
Abstract
Background
This study aimed to investigate the influence of body weight, exercise modality, and pace on physiological and perceptual responses to determine the relation between perceptual and physiological responses.
Methods
Aerobically untrained, normal weight, and overweight males and females participated. Participants were randomly assigned to one exercise condition for a 1-mile walk.
Results
Prescribed pace resulted in a greater physiological stress than self-selected pace (all p < 0.001) through blood lactate (1.3 ± 0.4 vs 1.7 ± 0.5 mmol), systolic blood pressure (128.9 ± 10.3 vs 139.2 ± 13.2 mmHg), heart rate recovery (2.1 ± 1.7 vs 4.5 ± 2.6 min), oxygen consumption (15.1 ± 2.6 vs 18.1 ± 3.6 ml/kg/min), heart rate (111.7 ± 16.6 vs 134.4 ± 8.3 bpm), and energy expenditure (5.5 ± 1.4 vs 6.8 ± 1.7 kcal/min). Overweight individuals exhibited higher values than normal weight for heart rate (113 ± 8.8 vs 125.5 ± 13.2 bpm, p < 0.001), percentage of max heart rate (60.7 vs 69.0%, p < 0.001), percent of VO2peak (42.2 vs 55.6%, p < 0.001), and total energy expenditure (100.9 ± 27.4 vs 114.1 ± 33.5 kcal, p = 0.022). Greater perceived effort was seen on a treadmill (6.3 ± 0.5 vs 12.5 ± 2.0 RPE, p < 0.001) and at prescribed pace (6.5 ± 1.1 vs 8.9 ± 1.9 RPE, p < 0.001).
Conclusion
A novel finding of this study was the increased physiological stress and perception of effort on a treadmill and at a prescribed pace, while total energy expenditure showed no significant differences. This could indicate an unfavorable perception and less affective response to the treadmill modality. These results indicate exercise at self-selected pace in preferred environments promotes enjoyable experiences with similar health benefits as those during prescribed higher intensity exercise.
Similar content being viewed by others


Introduction
The American College of Sports Medicine (ACSM) lists obesity and physical inactivity as major risk factors for coronary artery disease [1, 2]. Prevalence of inactivity remains high despite evidence continuing to support the inverse relation between physical activity (PA) and premature mortality, cardiovascular disease, stroke, osteoporosis, type 2 diabetes mellitus, cancer, depression, cognitive function, obesity, and many other debilitating conditions [1, 3,4,5]. Physical inactivity is one of a plethora of complex, interrelated factors contributing to obesity. The cultural, psychosocial, physiological, and biological influences make it difficult to accurately identify exact etiology [6]. Nevertheless, it can be argued an individual becomes obese from excessive energy intake chronically coupled with insufficient energy expenditure (EE).
Accurate knowledge of EE during exercise is needed for effective weight management interventions, while additional focus should be directed toward the increased EE of obese adults compared to normal weight adults regardless of exercise intensity [7,8,9]. The inclusion of PA recommendations remains a vital part of weight management and continues to be an emphasis of major organizations including the ACSM, Center for Disease Control, American Heart Association, and National Heart, Lung, and Blood Institute [8, 10]. The Surgeon General, American Heart Association, and ACSM endorse a recommendation of at least 30 min of moderate intensity aerobic PA on most, preferably all, days of the week [6, 11, 12]. However, there remains a paucity of the literature investigating exercise intensities which simultaneously promote physiological and psychological benefits.
