb measurements after a specific number of chelation therapy treatments
The study received IRB approval from Purdue University and Xinhua Hospital. When recruited, a trained research assistant would present the subjects and their parents with the details of the study and the consent forms. Signed consent forms were received from the parents of each subject, as well as an assent form from any child age 7 or older.
KXRF bone Pb measurement system
The KXRF bone Pb measurement system was used to measure tibia bone Pb as a metric of each individual’s cumulative Pb exposure. The setup was the same as used in previous studies [18,19,20]. Before measurement, the subjects’ legs were cleaned using alcohol and EDTA cotton swabs to remove any Pb contamination. Each measurement was taken for 30 min while the subject watched a movie. XRF provides a point estimate of Pb concentration, which can be negative if an individual’s bone Pb is close to zero. It is important to include these negative values, as with their associated uncertainties, they are still a point estimate of that individual’s bone Pb.
The whole body effective radiation dose delivered to the subject from this system was estimated to be less than 5 µSv for this population [21].
Portable XRF device
The pXRF device used in this study was a customized device manufactured by Thermo Fisher (XL3t GOLDD+, Thermo Fisher Scientific Inc., Billerica, MA). The device specifications and optimization were discussed in a previous study [20]. The subject’s measurement site was cleaned before each measurement with the EDTA and alcohol cotton swabs. The measurement for pXRF was made after the blood collection and before the KXRF bone Pb measurement during the study visit. We estimated the entrance skin dose of the system was 21 mSv to a 1 cm2 area and the whole body effective dose was 2.4 μSv [22]. This can be compared to the whole body effective dose for a standard AP chest x-ray of about 100 μSv.
Blood Pb analysis
The blood of the subjects was collected in a Pb-free environment. We cleaned the subjects’ skin using alcohol swabs before sampling. The blood collection tubes along with the EDTA-K2 anticoagulants were measured to be Pb free before sampling. All the samples were frozen and kept at −80 °C immediately after the collection. Blood Pb concentrations were measured and analyzed by an atomic absorption spectrometer (AA900Z, PE) [23]. The sensitivity of our device was 0.01 μg/dL, and inter and intra assay variability was 5%.
Total body blood and bone Pb
Similar to our previous analysis, we calculated some values for the biokinetics of Pb in the body [12]. Here we will summarize briefly the analysis we performed in the previous study, and again with additional data and analysis in the results presented here. We were able to calculate total blood volume and total bone mineral content using a combination of age, height, and weight models from various sources in the literature [24, 25]. We used these sources as they gave us the predictions for a population very similar to the age distribution of the population in our study. To identify total blood volume, we used the three separate equations (dependent on age grouping), which would give blood volume based on height and weight variables. These equations are given in Table 1. For total body bone mineral content (TBBMC), we used Specker et al. [24], because they gave us a more detailed identification of individual measures based on age, height, and weight of our subjects. We used their equation to calculate total body bone area (TBBA), which was then used to calculate TBBMC. The equations used for this calculation are given in Table 1. For body fat percentage and calcium intake in the equations we assumed the averages of 27.9% and 23.7% for females and males, respectively, and 0.6 mg/kcal for calcium intake to be used in the equations in Table 1. These were the average values for the population in Specker et. al., which would be approximations of the averages for the similar population in this study [24]. These assumptions should not greatly change the results as removal of the terms with calcium intake and body fat percentage entirely only resulted in a 6% difference in average TBBMC. We used this to determine the estimated body burden for Pb in blood and bone.
