

Abstract
Immunotherapy is proving to be an effective therapeutic approach in a variety of cancers. But despite the clinical success of antibodies against the immune regulators CTLA4 and PD-L1/PD-1, only a subset of people exhibit durable responses, suggesting that a broader view of cancer immunity is required. Immunity is influenced by a complex set of tumour, host and environmental factors that govern the strength and timing of the anticancer response. Clinical studies are beginning to define these factors as immune profiles that can predict responses to immunotherapy. In the context of the cancer-immunity cycle, such factors combine to represent the inherent immunological status — or 'cancer–immune set point' — of an individual.
Similar content being viewed by others


Main
Cancer is a genetic disease, with the growth of tumour cells initiated by mutations that activate oncogenic drivers. This process is combined with the genetic or non-genetic activation or inactivation of genes that promote or suppress the proliferation of tumours. In many cancers, oncogenesis is accompanied by the accumulation of mutations, which can provide a selective advantage to populations of cancer cells by increasing their degree of genetic diversity, accelerating their evolutionary fitness. Yet this diversity comes at a cost: the further a cancer cell diverges from a normal cell, the more likely it is to be recognized as foreign by the immune system. Although long considered a possibility, it has been demonstrated only in the past five years that the mutational burden of tumours contributes to immune recognition of cancer and that it may, at least partly, determine a person's response to cancer immunotherapy1,2,3,4.
The role of the immune system in cancer remained unappreciated for many decades because tumours effectively suppress immune responses by activating negative regulatory pathways (also called checkpoints) that are associated with immune homeostasis or by adopting features that enable them to actively escape detection5,6,7. Two such checkpoints, cytotoxic T-lymphocyte protein 4 (CTLA4) and programmed cell death protein 1 (PD-1), have garnered the most attention so far. CTLA4 is a negative regulator of T cells that acts to control T-cell activation by competing with the co-stimulatory molecule CD28 for binding to shared ligands CD80 (also known as B7.1) and CD86 (also known as B7.2). The cell-surface receptor PD-1 is expressed by T cells on activation during priming or expansion and binds to one of two ligands, PD-L1 and PD-L2. Many types of cells can express PD-L1, including tumour cells and immune cells after exposure to cytokines such as interferon (IFN)-γ; however, PD-L2 is expressed mainly on dendritic cells in normal tissues. Binding of PD-L1 or PD-L2 to PD-1 generates an inhibitory signal that attenuates the activity of T cells. The 'exhaustion' of effector T cells was identified through studies of chronic viral infection in mice in which the PD-L1/PD-1 axis was found to be an important negative feedback loop that ensures immune homeostasis; it is also an important axis for restricting tumour immunity.
Although blocking these checkpoints is known to elicit antitumour responses in mice8,9,10,11, clinical trials are now providing evidence of their importance in cancer. Specifically, for antibodies that block the interaction between PD-L1 and PD-1, clinical responses to monotherapy have been seen across a wide range of solid and haematologic cancers12. Importantly, the responses are often durable, lasting years or indefinitely, and occur without causing serious toxicity in most people. These results suggest that many people with cancer have pre-existing T-cell-mediated immunity that is restrained by the PD-L1/PD-1-induced suppression of T cells. They also emphasize the role of immunosuppression as a main impediment to the series of steps that is required for effective anticancer responses — the cancer–immunity cycle13. However, the PD-L1/PD-1 axis cannot solely account for restraining the immune response. Not only do other negative regulators exist, but the immune profile of an individual reflects the contribution of an array of factors, including the intrinsic properties of a tumour (for example, cytokine secretion or genetic composition) and extrinsic factors such as the gut microbiota, the presence of infection or exposure to sunlight. These elements combine to produce a 'cancer–immune set point', which can be defined as the equilibrium between the factors that promote or suppress anticancer immunity. The set point therefore represents the threshold that must be surpassed for a person with cancer to respond to immunotherapy. This is a useful concept as the responses of people (or even mice) with overtly similar tumours can vary considerably.
The mechanisms that underlie cancer immunotherapy differ considerably from those of other approaches to cancer treatment. Unlike chemotherapy or oncogene-targeted therapies, cancer immunotherapy relies on promoting an anticancer response that is dynamic and not limited to targeting a single oncogenic derangement or other autonomous feature of cancer cells. Cancer immunotherapy can therefore lead to antitumour activity that simultaneously targets many of the abnormalities that differentiate cancer cells and tumours from normal cells and tissues.
The pace of cancer immunotherapy clinical studies is such that they have outstripped our progress in understanding the underlying basic science. However, this situation has created the opportunity to combine emerging scientific and clinical insights in a synergistic fashion that will not only inform our knowledge of the basic cellular mechanisms of cancer immunity, but will also provide guidance for the identification of new targets, the conduct of future clinical trials and the crafting of a framework for making treatment decisions on a personalized basis14. This Review will synthesize what has been learned with relevance to each of these considerations to define the most important challenges and opportunities, as well as to evaluate the factors that contribute to the cancer–immune set point.
The tumour genome as a driver of cancer immunity
The immune response to cancer is dependent on T cells that are specific for cancer-associated antigens. The idea that T cells can recognize new epitopes (neoepitopes) generated by mutation or transcriptional aberrations in cancer originated in the 1980s from the work of Thierry Boon, Hans Schreiber and others, who identified the first mutant T-cell neoepitopes in mice15,16,17.
Perhaps owing to the difficulty of DNA sequencing at that time, interest in T-cell epitopes turned from mutated antigens to the cancer–testis antigens, which are expressed both in germline cells and in many cancers18,19. Well-studied examples include cancer/testis antigen 1 (also known as NY-ESO-1) and melanoma-associated antigen 3 (MAGE-A3). Cancer–testis antigens contain epitopes for both T cells that carry the CD4 antigen and those that carry CD8 that have been detected in people with cancer20,21,22. Similarly, differentiation antigens, including abundant melanosome-specific proteins such as glycoprotein 100 and tyrosinase, have also been found to generate T-cell epitopes in some people. However, the use of these antigens for therapeutic vaccination has not been successful so far23.
By contrast, results from mouse syngeneic tumour models demonstrate that point mutations can yield mutant antigens that prime T-cell responses to generate protective endogenous immunity or immunity in the setting of a therapeutic vaccine, achieved by the injection of synthetic peptides or messenger RNA24,25,26,27. The recognition of these mutant antigens by T cells is relatively inefficient, however. A study of the syngeneic tumour model MC38 found only 10% of nonsynonymous point mutations generated peptides that bound to major histocompatibility complex (MHC) class I molecules with high affinity; furthermore, only a fraction of these peptides were highly immunogenic when tested by vaccination27. Immunogenic peptides include peptides containing mutations that are exposed to the T-cell receptor or peptides with mutations that create new anchor residues that increase binding affinity for MHC class I molecules (Fig. 1). Although much of the current focus is on point mutations, frameshift mutations or insertion or deletion mutations may create new protein or peptide sequences called neoantigens that are even more immunogenic owing to their greater sequence divergence. It will be crucial to better understand the determinants of immunogenicity as, ultimately, these will determine whether a given neoantigen is recognized as foreign by the immune system.

The development of different types of mutations during the oncogenic process can lead to the generation of new protein or peptide sequences, which are referred to as neoantigens. These may be presented on the surface of cancer cells bound to MHC class I molecules, if they contain appropriate MHC class I binding motifs. T cells may recognize neoantigens if they are presented when bound to a MHC class I molecule and if the mutant amino acids project towards the T-cell antigen receptor (TCR). In the hypothetical examples shown here, a sequence of nine amino acids (ILQLMPFSV) acquires alterations (red) generated by various mutations. The peptide is then cleaved from the parental protein and becomes bound to an MHC class I molecule (using a human leukocyte antigen (HLA)-A201 motif, in this example). In the case of a non-immunogenic point mutation, the mutated peptide may bind poorly to the MHC class I molecule or might not contain mutant amino acids at the appropriate position. The mutated amino acids might also not be displayed outwards, towards the TCR (shown). In an immunogenic point mutation, the altered amino acid may enable binding of the mutated (and now immunogenic) peptide to an MHC class I molecule through the creation of an 'anchor' residue (top), or it may project towards the TCR (bottom). An insertion or deletion (indel) mutation can create similarly immunogenic peptides through the juxtaposition of two peptide sequences. And a frameshift mutation creates entirely foreign peptide sequences, which may also be immunogenic when the new peptide sequence binds to an MHC class I molecule and creates a mutant projected amino acid. X, any amino acid.
