
Abstract
Intratumoral heterogeneous MYCN amplification (hetMNA) is an unusual event in neuroblastoma with unascertained biological and clinical implications. Diagnosis is based on the detection of MYCN amplification surrounded by non-amplified tumor cells by fluorescence in situ hybridization (FISH). To better define the genetic features of hetMNA tumors, we studied the Spanish cohort of neuroblastic tumors by FISH and single nucleotide polymorphism arrays. We compared hetMNA tumors with homogeneous MNA (homMNA) and nonMNA tumors with 11q deletion (nonMNA w11q-). Of 1091 primary tumors, 28 were hetMNA by FISH. Intratumoral heterogeneity of 1p, 2p, 11q and 17q was closely associated with hetMNA tumors when analyzing different pieces for each case. For chromosome 2, 16 cases showed 2p intact, 4 focal gain at 2p24.3 and 8 MNA. The lengths of the smallest regions of overlap (SROs) for 2p gains and 1p deletions were between the SRO lengths observed in homMNA and nonMNA w11q- tumors. Co-occurrence of 11q- and +17q was frequently found with the largest SROs for both aberrations. The evidence for and frequency of different genetic subpopulations representing a hallmark of the hetMNA subgroup of NB indicates, on one hand, the presence of a considerable genetic instability with different SRO of either gains and losses compared with those of the other NB groups and highlights and, on the other hand, the need for multiple sampling from distant and macroscopically and microscopically distinct tumor areas. Narrowing down the different SRO for both deletions and gains in NB groups would be crucial to pinpointing the candidate gene(s) and the critical gene dosage with prognostic and therapeutic significance. This complexity of segmental chromosomal aberration patterns reinforces the necessity for a larger cohort study using FISH and pangenomic techniques to develop a suitable therapeutic strategy for these patients.
Similar content being viewed by others


Introduction
The MYCN proto-oncogene, on chromosome 2p24, is found to be amplified in different human malignancies.1 MYCN amplification (MNA) is par excellence a marker of poor outcome, having clinical and treatment implications in neuroblastoma (NB).2, 3 In addition, defining new therapeutic strategies in NB targeting MYCN is a demanding task.4, 5 Fluorescence in situ hybridization (FISH) for MYCN gene analysis is critical when describing the MYCN status because of its high sensitivity and rapid morphological correlation.6, 7 Homogeneous MNA (homMNA) is defined by the International NB Risk Group (INRG) Biology committee as the presence of a more than fourfold increase in the MYCN signal number compared with the reference probe located on chromosome 2 in all tumor cells. Although rare, a proportion of tumor cells may also show MYCN gain (MNG).
Intratumoral heterogeneity for MNA (hetMNA) refers to the coexistence of amplified (frequently including tumor cells with MNG) as well as non-amplified tumor cells in the tumor as cluster (focal) or as single (scattered) cells.8 In addition, temporospatial differences in MNA leading to a hetMNA status have also been described, as well as marked variations in the relation of MYCN amplified versus non-amplified tumor cells.9, 10 As the MNA clones in hetMNA tumors are frequently small, their diagnosis requires a thorough examination and confirmation, and is therefore difficult or impossible in small or inadequate biopsies. In addition, validation of hetMNA, ideally in paraffin sections by FISH, can be crucial to exclude false-positive results by ‘contamination’ of MNA cells from another tumor.11 If these points are not considered, then hetMNA cases can be either missed entirely or included in studies as non-amplified MYCN (nonMNA) or as MNA tumors.6, 12, 13 The few studies of hetMNA existing in the literature revealed that only 1–2% of all NB are hetMNA tumors, while MNA is detected in 20–25%, especially in stage 4 patients (~40%).3, 7, 9, 10, 13, 14, 15, 16, 17 HetMNA is more frequently described in advanced stages 3, 4 and in stage 4S than in localized tumors (discussed in Bishop et al.18). Theissen et al.9, in a review of German cooperative trials, concluded that a small amount of MNA cells is not correlated with adverse outcome. However, owing to the limited clinical information on the hetMNA phenomenon, clinicians are faced with a significant dilemma when deciding on treatment strategy.12, 18
Pangenomic analyses are essential in current diagnosis and treatment allocation for NB patients because, in addition to the MYCN status, the overall genetic profile is essential for outcome prediction.7, 19, 20 Seven recurrent segmental chromosome aberrations (SCA, that is, losses at 1p, 3p, 4p, 11q and gains at 1q, 2p and 17q), which can also show intratumoral heterogeneity, were recently used for therapy stratification in a European SIOPEN study (LINES, Low and Intermediate Neuroblastoma European Study).21 As MNA tumors display an SCA pattern distinct from those of nonMNA tumors, it might be useful to further investigate SCAs and possible intratumoral heterogeneities of hetMNA tumors to ascertain their pattern and to detect indications of intratumoral genetic instability which could influence outcome.22, 23 Furthermore, as genetic characterization by means of single nucleotide polymorphisms array (SNPa) is able to reveal gains and losses of chromosomal fragments of any size and subpopulations, we decided to study the hetMNA cases using this high-throughput technique in several pieces of the same tumor to improve the identification of a heterogeneous SCA (hetSCA) status.7, 20, 24, 25, 26 To better demarcate the genetic characteristics of hetMNA tumors, we also studied the following aggressive genetic subgroups of NB: homMNA tumors with and without deletion of 11q (w11q- and w/o11q-, respectively) and nonMNA tumors with and without these specific aberrations.26 Because many SCA in NB are large and encompass numerous genes, narrowing down the different SRO for both deletions and gains in NB groups would be crucial to pinpointing the candidate gene(s) and the critical gene dosage with prognostic and therapeutic significance. We also discuss the biological and prognostic implications in the cohort of NBs with a heterogeneous MYCN status.
