
Abstract
It is important to understand what genetic risk factors lead to hypertension and how genotype-specific dietary and lifestyle modification can mitigate the risk of developing hypertension. The ATP2B1 rs17249754 gene, which encodes a calcium pump expressed in vascular smooth muscle was identified as having variants that conferred higher or lower risk of hypertension—with the major allele carriers being increased at risk. However, the effects of dietary intakes on risk of hypertension among carriers of the different alleles have not been fully elucidated. Therefore, we evaluated ATP2B1 rs17249754 and its interaction with dietary intakes of sodium (Na), potassium (K) and calcium (Ca) on the risk of developing hypertension using the Ansan/Ansung (n=8842) and City-Rural (n=5512) cohorts from the Korean Genome and Epidemiology Study. Carriers of the major allele of ATP2B1 rs17249754 were at greater risk of developing hypertension and high Na intake and low Ca increased the risk more in major allele than among minor allele carriers. High potassium intake was more protective against hypertension in the subjects expressing minor alleles and a low Na/K intake ratio was the most consistently beneficial to the subjects expressing the minor allele. When controlling for Na and K, low Ca intake was associated with a substantially higher risk for high systolic blood pressure in the major allele carriers compared with minor allele, suggesting good calcium status is especially important for the major allele carriers. In conclusion, people with the major allele of ATP2B1 rs17249754 are susceptible to hypertension especially in low intake of Ca and high ratio of Na and K.
Similar content being viewed by others


Introduction
Hypertension is a leading cause of morbidity and mortality (about 9.4 million deaths worldwide per year) and affects about one-third of adults.1 An increase of 20 mm Hg in systolic blood pressure (SBP) and 10 mm Hg in diastolic blood pressure (DBP) is estimated to double the risk of cardiovascular diseases.2 High blood pressure is attributable to the occurrence of 35–54% of stroke and 21–47% of ischemic heart diseases in worldwide.2 The prevalence of hypertension in the age 30 or more Korean population was 32.9% in men and 23.7% in women, and the prevalence of prehypertension was 28.4% in men and 18.8% in women in the Korean National Health and Nutrition Examination Survey in 2011.3 Women have especially increased susceptibility to developing hypertension after menopause. It is much greater in elderly people over 65 years old (58.4% in men and 68.9% in women) in Korea.3 Thus, hypertension is the most prevalent metabolic disease in elderly Koreans.
Although the cause of hypertension remains unclear, age, overweight, lack of physical activity, dyslipidemia, habitual smoking and alcohol consumption are identified risk factors.4 High fat and Na intakes and low Ca intake are also known to increase the risk of hypertension. The NHANES cross-sectional study in the United States has reported that subjects in the highest quartile of Na intake tend to have a higher DBP. In the 2010 Korean National Health and Nutrition Examination Survey5 study Koreans consumed ~7200 mg Na and 552 mg Ca daily, which did not meet their targets proposed by Geleijnse et al.6 of 3500 mg for Na and 800 mg for Ca. Thus, the improper consumptions of Na and Ca may be crucial factors for hypertension. However, salt intake acts as an independent parameter with a significant association with blood pressure only in people with metabolic syndrome, but not the general adult population.7, 8 Calcium intake is inversely associated with both SBP and DBP after adjusting for energy intake among 30~49-year-old adults in Korean National Health and Nutrition Examination Survey.7 Thus, Na and Ca intakes may interact with other factors such as genetic variants to develop hypertension.
Genome wide association studies have identified important genes associated with hypertension. The joint meta-analysis of the Cohorts of Heart and Aging Research in Genome Epidemiology Consortium (n=29 136 European descents) and the Global BPgen Consortium (n=34 433) identify novel genes related to hypertension: only ATPase plasma membrane Ca2+ transporting 1 (ATP2B1) genetic variants were associated with the risk of hypertension.9 ATP2B1 genetic variants were associated with blood pressure in meta-analysis of East Asians including Korean, Chinese and Japanese cohorts.10, 11 In the Cohorts of Heart and Aging Research in Genome Epidemiology consortium ATP2B1 rs2681472 risk allele (A) near ATP2B1 was the only genetic variant to have a positive association with hypertension risk. ATP2B1 rs172497554 risk allele (G), which has high linkage disequilibrium with rs2681472, is also associated with the increase of SBP.9, 10 These results suggest that subjects with ATP2B1 rs172497554 and rs2681472 major alleles are more susceptible to hypertension. Therefore, the majority of the population is genetically at high risk of hypertension.