Despite the knowledge of health benefits associated with PA, promoting behavioral change remains a continuous and multifaceted challenge. Development of effective and positively perceived programs may aid in integrating PA into inactive lifestyles, as well as maintenance of active lifestyles [1, 3, 13]. Barriers to initiation may include disruptions in routine, financial cost, lack of time, social support, or access to facilities, and dislike for or misinterpretation of different levels of intensity [1, 14]. Following initiation of exercise, prolonged adherence is imperative and success relies partly on proper prescription conforming to the individual’s lifestyle and functional capacity along with positive affective valence [1, 6, 14, 15]. Walking can be considered a lifestyle classification of PA and is a popular, convenient method of weight management, and assists in reduction of cardiovascular disease risk [7, 9,10,11,12]. Moderately intense walking speeds, between 3 and 4 mph, are recommended by ACSM to maintain an active, healthy lifestyle; however, Browning et al. [7] reported the mean walking speed of overweight adults to be ~2.68 mph. The discrepancy between the recommended and preferred walking speeds among overweight individuals creates concern when considering general PA guidelines. Walking at a prescribed pace may be an exhaustive task with studies showing greater than 50% of an overweight individuals’ maximal aerobic capacity being reached (~56%) [9]. Similarly, Hall et al. [14] observed when obese participants were asked to increase workload to the high end of the moderate intensity range from their preferred walking pace, 68% of participants could not complete the prescribed regimen and workload had to be reduced after 15–20 min. Limited research has compared the energetic cost of overweight with normal weight adults during walking [11], especially at alternate speeds and in different environments.
A potential method to combat prescribing inappropriate intensity is using self-selected pace. Studies have shown participants in exercise programs tend to exercise at self-selected intensities rather than abide to prescribed intensity [1, 3, 4]. A self-selected walking pace performed as continuous exercise aids in weight loss and providing desired health benefits [4]. By exercising at self-selected intensities, positive parameters of perceived exertion and affect may contribute to individuals’ intrinsic motivation and exercise program adherence. However, exercising at prescribed intensity may elicit reduced affective response thus reducing exercise program adherence [13, 16, 17].
Exercise prescription is multifaceted and specific to everyone, although often, these components are not individualized creating inquiry as to whether the program is providing optimal benefits. Exercise prescriptions should be modified based on the individual’s daily PA, functional capacity, health status, stress level, psychophysiological perceptions, and goals [18]. Those unwilling or unable to meet ACSM exercise guidelines can still benefit from PA, reducing physically inactive behavior [19]. Previous research has shown alternate modalities of exercise provide differing physiological and perceptual responses in normal weight individuals [17]. Therefore, the purpose of the present investigation was to identify physiological and perceptual differences to walking in two commonly used environments (indoor track and treadmill) and between a prescribed moderate intensity (percent of heart rate reserve (HRR)) and self-selected intensity. We also aimed to determine differences between normal weight and overweight individuals and between sexes.
Methods
Participants
Following power analysis, untrained individuals (N = 160) were recruited via informational fliers and stratified by sex and weight status (normal weight and overweight as described below), then were assigned to one of the four weight status categories: overweight males (n = 40), normal weight males (n = 40), overweight females (n = 40), and normal weight females (n = 40). Participants were considered untrained, defined as <60 min of aerobic exercise per week for the last 3–6 months, which was verified through a health history questionnaire (PAR-Q). Weight status was determined through body fat percentage (BF%) using dual-energy x-ray absorpitometry [(DXA) (Hologic Delphi, QDR series, Bedford, MA)] and standard ranges for classification [20]. Each session commenced at the same time of day for all participants and they were instructed to follow their regular nutritional pattern while refraining from exercise within 72 h prior to initial testing session. All procedures were approved by university Institutional Review Board.
Testing sessions
The first testing session consisted of completing informed consent and obtaining anthropometric measurements including body weight, height, and BF%. Body weight was measured using a calibrated platform scale with digital display (Health O Meter, Electronic Doctor’s Scale), while height was obtained from a portable stadiometer (Seca 213, Seca, Germany). BF% was determined using DXA as mentioned previously. Familiarization for the portable metabolic system (Cosmed K4b2, Rome, Italy), Borg Rating of Perceived Exertion (RPE) scale, Category Ratio Pain Intensity Scale (CR-10), and blood lactate (BLa) analysis equipment (Lactate Plus, Nova Biomedical, Waltham, MA) also took place. BLa sampling procedure followed previously established methodology [21,22,23,24]. Resting HR and blood pressure (BP) were assessed following a 5-min quiet supine rest using a Polar HR monitor and automated BP cuff (Omron HEM-907XL, Bannockburn, USA), respectively. Each participant’s self-selected walking pace was determined using predetermined distance trials explained in previous research [8, 11, 25]. This session concluded with a peak oxygen uptake (V̇O2peak) test until volitional fatigue following the Bruce protocol.