Mutant peptides that bind MHC class I or MHC class II molecules can generate protective immunity25,28,29,30, although the role of T cells that express CD4 in the anticancer immune response is still uncertain. Clearly, CD4-carrying T cells are important in helping to drive both the antibody response and that of cytotoxic CD8-expressing T cells, and they can produce IFN-γ, thereby contributing to an inflammatory environment that favours antitumour immunity. T cells that carry CD4 have also been reported to mediate cytotoxicity; indeed, some tumours such as melanoma can express MHC class II molecules, often on exposure to IFN-γ, and may be the direct targets of cytotoxic CD4-expressing populations.
Direct evidence that mutant epitopes are recognized by T cells in cancer in humans has been provided by studies in which the specificities of tumour-infiltrating lymphocytes were determined by large-scale screening. Several such reports in melanoma identified both CD4- and CD8-expressing T cells that were specific for mutant epitopes31,32,33. The adoptive transfer of antigen-specific tumour-infiltrating lymphocytes into cancer patients has been shown to correlate with tumour regression34,35,36,37,38.
Together, these results indicate that the main targets of protective anticancer T cells are the genetic alterations associated with all forms of cancer. Although this does not eliminate the possible contribution of other cancer-associated antigens to cancer immunity, it does lend credence to the concept that the large number of passenger mutations that occur in cancer form the most probable targets for T cells. A further class of cancer-associated neoantigen occurs in cancers that are characterized by a viral aetiology, most commonly human papillomavirus 16. Such viral antigens are foreign to the immune system and have proved to be good targets for therapeutic vaccination, especially in premalignant lesions of the genitourinary tract19. Tumour genomes may also contain and possibly reactivate endogenous viruses or transposable elements as a consequence of epigenetic alterations39. Because central tolerance has not been developed for these antigens, they might also prove to be targets of protective T cells that merit further investigation. As a driver of anticancer T-cell responses, the mutational neoepitope load of a given tumour must therefore be considered an important element of the cancer–immune set point.
The essential role of T-cell memory
Curative treatment of tumours can render individual mice refractory to subsequent challenge with the same — but not different — tumours, suggesting that the mice generate a memory response to tumour-associated antigens40. In further support of a role for memory T cells in antitumour responses, tumour-infiltrating lymphocytes that express CD4 or CD8 extracted from experimental tumour models typically have the features of memory T cells and can possess an activated or exhausted phenotype, expressing markers such as PD-1, T-cell immunoglobulin and mucin-domain containing protein 3 (TIM-3) and lymphocyte activation gene 3 (LAG-3).
The priming of T cells for the generation of effector T cells and memory T cells has been well studied in response to infectious agents, and it is probable that the same basic features also apply in the context of cancer. Naive T cells, which may be primed in tumour-draining lymph nodes or in tertiary lymphoid structures in solid tumours41, yield both effector and memory T cells that give rise to terminally differentiated effectors such as cytotoxic T cells (Fig. 2a), which may occur in the blood, lymphoid organs, tissues or tumours. As exposure to an antigen is prolonged, T cells upregulate activation markers, including negative regulators such as PD-1, which leads to the appearance of effector T cells with increasing degrees of functional exhaustion.

Evidence of an anticancer immune response may be detectable in several biological compartments, including the spleen, the lymphatic system, bone marrow, tumour-draining lymph nodes, the blood and tumours. a, The development of CD8-expressing populations of T cells, including effector T cells, memory T cells and exhausted T cells, is shown, with the expression of relevant proteins indicated for each. Naive CD8+ T cells generally reside in the lymph nodes and the spleen. After exposure to and activation by an antigen, short-term memory T cells can proliferate and differentiate into effector T cells, effector memory T cells, central memory T cells (not shown) and cytotoxic T cells. With chronic antigen exposure, effector T cells can become progressively exhausted; conceivably, only freshly exhausted cells that express relatively low amounts of PD-1 (PD-1med) are recoverable on treatment with anti-PD-L1/PD-1 therapies, whereas 'hyperexhausted' effector T cells that express high levels of PD-1 (PD-1high) as well as other markers of activation (for example, LAG-3, TIM-3 or TIGIT) may be unrecoverable. Hyperexhausted effector T cells may represent T cells that are committed by chronic TCR stimulation to a pathway of TCR-induced apoptosis. Anti-PD-L1/PD-1 treatment or treatment with inhibitors of the mitogen-activated protein kinase pathway (MEKi) may block or slow T-cell exhaustion by attenuating the strength of the TCR signal. EOMES, eomesodermin; TNF, tumour-necrosis factor. b, The lymph nodes, the blood and tumours represent the main compartments in which elements of the anticancer immune response can be detected. Biomarker sampling in these compartments must take into account the dynamic processes that are involved in cancer immunity, including the timing of the activation of anticancer T cells, the rate of migration of anticancer T cells from the lymph nodes to the blood (kmig), the rate of T-cell infiltration into tumours (kinf) and the rate of T-cell efflux from tumours into the blood (keff). The interrogation of immunity may be able to separate anticancer immunity (Δ2) from systemic immunity against non-cancer cells (Δ1), depending on the specific biomarker under investigation. Other factors that are important for biomarker interpretation include the change in tumour size with time (δvol/δt) and the rate of apoptosis of anticancer T cells (kapop).
Recent evidence, especially from the lymphocytic choriomeningitis virus mouse model of chronic virus infection, suggests that priming first yields a self-renewing population of short-term memory T cells. These cells are characterized by a high level of expression of the transcription factor T-bet and by a low level of expression of eomesodermin (EOMES) and PD-1 (refs 42 and 43).
In mouse models of cancer, a T-cell population similar to the short-term memory T cells has also been observed in tumour-bearing animals that were treated with inhibitors of the mitogen-activated protein (MAP) kinase pathway (known as MEKi)44. Although, as expected, these inhibitors blocked the priming of naive T cells, there was a transient accumulation of tumour-infiltrating lymphocytes expressing CD4 or CD8 (ref. 45) that exhibited lower levels of PD-1 as well as elevated levels of T-bet and low levels of EOMES, indicating that these cells were less exhausted than T cells from control tumours44. Although PD-L1/PD-1 blockade has also been shown to restore the functionality of exhausted T cells46, evidence suggests that less exhausted populations may be the target population. Despite not yet being demonstrated in people with cancer, the proposed self-renewing population of short-term memory T cells that express high levels of T-bet and low levels of EOMES or the population of CD8-, CXCR5- and TCF1-expressing short-term memory T cells described in mice infected with lymphocytic choriomeningitis virus may selectively proliferate after PD-1 blockade, thereby expanding the pool of antigen-specific T cells47,48,49.
Why is this an important consideration? As well as the need to define anatomic sites of PD-L1/PD-1 inhibition, the fact remains that even when individuals respond, the tumour burden often fails to disappear entirely. Although this may reflect the development of alternative mechanisms of immunosuppression50,51, or the evolution of the tumour to lose immunodominant epitopes38 or to acquire mutations that facilitate resistance50, a sustained partial response might also suggest that a new equilibrium may have been reached between the tumour and the greater number of antitumour T cells that are produced52,53. Therefore, even after successful anti-PD-L1/PD-1 therapy, a putative self-renewing or expanding memory T cell compartment may be too small to keep pace with tumour growth. In such instances, the continued priming of naive T cells may be needed to replenish and maintain the antitumour response. In support of this, the blockage of priming by long-term MEK inhibition in mice with tumours led to a loss of tumour-infiltrating lymphocytes and memory T cells44. In people with cancer, greater clearance of tumours has been observed when anti-PD-1 therapy is combined with anti-CTLA4 therapy54, possibly because of an increase the total number of T cells caused by the removal of a checkpoint for T-cell proliferation and priming.