Only limited studies have explored the interaction between genetic variants associated with hypertension and most nutrient intakes. We hypothesized that ATP2B1 rs17249754 variants modify the risk of hypertension and that an interaction between the variants and nutrient intakes is involved in the development of hypertension. The hypothesis was examined in 8842 middle-aged adults in the Ansan/Ansung cohorts in Korea.
Subjects and methods
Study population
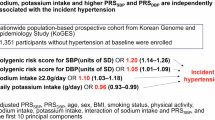
The data were obtained from the Ansan/Ansung cohort from the Korean Genome and Epidemiology Study. Ansan and Ansung cohorts represented urban and rural communities in Korea. In Ansan/Ansung cohirt 8842 subjects aged 40–69 years (4183 men and 4659 women) were recruited from 2001 to 2002. The City-Rural cohort was composed of participants (2379 men and 2863 women). The 5512 subjects aged 40–65 years in the City-cohort and Rural-cohort were recruited from 2004 to 2013 and from 2004 to 2011, respectively. The genetic study was designated as the Korea Association Resource project. These studies were large epidemiological and population genetics studies conducted by Korea Center for Disease Control and Prevention, and were carefully designed to implement proven methods. This study was approved by the199 institutional review board of the Korean National Institute of Health. Written informed consent was obtained from all subjects.
Data collection of lifestyle parameters
Similar protocols were used to collect the data and samples in the studies of both cohorts.12 However, some biochemical parameters were not measured in the City-Rural cohort. The common parameters that influence hypertension were included in the present study. The protocols for collecting data were described at once unless it needed to be explained separately. Personal history information was collected during the health interview. Anthropometry measurements were conducted as described in previous study.13 Body mass index was calculated as weight in kilograms divided by the square of the height in meters.
Definition of hypertension
SBP and DBP were measured by trained technicians for three times every 30 s using mercury sphygmomanometers (Baumanometer-Standby; W.A. Baum Co. Inc., New York, NY, USA) after subjects were rested in supine position for 5 min. The mean values of the three measurements was used to diagnose hypertension. When subjects had SBP⩾140 mm Hg, DBP⩾90 mm Hg or were taking anti-hypertensive medication, they were considered as hypertensive. Although subjects were questioned about previous diagnoses of hypertension, that information was not used for categorizing subjects as hypertensive, as many subjects did not have routine health examinations.
Laboratory biochemical tests
Blood samples were obtained in the morning after overnight fasting. Serum concentrations of total and HDL cholesterol, triglycerides, creatine and blood urea nitrogen (BUN) were measured using an automatic analyzer (ZEUS 9.9; Takeda, Tokyo, Japan).
Genotyping and quality control
DNA samples were isolated from the peripheral blood of participants. A large-scale genome-wide genotyping was performed using the Affymetrix Genome Wide SNP 5.0 for Ansan/Ansung cohort (Gyeonggi-do, Korea) and the AffymetrixGenomeWide SNP 6.0 for the City–Rural cohort.13 The accuracy of the genotyping was examined by Bayesian Robust Linear Modeling using the Mahalanobis Distance Genotyping Algorithm using GPLINK version 2.0.14 The ATP2B1 genotype quality score for data retention was set at 0.1. ATP2B1 contains 14 single-nucleotide polymorphisms (SNPs) of which 6 SNPs (rs17249754, rs11105354, rs12579302, rs2681485, rs12581002 and rs10506974) had a significant association with hypertension risk in the Korea Association Resource data.
