
Abstract
Background:
Patients with chronic obstructive pulmonary disease (COPD) who were naive to anticholinergics before the TIOtropium Safety and Performance In Respimat (TIOSPIR) trial may reflect patients seen in practice, in particular in primary care. In addition, investigating safety in these patients avoids the potential bias in patients who previously received anticholinergics and may be tolerant of their effects.
Aims:
The aim of this study was to evaluate whether patients naive to anticholinergic therapy who were treated with tiotropium Respimat 2.5 or 5 μg had different safety and efficacy outcomes than patients treated with tiotropium HandiHaler 18 μg.
Methods:
A post hoc analysis of patients who were not receiving anticholinergics before TIOSPIR (N=6,966/17,135) was conducted. Primary end points were risk of death from any cause and risk of COPD exacerbation. Secondary outcomes included severe exacerbation and major adverse cardiovascular events (MACE). Additional analysis of exacerbations was carried out in anticholinergic-naive patients with moderate (GOLD II) disease.
Results:
Anticholinergic-naive patients had less severe disease than the total TIOSPIR population. Discontinuations because of anticholinergic side effects were infrequent (0.9% overall). Similar to the primary study, patients in the tiotropium Respimat groups had no difference in the risk of death or risk of any or severe exacerbation than patients treated with tiotropium HandiHaler. Risk of MACE was similar across the Respimat and HandiHaler groups. Rates of exacerbations in the subgroup of patients with moderate disease were similar across the Respimat and HandiHaler groups.
Conclusions:
Tiotropium Respimat and HandiHaler have similar safety and efficacy profiles in patients who are naive to anticholinergic therapy.
Similar content being viewed by others


Introduction
Tiotropium (SPIRIVA, Boehringer Ingelheim Pharma & Co KG, Ingelheim am Rhein, Germany) is a once-daily, long-acting, anticholinergic bronchodilator available in two formulations: dry powder via HandiHaler (18 μg once daily) and as an aqueous solution via the Respimat Soft Mist Inhaler (5 μg (two puffs of 2.5 μg once daily)).1,2 Tiotropium HandiHaler 18 μg and tiotropium Respimat 5 μg have demonstrated similar improvements in lung function, symptoms and quality of life3–6 and have similar pharmacokinetic profiles in patients with chronic obstructive pulmonary disease (COPD).7
Queries around the safety of Respimat8–10 were addressed in the TIOtropium Safety and Performance In Respimat (TIOSPIR; NCT01126437) trial11—the largest long-term, randomised, double-blind trial in patients with COPD performed to date. The trial showed similar safety and exacerbation efficacy profiles for tiotropium Respimat 2.5 μg and 5 μg compared with HandiHaler 18 μg.
A common criticism of randomised clinical trials (RCTs) is that the selected patient populations may not be truly representative of patients seen in routine clinical practice—in particular, patients treated in primary care.12–14 A unique characteristic of TIOSPIR was the liberal inclusion criteria that were chosen to select a typical COPD patient population, including patients with a wide range of disease severities, as well as patients with stable cardiac disease.11
TIOSPIR also included a large population of patients with COPD who were naive to anticholinergic treatment at baseline. This represents an important patient group that may be highly representative of patients commonly seen in primary care. Patients within the primary TIOSPIR study who were previously treated with anticholinergics might be seen to constitute a selected population with a higher tolerance to anticholinergic effects and could have introduced a selection bias in the analysis of tiotropium’s safety. Therefore, it is conceivable that the anticholinergic-naive group might have been at an increased risk of side effects commonly associated with the class and may have responded differently to treatment with tiotropium Respimat or HandiHaler.
To investigate this possibility, this post hoc analysis of the TIOSPIR trial studied whether patients who had not previously received anticholinergic therapy and who were treated with Respimat 2.5 or 5 μg had different safety and/or efficacy outcomes compared with patients treated with HandiHaler 18 μg.