Using parallel design, participants were then randomly assigned to one of the four exercise conditions: (1) 1-mile walk at self-selected pace on an indoor track; (2) 1-mile walk at self-selected pace on a treadmill; (3) 1-mile walk at a prescribed pace to elicit 50–70% of heart rate reserve (HRR) on an indoor track; or (4) 1-mile walk at a prescribed pace to elicit 50–70% of HRR on a treadmill. The HRR range was selected to represent, in part, the recommendations of ACSM while achieving an average at the higher end of moderate intensity exercise [20]. Exercise conditions on the indoor track required the completion of 8.5 laps while staying in the middle lane. All sessions were completed within controlled environment from temperature, relative humidity, and ambient noise.
Following a minimum of 72 h, the second testing session (within a 7-day period) consisted of repeat body weight measurement along with resting HR, BLa, and BP. Participants then completed a 1-mile walk according to their designated exercise condition. For all exercise conditions, walking pace was continuously monitored and participants were instructed to adjust their pace accordingly via hand signals from the researchers to avoid motivational speech. Perceptive variables (RPE and CR-10) were nonverbally communicated and collected upon each lap on the track and time equivalent on the treadmill. Metabolic parameters and HR were continously collected throughout the exercise via Cosmed K4b2 unit. Once each condition was completed, BLa and BP measurements were obtained post exercise.
Statistical analysis
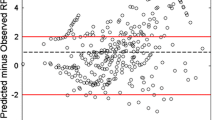
All data were organized according to the four independent (prescribed and self-selected pace, track and treadmill, normal weight and overweight, male and female) and two dependent (physiological and perceptual responses) variables of interest. Data have been presented as mean ± standard deviation. All variables were used for a between groups analysis using factorial ANOVA procedure. Initially, a factorial ANOVA was used for the evaluation of effect of weight status, modality, pace, and sex on physiological and perceptual values. Relations were determined between a perceptual measure (final RPE) and a physiological measure (final HR) for all between group conditions using multiple regression analysis. For purpose of these analyses, HR values were used to predict RPE values across all exercise conditions. All statistical analyses were conducted using SPSS software (version 22, SPSS, Inc., Chicago, IL). Statistical significance was defined as a p value less than 0.05.
Results
Males exhibited significantly greater (p < 0.001) descriptive values (Table 1) including height and weight, while females had a significantly greater BF% (p < 0.001). Males demonstrated significantly higher values than females for V̇O2peak (41.4 ± 7.9 and 33.6 ± 7.9 ml/kg/min, respectively, p < 0.001), while females achieved a higher percentage of maximal heart rate (%HRmax) during exercise (62.7 vs 67%, p < 0.001). No sex differences were observed for resting HR or resting BLa. Speed did not significantly differ between sexes nor the normal weight and overweight participants during the self-selected walking paced condition. Normal weight participants achieved higher V̇O2peak values compared to overweight (41.6 ± 6.6 and 33.3 ± 7.9 ml/kg/min, respectively, p < 0.001), while resting BLa showed no difference between groups (1.3 ± 0.4 vs 1.3 ± 0.5, respectively).
Physiological responses to modalities and pace between weight status
Table 2 displays results separated by condition and weight status for each physiological outcome variable effected by pace. A significant interaction was found between modality and pace between pre- and postexercise BLa levels. Prescribed intensity resulted in a significantly increased BLa (p < 0.001) on both the track and treadmill (1.8 ± 0.5 and 1.2 ± 0.4 mmol, respectively). Furthermore, prescribed track intensity increased BLa (2.0 ± 0.5 mmol) to a greater extent than the treadmill (1.5 ± 0.4 mmol, p = 0.041). No significant increase in BLa was seen at self-selected pace for either track or treadmill.
