
Abstract
We investigated the genetic overlap between Alzheimer’s disease (AD) and Parkinson’s disease (PD). Using summary statistics (P-values) from large recent genome-wide association studies (GWAS) (total n=89 904 individuals), we sought to identify single nucleotide polymorphisms (SNPs) associating with both AD and PD. We found and replicated association of both AD and PD with the A allele of rs393152 within the extended MAPT region on chromosome 17 (meta analysis P-value across five independent AD cohorts=1.65 × 10−7). In independent datasets, we found a dose-dependent effect of the A allele of rs393152 on intra-cerebral MAPT transcript levels and volume loss within the entorhinal cortex and hippocampus. Our findings identify the tau-associated MAPT locus as a site of genetic overlap between AD and PD, and extending prior work, we show that the MAPT region increases risk of Alzheimer’s neurodegeneration.
Similar content being viewed by others

Introduction
Alzheimer’s disease (AD) and Parkinson’s disease (PD) are the two most common neurodegenerative disorders. Neuropathologically, AD is characterized by the presence of extracellular amyloid-β plaques and intracellular tau-associated neurofibrillary tangles, whereas PD involves deposition of α-synuclein-containing Lewy bodies.1 Though AD and PD are considered distinct neurodegenerative entities, there is evidence for Lewy body pathology in AD2 and Alzheimer’s-type pathology in PD3 suggesting overlap between these two disorders. Importantly, although tau-associated pathology is considered a hallmark of AD, genome-wide association studies (GWAS) in PD have identified several polymorphisms in and around the tau-encoding microtubule-associated protein gene (MAPT)4, 5 indicating that similar biochemical perturbations may contribute to both AD and PD.6 Furthermore, prior reports investigating the genetic relationship between MAPT and AD risk have been conflicting, with some studies finding a positive association7, 8 and other studies showing no association,8, 9 indicating that the role of the MAPT gene in influencing Alzheimer’s neurodegeneration is still largely unknown.
Combining GWAS from two disorders provides insights into genetic pleiotropy (defined as a single gene or variant being associated with more than one distinct phenotype) and could elucidate shared pathobiology. Here, using summary statistics (P-values) from large genetic studies,10, 11, 12, 13, 14 we sought single nucleotide polymorphisms (SNPs) associating with both AD and PD.
Methods
Participant samples
We obtained complete GWAS results in the form of summary statistics from the PD International Parkinson’s Disease Genetics Consortium (IPDGC) and AD Alzheimer’s Disease Genetics Consortium (ADGC). The PD GWAS summary statistic results from IPDGC consisted of 5333 cases and 12 019 controls obtained from five studies with genotyped and imputed data at 7 689 524 SNPs (Table 1a, for additional details, see International Parkinson Disease Genomics Consortium10). The AD GWAS summary statistic data from ADGC consisted of 11 840 cases and 10 931 controls obtained from 15 studies with genotyped and imputed data at 2 324 889 SNPs (Table 1a, for additional details, see Naj et al.11). The ADGC GWAS summary statistic data were co-varied for age, sex and number of apolipoprotein E (APOE) alleles. There was no overlap between the ADGC and the IPDGC cases/controls.
To test for replication, we also assessed the P-values of the PD genome-wide significant SNPs in four separate AD cohorts, namely the Genetic and Environmental Risk in Alzheimer's Disease (GERAD) sample, a cohort of AD cases and controls drawn from the population of Iceland (deCODE cohort), a small cohort of mild cognitive impairment or AD cases and controls drawn from the population of Norway (Oslo), and the Cohorts for Heart and Aging Research in Genomic Epidemiology (CHARGE) consortium. The AD GWAS summary statistic results from the GERAD consortium were obtained from 13 studies and consisted of 3941 cases (62.7% female) and 7848 controls (55.6% female) with genotyped data at 529 205 SNPs (for additional details, see Harold et al.12). A total of 5571 controls from the PD IPDGC GWA were also present in the AD GERAD GWA. The AD GWAS summary statistic data drawn from the Icelandic population (deCODE) included 3759 AD cases (65.8% female) and 8888 older controls (57.8% females) greater than 85 years of age (for additional details, see Jonsson et al.13, 14). The AD GWAS summary statistic data from the CHARGE consortium were obtained from four studies and included 1315 AD cases (62.1% female) and 21 766 controls (56.9% female) (for additional details, see Lambert et al.15). The AD GWAS summary statistic data drawn from the Norwegian population (Oslo) included 434 individuals classified as AD or mild cognitive impairment (57% female) and 1830 controls (49% female) (for additional details, please see Supplementary Information).
These studies addressed potential concerns of population stratification by limiting analysis to individuals of European descent, including principal components of genetic variation in the regression tests and controlling post hoc for genomic inflation with genomic control (for additional details, see International Parkinson Disease Genomics Consortium,10 Naj et al.,11 Harold et al.,12 Jonsson et al.13,14 and Lambert et al.15).