Tumour-infiltrating lymphocytes from humans can also have the features of memory T cells55,56,57,58. One study found that a high frequency of CD8-carrying tumour-infiltrating lymphocytes were of the effector memory phenotype, which lack CD62L (L-selectin) but express the RO isoform of the antigen CD45, and also exhibited high levels of PD-1 and other markers of activated or exhausted T cells55. The fact that tumour-infiltrating lymphocytes extracted from humans can be expanded in vitro and re-administered with potential clinical benefit34,35,36,37 further indicates that these cells were derived from memory T cells.
Which factors might limit the production of memory T cells? Even if sufficient epitopes exist and are loaded onto MHC molecules, the T-cell response itself may be insufficient to mediate tumour regression. The manner in which tumour cells die probably also affects the type of T-cell response that is generated. This is because some forms of cell death seem to be more immunogenic than others59,60. Understanding this issue will be crucial, as the ability of conventional or targeted therapies to generate one form or another of immunogenic cell death may facilitate the design of effective combination therapies61.
When a response to anti-PD-L1/PD-1 antibodies occurs, it most often reflects some level of prior T-cell immunity. This is consistent with the observed timing of increased numbers of T cells expressing CD8, the MHC class II molecule human leukocyte antigen (HLA)-DR and proliferation marker Ki-67 in the blood of cancer patients 1 week after beginning treatment with a PD-L1 inhibitory antibody62. However, neither these data nor the extent of the clinical response are necessarily informative about the breadth or depth of the anticancer T-cell response, which has yet to be measured directly. Indeed, several factors contribute to the development of this response. Potential rate-limiting steps include the initial priming and expansion of T cells, their conversion to memory and effector T cells and the fate and survival of effector T cells after they enter the tumour, where the abundance of antigens and immunosuppressive factors can trigger T-cell exhaustion and death.
Also of importance are the rates of trafficking of antigen-specific T cells from lymph nodes to tumours through the bloodstream (Fig. 2b). The rate constants that govern T-cell migration clearly have a crucial role in controlling the migration of tumour-infiltrating lymphocytes into certain types of tumour. Determining these values in people will be a challenge.
Correlates of the response to immunotherapy
As effective as immunotherapy can be, only a minority of people exhibit dramatic responses, with the frequency of rapid tumour shrinkage from single-agent anti-PD-L1/PD-1 antibodies ranging from 10–40%, depending on the individual's indication12. Responses to other single-agent immunotherapeutics such as anti-CTLA4 antibodies or interleukin(IL)-2 are even lower63,64. A variety of factors contribute to determining whether a response occurs. However, before the underlying mechanisms can be considered, it is important to define the associated phenotypes that have been revealed by clinical studies. By examining histological sections of tumour biopsies collected from patients before they received therapy, it is possible to distinguish three basic immune profiles that correlate with a person's response to anti-PD-L1/PD-1 therapy14,51,62.
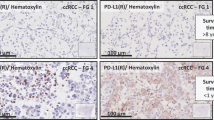
The first profile, the immune-inflamed phenotype (Fig. 3), is characterized by the presence in the tumour parenchyma of both CD4- and CD8-expressing T cells, often accompanied by myeloid cells and monocytic cells; the immune cells are positioned in proximity to the tumour cells62,65,66,67,68,69,70,71,72. Samples from inflamed tumours may exhibit staining for PD-L1 on infiltrating immune cells and, in some cases, tumour cells62,69,70,73,74. Many proinflammatory and effector cytokines can also be detected by mRNA analysis in these sections of tumours62,69,70,72. This profile suggests the presence of a pre-existing antitumour immune response that was arrested — probably by immunosuppression in the tumour bed. Indeed, clinical responses to anti-PD-L1/PD-1 therapy occur most often in patients with inflamed tumours62,67,70,75. However, a response is not assured in these individuals, which indicates that immune-cell infiltration is necessary but insufficient for inducing a response.

Anticancer immunity in humans can be segregated into three main phenotypes: the immune-desert phenotype (brown), the immune–excluded phenotype (blue) and the inflamed phenotype (red). Each is associated with specific underlying biological mechanisms that may prevent the host's immune response from eradicating the cancer. A tumour that is characterized as an immune desert can be the result of immunological ignorance, the induction of tolerance or a lack of appropriate T-cell priming or activation. Immune-excluded tumours may reflect a specific chemokine state, the presence of particular vascular factors or barriers, or specific stromal-based inhibition. Inflamed tumours can demonstrate infiltration by a number of subtypes of immune cells, including immune-inhibitory regulatory T cells, myeloid-derived suppressor cells, suppressor B cells and cancer-associated fibroblasts. Tumour-infiltrating lymphocytes that express CD8 may also demonstrate a dysfunctional state such as hyperexhaustion. Tumour cells in inflamed tumours can also express inhibitory factors, downregulating MHC class I molecule expression or other pathways that de-sensitize them to anticancer immunity. APC, antigen-presenting cell; B2M, β-2-microglobulin; IDO, indoleamine 2,3-dioxygenase; LN, lymph node; TAP, transporter associated with antigen processing; TDO, tryptophan 2,3-dioxygenase; TGF, transforming growth factor; VEGF, vascular endothelial growth factor.
The second profile is the immune-excluded phenotype, which is also characterized by the presence of abundant immune cells. However, the immune cells do not penetrate the parenchyma of these tumours but instead are retained in the stroma that surrounds nests of tumour cells51,62,76,77. The stroma may be limited to the tumour capsule or might penetrate the tumour itself, making it seem that the immune cells are actually inside the tumour. After treatment with anti-PD-L1/PD-1 agents, stroma-associated T cells can show evidence of activation and proliferation but not infiltration, and clinical responses are uncommon. These features suggest that a pre-existing antitumour response might have been present but was rendered ineffective by a block in tumour penetration through the stroma or by the retention of immune cells in the stroma. T-cell migration through the tumour stroma is therefore the rate-limiting step in the cancer–immunity cycle for this phenotype.
The third profile, the immune-desert phenotype, is characterized by a paucity of T cells in either the parenchyma or the stroma of the tumour14,51,62,65. Although myeloid cells may be present, the general feature of this profile is the presence of a non-inflamed tumour microenvironment with few or no CD8-carrying T cells. Unsurprisingly, such tumours rarely respond to anti-PD-L1/PD-1 therapy62. This phenotype probably reflects the absence of pre-existing antitumour immunity, which suggests that the generation of tumour-specific T cells is the rate-limiting step. The immune-desert phenotype and the immune-excluded phenotype can both be considered as non-inflamed tumours.
Inflamed versus non-inflamed tumours
What is the basis for the three immune profiles observed in tumours? To a first approximation, differences between the profiles can be ascribed to whether tumours harbour an inflammatory microenvironment, which can reflect variations in a number of cellular and other factors (Fig. 4). The degree of inflammation can be gauged by the cellular content of the tumour — for example, the presence of immune cells, either in the parenchyma or at the invasive margin of the tumour78,79. Inflamed tumours also contain proinflammatory cytokines that should provide a more favourable environment for T-cell activation and expansion, including type I and type II IFNs, IL-12, IL-23, IL-1β, tumour-necrosis factor (TNF)-α and IL-2. However, it is unclear whether the presence of these cytokines is the cause or consequence of the cellular influx. The production of tropic chemokines by lymphocytes and myeloid cells is therefore likely to be an important feature of inflamed tumours.