Average self-selected speed was 3.01 mph, while prescribed pace was 3.45 mph. In order to reach the 50–70% of HRR, participants increased their walking speed 17.38% above their self-selected pace during the prescribed pace conditions. V̇O2 (ml/kg/min) during prescribed pace (18.9 ± 3.3) was significantly greater (p < 0.001) than self-selected pace (14.9 ± 2.4) along with mean exercise HR (133 ± 8 vs 109 ± 13 bpm, respectively, p < 0.001). Participants exercised at a significantly greater %HRmax (73.9%) and VO2peak (57.4%) during prescribed intensity (p < 0.001 and p < 0.001) as compared to self-selected (54.5% and 43.1%, respectively) leading to potentially excessive elevated intensity. The prescribed paced conditions resulted in significantly higher EE (6.5 ± 1.5 vs 5.5 ± 1.3 kcal/min, p < 0.001), although the difference yields little clinical relevance as differences were within 1 kcal/min. Total EE was significantly higher for overweight participants in all conditions (113.2 ± 33.6 vs 91.9 ± 27.4 kcal, p = 0.019). Overweight participants achieved a higher HR which led to a greater %HRmax as compared to normal weight participants (60.7 vs 69.0%, respectively, p < 0.001). This trend was also seen in a greater %VO2peak during exercise for overweight participants (42.2 vs 55.6%, p = 0.003).
Perceptual responses to modalities and intensities between weight status
Perceptual response descriptive statistics by condition and weight status and differences due to pace and modality can be found in Tables 3 and 4, respectively. Average RPE was significantly higher during prescribed pace (12.6 ± 8.2) compared to self-selected pace (8.2 ± 0.9) irrespective of modality (p < 0.001). Similarly, the prescribed pace resulted in higher final RPE values in both modalities (6.5 ± 1.1 vs 8.9 ± 1.9 RPE, p < 0.001). Mean CR-10 was significantly higher on the treadmill and track at prescribed pace compared to self-selected pace (p = 0.005). Final RPE was significantly higher for the treadmill compared to the track at both self-selected and prescribed pace (6.3 ± 0.5 vs 12.5 ± 2.0 RPE, p < 0.001). Lastly, the CR-10 scores showed a higher score on the treadmill (2.2 ± 0.6) compared to the track (0.07 ± 0.2) regardless of pace (p = 0.038).
Relation between physiological and perceptual responses across conditions
Regression analysis elucidated no significant difference in the relation between physiological and perceptual responses across conditions (p = 0.91). Weight status did not influence the relation between responses (p = 0.1). When comparing variability in RPE between exercise conditions, prescribed pace was significantly higher than both modalities at self-selected pace (p < 0.001). Further, greater variability in RPE was observed for the treadmill prescribed pace compared to both modalities at self-selected pace (p < 0.001).
Discussion
Interaction of modality and pace on physiological responses
The first study aim was determining the effect of modality, pace, weight status, and sex on physiological and perceptual response. Expected sex differences were seen for anthropometrics and males producing higher V̇O2peak values due to larger muscle mass as confirmed by DXA results. Significant differences were found in physiological and perceptual responses resultant of modality, pace, and weight status. BLa was seen to differ across exercise conditions due to interaction between modality and pace. From pre to post exercise, both modalities at prescribed pace showed a 37% increase in BLa, while self-selected pace showed a 19% decrease. Elevated BLa accumulation during prescribed pace may be the result of greater muscle activation increasing agonist-antagonist co-contraction frequency. Ali et al. [26] and Goodwin et al. [27, 28] derived similar interpretations with BLa accumulating to a greater extent in individuals exercising at a higher intensity. Dasilva et al. [29] found individuals typically self-select a pace at or near their ventilatory threshold and any pace above this would pose a significant disturbance to homeostasis [29, 30]. This could be interpreted as the self-selected conditions eliciting an intensity below ventilatory threshold, while prescribed pace conditions elicited intensities above ventilatory threshold, leading to increased metabolic demand. Supporting findings have shown overweight participants work at a higher percentage of aerobic capacity when prescribed to a fixed speed as compared to nonoverweight individuals (50–55% vs 35–40%, p < 0.001) [8]. Although further research is needed to explicate this relation, these findings are of great interest when considering the variability of physiological stress placed on the body at different intensities. Elevated BLa accumulation of those exercising at prescribed pace could represent greater physiological stress and a possible mechanism for the greater RPE. Those exercising at self-selected pace were able to maintain sufficient intensity for health benefits while minimizing physiological stress.