For the gene expression analyses, we used publicly available, genotyping (performed on the Affymetrix GeneChip Human Mapping 500K Array Set platform (Santa Clara, CA, USA)) and RNA expression data (performed on the Illumina HumanRefseq-8 Expression BeadChip system (San Diego, CA, USA)) from neuropathologically confirmed 176 late-onset AD cases (mean age=83.4 years, s.d.=6.6) and 188 controls (mean age=81.2 years, s.d.=9.1) from the Gene Expression Omnibus (GEO) data set GSE15222.16 We additionally evaluated genotype and imaging data obtained from 620 older participants (174 healthy older controls, 311 individuals with mild cognitive impairment and 135 individuals with probable AD) from the Alzheimer’s Disease Neuroimaging Initiative (ADNI—see Table 1b and Supplementary Methods). We restricted our analyses to those participants with available genotype and quality-assured baseline and follow-up MRI scans (6 months to 3.5 years, mean of 2.02 years, s.d.=0.80 years) available as of April 2011. We assessed longitudinal sub-regional change in grey matter volume (atrophy) on serial 2471 T1-weighted MRI scans using a modified version of the FreeSurfer software package (for additional details, see Supplementary Methods).
Statistical analyses
We used stepwise gatekeeper hypothesis testing17 to identify SNPs associating with both PD and AD. We restricted our analyses to only those SNPs assayed in both GWASs from the IPDGC and the ADGC Consortia. First, we identified ‘pruned’ SNPs (removing all SNPs with r2>0.2, within 1 Mb of a given SNP) that were significant at a genome-wide level (P<5 × 10−8) within PD. Next, we evaluated the P-values of these PD genome-wide significant SNPs within the AD ADGC GWAS APOE, age and sex co-varied summary statistic P-values) and applied a Bonferroni correction to control for multiple comparisons. Note that because the SNPs were a priori selected independently of the P-values from AD ADGC, the proper Bonferroni correction is in terms of the number of PD genome-wide significant SNPs. Therefore, the P-value threshold for detecting significant ADGC loci controls for the number of PD genome-wide significant SNPs rather than P<5 × 10−8. It is important to note that this stepwise gatekeeper hypothesis testing approach implies a strict control for family-wise error rate in a multiple testing framework. 17
Results
Genetic overlap between AD and PD at the A allele of rs393152
We found eight SNPs on four chromosomes that were genome-wide significant in PD, thus requiring a Bonferroni-corrected P-value significance threshold of 0.00625 (Table 2). Across all eight SNPs, we found that the A allele of rs393152, within the CRHR1 region on chromosome 17 (within the extended MAPT locus) and with a minor allele frequency of 23.1%, significantly increased AD risk in the ADGC cohort (P-value=1.17 × 10−4, odds ratio (OR) for the minor allele=0.90, 95% confidence interval (CI)=0.86–0.95) (Table 2; Figure 1). In a replication analysis, we found that the A allele of rs393152 also significantly increased AD risk within the GERAD (one-tailed P-value=0.0048, OR for the minor allele=0.92, 95% CI=0.86–0.98), deCODE (one-tailed P-value=0.017, OR for the minor allele=0.92, 95% CI=0.85–0.99) and Oslo cohorts (one-tailed P-value=0.047, OR for the minor allele=0.85, 95% CI=0.71–1.02). We replicated the directionality of effect for the A allele of rs393152 within the CHARGE cohort (one-tailed P-value=0.318, OR for the minor allele=0.97, 95% CI=0.85–1.10). We conducted an inverse variance-weighted meta-analysis18 and found a two-tailed meta-analysis P-value of 1.65 × 10−7 (meta analysis OR=0.91, 95% CI=0.88–0.94) (Figure 1).

Forest plot for rs393152. As rs393152 was not available within the Oslo cohort (*), we used a proxy SNP (rs17690703; r2=.765, D'=1 in Hapmap2).
We evaluated the statistical power for detecting an association of rs393152 with AD across the discovery (ADGC) and the combined, meta-analysis AD cohorts (ADGC+GERAD+deCODE+Oslo+CHARGE). Using a GWAS threshold of P<5 × 10−8, the power within ADGC was 0.028 and within the meta-analysis cohort was 0.36, demonstrating that even the combined cohort consisting of 21 289 AD cases and 51 263 controls was underpowered to detect an association between AD and rs393152 using a standard GWAS approach. However, leveraging PD such that power is computed conditional on discovery in the PD sample (stepwise gatekeeper hypothesis testing), by using P<0.00625 (where Bonferroni corrected P=0.05/number of genome-wide significant SNPs in PD), the power within ADGC was 0.854 and within the meta-analysis cohort was 0.998 indicating that restricting evaluation to only PD-significant SNPs results in considerable increase in statistical power for AD gene discovery. We also calculated the sample size needed to detect rs393152 ((C-1 Θ-1(5 × 10−8)2/ Θ-1(0.00625)2), where Θ-1 is the inverse standard normal cumulative distribution function) and found that in comparison with our discovery cohort, 4.5 times as many subjects would be needed to detect rs393152 using a standard GWAS approach at the same alpha/Type I error.