Materials and methods
Study design
TIOSPIR was a large (N=17,135) long-term (2–3 years), randomised, double-blind, double-dummy, parallel-group, actively controlled, event-driven trial in patients with COPD.11,15 Patients received once-daily Respimat 2.5 μg (two puffs of 1.25 μg) or 5 μg (two puffs of 2.5 μg) or once-daily HandiHaler 18 μg. Primary outcomes were time to death from any cause and time to first COPD exacerbation. Secondary outcomes included time to severe (hospitalised) exacerbations and time to major adverse cardiovascular events (MACE). The study design has been described previously.11,15
Study population
Patients had a diagnosis of COPD with forced expiratory volume in 1 s (FEV1)⩽70% of forced vital capacity, FEV1⩽70% predicted and ⩾10 pack-years of smoking history, were aged ⩾40 years and were permitted to use their usual background treatment for COPD other than anticholinergics. All patients (including those with premature discontinuation) were followed up for vital status until the end of the study.
At enrolment, patients were asked to provide details of COPD and other medication received within the past 2 months. For this post hoc subgroup analysis, patients were included if they were not receiving short- or long-acting inhaled anticholinergics during the 2 months before the start of the trial.
Statistical analysis
Hazard ratios (HR) and 95% confidence intervals (CI) were calculated using a Cox-proportional hazards regression model (without covariate adjustment). Rate ratios and 95% CI were used to compare incidence rates. Negative binomial regression models were used to compare event rates.
For analysis of death (including fatal MACE), events occurring during treatment and vital status follow-up (vital status analysis) were considered. For all other analyses (including MACE and COPD exacerbations), only events with onset in the on-treatment period were noted (on-treatment analysis). An on-treatment sensitivity analysis was conducted for time to death. Subgroup analyses by patient characteristics at baseline were conducted for time to death and exacerbation risk.
Results
Study population
Overall, 6,966 patients naive to anticholinergic treatment at baseline (Respimat 2.5 μg n=2,345; Respimat 5 μg n=2,312; HandiHaler 18 μg n=2,309) were randomised and treated for a mean follow-up duration of 834 days. A total of 541 (23.1%), 517 (22.4%) and 500 (21.7%) patients in the Respimat 2.5 μg, 5 μg and HandiHaler 18 μg groups, respectively, prematurely discontinued from the study. Discontinuation attributed to anticholinergic side effects occurred in 0.7 and 1.0% of patients in the Respimat 2.5 and 5 μg groups, respectively, and 0.9% of patients in the HandiHaler group.
Patient baseline demographics and characteristics were similar in the three groups (Table 1). Most patients were Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages II (48.8%) and III (38.4%). The majority of patients (77.3%) were receiving pulmonary medication at baseline; approximately half of the patients were taking an inhaled corticosteroid or long-acting β2-agonist (50.2 and 51.6%, respectively) (Table 1). Of the patients who reported symptoms of breathlessness (n=6,688; 96.1%), the majority were classified as modified Medical Research Council (mMRC) scale 1 (n=2,694, 40.3%) or scale 2 (n=2,486, 37.2%) (Table 1). Approximately 8–9% of patients had a history of cardiac arrhythmia (Table 1). A total of 3,349 (48.1%) patients had ⩾1 COPD exacerbation in the year before the study (Table 1).
Safety
Risks of death (measured as time to death, vital status analysis) and the adjudicated causes of death were similar between both doses of Respimat and HandiHaler 18 μg (Figures 1a, b; Table 2). Similar results were obtained for an on-treatment sensitivity analysis of time to fatal adverse event (Respimat 2.5 μg versus Respimat 5.0 μg: HR (95% CI) 1.21 (0.95, 1.54); Respimat 2.5 μg versus HandiHaler 18 μg: HR (95% CI) 1.11 (0.87, 1.40); Respimat 5 μg versus HandiHaler 18 μg: 0.91 (0.71, 1.17)). Subgroup analyses (including cardiac history at baseline and pulmonary comedication at baseline) showed no difference between groups.

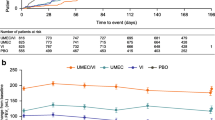
Kaplan–Meier plots showing time to (a) death, (b) FAE, (c) first MACE and (d) fatal MACE. Data for patients with event are n (%). CI, confidence interval; COPD, chronic obstructive pulmonary disease; FAE, fatal adverse event; MACE, major adverse cardiovascular event. Six patients (Respimat 2.5 μg, one patient; Respimat 5 μg, three patients; HandiHaler 18 μg, two patients) from sites with data irregularities were excluded from first MACE analyses. On-treatment analyses (from randomisation to drug stop+30 days).