Main effect of modality, pace, or weight status on physiological responses
Exercise HR, %HRmax, and %VO2peak were significantly greater for prescribed exercise and also for overweight participants. The significant difference of %HRmax and %VO2peak between paces contrasts with Hall et al. [14] who found no differences between prescribed and self-selected paces. This study indicated prescribed pace consistently induced a higher intensity which could lead to greater cardiovascular demand. Although this higher intensity may potentially translate into greater health benefits, the risk-to-reward ratio is concerning especially in overweight and obese populations as higher intensities create an exhausting and less enjoyable task which jeopardizes walking economy and biomechanical stress [9]. An unfavorable ratio may also increase the risk of adverse events during or immediately after exercise due to an excessive intensity [12, 31].
Relative differences in V̇O2 and EE response to exercise among the overweight and obese populations have received increased attention in the literature in the last decade. In the present study, V̇O2 was significantly higher during prescribed pace compared to self-selected pace, irrespective of modality. These results follow those of Peyrot et al. [9]. In addition, V̇O2 was significantly higher for all conditions in normal weight participants compared to overweight participants, contradicting Browning and Kram [25] who observed V̇O2 to be higher for obese participants. These results may be explained by greater oxygen demand and consumption due to higher intensities and larger lean mass. Existing research denotes EE as an influential factor in healthy weight loss and prevention of weight regain [6, 7, 10, 14]. EE was higher for participants exercising at the prescribed pace compared to self-selected pace. However, total EE did not significantly differ between modalities. This difference in pace is likely not considered great enough to be clinically relevant. Hall et al. [14] observed greater total EE from prescribed pace compared to self-selected pace; however, those results could be due to variability in walking pace as prescribed pace was equivalent to the high end of vigorous intensity range, while self-selected was equivalent to the lower end of moderate intensity. Similar to Browning and Kram [25], differences were seen between normal weight and overweight participants for all exercise conditions when examining total EE. Overweight participants showed a greater total EE while walking as compared to normal weight participants regardless of pace. This may be due to the greater absolute load of body mass carried by overweight participants. In addition, previous researchers have stated individuals with less body fat work more efficiently by utilizing less energy while maintaining the same relative volume due to a greater work-to-EE ratio [9]. For the overweight population, the elevated EE across all conditions is beneficial for individuals striving to lose excess body fat. Likewise, findings from Hall et al. [14] indicate when participants are allowed to self-select exercise intensity, workload would still be sufficient for weight loss and management. In addition to an appropriate and sufficient stimulus, self-selected pace poses less physiological stress. This could play a crucial role in exercise adherence allowing individuals to exercise for longer periods of time optimizing the dose–response relation between PA and health benefits [32].
Main effect of modality, pace, or weight status on perceptual responses
Differing exercise modalities can produce negative perceptions (e.g., overexertion) leading to a significant decline in exercise duration and adherence [15]. Perception of effort and discomfort were significantly higher on the treadmill compared to the track. These results support those of Dasilva et al. [29] who found negative perceptions and less affective responses on the treadmill compared to over ground walking. This provides evidence the treadmill moderates individuals’ RPE higher than the track, although the intensity and distance remains the same. This higher RPE could induce intensity misinterpretation by individuals and previous researchers have found this misinterpretation leads to more strenuous exercise resulting in decreasing intensity, duration, and frequency [14, 33, 34]. These effects are further exacerbated by weight status in overweight and obese populations [7, 8].