Anticancer immunity is subject to a multitude of factors that contribute to the generation of activated T-cell immunity or tolerance. Immunity in humans can be influenced by the genetics of an individual, age, the microbiota, the presence of infection, exposure to sunlight and the intake of immune-modifying drugs. These factors are distributed in a continuum (red–blue bars) and act to determine the set point by directly or indirectly controlling the expression of tolerogenic (blue circles) or immunogenic (red circles) cytokines and cell types. The bell curve represents the population distribution of variability in these factors, which is related to the likelihood that a given person's tumour will adopt a more inflamed or a non-inflamed phenotype, effectively defining the cancer–immune set point. Although individuals may be found at the extremes, it is probable that only slight differences exist in the balance of tolerogenic factors versus immunogenic factors in most people, suggesting that stochastic forces may play a part in determining whether a given person (or a particular tumour) responds or not to immunotherapy. CAFs, cancer-associated fibroblasts; n, number of people; TLR, Toll-like receptor.
Non-inflamed tumours generally express cytokines that are associated with immune suppression or tolerance. They can also contain cell types associated with immune suppression or tissue homeostasis. As well as regulatory T cells, these cells include the lesser characterized populations of myeloid-derived suppressor cells (for example, immature granulocytes) and tumour-associated macrophages, which are unactivated and often called M2 macrophages. However, regulatory T cells are not associated uniquely with non-inflamed tumours as they typically accompany effector T cells into inflammatory sites and are important for maintaining immune homeostasis, even in the presence of an active antitumour immune response80,81.
Predicting response
The immune-inflamed phenotype correlates generally with higher response rates to anti-PD-L1/PD-1 therapy51,62,67,69,70,71, which suggests that biomarkers could be used as predictive tools. Most attention has been paid to PD-L1, which is thought to reflect the activity of effector T cells because it can be adaptively expressed by most cell types following exposure to IFN-γ6,82. In an increasingly large clinical data set, it is becoming clear that the expression of PD-L1 in pretreatment biopsies facilitates enrichment with people who are most likely to respond to antibodies against PD-L1 or PD-1 (refs 62, 69, 70, 73, 75, 83 and 84). PD-L1 expression also correlates strongly with various markers of active cellular immunity, including IFN-γ, granzymes and CXCL9 and CXCL10. The presence of these biomarkers or others such as T cells that carry the CD3 antigen or tumour mutational burden may also enrich for responders1,2,67,85. When used in combination with PD-L1 expression, these biomarkers may enhance predictive power86. Clinically, it will be important to select individuals who are most likely to respond to anti-PD-L1/PD-1 therapies given as single agents rather than those who might require combination therapy14,51, which could add considerable toxicity54. This therapeutic approach, which combines a set of specific biomarkers with a selection of potential therapeutic options, is referred to as personalized cancer immunotherapy. Scientifically, the identification of predictive biomarkers will greatly expand our understanding of the mechanisms of cancer immunity, providing information on the immune context in individuals.
An important consideration when using PD-L1 and other biomarkers to predict response to treatment is that the degree of inflammation can vary widely and will probably reflect a variety of genetic and environmental factors that may change with time. Their utility could therefore be confounded by temporal changes in expression and the timing of biopsy collection. It is assumed that archival specimens will be less accurate because the people from whom they were taken may have undergone several lines of therapy since the biopsies were performed. However, an analysis in 2015 found that the frequency and intensity of PD-L1 immunohistochemistry signals were similar in fresh versus archival specimens and primary versus metastatic lesions in the same individuals87. These data suggest that tumours may have characteristic immune profiles that are at least partially preserved in time and location. Despite the use of treatments that may alter such signatures, the tumour microenvironment may return to a baseline profile that is controlled by a variety of genetic or environmental factors that characterize a given person or tumour88. Another consideration in the study of predictive biomarkers is the potential variation in the immune phenotype of primary and metastatic lesions. In fact, studies in renal cell carcinoma and non-small cell lung cancer have found differences in the density of CD8-expressing tumour-infiltrating lymphocytes in primary and metastatic lesions89,90.
Elements that determine immune profiles
The factors that determine the baseline immune profile or cancer–immune set point of a given tumour represent a key unknown, but they are likely to include variations in tumour genetics, germline genetics, age, the microbiome, the presence of infectious agents, exposure to sunlight and pharmacological agents (Fig. 4). Even for the same indications, the immunological profiles of tumours can vary from person to person. Although three basic immune phenotypes can be distinguished (as discussed previously), there is a wide continuum of cytokines, chemokines and immune and non-immune tumour-associated cell types that determine whether sufficient inflammation is present to favour the development of an effective antitumour immune response following immunotherapy. A presumptive population distribution of patients is depicted as a bell curve in Fig. 4. Small variations in factors — rather than dramatic alterations — may be sufficient to tip the balance between tolerance and immunity. Together, these factors act by promoting the predominance, even if subtle, of various inflammatory states, and they may also be associated with a particular immune profile and degree of clinical response. For people who fall near to the top of the distribution curve, where the extent of variation is low, the response (or lack of response) to immunotherapy may be influenced strongly by stochastic considerations. Not all people with inflamed, PD-L1-expressing tumours are responsive to PD-L1/PD-1 blockade. It is therefore reasonable to presume that the ability of anti-PD-L1/PD-1 therapies to promote antitumour immunity may be stochastic, with the probability of a response reflecting the immune status, or immune set point, that is associated with each tumour.
How the factors that influence the balance between tolerance and immunity combine to affect the cancer–immune set point remains to be elucidated, and this will probably be addressed only by large-scale, quantitative data sets that score a level of benefit to immunotherapy as a function of the immunomodulatory variables present. Figure 5 maps how the factors that are proposed to establish a person's immune profile (tumour genetics, germline genetics, the microbiome, the environment and the presence of certain pharmacological agents) can be arranged in relation to the seven steps of the cancer–immunity cycle. It should be noted that this representation is only a partial list and that factors will be added, removed or modified in the future.

A map of cancer immunity showing the factors that affect the cancer–immune set point. The factors are placed on rings that denote their type, and each factor is also placed in the step of the cancer-immunity cycle in which they mainly act. For example, variations in HLA type reflect host genetics and are of greatest importance for T cell activation. Additional factors are being discovered rapidly. ARNTL, aryl hydrocarbon receptor nuclear translocator–like protein 1; ATG16L, autophagy-related protein 16; FcγRIII, Fc γ receptor III; HMGCR, HMG-CoA reductase; JAK/STAT, Janus kinase–signal transducers and activators of transcription; LOX, lysyl oxidase; NOD, nucleotide-binding oligomerization domain-containing protein; NSAIDs, non-steroidal anti-inflammatory drugs; RANKL; receptor activator of NF-κB ligand; ROS, reactive oxygen species.
Tumour genetics and epigenetics
As described previously, it is probable that the mutation burden of a given tumour will contribute to its immune profile. Perhaps the clearest association is demonstrated by the overall mutational burden. The greater the number of mutations in a given tumour, the more probable it is that some of the mutations will be immunogenic, providing targets for T-cell attack1,85,86,91. Mutations that arise early in oncogenesis and are shared by almost all of the cancer cells in an individual (known as truncal mutations) may generate more effective anticancer T-cell responses than mutations that arise later on and are limited to only a subpopulation of cancer cells (known as branch mutations)2.
Although mutations are generally thought to promote T-cell-mediated immunity, some — especially, cancer-associated driver mutations — may act to attenuate immune responses. For example, mutations in the genes KRAS and BRAF or other mutational activations of the MAP kinase pathway will decrease the transcription of MHC class I molecules as well as the expression of other genes encoding molecules that are essential for peptide loading92,93,94,95. These alterations might reduce inflammation in tumours and the killing of tumour cells by decreasing the density of T-cell ligands on tumour cells.
The systematic analysis of tumour genomes should reveal further information about the relationship between tumour genetics and the tumour microenvironment. One such study demonstrated that recurring mutations in genes that control the expression of MHC class I products or cell death in tumours (such as caspase 8) affect the degree of inflammation in a tumour88. The study also found that tumours can selectively increase, through amplification or enhanced transcription, the expression of genes that encode proteins associated with immunosuppression, including PD-L1, the arachidonate lipoxygenases and IDO-1 and IDO-2.