On the basis of the 1000 Genomes Project LD structure, we found that rs393152 was in r2 LD>0.8 with a number of variants within the MAPT gene on chromosome 17 (Figure 2a). Fine mapping showed that rs1981997 constituted the peak of the AD association signal within MAPT (r2=1.0 with rs393152 in HapMap 2; Figure 2b). Across the ADGC (risk allele=A, two-tailed P-value=9.54 × 10−5, OR=0.90, 95% CI=0.85–0.95), GERAD (one-tailed P-value=0.006, OR=0.92, 95% CI=0.86–0.98, deCODE (one-tailed P-value=0.018, OR=0.92, 95% CI=0.84–0.99), Oslo (one-tailed P-value=0.047, OR=0.85, 95% CI=0.71–1.03) and CHARGE (one-tailed P-value=0.0327, OR=0.96, 95% CI=0.84–1.08) cohorts, the leading SNP in the MAPT region, rs1981997, demonstrated a similar meta-analysis P-value to rs393152 (two-tailed meta-analysis P-value of 1.29 × 10−7, see Supplementary Figure 4) providing further evidence that our AD/PD pleiotropic variant was tagging the MAPT gene and not a false-positive result. We also note that rs393152 has been previously shown to tag the H1 haplotype at the MAPT locus (r2=0.761).5 Because of the extensive LD structure in this region, we cannot exclude the possibility that other genes, besides MAPT, are the pathologically relevant genes. However, MAPT is biologically the most plausible candidate.

(a) Regional linkage disequilibrium (LD) plot demonstrating the relationship between rs393152 on chromosome 17 and loci greater than and less than 1 Mb. The bottom panel indicates the location of genes in the region. LD measured in the 1000 genomes European Populations using plink v1.07. (b) Regional association plot illustrating the association signal within the MAPT region on chromosome 17. The bottom panel indicates the location of genes in the region. LD measured in the 1000 genomes European Populations using plink v1.07.
Non-polygenic pleiotropy between AD and PD
We further investigated whether the observed genetic overlap between AD and PD was polygenic and generalizable across a number of loci or non-polygenic and driven by the MAPT locus alone. Using recently developed statistical methods to evaluate pleiotropic effects,19, 20, 21, 22 we investigated relative ‘enrichment’ of pleiotropic SNPs in AD (APOE, age and sex co-varied summary statistic P-values from ADGC) as a function of significance in PD (summary statistic P-values from IPDGC) (for additional details, see Supplementary Methods). Removing the MAPT-associated genetic signal, consisting of all SNPs in r2>0.2 (based on 1000 Genomes Project LD structure) within 1 Mb of MAPT variants, resulted in considerable attenuation of genetic enrichment (Supplementary Figures 1a and d) indicating that the observed pleiotropy between AD and PD was non-polygenic and likely confined to the MAPT region. Similarly, after ‘pruning’ (removing SNPs in r2>0.2) all available ADGC SNPs, we found a single pleiotropic locus on chromosome 17 between AD and PD that was in r2=1.0 with MAPT. Though some genetic enrichment was still present after removing the MAPT-associated SNPs, we found a similar pattern in PD SNP enrichment conditioned on AD (Supplementary Figure 2).
AD-PD pleiotropic locus correlates with MAPT transcript levels
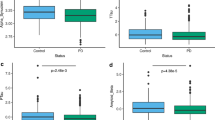
We assessed the relationship between the AD-PD pleiotropic locus on chromosome 17 and MAPT transcript levels within the brain (target id=GI_8400714-A and reference sequence=NM_016841. 1 in GSE15222, for additional details, see Webster et al.16 and Myers et al.23). As rs393152 was not available in the GEO dataset, we focused on rs422112 within the CRHR1 locus on chromosome 17, the best available proxy (closest distance and r2>0.98) for rs393152. We used an additive model with minor allele (T) counts coded as 0, 1 and 2. Given the allele frequencies and near-complete LD between rs393152 and rs422112, the ‘A’ allele of rs393152 tags the ‘C’ allele of rs422112 and the ‘G’ allele of rs393152 tags the ‘T’ allele of rs422112. Using linear regression, co-varying for the effects of age at death, APOE ɛ4 carrier status, diagnosis (AD cases vs controls), brain tissue region (frontal, parietal, temporal or cerebellar), postmortem interval, institute source of sample and hybridization date, we evaluated the relationship between rs422112 and MAPT transcript expression levels. Across all cases and controls, we found a strong association between the T allele of rs422112 and decreased MAPT transcript expression levels (standardized β-coefficient=−0.27, t-statistic=−6.61, P-value=1.45 × 10−10), which corresponds to presence of the A allele of rs393152 and increased MAPT transcript expression (Figure 3). Subgroup analyses demonstrated similar results within the AD cases and controls (see Supplementary Results). We further assessed the specificity of our findings by evaluating the relationship between the AD-PD pleiotropic locus and transcript levels of synaptophysin (SYP), a neuronal protein, and synuclein (SNCA), a neural protein associated with tau and PD. In contrast to MAPT transcript levels, we found no relationship between rs422112 and transcript levels of either SYP or SNCA (see Supplementary Results and Figure 3). We additionally performed a ‘locus-wide association study’ testing all SNPs in the MAPT region for association with MAPT transcript expression levels. SNPs in r2=1.0 with rs393152 constituted the peak of the association signal (P<1.0 × 10−8) with MAPT transcript expression levels (Figure 4). We also evaluated the relationship between SNPs in LD with rs393152 and transcript levels of other chromosome 17 genes within the larger MAPT region that were available within GSE15222.16 As illustrated in Supplementary Figures 3a and f, SNPs in LD with rs393152 did not demonstrate significant association with transcript levels of other genes within the MAPT region further illustrating the specificity of our MAPT findings.