Prescribed pace, for both treadmill and track, lead to increased RPE [14] which, in turn, emphasizes the importance of creating an enjoyable activity for exercise program adherence [15]. Although ratings on the CR-10 scale were minimal, any sensation of discomfort during exercise could lead to cessation and return to the program may be significantly affected [2].
Relation between physiological and perceptual response
The secondary aim of this study was to investigate the relation between physiological response (e.g., HR) and perceptual response (e.g., RPE) due to exercise modality, pace, or weight status. An increase in HR should have a corresponding increase in RPE [35]. The present study found the relation between HR and RPE across all conditions was not significantly affected. These results contradict research observing inconsistencies in the HR–RPE relation as intensity increases [35, 36] including between treadmill and field modalities [37]. This contradiction may be due, in part, to previous research induced higher intensities as compared to this investigation.
Although no differences were observed in the relation between HR and RPE from modality, pace, or weight status, variation in responses was significantly different as a result of modality and pace. Variation of RPE scores during prescribed pace was significantly greater than self-selected pace. RPE response variation due to pace is noteworthy because of the potential misinterpretation of intensity as previously mentioned. The high degree of RPE variation from prescribed pace, regardless of modality, could indicate discomfort and negative affective response. This may lead to less pleasurable and enjoyable exercise experiences, negatively affecting one’s exercise habits [14]. Several explanations have been proposed for the mismatch between physiological and perceptual responses. Coutts et al. [23] suggest psychobiological factors such as metabolic acidosis, ventilatory drive, catecholamines, and body temperature are related to RPE. Further research is needed to determine how these factors contribute to the relation between physiological and perceptual response.
Self-determination is believed to be a key component to intrinsic motivation for exercise [15] where one exercises not because it is imposed, but because of internal motives. It is important to identify the aspects of exercise programs and experiences perceived as enjoyable to the participant, so the exercise becomes individualized and concern of program adherence could become minimized. Subjectively adjusting exercise intensity can be seen as a continuous and simultaneous process of monitoring internal and external cues [35, 37]. In overweight and obese populations, emphasis should be placed on reliable and safe guidelines for exercise to promote health benefits and weight loss. These results exemplify self-selected pace functions well in providing a sufficient stimuli for health benefits while maintaining positive affective valence. Twice as many adults adopt a new routine when it is self-selected compared to a prescribed high intensity [3].
Conclusion
Determining an optimal modality and pace, both in physiological and perceptual responses, for overweight individuals is imperative to provide the greatest possible health benefits. The practical applications of the current findings provide encouraging information for addressing exercise adherence, especially in overweight and obese populations. Ceci and Hassmen [37] note that exercising in a free environment such as a track can provide visual, auditory, and thermal feedback which may act as “reducers” of RPE. This study observed negligible differences in total EE between modality and pace, while a higher RPE was seen at a prescribed pace and on the treadmill. These results suggest individuals can foster enjoyable exercise at their self-selected intensity in their preferred environment while gaining similar health benefits as exercise of prescribed intensity, such as the ACSM recommended guidelines. Standard exercise recommendations could result in individuals misinterpreting intensity leading to barriers to initiation and adherence. People may not only be predisposed to select exercise intensities producing positive perceptions and affective responses but also be able to choose an intensity providing physiological stimuli adequate to promote health.
References
Dunn AL, Marcus BH, Kampert JB, Garcia ME, Kohl HW 3rd, Blair SN. Comparison of lifestyle and structured interventions to increase physical activity and cardiorespiratory fitness: a randomized trial. JAMA. 1999;281:327–34.
Greene NP, Lambert BS, Greene ES, Carbuhn AF, Green JS, Crouse SF. Comparative efficacy of water and land treadmill training for overweight or obese adults. Med Sci Sports Exerc. 2009;41:1808–15.