Blood Pb half-life calculations
We used data from the follow-up visits (after the first chelation treatment) to calculate blood half-life for Pb-poisoned children. The bone remodeling rate was estimated from data for cortical bone in ICRP 70, page 35 [26], and for our calculation we used a power function to determine the appropriate turnover rate for each subject’s age as shown in Fig. 2. We converted the value for each subject to a bone to blood rate per day. For the calculation we assumed bone and blood Pb have reached equilibrium, because the Pb exposure source has been removed. Assuming equilibrium blood and bone Pb after removal of the primary source of Pb exposure and cessation of chelation treatment, we could identify the half-life of blood Pb using the following equation:
where \(\lambda _{{\mathrm{Blood}}\,{\mathrm{Pb}}}\) is the rate of blood Pb transferred to urine, feces, and other organs per day and is equal to \(\frac{{\mathrm{Ln}(2)}}{{T_{\frac{1}{2},\mathrm{blood}}}}\); \(\lambda _{\mathrm{Bone} \to \mathrm{Blood}}\) is the amount of bone Pb absorbed into blood per day found using the bone remodeling rate derived earlier from the data in ICRP 70 and Fig. 2 converted to a per day rate; \(T_{\mathrm{{Bone}}\,{\mathrm{Pb}}}\) is total bone Pb; and \(T_{{\mathrm{Blood}}\,{\mathrm{Pb}}}\) is total blood Pb. Total bone Pb can be estimated by multiplying our value for TBBMC by our KXRF bone Pb value (µg/g bone mineral). The bone Pb value used was the second visit at time point 2 in Fig. 1. Total body blood Pb is estimated from total body blood volume multiplied by the blood Pb concentration taken at point 2 in Fig. 1, which will satisfy the equilibrium assumption and source removal after the visit at point 1 in Fig. 1. Finally, to convert the \(\lambda _{\mathrm{Bone} \to \mathrm{Blood}}\) value to more familiar units we used the formula \(\frac{{\mathrm{Ln}(2)}}{{\lambda _{\mathrm{Bone} \to \mathrm{Blood}}}}\) to get blood Pb half-life in days.

Bone remodeling rate for different age groups with data taken from ICRP 70 page 35
Statistical methods
Linear regressions were used to determine correlation values and levels of significance of relationships between KXRF bone Pb and blood Pb, pXRF bone Pb and blood Pb, and age and blood Pb half-life. The biomarker data is skewed from normal as a result of the group being more highly exposed, but this data was used primarily for comparison between biomarker values. The blood Pb half-life data was normally distributed. The KXRF bone Pb data was excluded from our analysis if the final uncertainty was >10 µg/g, as has been done in previous studies using KXRF [27]. This would indicate an excessive amount of movement during the measurement or a measurement taken for less than 30 min. Portable XRF data was excluded if the measurement time was <2 min. We did not exclude data based on the uncertainty measurements given from pXRF, since the values that would indicate an erratic measurement are not well known due to the more recent development of the pXRF measurement system. The difference measures between age groups for blood Pb half-life and patient and control measures used rank sum tests to identify significant differences with p-values reported. The statistical analysis was done using R version 3.3.3.
Results
The earlier results of the study were summarized in a previous publication by Specht et al. 2016 [12]. Summary data and analysis were completed and discussed in that manuscript. The current study had 250 participants (170 male and 80 female) with average age 5.7 ± 3.1 years. One hundred fifty-seven, point 1 in Fig. 1, were Pb poisoned and in the exposed group with 93 being in the control group.
Bone and blood Pb concentrations and age, sex, height, and weight measurements in the study population
Table 2 summarizes the data for blood Pb and bone Pb measurements between the exposed and control groups. The blood and bone Pb data reflect only the first measurements for the exposed group. Note that for the exposed group, the average blood Pb is lower than recruitment criteria, because some subjects had a time gap between being diagnosed as Pb poisoned and being enrolled in the study. However, with the blood Pb being high at a previous time, the bone Pb should still reflect the exposed status. Table 3 summarizes the age, sex, height, and weight distributions in the population for different age groups.
Correlation between blood and KXRF bone Pb concentrations
In our previous analysis with these children, we identified a strong correlation between bone and blood Pb in subjects with R2-values of about 0.6 (N = 86). The correlation for just exposed and all subjects remained the same as before and is presented in Fig. 3 for the exposed group (N = 157). We present in Fig. 4 the correlation among Pb-poisoned children between KXRF bone Pb and blood Pb (N = 59) from only the second measurements prior to the second chelation treatment (four children with chelation treatments before our first measurements were excluded). This corresponds with bone and blood Pb measures taken at point 2 in Fig. 1. The p-value of this regression was <0.001. Figure 4 shows a non-linear relationship between blood and KXRF bone Pb data for subjects that have at least one follow-up visit. This was found to be significantly different from the linear model using a likelihood ratio test comparing the non-linear and linear regressions, which resulted in a p-value of 0.01. Then, we isolated those Pb-poisoned children who had undergone at least two chelation treatments (N = 24) prior to bone and blood Pb measures. A significant correlation (p-value < 0.001) is presented in Fig. 5. This corresponds with point 3 in Fig. 1. For the Pb-poisoned children that completed at least one visit (N = 157), there was a weak (R2 = 0.11, p < 0.01) negative correlation between their initial blood Pb measurement and age. For Pb-poisoned children at their second visit (N = 59), there was an insignificant (R2 = 0.05, p = 0.08) trend for a negative correlation between blood Pb and age. At the third measurement time (N = 24), there was no observed trend between blood Pb and age.