Results
Overview of clinical features
The main clinical features of the 28 patients with hetMNA are provided in Table 1. For patients with hetMNA tumors, age at diagnosis ranged from 5 to 86 months (mean 24.5, median 22). Advanced disease stages 3 and 4 were the most prevalent (70.3%). The mean overall survival for the hetMNA cohort was 92 months (confidence interval, 67–116) with an estimated 5-year overall survival and event-free survival rate of 51% (s.e. 0.13) and 58% (s.e. 0.11), respectively. For the homMNA cohort, the 5-year overall survival and event-free survival were 35% (s.e. 0.09) and 30% (s.e. 0.10), respectively; and for the nonMNA w11q- cohort, 30% (s.e. 0.08) and 39% (s.e. 0.09), respectively. Eight patients (30.7%) experienced relapse (mean 24.5 months). To date, eight (30.7%) patients have died of disease after a mean of 26.6 months (median 32) within the hetMNA cohort.
Overview of the genetic profiles of the entire cohort
The final diagnosis of MYCN status of the 1091 tumors studied by FISH revealed that 28 cases presented hetMNA (2.5%), 197 homMNA (18.1%) and 866 nonMNA (79.4%). Of the 273 tumors analyzed by SNPa, 28 showed hetMNA (10.3%) while of the remainder, 37 were homMNA (13.5%) and 208 nonMNA cases (76.1%). Different genetic profiles were revealed by SNPa analyses in each MYCN status subgroup. In hetMNA tumors, 26 cases had an SCA profile (92.9%), 4 of which had only one SCA, and 2 cases had a numeric chromosome aberrations (NCA) profile (7.1%). All homMNA tumors had an SCA profile. Of the nonMNA tumors, 117 cases had an SCA profile (56.3%), 55 cases w11q- (47%) and 62 cases w/o11q- (53%), 87 cases had an NCA profile (41.8%) and 4 a flat genetic profile (neither SCA nor NCA, 1.9%).
Out of 180 cases with an SCA profile, the highly recurrent SCA, including hetSCA, affected: 1p-, +1q, +2p, -3p, 11q- and +17q. Co-occurrence of 1p- plus +17q (15 cases, 53.5%), 11q- plus +17q (12 cases, 42.8%) or +2p plus +17q (10 cases, 35.7%) were frequently found in hetMNA tumors; whereas in homMNA tumors, co-occurrence of 1p-, +2p and +17q occurred in 43%. For the remaining cases (nonMNA w11q- and w/o11q-), the highly recurrent typical SCA was +17q (90.9% and 54.8%, respectively). In the hetMNA cohort, uniparental isodisomies (UPDs) were found in 39.3%, UPDs for chromosome 11 were more frequent in older than in younger patients (12 versus 9%), and 11q- with large terminal SRO was observed in 42.8% by SNPa. In homMNA, UPDs at chromosome 11, and 11q aberrations, were rare, and present in 0% and 24.3% of the cases, respectively, despite the bias introduced by the inclusion of our previously published unusual homMNA plus 11q cohort.19 No association patterns for the remaining typical and atypical SCA or NCA were found for hetMNA, homMNA or nonMNA cases. Regarding the number of chromosomal breakpoints for each subgroup, hetMNA cases had an intermediate number of breakpoints, 7.3 (median 7), while homMNA and nonMNA w and w/o11q- had an average of 6.7 (median 6), 10 (median 10) and 3.96 (median 3) breakpoints, respectively (P=0.04 for hetMNA and nonMNA w11q-; and P=0.000 for hetMNA and nonMNA w/o11q- groups). Considering homMNA w11q- tumors, the average number of breakpoints was 10.5 (median 7), versus 5.2 (median 5) for homMNA w/o11q-. Interestingly, this tendency for a higher number of breakpoints for 11q- tumors was also seen within hetMNA cases, with 8.9 breakpoints for the 11q- tumors and 5.2 for those w/o11q- (median 7.5 and 6.5, respectively). When grouping the patients above and below 18 months of age, little difference in the number of SCA was found (6.6 versus 7.8), although most of the hetMNA w11q- tumors belonged to patients older than 18 months (8 out of 12 cases).
Intratumoral heterogeneity for hetMNA
The genomic findings for hetMNA tumors are detailed in Table 2. Alterations of the 1p, 2p, 11q and 17q chromosome regions are represented in Figures 1 and 3. HetMNA occurred either as small foci with 5–10 cells (n=11), large foci with 50–55 cells (n=2) or scattered cells (n=15). Intratumoral hetSCA, occurred more often within hetMNA tumors (50%, 14 cases) than within homMNA (18.9%, 7 cases) or nonMNA tumors (20.9%, 13 cases). A diversity in the MYCN status was found when analyzing more than one piece by FISH (four cases) or by SNPa (six cases) and/or by divergent results obtained by the two techniques (Table 2, Figures 1 and 2). For cases with different MYCN status analyzed by FISH, hetMNA and nonMNA were detected in three tumors (cases 10, 11 and 20) and hetMNA and homMNA in one tumor (case 17). In case 11 hetMNA, MNG and nonMNA were found. In two other tumors (cases 18 and 19), the hetMNA findings were unequal, showing an evident disparity in the number of amplified cells (10–50%) and variation in the number of double minutes (from 15 to 100) between the two tumor pieces in each case. In these six cases, complex MYCN heterogeneity was present, because different results were also found by SNPa. HetMNA was confirmed in paraffin-embedded whole tissue sections from all cases by FISH. Regarding the SNPa results (4 cases), MNG (found as micro gain on 2p24.3) was detected in three cases, and in the fourth case, MNA was detected only in one of the pieces analyzed, whereas the second piece showed no trace of MNA cells (cases 9, 19, 27 and 20, respectively). Furthermore, in two more cases, MNG was detected in the first piece and MNA in the second piece (cases 17 and 28). There was also a clear difference in the level of amplification between the two pieces of case 22. Among all the hetMNA cases, SNPa showed nonMNA in 16 cases, MNA in 8 and MNG in 4 cases. Presence of hetMNA plus MNG was found in 12 cases by FISH, which resulted as MNA or MNG in 6 cases, and nonMNA in the remainder, by SNPa. Specifically, MNA plus gain at 2p was found in cases 12 and 20 by SNPa, while in case 22 only MNA was found. In cases 24 and 28, MNG plus gain at chromosome arm 2p was found, while in case 19 only MNG was detected by SNPa (Figure 1). Six out of eight cases that showed MNA and three out of four cases that showed MNG by SNPa had ⩽10 MNA cells per slide by FISH. The cases with 35–90 MNA cells per slide (n=5) presented nonMNA status by SNPa. The amplicon or the gained region extended from 15.2 to 18.7 Mb, depending on the sample; the smaller region ranged from 15.8 to 16.2, affecting only the MYCN gene (case 12). The NBAS gene was excluded in two cases, while the DXX1 and MYCN genes were usually involved. One or two extra amplifications distal to MYCN amplicon were observed in two hetMNA and nine homMNA cases and in one nonMNA tumor (Figure 3b).