Risk of first MACE (on-treatment analysis) was similar for Respimat 2.5 μg and 5.0 μg versus HandiHaler 18 μg (HR (95% CI): 1.11 (0.81, 1.51) P=0.523, and HR (95% CI) 1.20 (0.88, 1.63) P=0.244, respectively; Figure 1c). Rates of fatal MACE (vital status analysis) were similar in each of the treatment groups (Figure 1d; Table 2).
Efficacy
Risk of exacerbation (measured as time to first exacerbation, on-treatment analysis) showed no significant difference between the Respimat groups and HandiHaler 18 μg (Figure 2a; Table 3). The risk of moderate-to-severe and severe (hospitalised) exacerbations was also similar across groups (Figure 2b; Table 3).

Kaplan–Meier plots showing time to (a) first exacerbation, and (b) first severe (hospitalised) exacerbation. Data for patients with event are n (%). COPD exacerbations were defined as the worsening of two or more major respiratory symptoms (dyspnoea, cough, sputum, chest tightness or wheezing) with a duration of at least 3 days requiring specified treatment changes: (a) mild exacerbations: a newly prescribed maintenance bronchodilator; (b) moderate exacerbations: a prescription for antibiotics, systemic glucocorticoids or both; (c) severe exacerbations: hospitalisation. Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease. Six patients (Respimat 2.5 μg, one patient; Respimat 5 μg, three patients; HandiHaler 18 μg, two patients) from sites with data irregularities were excluded from analyses. On-treatment analyses (from randomisation to drug stop+1 day).
Exacerbation risk did not differ between treatments in any of the patient subgroups. Patients with less impaired lung function (GOLD stage II) responded equally to Respimat and HandiHaler with respect to the rate of any exacerbation, moderate-to-severe exacerbations and severe exacerbations (Table 3). As might be expected, patients in the GOLD stage II category experienced fewer exacerbations than the overall population of anticholinergic-naive patients (Table 3).
Discussion
Main findings
The present study showed that patients with COPD who were naive to anticholinergic treatment at baseline, and who were treated with Respimat 2.5 or 5 μg, were at a similar risk of mortality and adverse cardiac events as patients receiving HandiHaler 18 μg.
Compared with the overall population, the present patient subgroup was similar to the TIOSPIR primary study population with regards to baseline characteristics; however, mortality rates during the study were slightly lower. It is likely that patients who were anticholinergic naive at baseline had less severe disease than the overall population; indeed, a slightly higher percentage of patients was classified as GOLD stage II. In addition, patients in the anticholinergic-naive subgroup were receiving fewer cardiovascular medications at baseline, indicating fewer cardiovascular comorbidities. Together, this may have contributed to the lower mortality rates observed. Nevertheless, the results of this post hoc analysis of TIOSPIR were consistent with the main study findings. In addition, the analysis addresses concerns that the safety of tiotropium Respimat could not be completely demonstrated in TIOSPIR because of a potentially selected population with a higher tolerance to anticholinergic effects at baseline.
Interpretation of findings in relation to previously published work
COPD is a heterogeneous disease comprising a wide range of clinical phenotypes that may respond differently to treatment.16 Not all of these phenotypes (particularly patients with mild COPD) are represented within populations included in RCTs. Indeed, a common criticism of evidence-based medicine is that it is not known how well RCT evidence applies to COPD patients typically seen within clinical practice.12–14
In a comparison of primary care data from the Uncovering and Noting Long-term Outcomes in COPD (UNLOCK) database with six large RCTs of patients with COPD, significant differences were observed with respect to baseline characteristics.13 Patients included in the RCTs tended to be younger, were predominantly male and had significantly worse lung function and quality-of-life scores than primary care patients. Disparities were also observed with respect to exacerbations: a lower mean exacerbation rate per year and lower number of patients with ⩾1 or ⩾2 exacerbations being observed in the UNLOCK population.13 A further interesting observation from the UNLOCK analysis is that patients with GOLD stage I or II COPD comprised 20.7% and 53.3%, respectively, of the total UNLOCK population.13 This compares with a complete absence of patients at GOLD stage I and 45% of patients at GOLD stage II in the combined RCTs, normally caused by exclusion criteria for mild patients. In the TIOSPIR anticholinergic-naive subpopulation, 0.3% patients were at GOLD stage I (because of the inclusion of patients with an FEV1 percent predicted of <70%) and 48.8% patients were at GOLD stage II. Thus, almost half of the patients in this subgroup were considered to have moderate COPD. Comparison of other baseline characteristics from the TIOSPIR anticholinergic-naive subpopulation with those from the UNLOCK cohort and combined RCTs indicate that this subgroup may have greater similarity to the UNLOCK population than other large COPD trials. Fewer patients in the anticholinergic subgroup had also experienced one or more exacerbation in the year before the study (48%) than patients from other large RCTs (59%), thus better reflecting the UNLOCK population (44%; Supplementary Table 1). Together, these comparisons indicate that the anticholinergic-naive subgroup from TIOSPIR may better reflect patients observed in primary care than patients typically randomised to other large COPD trials.