Correlation between blood and KXRF bone lead for measures at the initial visit (point 1 in Fig. 2 N = 157) for lead-poisoned subjects (R2 without highest point is 0.6174)

Correlation between blood and KXRF bone lead for measures at second visit (point 2 in Fig. 2 N = 59) for lead-poisoned subjects and significant second order polynomial relation (R2 without two highest points is 0.691 and 0.656 for the polynomial and linear fit, respectively)

Correlation between blood and KXRF bone lead at third visit (point 3 in Fig. 2 N = 24) for lead-poisoned subjects (R2 without highest point is 0.866)
pXRF bone Pb results between exposed and control groups
The correlation between KXRF and pXRF bone Pb remained similar to that reported previously [12]. With the inclusion of the additional data and isolating only exposed children with pXRF and KXRF bone Pb measurements at time point 1 in Figure 1 (N = 157), the R2 was 0.18 with a p-value of <0.001. The correlation between blood Pb and pXRF bone Pb was significant including all subjects and isolating exposed (p-value of <0.001 and 0.001 with an R2 of 0.07 and 0.06, respectively). The correlation between pXRF bone Pb and blood Pb for exposed individuals can be seen in Fig. 6.

Correlation between blood lead and pXRF measured bone lead measurements at initial study visit for exposed subjects (N = 157)
We performed a rank sum difference test between exposed and control groups (Table 2) to identify the ability of the pXRF to determine exposure status and found that the exposed and control groups were significantly different with a p-value of 0.0003. The average pXRF measured bone Pb for the exposed group was 28.2 ± 53.6 ppm and for the control group was 3.8 ± 52.8. The average uncertainty for the pXRF bone Pb measurement was 9.6 ± 2.6 ppm, and did not differ significantly between Pb-poisoned and non-Pb-poisoned children.
Bone and blood Pb burden
We determined an estimation for body burden of blood and bone Pb. With the additional data in our study, the difference between ages for body burden of Pb proved to be null with an average of 97.2 ± 1.5 percent bone Pb compared to blood Pb burden for ages 1–3 and 97.3 ± 1.7 percent for ages 3+ found in our 154 subjects for this calculation.
Blood Pb half-life calculations
The blood Pb half-life was calculated among only 50 of the 59 exposed subjects that had all the necessary measurements to perform the calculation, because eight subjects did not show decreases in blood Pb at the 2nd measurement and were removed. One subject had a bone Pb value of <2 µg/g at the second visit, which created an outlying data point and was removed. Not showing decreased blood Pb suggests that these subjects were still being exposed to Pb, and thus did not meet the assumptions made for our calculation. Blood Pb half-life results are presented in Table 4 and Fig. 7. Figure 7 shows a significant correlation between age and blood Pb half-life with a p-value < 0.001 (slope of 2.92 with 95% confidence interval (2.35, 3.49)). No significant differences or trends between blood Pb half-life and sex were identified. Summary of all the data used for calculation of the blood Pb half-life is shown in the supplement.

Correlation between blood lead half-life and age (N = 50)
Discussion
This study further explored Pb biokinetics in children and expanded the analysis from our previous publication [12]. With the additional data we found a significant relationship between age and blood Pb half-life, which demonstrates significant evidence for Pb biokinetic differences between children and adults. We demonstrated in Figs. 3–5 that as Pb in bone and blood reached equilibrium the correlation between these two biomarkers became much stronger. We found significant differences in pXRF measured bone Pb between exposed and control groups.