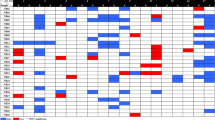
Correlation between FISH (touch imprints) and SNPa results in hetMNA tumors. HetMNA status, ranging from a low to high number of amplified cells, was confirmed by FISH in paraffin-embedded tissue sections in all cases. For MYCN gene results, the correlation between techniques was independent of the number of MNA and/or the percentage of MNG cells. In some cases where 1p deletion was missed by SNPa, non-deleted tumor cells in conjunction with 1p imbalance and deleted cells were observed by FISH. Intratumoral homogeneity and heterogeneity was found for 11q and 17q chromosome regions, respectively. a/b, indicates equal results between fragments (when different results both results are indicated); MNA, MYCN amplification; f, focal (1–2 MNA foci); s, scattered MNA cells; nonMNA, no MYCN amplification; homMNA, homogeneous MYCN amplification; MNG, MYCN gain; G, Gain; het, intratumoral heterogeneity of MYCN /chromosome aberration; D, deleted; ND, Non-deleted; Im, 1p imbalance; *, >50% difference in copy number from cell to cell of double minutes and different percentages of 1p-, 11q- or +17q cells; ↑or ↓, higher or lower level MYCN amplification. FISH color box definition: no color, intratumoral heterogeneity of MYCN status/chromosome aberration; purple, no SCA detected; red, SCA only detected for one fragment; blue, SCA detected. SNPa color box definition: no color, concordant MYCN gene status with FISH results orange, discordant with FISH results (described when nonMNA or SCA); green, concordant with FISH results. Case 11c, additional piece analyzed with different results.

Schemas presenting the various possible spatial distributions of tumor cells, chromosome 2p SNPa profiles and FISH images of nonMNA, homMNA and hetMNA cases to illustrate the effects of MNA DNA dilution within DNA of nonMNA. Schemas showing nonMNA neuroblasts (green circles), MNA cells (red circles) and stromal cells (blue ovals) in a whole tumor (large cylinder) and pieces of the tumor (small cylinders demarcated by dashed lines). Tumor touch imprints of the surface of each fragment were used for FISH and the whole fragment for SNPa analyses. FISH images show MYCN gene in red, LAF region in green and DAPI nuclear counterstaining in blue. (a) In nonMNA tumors, the two techniques detect only nonMNA cells. (b) In homMNA tumors, homogeneous distribution and large amount of MNA cells without nonMNA neuroblasts facilitates the detection of the MNA by either SNPa or FISH. (c) In hetMNA tumors, the heterogeneous distribution and differing amount of MNA cells, nonMNA neuroblasts and stromal cells generate discrepant FISH and SNPa results. MNA and tumor nonMNA cells are detected in all FISH touch preparations. (d) The low ratio between MNA and nonMNA cells does not allow the detection of 2p24.3 alteration by SNPa. (e) The higher presence of MNA cells enables their detection as a 2p24.3 high peak by SNPa. (f) The amount of intermingled MNA cells is reflected as MYCN gain by SNPa owing to the dilution of the MNA DNA content. nonMNA, no MYCN amplification; homMNA, homogeneous MYCN amplification; MNG, MYCN gain; hetMNA, heterogeneous MYCN amplification; f, focus of MNA cells; s, scattered MNA cells.
Intratumoral hetSCA was found when analyzing several pieces with SNPa and when comparing FISH and SNPa results. With regard to the discrepant results in the detection of 1p deletion by FISH and SNPa, we hypothesize that 1p deletion in hetMNA tumors occurred in a similar manner to that of MNA (Figure 2). Clones with 1p deletion are admixed with clones without aberration at 1p in a heterogeneous manner, and thus the aberration may remain hidden. In view of the discrepant results in the detection of 1p deletion by SNPa, we hypothesize that 1p deletion in hetMNA tumors occurs similar to the detection of hetMNA by FISH (Figure 2). Heterogeneity for large segmental UPDs (11p, 12q, 14q, 17q, 18p and 22q) was found in four cases, in half of these, loss of the same chromosome regions was seen instead of the UPD in the second piece; interestingly, for the case with 17q UPD, a gain of 17q was seen by FISH. The case with the highest number of SCA, in addition to hetUPD (14q and 22q), also presented heterogeneity for up to three SCA, and for one micro SCA (+5p) and different MYCN status (MNA/MNG), indicating a high intratumoral genetic instability. In two cases, heterogeneity in the SNPa was present in relation to 2p alterations other than MYCN: with and without amplification at 2p.25.1 and with and without gain in 2p24.1. Altogether, the average number of chromosomal breakpoints was 7.3 (median 7). The most frequent NCA in hetMNA tumors were +7 and +17, alone or together with other NCAs (13 cases, 47%). Micro SCAs were present and randomly distributed along the genome in nine cases (32.1%), two of which were heterogenous cases, except for the MYCN gain region. Large UPD events (11 cases, 39.3%) were randomly distributed along the genome and more frequent for the cases with an increased number of breakpoints (72.7%, 8/11 cases). UPD and micro SCA were also present in NCA cases. Chromothripsis-like pattern was present in four chromosomes (5, 6 and 11) of three cases, all with ⩾7 breakpoints.
Patterns of 1p-, +2p, 11q- and +17q in all subgroups analyzed
We focused on frequency (FISH and SNPa data), length and type (intrachromosomal, terminal, micro SCA and SROs) of the typical SCAs 1p-, +2p, 11q- and +17q. A representation of SNPa results for each region of the aggressive subgroups is shown in Figure 3. The differential distribution of other typical and atypical SCAs is shown in Table 3.