Box plots illustrating the relationship between rs393152 alleles (x axis) and gene expression levels of MAPT, SYP and SNCA (y axis). For each plot, thick black lines show the median value. Regions above and below the black line show the upper and lower quartiles, respectively. The dashed lines extend to the minimum and maximum values with outliers shown as open circles. For MAPT, a proxy SNP was used (please see Results for additional details). As illustrated, the A allele of rs393152 demonstrated a selective dose-dependent effect on the level of intracranial MAPT transcript.

Regional association plot demonstrating the relationship between MAPT transcript expression levels (y axis) and SNPs in LD with rs393152 on chromosome 17. The bottom panel indicates the location of genes in the region. Linkage disequilibrium measured in the 1000 genomes European Populations using plink v1.07. As illustrated, SNPs in r2 LD=1 with rs393152 constituted the peak of the association signal with MAPT transcript expression levels.
AD-PD pleiotropic locus correlates with longitudinal brain atrophy
Using linear mixed effects models, we assessed the relationship of rs393152 with longitudinal brain atrophy specifically within the entorhinal cortex and hippocampus, two medial temporal lobe regions selectively affected in the earliest stages of AD.24 These models co-varied for the effects of baseline age, sex, education, group status (healthy older control vs mild cognitive impairment vs AD), disease severity (Clinical Dementia Rating-Sum of Box score) and APOE ɛ4 carrier status. We used an additive model with major allele (A) counts coded as 0, 1, and 2. Across all available ADNI participants, we found that the A allele of rs393152 was significantly associated with increased atrophy rates (volume loss) of the entorhinal cortex (standardized β-coefficient=−0.003, s.e.=0.001, P-value=0.0071) and hippocampus (standardized β-coefficient=−0.003, s.e.=0.001, P-value=0.0031).
AD-PD pleiotropic locus demonstrates larger effect among APOE ɛ4 non-carriers
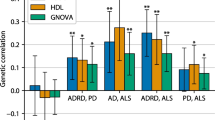
We further assessed the relationship between rs393152, MAPT transcript expression levels and medial temporal lobe atrophy separately among APOE ɛ4 carriers (presence of at least one ɛ4 allele) and non-carriers (absence of at least one ɛ4 allele). Using the linear regression and mixed effects model framework described above, we found a stronger effect between rs393152 and MAPT transcript expression levels among APOE ɛ4 non-carriers (standardized β-coefficient=−0.22, s.e.=0.04, P-value=1.1 × 10−6) than the APOE ɛ4 carriers (standardized β-coefficient=−0.14, s.e.=0.04, P-value=0.001). Similarly, we found a stronger effect between rs393152 and medial temporal lobe atrophy among APOE ɛ4 non-carriers (entorhinal cortex: standardized β-coefficient=−0.002, s.e.=0.001, P-value=0.04; hippocampus: standardized β-coefficient=−0.003, s.e.=0.001, P-value=0.01) than among APOE ɛ4 carriers (entorhinal cortex: standardized β-coefficient=−0.003, s.e.=0.002, P-value=0.07; hippocampus: standardized β-coefficient=−0.003, s.e.=0.002, P-value=0.07) (Figure 5).

Bar plots demonstrating the relationship between rs393152 alleles (x axis) and volume loss (annualized percent change—y axis) of the hippocampus (blue) and entorhinal cortex (grey) among APOE ɛ4 carriers (left panel) and APOE ɛ4 non-carriers (right panel). As illustrated, the A allele of rs393152 demonstrated a selective dose-dependent relationship with medial temporal lobe atrophy only among APOE ɛ4 non-carriers.
Discussion
In this study, we leveraged gene variants associating with PD to search for variants that associate with AD. We found a gene variant that was in strong LD with markers in the MAPT gene on chromosome 17 and that was previously associated with PD. This SNP was significantly associated with longitudinal atrophy of the entorhinal cortex and hippocampus and demonstrated a strong association with MAPT transcript levels within the brain. Considered together, our findings point to the tau-associated MAPT locus as a site genetic overlap between AD and PD.
These results indicate that leveraging the genetic signal in one phenotype may improve statistical power for gene discovery in a second, related phenotype. Rather than evaluating all possible AD susceptibility loci, we restricted our analyses to only those eight SNPs that were below genome-wide threshold in PD. As such, detection of AD susceptibility loci only among genome-wide significant PD susceptibility loci obviates the need for applying a P<5 × 10−8 threshold and constitutes stepwise gatekeeper hypothesis testing.17 This two-stage stepwise gatekeeper framework is conceptually similar to the ‘proxy-phenotype’ method, which has recently been utilized to identify common variants associated with cognitive performance. 25 It is important to note that this approach does not lower the statistical ‘bar’ for gene discovery and maintains a constant Type I error rate. By exploiting the statistical power from PD, we were able to identify one SNP within the CRHR1 locus on chromosome 17 (meta-analysis P-value=1.65 × 10−7, OR=0.91, 95% CI=0.88–0.94) that was significantly associated with increased AD risk. Importantly, the use of this stepwise, pleiotropic approach, where power is computed conditional on discovery in the PD sample, resulted in considerable improvement in statistical power for AD gene detection. In contrast, using a standard GWAS approach, neither the discovery ADGC cohort nor the combined meta-analysis cohort were sufficiently powered to detect rs393152. Given the comparable sample sizes with our current study, it is likely that the original AD GWASs11, 12, 26, 27 and even the recent meta-analysis (stage 1)15 were underpowered to detect MAPT-associated signal in AD.