Cox KL, Burke V, Gorely TJ, Beilin LJ, Puddey IB. Controlled comparison of retention and adherence in home- vs center-initiated exercise interventions in women ages 40-65 years: the S.W.E.A.T. Study (Sedentary Women Exercise Adherence Trial). Prev Med. 2003;36:17–29.
Freitas LAG, Ferreira SDS, Freitas RQ, Januario RSB, Alves RC, Silva AC, et al. Effect of self-selected and imposed-intensity walking programs on fat oxidation in obese women. J Exerc Physiol Online. 2015;18:62–70.
Physical Activity Guidelines Advisory Committee. Physical activity guidelines advisory committee report, 2008. Nutr Rev. 2009;67:114–20.
Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39:1423–34.
Browning RC, Baker EA, Herron JA, Kram R. Effects of obesity and sex on the energetic cost and preferred speed of walking. J Appl Physiol. 2006;100:390–8.
Morris C, Garner J, Owens S, Valliant M, Debusk H, Loftin M. A prospective study comparing distance-based vs. time-based exercise prescriptions of walking and running in previously sedentary overweight adults. Int J Exerc Sci. 2017;10:782–97.
Peyrot N, Thivel D, Isacco L, Morin JB, Belli A, Duche P. Why does walking economy improve after weight loss in obese adolescents? Med Sci Sports Exerc. 2012;44:659–65.
Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, Smith BK. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc. 2009;41:459–71.
Loftin M, Waddell DE, Robinson JH, Owens SG. Comparison of energy expenditure to walk or run a mile in adult normal weight and overweight men and women. J Strength Conditioning Res. 2010;24:2794–8.
Manson JE, Greenland P, LaCroix AZ, Stefanick ML, Mouton CP, Oberman A, et al. Walking compared with vigorous exercise for the prevention of cardiovascular events in women. N Engl J Med. 2002;347:716–25.
Antoniewicz F, Brand R. Dropping out or keeping up? Early-dropouts, late-dropouts, and maintainers differ in their automatic evaluations of exercise already before a 14-week exercise course. Front Psychol. 2016;7:838.
Hall CW, Holmstrup ME, Koloseus J, Anderson D, Kanaley JA. Do overweight and obese individuals select a “moderate intensity” workload when asked to do so? J Obes. 2012;2012:919051.
Caserta MS, Gillett PA. Older women’s feelings about exercise and their adherence to an aerobic regimen over time. Gerontologist. 1998;38:602–9.
Baldwin AS, Kangas JL, Denman DC, Smits JA, Yamada T, Otto MW. Cardiorespiratory fitness moderates the effect of an affect-guided physical activity prescription: a pilot randomized controlled trial. Cogn Behav Ther. 2016;45:445–57.
Jung ME, Bourne JE, Little JP. Where does HIT fit? An examination of the affective response to high-intensity intervals in comparison to continuous moderate- and continuous vigorous-intensity exercise in the exercise intensity-affect continuum. PLoS ONE. 2014;9:e114541.
Garber CE, Blissmer B, Deschenes MR, Franklin B, Lamonte MJ, Lee IM, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43:1334–59.
Ekblom O, Ekblom-Bak E, Rosengren A, Hallsten M, Bergstrom G, Borjesson M. Cardiorespiratory fitness, sedentary behaviour and physical activity are independently associated with the metabolic syndrome, results from the SCAPIS Pilot Study. PLoS ONE. 2015;10:e0131586.
American College of Sports Medicine. ACSM’s guidelines for exercise testing and prescription. Philadelphia: Lippincott Williams & Wilkins; 2017.
Abe D, Yoshida T, Ueoka H, Sugiyama K, Fukuoka Y. Relationship between perceived exertion and blood lactate concentrations during incremental running test in young females. BMC Sports Sci Med Rehabil. 2015;7:5.