Changes in gene expression in tumours owing to epigenetic modifications and the expression of microRNAs probably contribute directly to determining the immune microenvironment and immunogenicity of a tumour. Cytokine expression during T-cell development is regulated by epigenetic alterations to both DNA and chromatin96. Cancer can also be accompanied by epigenetic changes, which makes it probable that such changes will influence cytokine profiles that modulate the immune microenvironment. In fact, DNA methylation in lung-cancer cells has been shown to reduce the expression of IL-1β97. And PD-L1 expression can be modulated by microRNAs, with miR-200 (a repressor of epithelial-to-mesenchymal transition) and possibly others decreasing its expression98. Methylation of the promoter for the gene PD-L1 itself also seems to repress PD-L1 expression; demethylation can result in constitutive expression in tumours, especially non-small cell lung cancer99.
Another influence on the immune profile of a tumour that has an epigenetic mechanism involves the tissue of origin of the tumour. Colorectal cancer tumours commonly express elevated levels of transforming growth factor (TGF)-β100. Presumably, this reflects the importance of the TGF-β pathway in intestinal biology and, especially, its role in maintaining tolerance to the gut microbiota by favouring the development of regulatory T cells101. Elevated expression of TGF-β may also contribute to the development of abundant stromal elements in these tumours that can restrict the access of immune cells to the tumour parenchyma, as has been demonstrated in pancreatic cancer102. Although other factors also contribute, it is interesting to note that pancreatic cancer and most forms of colorectal cancer (except for the mutationally rich microsatellite-instability-high subgroup85) respond poorly to single-agent inhibition of PD-L1/PD-1 (refs 62, 83 and 103,104,105).
Host genetics
People vary in their response to infectious stimuli and they also exhibit different susceptibilities to chronic inflammatory and autoimmune disorders. This is mostly because of variation in the population in several immune-response genes106,107,108. It is probable that the same variation also contributes to the inherent immune profile of a tumour and to the immune set point of a person with cancer. One such example relates to polymorphisms in the gene TLR4 in breast cancer, which are thought to affect the priming of antigen-specific T cells. People with a TLR4 germline loss-of-function allele were found to respond less well to both radiotherapy and chemotherapy, suggesting the presence of an impaired immune response. However, it is unknown whether this allele also contributes to an alteration in the immune profile of pretreatment tumours. Polymorphisms at other immune-related loci (for example, genes that encode TNF-α, NF-κB, JAK/STAT proteins, FcγRIII, NOD2, autophagy related protein 16 (ATG16) and inflammasome pathway proteins) may also be associated with a diminished response to therapy in various indications and might influence the immune profile of pretreatment tumours.
Microbiome
Factors that are extrinsic to the tumour or host genomes may also affect the immune profile of tumours. Chief among these is the gut microbiome, which has an important role not only in influencing the initiation of some cancers, but also in the response to chemotherapy and immunotherapy109,110,111,112,113. Goldszmid, Zitvogel and their colleagues demonstrated that mice bearing subcutaneous syngeneic tumours do not respond to chemotherapy if sterilized by prior treatment with antibiotics or when raised in germ-free conditions110,113. The effect was attributed to the ability of commensal bacteria to activate the innate immune system of the host following chemotherapy, possibly by causing dysbiosis and penetration of commensal bacteria into the gut lamina propria.
Subsequent work established an even clearer link between T-cell responses and an intact microbiota111,112. Faecal transfer or co-housing experiments in mice demonstrated that defined species of gut bacteria enabled antitumour responses after treatment with anti-PD-L1/PD-1 or anti-CTLA4 therapies. Furthermore, the gut microbiota even influenced spontaneous antitumour responses, which correlated with the degree of T-cell infiltration into tumours before any therapy had been administered111.
Under the assumption that these findings also apply to humans, the degree to which a person's gut microbiome promotes antitumour immunity may be an important determining factor of both the baseline immune profile of a tumour and the cancer–immune set point of an individual. Indeed, resistance to drug-induced colitis (an adverse side effect that is associated with the anti-CTLA4 antibody ipilimumab) was found to be related to the presence of specific classes of bacteria114.
Environmental and other factors that influence immunity
Immunity in humans can also be affected by environmental factors. These include the presence of infectious agents, diet and the intake of pharmaceuticals. Agents that lower cholesterol have been associated with altered immune responses. For example, chronic statin therapy has been associated with a reduced response to the influenza vaccine in elderly people115. Intriguingly, even exposure to sunlight may influence immunity, which is referred to as photoimmunity. Human immune responses during periods of decreased exposure to sunlight are associated with enhanced levels of IL-6 and C-reactive protein, which are linked to an increased propensity for autoimmunity116. Conceivably, conditions of low sunlight may correlate with a more inflammatory systemic environment, leading to better responses to cancer immunotherapy. Although not strictly an environmental factor, alterations in immune activity as a function of age may also be an important variable in determining the immune response117,118.
The importance of the cancer–immune set point
The cancer–immune set point is the threshold that must be overcome to generate effective cancer immunity. The set point can be understood as a balance between the stimulatory factors (Fstim) minus the inhibitory factors (Finhib), which together must be equal to or greater than 1, over the summation of all T-cell antigen receptor (TCR) signals for tumour antigens. The cancer–immune set point is shown here:

The set point is defined by the summation of the frequency of peptide–MHC–TCR interactions and TCR signalling in all anticancer CD8+ T-cell clones (mainly, the TCR affinity for the antigen–MHC class I complex) against antigens present in the cancer cells, including neoantigens and cancer-associated antigens, and the endogenous balance of the positive and negative immune regulators that are inherent to each host or patient. This can be further influenced by other elements of immunity, including tumour-derived immunomodulatory components, as well as by exogenous factors such as infection and exposure to pharmacological agents. A given patient with cancer may have a low set point, making it easier to generate an anticancer immune response, or a high set point, which makes it more difficult. The aim of immunotherapy is to increase Fstim, decrease Finhib or increase TCR signalling to drive progression of the cancer-immunity cycle. These values are difficult to quantify with current techniques but represent a useful theoretical construct.
It is probable that the cancer–immune set point of a particular person is already determined by the time of clinical presentation, driven by the inherent immunogenicity of the tumour and by the responsiveness of the individual's immune system. Although it is reasonable to assume that various lines of cancer therapy or changes in environmental factors might alter Fstim and Finhib, such changes might only be transient. Often, the set point that is identified using pretreatment biopsies is similar to the set point determined by biomarker profiling from biopsies taken on progression after therapy87. Likewise, despite the continued accumulation of mutations in a tumour as a function of time, primary and metastatic lesions can exhibit similar immune profiles. The features that determine the set point may therefore reflect genetic factors that are specific to a given tumour, the genetics of the person with cancer, or the extent to which antitumour immunity had developed initially. Conceivably, immunotherapy may work as a consequence of either its direct effect on Fstim and Finhib (that is, by assisting the completion of a single revolution of the cancer-immunity cycle) or its ability to alter the set point (for example, by propagating the cancer-immunity cycle, which enhances the cancer-specific T-cell response).
Although largely conceptual, the idea of a set point provides a framework to help organize the torrent of clinical and biomarker data that will emerge over the coming months and years. The number of targets that could prove effective for cancer immunotherapy is great; the number of potential combinations of therapeutic agents that are directed against these targets (or combinations of such agents with conventional standard-of-care agents) is even greater (Supplementary Fig. 1). The development of some cancer therapies may be largely empirical, but it can be guided by considering, even in general terms, the elements that comprise cancer immunity.
References
Rizvi, N. A. et al. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 348, 124–128 (2015). A landmark demonstration that the abundance of mutations in tumours is directly correlated with the response to immunotherapy, which strongly implies that mutational neoantigens are important targets for T cells in cancer immunity.
McGranahan, N. et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 351, 1463–1469 (2016).
Snyder, A. et al. Genetic basis for clinical response to CTLA-4 blockade in melanoma. N. Engl. J. Med. 371, 2189–2199 (2014).