There are several indications that the detected pleiotropy within chromosome 17 represents biological signal and not analysis artifacts or type 1 error. First, the use of APOE co-varied SNPs from the ADGC minimizes concerns that the detected SNPs represent spurious association resulting from the known large effect of APOE on AD risk (for an example of this, see Wijsman et al.28). Importantly, our findings indicate the presence of genetic signal independent of the chromosome 19 APOE cluster. Second, rs393152 was significantly associated with AD risk in three independent AD replication cohorts and demonstrated equivalent effect sizes in all five AD cohorts. Third, the identified pleiotropic locus was in r2 LD>0.8 with a number of variants within the tau-encoding MAPT gene on 17q21 indicating that the detected signal was specific to the MAPT region. Fourth, the leading AD-associated SNP in the MAPT region (rs1981997, r2 LD=1.0 with rs393152 in the HapMap 2) demonstrated a similar meta-analysis P-value to rs393152 providing further evidence that our AD/PD pleotropic SNP was not a false-positive result. Finally, the A allele of rs393152 showed a dose-dependent effect specifically with MAPT transcript levels within the brain and was significantly associated with longitudinal medial temporal lobe atrophy, an established endophenotype of Alzheimer’s neurodegeneration.
These single locus results point to shared pathobiology between AD and PD. Although we cannot exclude the possibility that other genes at this chromosome 17 locus are the pathologically relevant genes, our data are biologically plausible and consistent with prior experimental evidence establishing the role of MAPT in neurodegenerative diseases.28 The pleiotropic variant we found, rs393152, tags the H1 haplotype at the MAPT locus,5 which has been associated with a number of tauopathies including corticobasal degeneration, progressive supranuclear palsy and PD.5, 29 Furthermore, broadly consistent with a prior study,30 our results suggest non-extensive, non-polygenic pleiotropy between AD and PD localized to the MAPT cluster on chromosome 17.
Despite a number of prior studies,7, 8, 9, 31 the role of MAPT in AD is still unclear. Extending prior work suggesting a significant relationship between the MAPT H17 (within the GERAD cohort) and H28 (within the ADGC cohort) haplotypes and AD risk, our findings indicate that the A allele of rs393152, which tags the H1 haplotype at the MAPT locus,5 increases risk for AD. Building on prior research demonstrating a robust association between a variant in the H2 haplotype and reduced MAPT brain expression levels,8 we found a dose-dependent effect of the A allele of rs393152 (Figure 3) on intracranial MAPT gene expression. In contrast, we found no association between rs393152 and transcript levels of either synaptophysin or synuclein indicating the specificity of the relationship between the identified AD-PD pleiotropic locus and MAPT transcript expression. Our gene expression findings are consistent with prior work demonstrating a significant relationship between the H1 haplotype and MAPT levels.23, 32 However, a previous study33 of exon levels from multiple human brain regions found no association between the H1c subhaplotype and MAPT expression indicating that additional work using large samples is needed to systematically investigate the H1/H2 sub-haplotypes and MAPT brain expression levels. Additionally, building on prior work detecting smaller grey matter volumes within cognitively normal34 and cognitively impaired carriers of the MAPT H1 haplotype,35 we found a significant relationship between the A allele of rs393152 and longitudinal atrophy of the entorhinal cortex and hippocampus, two medial temporal lobe regions selectively affected with tau-associated neurofibrillary pathology in the earliest stages of AD. Considered together, this suggests that the PD-associated MAPT region influences Alzheimer’s neurodegeneration likely via tau-related mechanisms.
From an AD perspective, these results highlight the importance of considering tau. Recent evidence indicates that dominantly inherited mutations in MAPT cause forms of frontotemporal dementia with parkinsonism,28 a rare MAPT variant (p.A152T) increases risk for AD and frontotemporal dementia syndromes,36 and tau modulates amyloid-β-associated Alzheimer’s neurodegeneration.37 Consistent with this work, our present results indicate that tau-associated polymorphisms impact MAPT transcript levels and affect medial temporal lobe volume loss. When considered together with prior CSF,38, 39, 40 and imaging research,41, 42 our findings suggest that data from GWAS, expression quantitative trait loci and structural imaging measures may better elucidate underlying pathobiology than any of these markers by themselves. These results also demonstrate the utility of using entorhinal cortex and hippocampal atrophy rates as endophenotypes to identify and confirm AD risk variants.