Demonstration of a stronger correlation between bone and blood Pb in individuals undergoing follow-up chelation treatment helps to validate our hypothesis of equilibrium between these two Pb storage sites. At the initial measurement the correlation value was lower, because it was offset by the still present exogenous Pb exposure for many of the exposed subjects. Some subjects did have blood Pb reflective of source removal beforehand, which contributes to the already high correlation observed. At point 1 in Fig. 1, the removal of the source of Pb exposure was achieved for almost all exposed subjects. After the effects of chelation subsided, the bone and blood Pb was in equilibrium for almost all of the subjects. This validates our use of this assumption for the calculation of blood Pb half-life and for calculation of bone turnover rate in these subjects.
It seems that there could be a non-linear relationship between bone and blood Pb as shown in Fig. 4. For the highest points, it seems that there was less Pb in blood than was predicted by the model, which would lead us to conclude that there is a saturation value for the amount of Pb resorbed from bone to blood. This would imply that heavily exposed individuals might have more difficultly removing Pb stores from the body than is estimated by current biokinetic models.
We expected the very strong correlation observed in Fig. 5 between third follow-up measured bone and blood Pb to be confounded by age. As shown in Fig. 2, the age-dependent bone remodeling rate is incredibly dependent on age early in life, and thus we would expect some variation between individuals based on age. However, we did not find significant relationships between blood Pb and age at follow-up visits. We would expect the dependency on age to continue throughout the study based on the age dependence of the transfer rate between bone and blood. There was no relationship between age and time to follow-up, which could have influenced this relationship. One possible explanation is that there are second order kinetic effects. The turnover rate is typically taken as a first order kinetic model, but it is possible during the transient period after chelation, all subjects had similar bone resorption driving Pb from bone due to transient second order effects. We found a second order relationship between bone and blood Pb at extreme values (Fig. 4), and the same could be true for low values of blood Pb as well. Since the time between visits in our study was short, the age dependency of bone turnover was lost due to these transient effects. More study would need to be done to identify whether this is the case.
The pXRF bone Pb data remained very similar in relation to KXRF bone Pb measurements as reported previously. In this final dataset, we had enough controls to determine that the pXRF measurements were significantly different between the exposed and the control groups. The average uncertainty for the pXRF measurements was about 10 µg/g. This is similar to the uncertainty associated with conventional KXRF systems in pediatric populations. Those systems were used widely to study lower-level, environmentally exposed populations, which suggest that the pXRF should also be usable in such populations. In older populations exposed to leaded gasoline, it is highly likely that the bone Pb levels are 10 µg/g or higher, which would be greater than the average uncertainty in this study. Children in general will have thicker overlying soft tissue than adults, and will have higher uncertainty in their measurements [28, 29].
The correlation between blood Pb and pXRF bone Pb is much lower than for KXRF bone Pb and blood Pb. It is likely that these two devices, which use different energies, are sampling different portions of the bone. The different portions of the bone likely relate differently to blood Pb and to each other. Also, since the subjects of this study were children, this issue is complicated further as studies of Pb biokinetics and storage in children are limited. This makes it difficult to assess the abilities of the device in comparison to some standard. In our previous work, we showed a correlation (R2 = 0.196) between KXRF and pXRF bone Pb measurements, which may indicate at least partial agreement between the biomarkers. Since this is a new measurement system, further work needs to be done to determine exactly what biomarker is being measured using the pXRF, and how it may relate to the traditional KXRF measurement of bone Pb and the biokinetics of Pb in the body.
This extended study confirmed the conclusion made in our previous paper that the majority of the Pb body burden (>90%) in a child is in the bone. In the previous study we observed trends toward age related differences in the proportion of Pb in bone (92.3% at 1–3 years vs. 96.5% at older than 3), which we have now shown to clearly have no difference based on age. In the previous paper, we had only 7 subjects in the group between 1–3 years of age, and our new analysis included 46 subjects in this age group.
We were able to build upon our previous calculations of blood Pb half-life, and with additional data were able to calculate the blood Pb half-life for 50 of our subjects. Our results suggest that blood Pb half-life is shorter in children than adults. The adult blood Pb half-life is generally accepted as ~20–30 days [13,14,15]. In our previous manuscript we discussed two other studies that looked at blood Pb half-life in children and got differing results [16, 17]. The study by Manton et al. [16] did not account for bone Pb, which would artificially increase the half-life in blood, since that is the primary storage compartment in the body. The study by Duggan et al. [17] only had two subjects, but was in better agreement with the results shown here. The main limitation of our study is the assumption of exposure source removal, but we believe in most cases this was satisfied for our subjects. As mentioned in our previous manuscript, this will have an impact on monitoring exposure levels in children. Since the blood Pb levels will change much more rapidly in children, bone may be a better marker for exposure levels in this particularly vulnerable group.