The primary efficacy outcome from TIOSPIR was time to first COPD exacerbation. Exacerbations are an important component of COPD, having a significant impact on disease progression and health status, as well as increasing the risk of further exacerbations and death.17–19 Thus, the prevention of exacerbations is a primary goal in COPD management.20 Tiotropium Respimat and HandiHaler have been shown to reduce COPD exacerbations versus placebo and other therapies, including among subgroups of patients.6,21–28 For example, in a prespecified secondary analysis of the Understanding Potential Long-term Impacts on Function with Tiotropium (UPLIFT) trial, tiotropium HandiHaler reduced the number of exacerbations per patient-year by 16% versus control in patients naive to maintenance therapy before the study.25 In subgroup analyses of the Prevention Of Exacerbations with Tiotropium in COPD (POET-COPD) study, tiotropium HandiHaler significantly prolonged the time to first exacerbation (HR (95% CI), 0.88 (0.79, 0.99); P=0.028) and first severe exacerbation (HR (95% CI), 0.66 (0.48, 0.91); P=0.012) in GOLD stage II patients, and significantly reduced the annual exacerbation rate (rate ratio [95% CI], 0.77 (0.63, 0.94); P=0.012) in maintenance therapy–naive patients, when compared with salmeterol.27 Before TIOSPIR, the relative efficacy of exacerbation reduction by Respimat and HandiHaler was unknown. In this current post hoc analysis, the incidence of exacerbations was shown to be similar among anticholinergic-naive patients who were treated with either Respimat or HandiHaler. Furthermore, the subgroup analysis of exacerbation risk in GOLD stage II patients shows that Respimat and HandiHaler have similar efficacy profiles in patients with less impaired lung function or health status.
Further evidence for tiotropium’s safety was provided by the low incidence of discontinuations observed in each of the treatment groups because of anticholinergic side effects. Other clinical studies of tiotropium in COPD have reported similarly low rates of discontinuation because of undesirable effects such as dry mouth, occurring in 0.1% of patients treated with tiotropium Respimat 5 μg (5 clinical trials)2 and 0.2% of patients treated with tiotropium HandiHaler 18 μg (28 clinical trials).1
Strengths and limitations of this study
A key limitation of the study is that it was a post hoc analysis rather than a prespecified subgroup analysis. Nevertheless, being one of the largest, long-term, randomised trials of a broad range of patients with COPD, TIOSPIR lends itself to statistically powerful subgroup analyses.
Implications for future research, policy and practice
This post hoc analysis examined whether the subpopulation of patients in TIOSPIR who were naive to anticholinergic therapy at baseline responded differently to treatment with tiotropium Respimat than to tiotropium HandiHaler. Patients who are naive to anticholinergic therapy are frequently seen within daily practice, and the results of this analysis will therefore be of particular interest to primary care physicians and policy makers. Better definition of treatment responses of individuals according to their treatment history will ultimately help tailor more targeted interventions in patients with COPD.
Conclusions
In this post hoc analysis, patients with COPD who were naive to anticholinergic treatment had similar efficacy and safety profiles when treated with tiotropium Respimat or HandiHaler in the TIOSPIR trial.