Buckley JD, Bourdon PC, Woolford SM. Effect of measuring blood lactate concentrations using different automated lactate analysers on blood lactate transition thresholds. J Sci Med Sport. 2003;6:408–21.
Coutts AJ, Rampinini E, Marcora SM, Castagna C, Impellizzeri FM. Heart rate and blood lactate correlates of perceived exertion during small-sided soccer games. J Sci Med Sport. 2009;12:79–84.
Medbo JI, Mamen A, Holt Olsen O, Evertsen F. Examination of four different instruments for measuring blood lactate concentration. Scand J Clin Lab Investig. 2000;60:367–80.
Browning RC, Kram R. Energetic cost and preferred speed of walking in obese vs. normal weight women. Obes Res. 2005;13:891–9.
Ali S, Bhatti A, Khan H, Jan R. Correlation between pre and post exercise blood lactate and pH. Gomal. J Med Sci. 2008;6:1–3.
Goodwin ML, Harris JE, Hernandez A, Gladden LB. Blood lactate measurements and analysis during exercise: a guide for clinicians. J Diabetes Sci Technol. 2007;1:558–69.
Marcora S. Perception of effort during exercise is independent of afferent feedback from skeletal muscles, heart, and lungs. J Appl Physiol. 2009;106:2060–2.
Dasilva SG, Guidetti L, Buzzachera CF, Elsangedy HM, Krinski K, DeCampos W, et al. Psychophysiological responses to self-paced treadmill and overground exercise. Med Sci Sports Exerc. 2011;43:1114–24.
Lind E, Joens-Matre RR, Ekkekakis P. What intensity of physical activity do previously inactivity middle-aged women select? Evidence of a coherent pattern from physiological, perceptual, and affective markers. Prev Med. 2005;40:407–19.
Levinger I, Bronks R, Cody DV, Linton I, Davie A. Perceived exertion as an exercise intensity indicator in chronic heart failure patients on beta-blockers. J Sports Sci Med. 2004;3:23–27.
Perri MG, Anton SD, Durning PE, Ketterson TU, Sydeman SJ, Berlant NE, et al. Adherence to exercise prescriptions: effects of prescribing moderate versus higher levels of intensity and frequency. Health Psychol. 2002;21:452–8.
Ekkekakis P, Lind E. Exercise does not feel the same when you are overweight: the impact of self-selected and imposed intensity on affect and exertion. Int J Obes. 2006;30:652–60.
Garcin M, Mille-Hamard L, Billat V. Influence of aerobic fitness level on measured and estimated perceived exertion during exhausting runs. Int J Sports Med. 2004;25:270–7.
Lewis JE, Nash MS, Hamm LF, Martins SC, Groah SL. The relationship between perceived exertion and physiologic indicators of stress during graded arm exercise in persons with spinal cord injuries. Arch Phys Med Rehabil. 2007;88:1205–11.
Figard-Fabre H, Fabre N, Leonardi A, Schena F. Physiological and perceptual responses to Nordic walking in obese middle-aged women in comparison with the normal walk. Eur J Appl Physiol. 2010;108:1141–51.
Ceci R, Hassmen P. Self-monitored exercise at three different RPE intensities in treadmill vs field running. Med Sci Sports Exerc. 1991;23:732–8.
Author information
Authors and Affiliations
Contributions
All authors have made significant contributions to research design, data collection and analysis, and development of the manuscript. RG: developed study design, conducted all data collection, and made significant contribution to manuscript development and revision. RB: made significant contribution to manuscript development and revision in all sections. ML: assisted in study design and data collection along with development of the “Methods” section of the manuscript. MEH: assisted in development of all sections and reviewing of manuscript. JG: conducted data filtering and statistical analysis and also contributed significantly to manuscript review and revisions.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Galloway, R., Booker, R., Loftin, M. et al. Physiological and perceptual responses during walking at set and preferred pace in normal and overweight adults. Int J Obes 46, 100–106 (2022). https://doi.org/10.1038/s41366-021-00963-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-021-00963-7
- Springer Nature Limited