Conclusions
The biokinetics of Pb in children are faster than in adults. We found blood Pb half-life changes with age and was on average 6.9 days for children ages 1–3 years old and 19.3 days for children 3–14 years old. Bone Pb accounts for over 95% of Pb body burden for children. For Pb-poisoned children, blood Pb is highly correlated with bone Pb after the removal of external Pb exposure, which indicates significant endogenous exposures for these children. Finally, pXRF can be used to effectively identify Pb exposed individuals from unexposed subjects in a study.
References
Canfield RL, Henderson CR, Cory-Slechta DA, Cox C, Jusko TA, Lanphear BP. Intellectual impairment in children with blood lead concentrations below 10 μg per deciliter. N Engl J Med. 2003;348:26.
Jusko TA, Henderson CR, Lanphear BP, Cory-Slechta DA, Parsons PJ, Canfield RL. Blood lead concentrations 10 microg/dL and child intelligence at 6 years of age. Environ Health Perspect. 2008;116:243–8.
Lanphear BP, Hornung R, Khoury J, Yolton K, Baghurst P, Bellinger DC, et al. Low-level environmental lead exposure and children’s intellectual function: an international pooled analysis. Environ Health Perspect. 2005;113:894–9.
Hong SB, Im MH, Kim JW, Park EJ, Shin MS, Kim BN, et al. Environmental lead exposure and attention deficit/hyperactivity disorder symptom domains in a community sample of South Korean school-age children. Environ Health Perspect. 2015;123:271–6.
Huang S, Hu H, Sánchez BN, Peterson KE, Ettinger AS, Lamadrid-Figueroa H, et al. Childhood blood lead levels and symptoms of attention deficit hyperactivity disorder (ADHD): a cross-sectional study of Mexican children. Environ Health Perspect. 2016;124:868–74.
Navas-Acien A, Guallar E, Silbergeld EK, Rothenberg SJ. Lead exposure and cardiovascular disease-a systematic review. Environ Health Perspect. 2007;115:472–82.
Pant N, Kumar G, Upadhyay AD, Patel DK, Gupta YK, Chaturvedi PK. Reproductive toxicity of lead, cadmium, and phthalate exposure in men. Environ Sci Pollut Res Int. 2014;21:11066–74.
Wu HM, Lin-Tan DT, Wang ML, Huang HY, Lee CL, Wang HS, et al. Lead level in seminal plasma may affect semen quality for men without occupational exposure to lead. Reprod Biol Endocrinol. 2012;10:91.
Boutwell BB, Nelson EJ, Emo B, Vaughn MG, Schootman M, Rosenfeld R, et al. The intersection of aggregate-level lead exposure and crime. Environ Res. 2016;148:79–85.
Wright JP, Dietrich KN, Ris MD, Hornung RW, Wessel SD, Lanphear BP, et al. Association of prenatal and childhood blood lead concentrations with criminal arrests in early adulthood. PLoS Med. 2008;5:e101.
National Toxicology Program N. NTP monograph on health effects of low-level lead. NTP Monogr. 2012;xiii, xv:148.
Specht AJ, Lin Y, Weisskopf M, Yan C, Hu H, Xu J, et al. XRF-measured bone lead (Pb) as a biomarker for Pb exposure and toxicity among children diagnosed with Pb poisoning. Biomarkers. 2016;21:347–52.
Nilsson U, Attewell R, Christoffersson JO, Schutz A, Ahlgren L, Skerfving S, et al. Kinetics of lead in bone and blood after end of occupational exposure. Pharmacol Toxicol. 1991;68(6):477–84.
EPA. US. Integrated science assessment (ISA) for lead (final report, Jul 2013). Washington, DC, EPA/600/R-10/075F: US Environmental Protection Agency; 2013.
Leggett RW. An age-specific kinetic model of lead metabolism in humans. Environ Health Perspect. 1993;101:18.