In this study, the diagnosis of AD and PD was based on clinical evaluations, without histopathological confirmation. Postmortem evidence indicates the co-occurrence of α-synuclein, tangle and amyloid pathology.43 Therefore, one concern is that concomitant Parkinson’s pathology may have contributed to our MAPT-associated effect in AD. In a small cohort of autopsy-confirmed AD cases and controls, we replicated the directionality and magnitude of the A allele of rs393152 (Supplementary Figure 5) indicating that our AD-associated findings are not due to concomitant PD pathology. Furthermore, building on prior genetic work,44 among APOE ɛ4 non-carriers, we found a stronger relationship between rs393152 and both gene expression levels and medial temporal lobe atrophy (Figure 5) suggesting that MAPT may predominantly influence Alzheimer’s neurodegeneration in a smaller subset of individuals who do not possess APOE ɛ4 alleles. As a caveat, we note that because we primarily evaluated summary statistics from the discovery and replication cohorts, additional work with raw genotype data is needed to determine whether the AD-associated MAPT effect varies based on APOE ɛ4 carrier status. Another concern is the potential ‘contamination’ of PD samples with other tauopathies (such as progressive supranuclear palsy and corticobasal degeneration) strongly associated with MAPT. Using neuropathologically confirmed PD cases, a recent study45 found a significant association between rs393152 and idiopathic PD indicating that our current findings are unlikely due to contamination with unrecognized cases of progressive supranuclear palsy or corticobasal degeneration.
From a translational perspective, this work illustrates that data from large GWAS and a pleiotropic framework can provide important insights into the relationships between various diseases. Complementary to recently developed polygenic pleiotropic methods,19, 20, 21, 22 the analytic framework used in this manuscript is useful for detecting non-polygenic pleiotropy and can be integrated with other biomarkers to test biologically driven hypotheses. The combination of genetic, molecular and neuroimaging measures may be additionally helpful for detecting and quantifying the biochemical effects of therapeutic interventions.
References
Nussbaum RL, Ellis CE . Alzheimer's disease and Parkinson's disease. N Engl J Med 2003; 348: 1356–1364.
Uchikado H, DelleDonne A, Ahmed Z, Dickson DW . Lewy bodies in progressive supranuclear palsy represent an independent disease process. J Neuropathol Exp Neurol 2006; 65: 387–395.
Mann DM, Jones D . Deposition of amyloid (A4) protein within the brains of persons with dementing disorders other than Alzheimer's disease and Down's syndrome. Neurosci Lett 1990; 109: 68–75.
Satake W, Nakabayashi Y, Mizuta I, Hirota Y, Ito C, Kubo M et al. Genome-wide association study identifies common variants at four loci as genetic risk factors for Parkinson's disease. Nat Genet 2009; 41: 1303–1307.
Simón-Sánchez J, Schulte C, Bras JM, Sharma M, Gibbs JR, Berg D et al. Genome-wide association study reveals genetic risk underlying Parkinson's disease. Nat Genet 2009; 41: 1308–1312.
Shulman JM, De Jager PL . Evidence for a common pathway linking neurodegenerative diseases. Nat Genet 2009; 41: 1261–1262.
Gerrish A, Russo G, Richards A, Moskvina V, Ivanov D, Harold D et al. The role of variation at AβPP, PSEN1, PSEN2, and MAPT in late onset Alzheimer's disease. J Alzheimers Dis 2012; 28: 377–387.
Allen M, Kachadoorian M, Quicksall Z, Zou F, Chai HS, Younkin C et al. Association of MAPT haplotypes with Alzheimer's disease risk and MAPT brain gene expression levels. Alzheimers Res Ther 2014; 6: 39.
Mukherjee O, Kauwe JS, Mayo K, Morris JC, Goate AM . Haplotype-based association analysis of the MAPT locus in late onset Alzheimer's disease. BMC Genet 2007; 8: 3.
International Parkinson Disease Genomics Consortium, Nalls MA, Plagnol V, Hernandez DG, Sharma M, Sheerin UM, Saad M et al. Imputation of sequence variants for identification of genetic risks for Parkinson's disease: a meta-analysis of genome-wide association studies. Lancet 2011; 377: 641–649.
Naj AC, Jun G, Beecham GW, Wang LS, Vardarajan BN, Buros J et al. Common variants at MS4A4/MS4A6E, CD2AP, CD33 and EPHA1 are associated with late-onset Alzheimer's disease. Nat Genet 2011; 43: 436–441.
Harold D, Abraham R, Hollingworth P, Sims R, Gerrish A, Hamshere ML et al. Genome-wide association study identifies variants at CLU and PICALM associated with Alzheimer's disease. Nat Genet 2009; 41: 1088–1093.
Jonsson T, Atwal JK, Steinberg S, Snaedal J, Jonsson PV, Bjornsson S et al. A mutation in APP protects against Alzheimer's disease and age-related cognitive decline. Nature 2012; 488: 96–99.
Jonsson T, Stefansson H, Steinberg S, Jonsdottir I, Jonsson PV, Snaedal J et al. Variant of TREM2 associated with the risk of Alzheimer's disease. N Engl J Med 2013; 368: 107–116.
Lambert JC, Ibrahim-Verbaas CA, Harold D, Naj AC, Sims R, Bellenguez C et al. Meta-analysis of 74,046 individuals identifies 11 new susceptibility loci for Alzheimer's disease. Nat Genet 2013; 45: 1452–1458.