Representation of chromosome aberrations detected by SNPa for hetMNA (the reference number for each patient is indicated at the top of each bar), homMNA and nonMNA w11q- subgroups of tumors. Length of small regions of overlap (SROs) of each aberration is indicated below the tittle of each subgroup, SROs are indicated by dashed horizontal lines. Ideograms on the left of (a–d) represent 1p, 2p, 11q and 17q chromosome arms, respectively. Vertical bars represent the length of 1p and 11q deletions in a and c, and the length of 2p and 17q gains in b and d. Horizontal bars represent amplifications, micro SCA are marked by §, and UPDs by a grey bar. Two oblique lines at the end of the vertical bars indicate where the alteration extends to the other chromosome arm. When other breakpoints are present in the altered regions, the bars are out of alignment.
1p deletion: of the total of 180 SCA tumors, this deletion was present in 44.4% (80 cases). HetMNA tumors showed less 1p deletions than homMNA (67.8 versus 86.4%). For nonMNA w11q- and w/o11q-, the difference was less marked (23.6 versus 25.8%). The SRO extended from pter in all cases (except for one homMNA tumor), to p36.21 for the hetMNA tumors (13.8 Mb), to p36.12 for homMNA (27.3 Mb) and to p36.22 for nonMNA w11q- cases (9.5 Mb) (Figure 3a). The differences between groups in the size of the 1p- region were statistically significant (P=0.007). An interstitial deletion, from p36.32 to p36.23 (3.5–8.6 Mb), was detected in one homMNA case, creating an interstitial SRO. The median length in the hetMNA cases was 66 Mb, 53.3 Mb for the homMNA and 28 Mb for the nonMNA w11q-.
2p gain: +2p (62 cases) accounted for 34.4% of all the SCA cases. For the hetMNA tumors, +2p was less common than for homMNA and nonMNA w11q- tumors (35.7%, 43.2% and 45.4%, respectively). However, in SCA tumors within the subgroup of nonMNA w/o11q-, proximal +2p accounted for 19.3%. In the strictest sense, the +2p SRO for the homMNA cases was from p24.3 to p24.1 (3.3 Mb) owing to loss of genetic material between the two amplified regions observed in one case. This fact was considered as a false effect of the amplification peaks, and when discounted, the SRO ranged from p25.1 to p24.1 (9.6 Mb). The hetMNA cases had an intermediate SRO, from p25.3 to p24.3 (14.3 Mb), and the nonMNA with 11q deletion had a shorter SRO, involving only the p24.3 region (0.7 Mb) (Figure 3b). The large 2p gain in hetMNA tumors was associated with 11q- in 41.6%, in contrast to 33% in homMNA tumors.
11q deletion: out of all SCA tumors, 11q- was present in 76 cases (42.2%); 55 were nonMNA (72.4%) and 21 het or homMNA (27.6%), being more frequent in hetMNA than in homMNA cases (42.8 versus 24.3%). Furthermore, hetMNA tumors had larger deletions than the homMNA and nonMNA subgroup of tumors (median 62 Mb, 44 Mb and 59 Mb, respectively) (P=0.038) (Figure 3c). When considering only the SRO, the differences between the deleted regions became more apparent, with a large terminal SRO for the hetMNA, from 11q14.1 (84.7 Mb) to qter, a short terminal SRO for the homMNA cases, from 11q23.1 (111 Mb) to qter, and an interstitial SRO for nonMNA cases, from 11q21 to 11q23.3 (96.8–118 Mb). In the latter subgroup, only 1 tumor out of 55 showed no terminal deletion; this meant that the most common 11q- type for nonMNA was also a terminal deletion with an SRO of a size between that from hetMNA and homMNA. One homMNA case showed two additional breakpoints located at 94.1–99.8 Mb. None of the hetMNA tumors presented a breakpoint between 112 and 117 Mb, where the FRAC11B and FRAC11G fragile sites are located, contrary to some of the homMNA and nonMNA tumors.
17q gain: as expected, +17q was the most frequent SCA, present in 134 cases (75.7%). The occurrence of +17q was evenly spread across the three genetic subgroups, although more frequent in nonMNA w11q- tumors (90.9%) (Figure 3d). The gain always included the telomeric region; having more than one breakpoint in 14 cases (14.5%) and interrupted by a UPD in one case. Although the average size of the 17q gain was similar in all the subgroups (45 Mb), the SRO was larger for the hetMNA (breakpoint at 45.3 Mb, q21.31-qter), intermediate for the nonMNA (breakpoint at 52.7 Mb, q23.2-qter) and smaller for the homMNA tumors (60.9 Mb, q23.3-qter). Grouping all the cases according to the 17q gain breakpoint positions and associating with better survival, as described by Theissen et al.,27 the frequencies were almost identical to those described: 11.5%, 77% and 11.5% for <26.6 Mb, 26.6–42.5 Mb and ⩾42.5 Mb breakpoint positions, respectively. The majority of nonMNA11q- cases mapped within the range 26.6–42.5 Mb, being more dispersed in both hetMNA and homMNA tumors.