Manton WI, Angle CR, Stanek KL, Reese YR, Kuehnemann TJ. Acquisition and retention of lead by young children. Environ Res. 2000;82(1):60–80.
Duggan MJ. The uptake and excretion of lead by young children. Arch Environ Health. 1983;38:246–7.
Nie H. Studies in bone lead: a new cadmium-109 XRF measurement system. Modeling bone lead metabolism. Interpreting low concentration data. PhD thesis, McMaster Univ. (Canada) 2005.
Nie H, Chettle DR, Stronach IM, Arnold ML, Huang SB, McNeil FE, et al. A Study of MDL improvements for the in vivo measurement of lead in bone. Nucl Instrum Methods Phys Res B. 2004;213:4.
Specht AJ, Weisskopf M, Nie LH. Portable XRF technology to quantify Pb in bone in vivo. J Biomark. 2014;2014:9.
Nie H, Chettle D, Luo L, O’Meara J. Dosimetry study for a new in vivo X-ray fluorescence (XRF) bone lead measurement system. Nucl Instrum Methods Phys Res B. 2007;263:225–30.
Nie H, Sanchez S, Newton K, Grodzins L, Cleveland RO, Weisskopf MG. In vivo quantification of lead in bone with a portable x-ray fluorescence system—methodology and feasibility. Phys Med Biol. 2011;56(3):N39–51.
Liu KL. [Review of atomic spectroscopy]. Guang Pu Xue Yu Guang Pu Fen Xi. 2005;25:95–103.
Specker B, Johannsen N, Binkley T, Finn K. Total body bone mineral content and tibial cotrical bone measures in preschool children. J Bone Miner Res. 2001;16:2298–305.
Linderkamp O, Versmold HT, Riegel KP, Betke K. Estimation and prediction of blood volume in infants and children. Eur J Pediatr. 1977;125:227–34.
ICRP. Publication 70, basic anatomical and physiological data for use in radiological protection—the skeleton. Ann ICRP. 1995;25:1–80.
Ji JS, Power MC, Sparrow D, Spiro A 3rd, Hu H, Louis ED, et al. Lead exposure and tremor among older men: the VA normative aging study. Environ Health Perspect. 2015;123:445–50.
Rosen JF, Markowitz ME, Bijur PE, Jenks ST, Wielopolski L, Kalef-Ezra JA, et al. Sequential measurements of bone lead content by L X-ray fluorescence in CaNa2EDTA-treated lead-toxic children. Environ Health Perspect. 1991;93:271–7.
Pejović-Milić A, Brito JA, Gyorffy J, Chettle DR. Ultrasound measurements of overlying soft tissue thickness at four skeletal sites suitable for in vivo x-ray fluorescence. Med Phys. 2002;29:2687–91.
Acknowledgements
The authors would like to acknowledge Dr. Jian Xu and Yanfen Lin for their tremendous help on subject recruitment and data collection. The research could not be done without them. The authors would also like to thank the MOE-Shanghai Key Laboratory of Children’s Environmental Health at Xinhua Hospital affiliated to Shanghai Jiao Tong University School of Medicine for providing much needed support and resources for the project. This work was supported by the Nuclear Regulatory Commission (NRC) Faculty Development Grant NRC-HQ-84-14-G-0048, National Natural Science Foundation of China (81373016, 30901205), National Basic Research Program of China (“973” Program,2012CB525001), Shanghai Science and Technology Committee (124119a1400), Purdue Ross Fellowship, and Purdue US-China visiting scholar network travel grant program.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Specht, A.J., Weisskopf, M. & Nie, L.H. Childhood lead biokinetics and associations with age among a group of lead-poisoned children in China. J Expo Sci Environ Epidemiol 29, 416–423 (2019). https://doi.org/10.1038/s41370-018-0036-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41370-018-0036-y
- Springer Nature America, Inc.
Keywords
This article is cited by
-
Portable x-ray fluorescence for bone lead measurement: Current approaches and future directions
Current Environmental Health Reports (2024)
-
Bone lead measurements of live condors in field to assess cumulative lead exposure
Environmental Science and Pollution Research (2024)
-
Identifying periods of heightened susceptibility to lead exposure in relation to behavioral problems
Journal of Exposure Science & Environmental Epidemiology (2022)