Webster JA, Gibbs JR, Clarke J, Ray M, Zhang W, Holmans P et al. Genetic control of human brain transcript expression in Alzheimer disease. Am J Hum Genet 2009; 84: 445–458.
Dmitrienko A, Wiens BL, Tamhane A C, Wang X . Tree‐structured gatekeeping tests in clinical trials with hierarchically ordered multiple objectives. Stat Med 2007; 26: 2465–2478.
Willer CJ, Li Y, Abecasis GR . METAL: fast and efficient meta-analysis of genomewide association scans. Bioinformatics 2010; 26: 2190–2191.
Andreassen OA, Harbo HF, Wang Y, Thompson WK, Schork AJ, Mattingsdal M et alThe Psychiatric Genomics Consortium PGC Bipolar Disorder and Schizophrenia Work Groups and The International Multiple Sclerosis Genetics Consortium IMSGC. Genetic pleiotropy between multiple sclerosis and schizophrenia but not bipolar disorder: implications for immune related disease mechanisms. Mol Psychiatry 28 January 2014 [e-pub ahead of print].
Andreassen OA, Thompson WK, Schork AJ, Ripke S, Mattingsdal M, Kelsoe JR et al. Improved detection of common variants associated with schizophrenia and bipolar disorder using pleiotropy-informed conditional false discovery rate. PLoS Genet 2013; 9: e1003455.
Andreassen OA, Djurovic S, Thompson WK, Schork AJ, Kendler KS, O'Donovan MC et al. Improved detection of common variants associated with schizophrenia by leveraging pleiotropy with cardiovascular-disease risk factors. Am J Hum Genet 2013; 92: 197–209.
Liu JZ, Hov JR, Folseraas T, Ellinghaus E, Rushbrook SM, Doncheva NT et al. Dense genotyping of immune-related disease regions identifies nine new risk loci for primary sclerosing cholangitis. Nat Genet 2013; 45: 670–675.
Myers AJ, Pittman AM, Zhao AS, Rohrer K, Kaleem M, Marlowe L et al. The MAPT H1c risk haplotype is associated with increased expression of tau and especially of 4 repeat containing transcripts. Neurobiol Dis 2007; 25: 561–570.
Braak H, Braak E . Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol 1991; 82: 239–259.
Rietveld CA, Esko T, Davies G, Pers TH, Turley P, Benyamin B et al. Common genetic variants associated with cognitive performance identified using the proxy-phenotype method. Proc Natl Acad Sci U S A 2014; 111: 13790–13794.
Lambert JC, Heath S, Even G, Campion D, Sleegers K, Hiltunen M et al. Genome-wide association study identifies variants at CLU and CR1 associated with Alzheimer's disease. Nat Genet 2009; 41: 1094–1099.
Seshadri S, Fitzpatrick AL, Ikram MA, DeStefano AL, Gudnason V, Boada M et al. Genome-wide analysis of genetic loci associated with Alzheimer disease. JAMA 2010; 303: 1832–1840.
Spillantini MG, Goedert M . Tau pathology and neurodegeneration. Lancet Neurol 2013; 12: 609–622.
Pittman AM, Fung HC, de Silva R . Untangling the tau gene association with neurodegenerative disorders. Hum Mol Genet 2006; 15: R188–R195.
Moskvina V, Harold D, Russo G, Vedernikov A, Sharma M, Saad M et al. Analysis of genome-wide association studies of Alzheimer disease and of Parkinson disease to determine if these 2 diseases share a common genetic risk. JAMA Neurol 2013; 70: 1268–1276.
Abraham R, Sims R, Carroll L, Hollingworth P, O'Donovan MC, Williams J, Owen MJ . An association study of common variation at the MAPT locus with late-onset Alzheimer's disease. Am J Med Genet B Neuropsychiatr Genet 2009; 150B: 1152–1155.
Zou F, Chai HS, Younkin CS, Allen M, Crook J, Pankratz VS et al. Brain expression genome-wide association study (eGWAS) identifies human disease-associated variants. PLoS Genet 2012; 8: e1002707.
Trabzuni D, Wray S, Vandrovcova J, Ramasamy A, Walker R, Smith C et al. MAPT expression and splicing is differentially regulated by brain region: relation to genotype and implication for tauopathies. Hum Mol Genet 2012; 21: 4094–4103.
Canu E, Boccardi M, Ghidoni R, Benussi L, Testa C, Pievani M et al. H1 haplotype of the MAPT gene is associated with lower regional gray matter volume in healthy carriers. Eur J Hum Genet 2009; 17: 287–294.
Goñi J, Cervantes S, Arrondo G, Lamet I, Pastor P, Pastor MA . Selective brain gray matter atrophy associated with APOE ɛ4 and MAPT H1 in subjects with mild cognitive impairment. J Alzheimer’s Dis 2013; 33: 1009–1019.
Coppola G, Chinnathambi S, Lee JJ, Dombroski BA, Baker MC, Soto-Ortolaza AI et al. Evidence for a role of the rare p.A152T variant in MAPT in increasing the risk for FTD-spectrum and Alzheimer's diseases. Hum Mol Genet 2012; 21: 3500–3512.
Huang Y, Mucke L . Alzheimer mechanisms and therapeutic strategies. Cell 2012; 148: 1204–1222.