Discussion
To date, hetMNA studies in NB have comprised small cohorts providing limited genetic data, there have been no pangenomic studies, and the related clinical features remain unclear (reviewed in Bishop et al.18). We present a large cohort of hetMNA NBs studied using a pangenomic approach intending to identify the genetic profile, distinguish the underlying genetic pattern of intratumoral hetMNA, describe the presence of intratumoral heterogeneity of SCA and compare the SRO for both deletions and gains. The incidence of hetMNA in primary tumors in the largest cohort reported so far is 1.1% (15 out of 1341), with similar small frequencies reported by others, and similar to the results of the present study.7, 9, 15, 16 The low frequency of hetMNA described might be explained by the complex and not always feasible work-up required for its diagnosis, and also by the presence of focal genetic alterations, methodologically difficult to identify, which lead to an underestimation of the frequency. In hetMNA tumors, either focal or scattered MNA neuroblasts are admixed with non-MNA neuroblasts, producing a speckled or mottled appearance. HetMNA should therefore be considered as a single mass sprinkled with diverse tumor cell clones, including MNA cells, tumor nonMNA cells and stromal cells. Whereas a hetMNA tumor evaluated by FISH shows a combination of MNA cells (usually in low percentages and with less MYCN copies per cell than in homMNA), with nonMNA and occasionally MNG neuroblastic cells, SNPa results do not always show conspicuities in the MYCN region. HetMNA cases, ideally when more than one tumor piece is analyzed, can show a more than fourfold peak (as compared with the chromosome 2 baseline) at 2p24.3 (usually at lower levels as compared with homMNA tumors), or a gain (up to fourfold) restricted to the MYCN gene locus (MNG, equal to a micro 2p24.3 gain, DDX1 and NAG genes can be included), not found in either MNA (only in case of low tumor cell contents) or in nonMNA tumors. However, hetMNA may also be present without any visible alteration in the MYCN gene region by SNPa, even when several fragments are studied. Our results support those previously reported by others which use methods that rely on pooled DNA samples in hetMNA NB, and reflect the admixture with tumor DNA not showing MNA or normal cell DNA that can hinder the detection of the genetic alteration.10 Such findings strengthen the use of FISH for MYCN status diagnosis, with an internal control of somy of chromosome 2, in conjunction with pangenomic techniques. The International Society of Pediatric Oncology, Europe Neuroblastoma Group (SIOPEN) is involved in the assembly of clinical and FISH data of hetMNA tumors from eight participating countries (Ambros IM and Noguera R, manuscript in preparation).
Apart from the intertumoral genetic heterogeneity characteristic of NB, intratumoral diversity, although not very frequently reported, is also known to be present in primary NB.28 Our group and others have previously described intratumoral hetSCA, of 1p and 17q by FISH and genome-wide techniques without ascertaining biological and clinical significance.7, 19, 29, 30, 31 HetMNA presented genetic profiles ranging from pure NCA to SCA with multiple rearrangements. The data on hetMNA tumors reveal a spectrum of genetic heterogeneity, here referred to as intratumoral hetSCA, for typical SCA, but which also appeared in non-typical SCA. This heterogeneity among hetMNA NB was higher compared with homMNA and nonMNA w11q- tumors. A close association between homMNA and 1p deletion is well-known; a similar close coexistence of hetMNA and het1p deletion was revealed. Therefore, analyzing several pieces of hetMNA tumors would not only help in clarifying MYCN status, but also in obtaining an accurate and complete genetic profile of each tumor. This is especially important in treatment approaches for low-risk patients, that is, localized stages in children aged ⩽18, and Ms stage.32 In the present cohort, four patients presented with localized disease and two with Ms stage. Whether this intratumoral heterogeneity might be a result of a clonal evolution process and would lead to clinical progression and resistance to chemotherapy is difficult to assess. It could be reasoned that in NBs with NCAs, the presence of hetMNA (and hetSCA) represents an earlier stage in NB evolution on its way to reaching the threshold of malignant transformation.23, 33 Unfortunately, no differences in age could be seen in patients between any of the genetic subtypes studied.
Remarkably, the predominance of SCA tumors was noticeable, with large regions of 17q gain, with large regions of 11q loss, or intermediate regions of 2p gain. 17q gain is almost ubiquitous in SCA profiles of NBs, assuming an oncogenic gene dosage effect for this aberration.8, 34, 35 Recently, a better prognosis has been ascertained for patients with a more distal 17q gain breakpoint (26.6 Mb).9 However, the more proximal breakpoint identified herein was not associated with poorer survival for most of the hetMNA patients. In addition to +2p and +17q, 1p- is also known to be strongly correlated with homMNA tumors. Interestingly, several tumor suppressor genes located in this region have been explored.36, 37 Nevertheless, our results and those of previous studies did not detect a strong correlation between hetMNA tumors and 1p deletion. Half of the hetMNA tumors show mainly het1p-, denoting that the overall proportion of deleted cells is low.7, 9 Compared with 1p-, 11q- was more frequently represented in hetMNA, than in homMNA tumors, especially in older patients with advanced stage tumors and was associated with a higher number of SCA.26, 38, 39 As 11q- rarely co-occurs in homMNA tumors, it is recognized as an alternative mechanism by which full oncogenic potential is attained through haploinsufficiency of the genes mapping to the deleted region.19, 26, 40, 41 11q- tumors are distinguishable also at the mRNA and miRNA level, but the genetic factors that mediate the poorer outcome on 11q- tumors are not clear.42, 43 HomMNA is known to occur at an earlier stage than 11q deletion and with less associated SCA. On the other hand, unfavorable nonMNA w11q- tumors have a later onset and frequently an increased number of associated SCA, suggesting that nonMNA w11q- tumors achieve their strong oncogenic potential by acquisition of genetic instability. Interestingly, hetMNA tumors seem to have a very 'unstable' genetic profile, different to homMNA tumors, and frequently with 11q- associated. Identification of hetSCA and genomic amplification other than MYCN, if present, can help in narrowing the region to search for target genes with impact on outcome, even genes implicated in the MYCN pathway.44, 45 In this regard, 2p25, 1p31 and 1p34.2, among other amplifications, have been detected in homMNA and are associated with a tendency towards poorer prognosis than homMNA only.46, 47 We found these amplifications in two low SCA tumors (stage 1 and 3) both in patients aged >18 months. The implications of other chromosomal alterations, such as 1p imbalance have been discussed in a short report, questioning whether nonfavorable neuroblastic clones are indeed evolving from favorable clones, and could be investigated in hetMNA tumors.48 The high presence of chromosome 11 UPDs associated with younger age, localized disease stage and aneuploidy founded in the Austrian cohort (data not shown) will be discussed elsewhere (Ambros IM, manuscript in preparation). In addition, epidemiologic differences may also be involved in this issue. Defining the SROs of both gains and deletions in each NB group will certainly aid in identifying the distinct gene dosages responsible for tumor progression. The finding that the SCA profile of hetMNA differed from that of the homMNA and nonMNA tumors has importance for identifying whether a distinct gene dosage or different tumor suppressor gene effects are related to the presence of multiple tumor cell subpopulations and their relationship with the microenvironment.