Chen, D. S., Irving, B. A. & Hodi, F. S. Molecular pathways: next-generation immunotherapy — inhibiting programmed death-ligand 1 and programmed death-1. Clin. Cancer Res. 18, 6580–6587 (2012).
Topalian, S. L., Drake, C. G. & Pardoll, D. M. Immune checkpoint blockade: a common denominator approach to cancer therapy. Cancer Cell 27, 450–461 (2015).
Mellman, I., Coukos, G. & Dranoff, G. Cancer immunotherapy comes of age. Nature 480, 480–489 (2011).
Sharma, P. & Allison, J. P. Immune checkpoint targeting in cancer therapy: toward combination strategies with curative potential. Cell 161, 205–214 (2015).
Leach, D. R., Krummel, M. F. & Allison, J. P. Enhancement of antitumor immunity by CTLA-4 blockade. Science 271, 1734–1736 (1996).
Dong, H. et al. Tumor-associated B7-H1 promotes T-cell apoptosis: a potential mechanism of immune evasion. Nature Med. 8, 793–800 (2002).
Iwai, Y. et al. Involvement of PD-L1 on tumor cells in the escape from host immune system and tumor immunotherapy by PD-L1 blockade. Proc. Natl Acad. Sci. USA 99, 12293–12297 (2002).
Blank, C. et al. PD-L1/B7H-1 inhibits the effector phase of tumor rejection by T cell receptor (TCR) transgenic CD8+ T cells. Cancer Res. 64, 1140–1145 (2004).
Zou, W., Wolchok, J. D. & Chen, L. PD-L1 (B7-H1) and PD-1 pathway blockade for cancer therapy: mechanisms, response biomarkers, and combinations. Sci. Transl. Med. 8, 328rv4 (2016).
Chen, D. S. & Mellman, I. Oncology meets immunology: the cancer-immunity cycle. Immunity 39, 1–10 (2013). A review article that lays out the series of stepwise events that must occur to generate and to sustain anticancer T-cell-mediated immunity.
Kim, J. M. & Chen, D. S. Immune escape to PD-L1/PD-1 blockade: seven steps to success (or failure). Ann. Oncol. 27, 1492–1504 (2016).
De Plaen, E. et al. Immunogenic (tum−) variants of mouse tumor P815: cloning of the gene of tum− antigen P91A and identification of the tum− mutation. Proc. Natl Acad. Sci. USA 85, 2274–2278 (1988).
Stauss, H. J., Van Waes, C., Fink, M. A., Starr, B. & Schreiber, H. Identification of a unique tumor antigen as rejection antigen by molecular cloning and gene transfer. J. Exp. Med. 164, 1516–1530 (1986).
Coulie, P. G., Van den Eynde, B. J., van der Bruggen, P. & Boon, T. Tumour antigens recognized by T lymphocytes: at the core of cancer immunotherapy. Nature Rev. Cancer 14, 135–146 (2014).
Simpson, A. J., Caballero, O. L., Jungbluth, A., Chen, Y. T. & Old, L. J. Cancer/testis antigens, gametogenesis and cancer. Nature Rev. Cancer 5, 615–625 (2005).
Melief, C. J., van Hall, T., Arens, R., Ossendorp, F. & van der Burg, S. H. Therapeutic cancer vaccines. J. Clin. Invest. 125, 3401–3412 (2015).
Jäger, E. et al. Identification of NY-ESO-1 epitopes presented by human histocompatibility antigen (HLA)-DRB4*0101–0103 and recognized by CD4+ T lymphocytes of patients with NY-ESO-1-expressing melanoma. J. Exp. Med. 191, 625–630 (2000).
Jäger, E. et al. Simultaneous humoral and cellular immune response against cancer–testis antigen NY-ESO-1: definition of human histocompatibility leukocyte antigen (HLA)-A2-binding peptide epitopes. J. Exp. Med. 187, 265–270 (1998).
Tanzarella, S. et al. Identification of a promiscuous T-cell epitope encoded by multiple members of the MAGE family. Cancer Res. 59, 2668–2674 (1999).
Melero, I. et al. Therapeutic vaccines for cancer: an overview of clinical trials. Nature Rev. Clin. Oncol. 11, 509–524 (2014).
Ikeda, H. et al. Mutated mitogen-activated protein kinase: a tumor rejection antigen of mouse sarcoma. Proc. Natl Acad. Sci. USA 94, 6375–6379 (1997).
Kreiter, S. et al. Mutant MHC class II epitopes drive therapeutic immune responses to cancer. Nature 520, 692–696 (2015).
Gubin, M. M. et al. Checkpoint blockade cancer immunotherapy targets tumour-specific mutant antigens. Nature 515, 577–581 (2014). This paper and ref. 27 show definitively (in mice) that mutational neoantigens are, indeed, important therapeutic targets in cancer and that it is possible to predict which mutations are likely to be immunogenic, enabling the design of neoantigen vaccines that can be used in a therapeutic setting.
Yadav, M. et al. Predicting immunogenic tumour mutations by combining mass spectrometry and exome sequencing. Nature 515, 572–576 (2014).
Castle, J. C. et al. Exploiting the mutanome for tumor vaccination. Cancer Res. 72, 1081–1091 (2012).
Tran, E. et al. Cancer immunotherapy based on mutation-specific CD4+ T cells in a patient with epithelial cancer. Science 344, 641–645 (2014). This paper shows that adoptive T-cell therapy using T cells specific for a single mutant neoantigen can lead to evidence of therapeutic benefit.
Lu, Y. C. et al. Mutated PPP1R3B is recognized by T cells used to treat a melanoma patient who experienced a durable complete tumor regression. J. Immunol. 190, 6034–6042 (2013).
van Rooij, N. et al. Tumor exome analysis reveals neoantigen-specific T-cell reactivity in an ipilimumab-responsive melanoma. J. Clin. Oncol. 31, e439–e442 (2013).
Robbins, P. F. et al. Mining exomic sequencing data to identify mutated antigens recognized by adoptively transferred tumor-reactive T cells. Nature Med. 19, 747–752 (2013).
Linnemann, C. et al. High-throughput epitope discovery reveals frequent recognition of neo-antigens by CD4+ T cells in human melanoma. Nature Med. 21, 81–85 (2015).
Dudley, M. E. et al. Cancer regression and autoimmunity in patients after clonal repopulation with antitumor lymphocytes. Science 298, 850–854 (2002).
Dudley, M. E. et al. Adoptive cell therapy for patients with metastatic melanoma: evaluation of intensive myeloablative chemoradiation preparative regimens. J. Clin. Oncol. 26, 5233–5239 (2008).
Besser, M. J. et al. Clinical responses in a phase II study using adoptive transfer of short-term cultured tumor infiltration lymphocytes in metastatic melanoma patients. Clin. Cancer Res. 16, 2646–2655 (2010).
Rosenberg, S. A. et al. Durable complete responses in heavily pretreated patients with metastatic melanoma using T-cell transfer immunotherapy. Clin. Cancer Res. 17, 4550–4557 (2011).
Verdegaal, E. M. et al. Neoantigen landscape dynamics during human melanoma-T cell interactions. Nature 536, 91–95 (2016).
Sadikovic, B., Al-Romaih, K., Squire, J. A. & Zielenska, M. Cause and consequences of genetic and epigenetic alterations in human cancer. Curr. Genomics 9, 394–408 (2008).
Srivastava, P. K. & Old, L. J. Individually distinct transplantation antigens of chemically induced mouse tumors. Immunol. Today 9, 78–83 (1988).
Dieu-Nosjean, M. C. et al. Tertiary lymphoid structures, drivers of the anti-tumor responses in human cancers. Immunol. Rev. 271, 260–275 (2016).
Angelosanto, J. M., Blackburn, S. D., Crawford, A. & Wherry, E. J. Progressive loss of memory T cell potential and commitment to exhaustion during chronic viral infection. J. Virol. 86, 8161–8170 (2012).
Paley, M. A. et al. Progenitor and terminal subsets of CD8+ T cells cooperate to contain chronic viral infection. Science 338, 1220–1225 (2012).