This study provides further data that addresses prior safety concerns regarding tiotropium Respimat and provides additional evidence that tiotropium Respimat treatment is also safe for patients who were not previously treated with an anticholinergic, including patients with mild disease more commonly seen in primary care.
References
Boehringer Ingelheim: Summary of Product Characteristics (SPC): Spiriva 18 microgram inhalation powder, hard capsule. EMC. Boehringer Ingelheim Ltd. February 2015. Available at: https://www.medicines.org.uk/emc/medicine/10039.
Boehringer Ingelheim: Summary of Product Characteristics (SPC): Spiriva Respimat 2.5 microgram, inhalation solution. EMC. Boehringer Ingelheim Ltd. January 2015. Available at: https://www.medicines.org.uk/emc/medicine/20134l
Karner C, Chong J, Poole P . Tiotropium versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2014; 7: CD009285.
Keating GM . Tiotropium bromide inhalation powder: a review of its use in the management of chronic obstructive pulmonary disease. Drugs 2012; 72: 273–300.
Keating GM . Tiotropium Respimat® Soft Mist inhaler: a review of its use in chronic obstructive pulmonary disease. Drugs 2014; 74: 1801–1816.
Tashkin DP, Celli B, Senn S, Burkhart D, Kesten S, Menjoge S et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med 2008; 359: 1543–1554.
Hohlfeld JM, Sharma A, van Noord JA, Cornelissen PJ, Derom E, Towse L et al. Pharmacokinetics and pharmacodynamics of tiotropium solution and tiotropium powder in chronic obstructive pulmonary disease. J Clin Pharmacol 2014; 54: 405–414.
Boehringer Ingelheim: Tiotropium (Spiriva) Respimat: evaluation of fatal events. Boehringer Ingelheim Ltd. 2010. Available at: http://trials.boehringer-ingelheim.com/content/dam/internet/opu/clinicaltrial/com_EN/results/Pooled%20analysis/PA_205.372_251_252_254_255_U10-3255-01.pdf
Dong YH, Lin HH, Shau WY, Wu YC, Chang CH, Lai MS . Comparative safety of inhaled medications in patients with chronic obstructive pulmonary disease: systematic review and mixed treatment comparison meta-analysis of randomised controlled trials. Thorax 2013; 68: 48–56.
Singh S, Loke YK, Enright PL, Furberg CD . Mortality associated with tiotropium mist inhaler in patients with chronic obstructive pulmonary disease: systematic review and meta-analysis of randomised controlled trials. BMJ 2011; 342: d3215.
Wise RA, Anzueto A, Cotton D, Dahl R, Devins T, Disse B et al. Tiotropium Respimat inhaler and the risk of death in COPD. N Engl J Med 2013; 369: 1491–1501.
Herland K, Akselsen JP, Skjonsberg OH, Bjermer L . How representative are clinical study patients with asthma or COPD for a larger "real life" population of patients with obstructive lung disease? Respir Med 2005; 99: 11–19.
Kruis AL, Stallberg B, Jones RC, Tsiligianni IG, Lisspers K, van der Molen T et al. Primary care COPD patients compared with large pharmaceutically-sponsored COPD studies: an UNLOCK validation study. PLoS ONE 2014; 9: e90145.
Travers J, Marsh S, Caldwell B, Williams M, Aldington S, Weatherall M et al. External validity of randomized controlled trials in COPD. Respir Med 2007; 101: 1313–1320.
Wise RA, Anzueto A, Calverley P, Dahl R, Dusser D, Pledger G et al. The Tiotropium Safety and Performance in Respimat Trial (TIOSPIR), a large scale, randomized, controlled, parallel-group trial-design and rationale. Respir Res 2013; 14: 40.
Mannino DM . COPD: epidemiology, prevalence, morbidity and mortality, and disease heterogeneity. Chest 2002; 121 (5 Suppl): 121S–126S.
Celli BR, Barnes PJ . Exacerbations of chronic obstructive pulmonary disease. Eur Respir J 2007; 29: 1224–1238.
Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA . Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax 2002; 57: 847–852.
Soler-Cataluna JJ, Martinez-Garcia MA, Roman SP, Salcedo E, Navarro M, Ochando R . Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005; 60: 925–931.