In conclusion, hetMNA tumors harbor an ‘unstable’ genetic profile, with genetically diverse subpopulations of tumor cells that diminish the utility of defining the cutoff for the number of MNA cells by FISH, and demands, when possible, performing multiple sampling from macroscopically and microscopically distinct tumor fragments. Further efforts using FISH together with pangenomic techniques are essential to developing a targeted therapeutic strategy for this subgroup of patients with hetMNA tumors, especially for those with NCA or low SCA profile.
Materials and methods
Clinical data and tumor material
Between January 1997 and January 2014, 1091 tumor samples were referred to the Department of Pathology (Medical School of Valencia) at the time of diagnosis. Clinical data are available in the Spanish NB database. In summary, all patients were studied and staged according to the INSS and from those diagnosed after 2009 according to the INRG. Except for one patient with a nodular ganglioneuroblastoma, all hetMNA cases were histopathologically classified as poorly differentiated NB, according to the International NB Pathology Classification (INPC).49 Informed consent from parents or guardians was obtained for all patients. Histologic and genetic studies were approved by Spanish Society of Pediatric Hematology and Oncology (file number: 59C18ABR2002) and as well as by the Ethical Committee of the University of Valencia and University Clinic Hospital of Valencia.
Fluorescence in situ hybridization (FISH)
Tumor touch imprints and paraffin sections were hybridized for FISH analyses in two to four fragments of each tumor, using commercial cocktail probes: 1p36(D1Z2)/centromere chromosome 1 (Qbiogene, Amsterdam, The Netherlands), MYCN(2p24)/LAF(2q11), MLL(11q23)/SE11 and MPO(17q22) ISO17q/p53(17p53) (Kreatech Biotechnology, Amsterdam, The Netherlands). Assessment and interpretation of FISH results were performed in accordance with previously published procedures and all hetMNA cases were centrally reviewed by the International Society of Pediatric Oncology Europe Neuroblastoma Biology Group.50 In this manuscript, the term intratumoral hetMNA has only been used as defined by the INRG Biology Committee, a definition also used by Theissen et al.8, 9 For the final diagnosis of the MYCN gene status, a FISH diagnosis of hetMNA prevailed of a normal MYCN status found by SNPa.
Genetic study by SNPa
DNA was extracted from fresh (n=237) and formalin-fixed paraffin-embedded tissue (n=36) as previously reported.19 All samples had tumor cell content >50%, except for five samples with only 50% of tumor cell content (cases 10,15,17,18 and 24). Two SNPa platforms were used: Genechip Human Mapping Nsp Array (262 256 markers) in 90 tumors and HumanCytoSNP-12 DNA Analysis BeadChip (299 140 markers) in 183 tumors from Affymetrix (Affymetrix, Inc., Santa Clara, CA, USA) and Illumina (Illumina Inc., San Diego, CA, USA), respectively. Previously described experimental procedures were used for all array platforms.19, 26 The complex genetic intratumoral composition demanded the analysis, when possible, of different pieces of the same tumor to achieve a precise and comprehensive diagnosis (at least two fragments in 14 cases, with a third fragment in cases 11, 21 and 22). The most aggressive genetic profile was taken as final diagnosis of MYCN gene status by SNPa (that is, MNA prevails over MNG or nonMNA status, and MNG prevails over nonMNA status). For each hetMNA tumor, we determined: (i) NCAs, (ii) hetSCA (which would lead to different diagnoses for SCA status in distinct tumor fragments within the same tumor), (iii) amplifications, (iv) focal or micro SCA, smaller than 2 Mb and excluding copy number variations, and (v) copy neutral loss of heterozygosity considered as UPD. MNA and MNG were detected by SNPa using AsCNAR (allele-specific copy-number analysis) and cnvPartition functions from CNAG and KaryoStudio software, respectively. MNA regions are tracked in dark red, and MNG regions in pale red for Affymetrix arrays. For Ilumina arrays, a value of 4 was assigned to the MNA region, and a value of 3 to the MNG region. In addition, MNA and MNG status was confirmed by visual inspection of the difference between the increased signals in the copy number plot. Micro SCAs were not taken into account when counting the number of SCA breakpoints, and hetSCAs by FISH were considered as a single event. For final diagnosis of SCA in cases with hetSCA, the most aggressive profile (that is, the highest number of SCA) was used. SCAs in hetMNA cases were classified as: NCA/low SCA (0–1), intermediate (3–7) and high SCA (>7) profiles. Comparison of SRO size and number of breakpoints between groups (hetMNA, homMNA and nonMNA) were carried out using Mann–Whitney U test (two groups) and Kruskal–Wallis (three groups), all P-values were two-sided. Some data for hetMNA w11q- cases (n=7), homMNA w11q- cases (n=11) and nonMNA w11q- cases (n=53) have already been published19 (Javanmardi and Berbegall et al. 2015, manuscript in preparation).
References
Beroukhim R, Mermel CH, Porter D, Wei G, Raychaudhuri S, Donovan J et al. The landscape of somatic copy-number alteration across human cancers. Nature 2010; 463: 899–905.
Maris JM . Recent advances in neuroblastoma. N Engl J Med 2010; 362: 2202–2211.
Brodeur GM, Seeger RC, Schwab M, Varmus HE, Bishop JM . Amplification of N-myc in untreated human neuroblastomas correlates with advanced disease stage. Science 1984; 224: 1121–1124.
Barone G, Anderson J, Pearson AD, Petrie K, Chesler L . New strategies in neuroblastoma: Therapeutic targeting of MYCN and ALK. Clin Cancer Res 2013; 19: 5814–5821.
Westermark UK, Wilhelm M, Frenzel A, Henriksson MA . The MYCN oncogene and differentiation in neuroblastoma. Semin Cancer Biol 2011; 21: 256–266.
Squire JA, Thorner P, Marrano P, Parkinson D, Ng YK, Gerrie B et al. Identification of MYCN Copy Number Heterogeneity by Direct FISH Analysis of Neuroblastoma Preparations. Mol Diagn 1996; 1: 281–289.