Ebert, P. J. et al. MAP kinase inhibition promotes T cell and anti-tumor activity in combination with PD-L1 checkpoint blockade. Immunity 44, 609–621 (2016). A demonstration that the MAP kinase pathway is required for T-cell priming but dispensable for T-cell effector activities; this paper also shows that by inhibiting TCR signalling through the MAP kinase pathway, MEKi can also slow the process of chronic TCR signalling, which leads to T-cell exhaustion and apoptosis.
Liu, L. et al. The BRAF and MEK inhibitors dabrafenib and trametinib: effects on immune function and in combination with immunomodulatory antibodies targeting PD-1, PD-L1, and CTLA-4. Clin. Cancer Res. 21, 1639–1651 (2015).
Barber, D. L. et al. Restoring function in exhausted CD8 T cells during chronic viral infection. Nature 439, 682–687 (2006).
Im, S. J. et al. Defining CD8+ T cells that provide the proliferative burst after PD-1 therapy. Nature 537, 417–421 (2016). Together with refs 48 and 49, this paper provides evidence that inhibiting the interaction between PD-L1 and PD-1 causes the proliferation of a population of T cells with low levels of PD-1 expression, rather than a reversal of the exhaustion of T cells with high levels of PD-1 expression.
Leong, Y. A. et al. CXCR5+ follicular cytotoxic T cells control viral infection in B cell follicles. Nature Immunol. 17, 1187–1196 (2016).
He, R. et al. Follicular CXCR5-expressing CD8+ T cells curtail chronic viral infection. Nature 537, 412–428 (2016).
Zaretsky, J. M. et al. Mutations associated with acquired resistance to PD-1 blockade in melanoma. N. Engl. J. Med. 375, 819–829 (2016).
Hegde, P. S., Karanikas, V. & Evers, S. The where, the when, and the how of immune monitoring for cancer immunotherapies in the era of checkpoint inhibition. Clin. Cancer Res. 22, 1865–1874 (2016).
Vesely, M. D. & Schreiber, R. D. Cancer immunoediting: antigens, mechanisms, and implications to cancer immunotherapy. Ann. NY Acad. Sci. 1284, 1–5 (2013).
Koebel, C. M. et al. Adaptive immunity maintains occult cancer in an equilibrium state. Nature 450, 903–907 (2007).
Larkin, J. et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Engl. J. Med. 373, 23–34 (2015).
Gros, A. et al. PD-1 identifies the patient-specific CD8+ tumor-reactive repertoire infiltrating human tumors. J. Clin. Invest. 124, 2246–2259 (2014).
Fang, L. et al. The immune cell infiltrate populating meningiomas is composed of mature, antigen-experienced T and B cells. Neuro. Oncol. 15, 1479–1490 (2013).
Zhou, J., Nagarkatti, P., Zhong, Y. & Nagarkatti, M. Characterization of T-cell memory phenotype after in vitro expansion of tumor-infiltrating lymphocytes from melanoma patients. Anticancer Res. 31, 4099–4109 (2011).
Wang, Q. J., Hanada, K., Robbins, P. F., Li, Y. F. & Yang, J. C. Distinctive features of the differentiated phenotype and infiltration of tumor-reactive lymphocytes in clear cell renal cell carcinoma. Cancer Res. 72, 6119–6129 (2012).
Inoue, H. & Tani, K. Multimodal immunogenic cancer cell death as a consequence of anticancer cytotoxic treatments. Cell Death Differ. 21, 39–49 (2014).
Yatim, N. et al. RIPK1 and NF-κB signaling in dying cells determines cross-priming of CD8+ T cells. Science 350, 328–334 (2015).
Galluzzi, L., Buque, A., Kepp, O., Zitvogel, L. & Kroemer, G. Immunological effects of conventional chemotherapy and targeted anticancer agents. Cancer Cell 28, 690–714 (2015).
Herbst, R. S. et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature 515, 563–567 (2014). A compilation of biomarker results from a series of people with cancer who were treated with the anti-PD-L1 antibody atezolizumab; this was the first study to clearly document that the expression of PD-L1 in tumours enriches for people who will respond to therapy, and that responders exhibit an influx of canonically activated T cells.
Hodi, F. S. et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 363, 711–723 (2010).
Rosenberg, S. A. IL-2: the first effective immunotherapy for human cancer. J. Immunol. 192, 5451–5458 (2014).
Gajewski, T. F. et al. Cancer immunotherapy strategies based on overcoming barriers within the tumor microenvironment. Curr. Opin. Immunol. 25, 268–276 (2013).
Gajewski, T. F. The next hurdle in cancer immunotherapy: overcoming the non-T-cell-inflamed tumor microenvironment. Semin. Oncol. 42, 663–671 (2015).
Tumeh, P. C. et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 515, 568–571 (2014).
Spranger, S. et al. Up-regulation of PD-L1, IDO, and Tregs in the melanoma tumor microenvironment is driven by CD8+ T cells. Sci. Transl. Med. 5, 200ra116 (2013).
Fehrenbacher, L. et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet 387, 1837–1846 (2016).
Rosenberg, J. E. et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: a single-arm, multicentre, phase 2 trial. Lancet 387, 1909–1920 (2016).
McDermott, D. F. et al. Atezolizumab, an anti-programmed death-ligand 1 antibody, in metastatic renal cell carcinoma: long-term safety, clinical activity, and immune correlates from a phase Ia study. J. Clin. Oncol. 34, 833–842 (2016).
Harlin, H. et al. Chemokine expression in melanoma metastases associated with CD8+ T-cell recruitment. Cancer Res. 69, 3077–3085 (2009).
Taube, J. M. et al. Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti-PD-1 therapy. Clin. Cancer Res. 20, 5064–5074 (2014).
Powles, T. et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature 515, 558–562 (2014).
Garon, E. B. et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N. Engl. J. Med. 372, 2018–2028 (2015).
Joyce, J. A. & Fearon, D. T. T cell exclusion, immune privilege, and the tumor microenvironment. Science 348, 74–80 (2015).
Salmon, H. et al. Matrix architecture defines the preferential localization and migration of T cells into the stroma of human lung tumors. J. Clin. Invest. 122, 899–910 (2012).
Gajewski, T. F., Schreiber, H. & Fu, Y. X. Innate and adaptive immune cells in the tumor microenvironment. Nature Immunol. 14, 1014–1022 (2013).
Woo, S. R., Corrales, L. & Gajewski, T. F. Innate immune recognition of cancer. Annu. Rev. Immunol. 33, 445–474 (2015).
Savage, P. A., Malchow, S. & Leventhal, D. S. Basic principles of tumor-associated regulatory T cell biology. Trends Immunol. 34, 33–40 (2013).
Muller, P. et al. Trastuzumab emtansine (T-DM1) renders HER2+ breast cancer highly susceptible to CTLA-4/PD-1 blockade. Sci. Transl. Med. 7, 315ra188 (2015). This paper showed that the ability of a targeted microtubule antagonist (bound as an antibody–drug conjugate with an anti-HER2 antibody) to sensitize tumours to the effects of immunotherapy is dependent on the presence of an intact immune system, leading to the concept that even chemotherapy may work, at least partly, by an immunological mechanism.
Pardoll, D. M. The blockade of immune checkpoints in cancer immunotherapy. Nature Rev. Cancer 12, 252–264 (2012).
Topalian, S. L. et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 366, 2443–2454 (2012).
Brahmer, J. R. et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 366, 2455–2465 (2012).
Le, D. T. et al. PD-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 372, 2509–2520 (2015).
Rosenberg, J. et al. PD-L1 expression, Cancer Genome Atlas (TCGA) subtype, and mutational load as independent predictors of response to atezolizumab (atezo) in metastatic urothelial carcinoma (mUC; IMvigor210). J. Clin. Oncol. 34 (suppl.), 104 (2016).