Fagan AM, Roe CM, Xiong C, Mintun MA, Morris JC, Holtzman DM . Cerebrospinal fluid tau/beta-amyloid(42) ratio as a prediction of cognitive decline in nondemented older adults. Arch Neurol 2007; 64: 343–349.
Li G, Sokal I, Quinn JF, Leverenz JB, Brodey M, Schellenberg GD et al. CSF tau/Abeta42 ratio for increased risk of mild cognitive impairment: a follow-up study. Neurology 2007; 69: 631–639.
Desikan RS, McEvoy LK, Thompson WK, Holland D, Brewer JB, Aisen PS et al. Amyloid-β—associated clinical decline occurs only in the presence of elevated P-tau. Arch Neurol 2012; 169: 709–713.
Desikan RS, McEvoy LK, Thompson WK, Holland D, Roddey JC, Blennow K et al. Amyloid-β associated volume loss occurs only in the presence of p-tau. Ann Neurol 2011; 70: 657–661.
Desikan RS, McEvoy LK, Holland D, Thompson WK, Brewer JB, Aisen PS et al. Apolipoprotein E {varepsilon}4 does not modulate amyloid-β-associated neurodegeneration in preclinical Alzheimer disease. Am J Neuroradiol 2013; 34: 505–510.
Sutherland GT, Siebert GA, Kril JJ, Mellick GD . Knowing me, knowing you: can a knowledge of risk factors for Alzheimer's disease prove useful in understanding the pathogenesis of Parkinson's disease? J Alzheimers Dis 2011; 25: 395–415.
Myers AJ, Kaleem M, Marlowe L, Pittman AM, Lees AJ, Fung HC et al. The H1c haplotype at the MAPT locus is associated with Alzheimer's disease. Hum Mol Genet 2005; 14: 2399–2404.
Charlesworth G, Gandhi S, Bras JM, Barker RA, Burn DJ, Chinnery PF et al. Tau acts as an independent genetic risk factor in pathologically proven PD. Neurobiol Aging 2012; 33: e7–11.
Wijsman EM, Pankratz ND, Choi Y, Rothstein JH, Faber KM, Cheng R et al. Genome-wide association of familial late-onset Alzheimer's disease replicates BIN1 and CLU and nominates CUGBP2 in interaction with APOE. PLoS Genet 2011; 7: e1001308.
Acknowledgements
We would like to thank Drs. Irene Litvan, Subhojit Roy and Marilyn Albert for helpful comments on an earlier version of this manuscript. This research was supported by grants from the National Institutes of Health (R01AG031224, K01AG029218, K02NS067427, T32 EB005970, UO1AG032984, U24-AG041689, and R01 MH100351), the Research Council of Norway (#213837, #225989, #223273, #237250/EU JPND), the South East Norway Health Authority (2013-123), the Norwegian Health Association and the KG Jebsen Foundation. AJS was supported by NIH grants RC2DA029475 and R01HD061414 and the Robert J. Glushko and Pamela Samuelson Graduate Fellowship. Please see Supplementary Acknowledgements for ADGC and ADNI funding sources.
Author information
Authors and Affiliations
Consortia
Corresponding authors
Ethics declarations
Competing interests
Disclosures Dr. Anders M. Dale is a Founder of and holds equity in CorTechs Labs, Inc, and serves on its Scientific Advisory Board. He is also a member of the Scientific Advisory Board of Human Longevity, Inc. (HLI), and receives funding through research agreements with General Electric Healthcare (GEHC) and Medtronic, Inc. The terms of these arrangements have been reviewed and approved by the University of California, San Diego in accordance with its conflict of interest policies. Dr. Linda K. McEvoy has stock options in CorTechs Labs, Inc. Dr. James B. Brewer holds stock options in CorTechs Labs, Inc and serves on the advisory board and receives financial support from the Eli Lilly Biomarker Unit (Amyvid). Dr. Brewer also receives research support from General Electric and Janssen Alzheimer Immunotherapy.
Additional information
Supplementary Information accompanies the paper on the Molecular Psychiatry website
Supplementary information
Rights and permissions
About this article

Cite this article
Desikan, R., Schork, A., Wang, Y. et al. Genetic overlap between Alzheimer’s disease and Parkinson’s disease at the MAPT locus. Mol Psychiatry 20, 1588–1595 (2015). https://doi.org/10.1038/mp.2015.6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/mp.2015.6
- Springer Nature Limited
This article is cited by
-
Local genetic correlations exist among neurodegenerative and neuropsychiatric diseases
npj Parkinson's Disease (2023)
-
Shared molecular genetic factors influence subcortical brain morphometry and Parkinson’s disease risk
npj Parkinson's Disease (2023)
-
Discerning the Prospects of miRNAs as a Multi-Target Therapeutic and Diagnostic for Alzheimer’s Disease
Molecular Neurobiology (2023)
-
Associations of ARHGAP26 Polymorphisms with Alzheimer’s Disease and Cardiovascular Disease
Journal of Molecular Neuroscience (2022)
-
17q21.31 sub-haplotypes underlying H1-associated risk for Parkinson’s disease are associated with LRRC37A/2 expression in astrocytes
Molecular Neurodegeneration (2022)