Ambros PF, Ambros IM, Kerbl R, Luegmayr A, Rumpler S, Ladenstein R et al. Intratumoural heterogeneity of 1p deletions and MYCN amplification in neuroblastomas. Med Pediatr Oncol 2001; 36: 1–4.
Ambros PF, Ambros IM, Brodeur GM, Haber M, Khan J, Nakagawara A et al. International consensus for neuroblastoma molecular diagnostics: report from the International Neuroblastoma Risk Group (INRG) Biology Committee. Br J Cancer 2009; 100: 1471–1482.
Theissen J, Boensch M, Spitz R, Betts D, Stegmaier S, Christiansen H et al. Heterogeneity of the MYCN oncogene in neuroblastoma. Clin Cancer Res 2009; 15: 2085–2090.
Thorner PS, Ho M, Chilton-MacNeill S, Zielenska M . Use of chromogenic in situ hybridization to identify MYCN gene copy number in neuroblastoma using routine tissue sections. Am J Surg Pathol 2006; 30: 635–642.
Ambros IM, Benard J, Boavida M, Bown N, Caron H, Combaret V et al. Quality assessment of genetic markers used for therapy stratification. J Clin Oncol 2003; 21: 2077–2084.
Kerbl R, Ambros IM, Ambros PF, Lackner H, Dornbusch HJ, Urban CE . Neuroblastoma with focal MYCN amplification and bone marrow infiltration: a staging and treatment dilemma. Med Pediatr Oncol 2002; 38: 109–111.
Cañete A, Gerrard M, Rubie H, Castel V, Di Cataldo A, Munzer C et al. Poor survival for infants with MYCN-amplified metastatic neuroblastoma despite intensified treatment: the International Society of Paediatric Oncology European Neuroblastoma Experience. J Clin Oncol 2009; 27: 1014–1019.
Matthay KK, Edeline V, Lumbroso J, Tanguy ML, Asselain B, Zucker JM et al. Correlation of early metastatic response by 123I-metaiodobenzylguanidine scintigraphy with overall response and event-free survival in stage IV neuroblastoma. J Clin Oncol 2003; 21: 2486–2491.
Spitz R, Hero B, Skowron M, Ernestus K, Berthold F . MYCN-status in neuroblastoma: characteristics of tumours showing amplification, gain, and non-amplification. Eur J Cancer 2004; 40: 2753–2759.
Valent A, Guillaud-Bataille M, Farra C, Lozach F, Spengler B, Terrier-Lacombe MJ et al. Alternative pathways of MYCN gene copy number increase in primary neuroblastoma tumors. Cancer Genet Cytogenet 2004; 153: 10–15.
Maris JM, Hogarty MD, Bagatell R, Cohn SL . Neuroblastoma. Lancet 2007; 369: 2106–2120.
Bishop MW, Yin H, Shimada H, Towbin AJ, Miethke A, Weiss B . Management of stage 4S composite neuroblastoma with a MYCN-amplified nodule. J Pediatr Hematol Oncol 2014; 36: e31–e35.
Villamon E, Berbegall AP, Piqueras M, Tadeo I, Castel V, Djos A et al. Genetic instability and intratumoral heterogeneity in neuroblastoma with MYCN amplification plus 11q deletion. PloS One 2013; 8: e53740.
Schleiermacher G, Mosseri V, London WB, Maris JM, Brodeur GM, Attiyeh E et al. Segmental chromosomal alterations have prognostic impact in neuroblastoma: a report from the INRG project. Br J Cancer 2012; 107: 1418–1422.
Ambros IM, Brunner B, Aigner G, Bedwell C, Beiske K, Benard J et al. A multilocus technique for risk evaluation of patients with neuroblastoma. Clin Cancer Res 2011; 17: 792–804.
Schleiermacher G, Michon J, Huon I, d'Enghien CD, Klijanienko J, Brisse H et al. Chromosomal CGH identifies patients with a higher risk of relapse in neuroblastoma without MYCN amplification. Br J Cancer 2007; 97: 238–246.
Capasso M, Diskin SJ . Genetics and genomics of neuroblastoma. Cancer Treat Res 2010; 155: 65–84.
George RE, Attiyeh EF, Li S, Moreau LA, Neuberg D, Li C et al. Genome-wide analysis of neuroblastomas using high-density single nucleotide polymorphism arrays. PloS One 2007; 2: e255.
Lastowska M, Viprey V, Santibanez-Koref M, Wappler I, Peters H, Cullinane C et al. Identification of candidate genes involved in neuroblastoma progression by combining genomic and expression microarrays with survival data. Oncogene 2007; 26: 7432–7444.
Caren H, Kryh H, Nethander M, Sjoberg RM, Trager C, Nilsson S et al. High-risk neuroblastoma tumors with 11q-deletion display a poor prognostic, chromosome instability phenotype with later onset. Proc Natl Acad Sci USA 2010; 107: 4323–4328.
Theissen J, Oberthuer A, Hombach A, Volland R, Hertwig F, Fischer M et al. Chromosome 17/17q gain and unaltered profiles in high resolution array-CGH are prognostically informative in neuroblastoma. Genes Chromosomes Cancer 2014; 53: 639–649.
Speleman F, De Preter K, Vandesompele J . Neuroblastoma genetics and phenotype: a tale of heterogeneity. Semin Cancer Biol 2011; 21: 238–244.
Ambros IM, Brunner C, Abbasi R, Frech C, Ambros PF . Ultra-high density SNParray in neuroblastoma molecular diagnostics. Front Oncol 2014; 4: 202.
Mosse YP, Diskin SJ, Wasserman N, Rinaldi K, Attiyeh EF, Cole K et al. Neuroblastomas have distinct genomic DNA profiles that predict clinical phenotype and regional gene expression. Genes Chromosomes Cancer 2007; 46: 936–949.
Morowitz M, Shusterman S, Mosse Y, Hii G, Winter CL, Khazi D et al. Detection of single-copy chromosome 17q gain in human neuroblastomas using real-time quantitative polymerase chain reaction. Mod Pathol 2003; 16: 1248–1256.
Lundberg G, Jin Y, Sehic D, Ora I, Versteeg R, Gisselsson D . Intratumour diversity of chromosome copy numbers in neuroblastoma mediated by on-going chromosome loss from a polyploid state. PloS One 2013; 8: e59268.