Global Initiative for Chronic Obstructive Lung Disease (GOLD): Global strategy for the diagnosis, management, and prevention of COPD. Available at: http://www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html, 2015.
Bateman ED, Tashkin D, Siafakas N, Dahl R, Towse L, Massey D et al. A one-year trial of tiotropium Respimat plus usual therapy in COPD patients. Respir Med 2010; 104: 1460–1472.
Decramer M, Anzueto A, Kerwin E, Kaelin T, Richard N, Crater G et al. Efficacy and safety of umeclidinium plus vilanterol versus tiotropium, vilanterol, or umeclidinium monotherapies over 24 weeks in patients with chronic obstructive pulmonary disease: results from two multicentre, blinded, randomised controlled trials. Lancet Respir Med 2014; 2: 472–486.
Decramer ML, Chapman KR, Dahl R, Frith P, Devouassoux G, Fritscher C et al. Once-daily indacaterol versus tiotropium for patients with severe chronic obstructive pulmonary disease (INVIGORATE): a randomised, blinded, parallel-group study. Lancet Respir Med 2013; 1: 524–533.
Niewoehner DE, Rice K, Cote C, Paulson D, Cooper JA Jr., Korducki L et al. Prevention of exacerbations of chronic obstructive pulmonary disease with tiotropium, a once-daily inhaled anticholinergic bronchodilator: a randomized trial. Ann Intern Med 2005; 143: 317–326.
Troosters T, Celli B, Lystig T, Kesten S, Mehra S, Tashkin DP et al. Tiotropium as a first maintenance drug in COPD: secondary analysis of the UPLIFT trial. Eur Respir J 2010; 36: 65–73.
Vogelmeier C, Hederer B, Glaab T, Schmidt H, Rutten-van Molken MP, Beeh KM et al. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N Engl J Med 2011; 364: 1093–1103.
Vogelmeier C, Fabbri LM, Rabe KF, Beeh KM, Schmidt H, Metzdorf N et al. Effect of tiotropium vs. salmeterol on exacerbations: GOLD II and maintenance therapy naive patients. Respir Med 2013; 107: 75–83.
Wedzicha JA, Decramer M, Ficker JH, Niewoehner DE, Sandstrom T, Taylor AF et al. Analysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): a randomised, double-blind, parallel-group study. Lancet Respir Med 2013; 1: 199–209.
Acknowledgements
Editorial and writing assistance was provided by Carol A Richter and Sarah J Petit at PAREXEL (funded by Boehringer Ingelheim). The TIOSPIR trial and this subsequent post hoc analysis were funded by Boehringer Ingelheim.
Funding
Funding was provided by Boehringer Ingelheim.
Author information
Authors and Affiliations
Contributions
Writing assistance was provided by PAREXEL, and all authors had equal contribution in terms of reviewing all drafts. All authors had full access to the data and read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
RW reports receiving consulting fees from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, GlaxoSmithKline, Janssen, Mylan, Novartis, Pfizer, Pulmonx, Roche, Spiration and Sunovion, with grant support from Boehringer Ingelheim, Forest Laboratories, GlaxoSmithKline, Takeda and Pearl Therapeutics; PMAC reports receiving consulting fees, lecture fees and travel support from Boehringer Ingelheim, GlaxoSmithKline, Novartis and Takeda; RD reports receiving consulting fees, lecture fees and grant support from Boehringer Ingelheim and Novartis; DD reports receiving consulting fees, lecture fees and payment for the development of educational activities from Boehringer Ingelheim, Chiesi, Dey Pharma, Novartis, Nycomed and Pfizer; AA reports receiving consulting fees, lecture fees and travel support from AstraZeneca, Boehringer Ingelheim, Forest Laboratories, GlaxoSmithKline and Novartis, and grant support to the University of Texas Health Science Centre from GlaxoSmithKline; NM, AF and AM are employees of Boehringer Ingelheim.
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Wise, R., Calverley, P., Dahl, R. et al. Safety and efficacy of tiotropium Respimat versus HandiHaler in patients naive to treatment with inhaled anticholinergics: a post hoc analysis of the TIOSPIR trial. npj Prim Care Resp Med 25, 15067 (2015). https://doi.org/10.1038/npjpcrm.2015.67
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/npjpcrm.2015.67
- Springer Nature Limited