Kowanetz, M. et al. Spatiotemporal effects on programmed death ligand 1 (PD-L1) expression and immunophenotype of non-small cell lung cancer (NSCLC). J. Thorac. Oncol. 10 (suppl. 2), S199 (2015).
Rooney, M. S., Shukla, S. A., Wu, C. J., Getz, G. & Hacohen, N. Molecular and genetic properties of tumors associated with local immune cytolytic activity. Cell 160, 48–61 (2015).
Müller, P. et al. Metastatic spread in patients with non-small cell lung cancer is associated with a reduced density of tumor-infiltrating T cells. Cancer Immunol. Immunother. 65, 1–11 (2016).
Baine, M. K. et al. Characterization of tumor infiltrating lymphocytes in paired primary and metastatic renal cell carcinoma specimens. Oncotarget 6, 24990–25002 (2015).
Schumacher, T. N. & Schreiber, R. D. Neoantigens in cancer immunotherapy. Science 348, 69–74 (2015).
Seliger, B. et al. Suppression of MHC class I antigens in oncogenic transformants: association with decreased recognition by cytotoxic T lymphocytes. Exp. Hematol. 24, 1275–1279 (1996).
Seliger, B. et al. Down-regulation of the MHC class I antigen-processing machinery after oncogenic transformation of murine fibroblasts. Eur. J. Immunol. 28, 122–133 (1998).
Atkins, D. et al. MHC class I antigen processing pathway defects, ras mutations and disease stage in colorectal carcinoma. Int. J. Cancer 109, 265–273 (2004).
Bradley, S. D. et al. BRAFV600E co-opts a conserved MHC class I internalization pathway to diminish antigen presentation and CD8+ T-cell recognition of melanoma. Cancer. Immunol. Res. 3, 602–609 (2015).
Chang, J. T., Wherry, E. J. & Goldrath, A. W. Molecular regulation of effector and memory T cell differentiation. Nature Immunol. 15, 1104–1115 (2014).
Tekpli, X. et al. DNA methylation at promoter regions of interleukin 1B, interleukin 6, and interleukin 8 in non-small cell lung cancer. Cancer Immunol. Immunother. 62, 337–345 (2013).
Chen, L. et al. Metastasis is regulated via microRNA-200/ZEB1 axis control of tumour cell PD-L1 expression and intratumoral immunosuppression. Nature Commun. 5, 5241 (2014).
Gettinger, S. N. et al. Molecular, immune and histopathological characterization of NSCLC based on PDL1 expression on tumor and immune cells and assocation with response to the anti-PDL1 antibody MPDL3280A. J. Clin. Oncol. 33 (suppl.), 3015 (2015).
Calon, A. et al. Dependency of colorectal cancer on a TGF-β-driven program in stromal cells for metastasis initiation. Cancer Cell 22, 571–584 (2012).
Coombes, J. L. et al. A functionally specialized population of mucosal CD103+ DCs induces Foxp3+ regulatory T cells via a TGF-β and retinoic acid-dependent mechanism. J. Exp. Med. 204, 1757–1764 (2007).
Feig, C. et al. Targeting CXCL12 from FAP-expressing carcinoma-associated fibroblasts synergizes with anti-PD-L1 immunotherapy in pancreatic cancer. Proc. Natl Acad. Sci. USA 110, 20212–20217 (2013).
Royal, R. E. et al. Phase 2 trial of single agent Ipilimumab (anti-CTLA-4) for locally advanced or metastatic pancreatic adenocarcinoma. J. Immunother. 33, 828–833 (2010).
Brahmer, J. R. et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J. Clin. Oncol. 28, 3167–3175 (2010).
Beatty, G. L. et al. A phase I study of an agonist CD40 monoclonal antibody (CP-870,893) in combination with gemcitabine in patients with advanced pancreatic ductal adenocarcinoma. Clin. Cancer Res. 19, 6286–6295 (2013).
Cho, J. H. & Feldman, M. Heterogeneity of autoimmune diseases: pathophysiologic insights from genetics and implications for new therapies. Nature Med. 21, 730–738 (2015).
Parkes, M., Cortes, A., van Heel, D. A. & Brown, M. A. Genetic insights into common pathways and complex relationships among immune-mediated diseases. Nature Rev. Genet. 14, 661–673 (2013).
Duffy, D. et al. Functional analysis via standardized whole-blood stimulation systems defines the boundaries of a healthy immune response to complex stimuli. Immunity 40, 436–450 (2014).
Garrett, W. S. Cancer and the microbiota. Science 348, 80–86 (2015).
Iida, N. et al. Commensal bacteria control cancer response to therapy by modulating the tumor microenvironment. Science 342, 967–970 (2013). Together with ref. 111 this paper demonstrates that the response to chemotherapy in mice is linked to the presence of a functional gut microbiome.
Sivan, A. et al. Commensal Bifidobacterium promotes antitumor immunity and facilitates anti-PD-L1 efficacy. Science 350, 1084–1089 (2015). Together with ref. 112 this paper demonstrates that the response to both chemotherapy and immunotherapy are linked to the gut microbiome.
Vétizou, M. et al. Anticancer immunotherapy by CTLA-4 blockade relies on the gut microbiota. Science 350, 1079–1084 (2015).
Viaud, S. et al. The intestinal microbiota modulates the anticancer immune effects of cyclophosphamide. Science 342, 971–976 (2013).
Dubin, K. et al. Intestinal microbiome analyses identify melanoma patients at risk for checkpoint-blockade-induced colitis. Nature Commun. 7, 10391 (2016).
Black, S., Nicolay, U., Del Giudice, G. & Rappuoli, R. Influence of statins on influenza vaccine response in elderly individuals. J. Infect. Dis. 213, 1224–1228 (2016).
Dopico, X. C. et al. Widespread seasonal gene expression reveals annual differences in human immunity and physiology. Nature Commun. 6, 7000 (2015).
Wang, C. et al. Effects of aging, cytomegalovirus infection, and EBV infection on human B cell repertoires. J. Immunol. 192, 603–611 (2014).
Sasaki, S. et al. Limited efficacy of inactivated influenza vaccine in elderly individuals is associated with decreased production of vaccine-specific antibodies. J. Clin. Invest. 121, 3109–3119 (2011).
Acknowledgements
The authors would like to thank S. Turley, M. Albert, W. Grossman, L. Delamarre, P. Hegde, A. Murthy, J. Grogan, G. Jarmy, L. Molinero, D. Berger and K. McClellan for their review of and input into this manuscript, and L. Molinero for coining the terms immune desert and hyperexhausted. Medical writing assistance was provided by L. Yauch of Health Interactions and paid for by F. Hoffmann-La Roche.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
D.S.C. and I.M. are employees of Genentech, Inc.
Additional information
Reprints and permissions information is available at www.nature.com/reprints.
Reviewer Information Nature thanks G. Dranoff, W.-H. Fridman and J. Wolchok for their contribution to the peer review of this work.
Supplementary Information is linked to the online version of the paper at go.nature.com/2iiur42.
Supplementary information
Supplementary Figure 1
Cancer immunotherapy-based combination studies underway in 2016. (DOC 479 kb)
Rights and permissions
About this article

Cite this article
Chen, D., Mellman, I. Elements of cancer immunity and the cancer–immune set point. Nature 541, 321–330 (2017). https://doi.org/10.1038/nature21349
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nature21349
- Springer Nature Limited
This article is cited by
-
Role of STING in the treatment of non-small cell lung cancer
Cell Communication and Signaling (2024)
-
Crosstalk between colorectal CSCs and immune cells in tumorigenesis, and strategies for targeting colorectal CSCs
Experimental Hematology & Oncology (2024)
-
Potential anti-tumor effects of regulatory T cells in the tumor microenvironment: a review
Journal of Translational Medicine (2024)
-
Effects of IFN-γ on the immunological microenvironment and TAM polarity in stage IA non-small cell lung cancer and its mechanisms
BMC Pulmonary Medicine (2024)
-
Cucurbit[8]uril-based supramolecular theranostics
Journal of Nanobiotechnology (2024)