Brodeur GM . Significance of intratumoral genetic heterogeneity in neuroblastomas. Med Pediatr Oncol 2002; 38: 112–113.
Lastowska M, Cotterill S, Bown N, Cullinane C, Variend S, Lunec J et al. Breakpoint position on 17q identifies the most aggressive neuroblastoma tumors. Genes Chromosomes Cancer 2002; 34: 428–436.
Vandesompele J, Michels E, De Preter K, Menten B, Schramm A, Eggert A et al. Identification of 2 putative critical segments of 17q gain in neuroblastoma through integrative genomics. Int J Cancer 2008; 122: 1177–1182.
Fujita T, Igarashi J, Okawa ER, Gotoh T, Manne J, Kolla V et al. CHD5, a tumor suppressor gene deleted from 1p36.31 in neuroblastomas. J Natl Cancer Inst 2008; 100: 940–949.
White PS, Thompson PM, Gotoh T, Okawa ER, Igarashi J, Kok M et al. Definition and characterization of a region of 1p36.3 consistently deleted in neuroblastoma. Oncogene 2005; 24: 2684–2694.
Coco S, Theissen J, Scaruffi P, Stigliani S, Moretti S, Oberthuer A et al. Age-dependent accumulation of genomic aberrations and deregulation of cell cycle and telomerase genes in metastatic neuroblastoma. Int J Cancer 2012; 131: 1591–1600.
Cetinkaya C, Martinsson T, Sandgren J, Trager C, Kogner P, Dumanski J et al. Age dependence of tumor genetics in unfavorable neuroblastoma: arrayCGH profiles of 34 consecutive cases, using a Swedish 25-year neuroblastoma cohort for validation. BMC Cancer 2013; 13: 231.
Attiyeh EF, London WB, Mosse YP, Wang Q, Winter C, Khazi D et al. Chromosome 1p and 11q deletions and outcome in neuroblastoma. N Engl J Med 2005; 353: 2243–2253.
Santo EE, Ebus ME, Koster J, Schulte JH, Lakeman A, van Sluis P et al. Oncogenic activation of FOXR1 by 11q23 intrachromosomal deletion-fusions in neuroblastoma. Oncogene 2012; 31: 1571–1581.
Wang Q, Diskin S, Rappaport E, Attiyeh E, Mosse Y, Shue D et al. Integrative genomics identifies distinct molecular classes of neuroblastoma and shows that multiple genes are targeted by regional alterations in DNA copy number. Cancer Res 2006; 66: 6050–6062.
Buckley PG, Alcock L, Bryan K, Bray I, Schulte JH, Schramm A et al. Chromosomal and microRNA expression patterns reveal biologically distinct subgroups of 11q- neuroblastoma. Clin Cancer Res 2010; 16: 2971–2978.
Kumps C, Fieuw A, Mestdagh P, Menten B, Lefever S, Pattyn F et al. Focal DNA copy number changes in neuroblastoma target MYCN regulated genes. PloS One 2013; 8: e52321.
Fix A, Lucchesi C, Ribeiro A, Lequin D, Pierron G, Schleiermacher G et al. Characterization of amplicons in neuroblastoma: high-resolution mapping using DNA microarrays, relationship with outcome, and identification of overexpressed genes. Genes Chromosomes Cancer 2008; 47: 819–834.
Guimier A, Ferrand S, Pierron G, Couturier J, Janoueix-Lerosey I, Combaret V et al. Clinical characteristics and outcome of patients with neuroblastoma presenting genomic amplification of loci other than MYCN. PloS One 2014; 9: e101990.
Fix A, Peter M, Pierron G, Aurias A, Delattre O, Janoueix-Lerosey I . High-resolution mapping of amplicons of the short arm of chromosome 1 in two neuroblastoma tumors by microarray-based comparative genomic hybridization. Genes Chromosomes Cancer 2004; 40: 266–270.
Brodeur GM . Commentary on Kaneko et al.: Intensified chemotherapy increases the survival rates in patients with stage 4 neuroblastoma with MYCN amplification. J Pediatr Hematol Oncol 2002; 24: 608–609.
Shimada H, Ambros IM, Dehner LP, Hata J, Joshi VV, Roald B et al. The International Neuroblastoma Pathology Classification (the Shimada system). Cancer 1999; 86: 364–372.
Piqueras M, Navarro S, Cañete A, Castel V, Noguera R . How to minimise the effect of tumour cell content in detection of aberrant genetic markers in neuroblastoma. Br J Cancer 2011; 105: 89–92.
Acknowledgements
Spanish Society of Hematology and Pediatric Oncology and Désirée Ramal (Pediatric Oncology Unit, Hospital Universitario y Politécnico La Fé, Valencia, Spain) are gratefully acknowledged for patient data management. We thank members of the International Society of Pediatric Oncology Europe Neuroblastoma Biology Group for validation of the genetic diagnosis. We also thank David Harrison for English language editing. This work was supported by FIS (contract PI10/15) and RTICC (contracts RD12/36/20 and RD06/20/102), Instituto de Salud Carlos III, Spanish Ministry of Science and Innovation & European Regional Development Fund.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Berbegall, A., Villamón, E., Piqueras, M. et al. Comparative genetic study of intratumoral heterogenous MYCN amplified neuroblastoma versus aggressive genetic profile neuroblastic tumors. Oncogene 35, 1423–1432 (2016). https://doi.org/10.1038/onc.2015.200
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/onc.2015.200
- Springer Nature Limited
This article is cited by
-
Impact of extracellular matrix stiffness on genomic heterogeneity in MYCN-amplified neuroblastoma cell line
Journal of Experimental & Clinical Cancer Research (2020)
-
Diagnostic accuracy of circulating-free DNA for the determination of MYCN amplification status in advanced-stage neuroblastoma: a systematic review and meta-analysis
British Journal of Cancer (2020)
-
Heterogeneous MYCN amplification in neuroblastoma: a SIOP Europe Neuroblastoma Study
British Journal of Cancer (2018)
-
11q deletion in neuroblastoma: a review of biological and clinical implications
Molecular Cancer (2017)