Assessment of nutrient intake
A semi-quantitative food frequency questionnaire (SQFFQ) was used for measuring the usual food intakes. The validity and reproducibility of the SQFFQ was checked before it was used to determine food intake. The SQFFQ developed for Korean Genome and Epidemiology Study was determined to be acceptable for calculating the participants’ average food intake during the past 1 year.15, 16 The SQFFQ included 103 food items and the frequencies of food intakes were categorized into never or seldom, once a month, two to three times a month, one to two times a week, three to four times a week, five to six times a week, once a day, twice a day and three times or more a day based on the portion sizes. The daily intake was computed based on the midpoint of the reported frequency categories multiplying food portion size for each food item. Energy and nutrients such as energy, protein, carbohydrates and fat were calculated from daily food intake determined by SQFFQ, using the Can-Pro 2.0 nutrient intake assessment software developed by the Korean Nutrition Society.16
Statistical analysis
Statistical analyses were performed using GPLINK version 2.0 (http://pngu.mgh.harvard.edu/ ~purcell/plink) and SAS (version 9.3; SAS Institute, Cary, NC, USA). Using the G power calculator, the sample sizes for Korea Association Resource (8842) and City-Rural (5412) were adequate to obtain significance at β=0.97 and b=0.90 at an odds ratio (OR) of 1.1 and α=0.05 in the logistic analysis. Hardy–Weinberg equilibrium was evaluated using GPLINK to show the constancy from one generation to the next without disturbing factors including natural selection, mutations, genetic drift and nonrandom mating. There were no missing data in ATP2B1 genotyping in any subjects. Comparisons were made using carriers of the minor allele as the reference group, as they had the lowest risk of developing hypertension. The data were checked and they were found to be normally distributed by Proc univariate. The descriptive statistics of participants for categorical variables, such as gender and dietary habits were obtained by determining frequency distributions and the significance was analyzed using the χ2-test. The descriptive statistics of continuous variables were expressed as means and s.d. The significant differences between the normotensive and hypertensive groups were analyzed by two-sampled t-test in each cohort. The continuous independent variables were adjusted for confounding variables such as age, gender and residence area body mass index, smoking and drinking status, daily energy intake, physical activity status, serum creatine and BUN levels, and serum total cholesterol, HDL cholesterol and triglyceride levels. Multiple comparisons were performed by Tukey tests among the different groups at P⩽ 0.05. Next, ORs and 95% confidence intervals for hypertension prevalence were calculated according to the different ATP2B1 genotypes with controlling for the covariates mentioned above. In addition, ORs and 95% confidence intervals were determined in the same models according to the energy intake status based on estimated energy requirements. Last, to examine the interaction between ATP2B1 variants and the levels of macronutrient intake based on dietary reference intakes, multivariate linear regression models were analyzed, including the corresponding main effects, interaction terms of ATP2B1 genotypes (rs17249754) and macronutrient intake, and potential confounders. Multiple comparisons of groups were conducted by Tukey tests. The ORs and 95% confidence intervals between ATP2B1 variants and type 2 diabetes prevalence were also calculated using Proc logist after adjusting for covariates according to the degree of macronutrient intake.
Results
Characteristics of ATP2B1 variants
Table 1 presents the ATP2B1 genetic variants involved in hypertension risk. The six SNPs in ATP2B1 (rs17249754, rs11105354, rs12579302, rs2681485, rs12581002 and rs10506974) were selected to show significant associations with the risk of hypertension. The six SNPs are located in the intron region of ATP2B1 in chromosome 12. Four of the SNPs, rs17249754, rs11105354, rs12579302 and rs2681485, exhibited very strong correlations with (r2=0.9677–0.9995) rs17249754. These four SNPs had a negative association with the risk of hypertension (ORs=0.8389–0.8503). However, rs12581002 and rs10506974 did not correlate with rs17249754 and these two SNPs were positively associated with hypertension risk (OR=1.1 and 1.098, respectively). All significant SNPs in ATP2B1 showed no disruption of Hardy–Weinberg equilibrium (P>0.05). Thus, one SNP (rs17249754) was used to reflect the four SNPs in ATP2B1.
Baseline characteristics of normotensive, borderline and hypertensive subjects
Subjects (23.1%, average age of 56.7) had hypertension and 24.3% of them were borderline hypertensive as hypertension was defined from measured blood pressure. However, the percentage of hypertension was 15.7% of subjects with average age of 51.4 using the previous diagnosis criteria (Table 2). The difference in the hypertension incidence was associated with the age of subjects diagnosed and some subjects did not know that they had hypertension since they did not have regular check-ups. In addition, the prevalence of hypertension was about 28.6% in Koreans aged over 30 years in Korean National Health and Nutrition Examination Survey in 2001.17 Thus, hypertension was decided with the blood pressure measured in the study or by use of medication for controlling blood pressure. About half of the subjects were affected by abnormally high blood pressure. The subjects with hypertension were much older than those with normotension, indicating that age was a major risk factor for hypertension (P<0.001; Table 2). Women aged 40–65 years old had a higher incidence of hypertension than men in the City-Rural cohort but not in the Ansan-Ansung cohort. Body mass index was much higher in the hypertensive group than in the normotensive group in both cohorts (P<0.001). Subjects with hypertension exhibited dyslipidemia such as higher total serum cholesterol and triglyceride levels, and lower HDL cholesterol levels in comparison with the normotensive subjects in both cohorts. The indicators of kidney disorders, serum creatine and BUN levels were higher in the hypertensive group than the normotensive group in both cohorts. Daily energy intake (% of estimated energy requirement) was not significantly different between two groups in the Ansan/Ansung cohort. Among daily macronutrient intakes, carbohydrate intake was higher in the hypertensive group than the normotensive group, whereas the normotensive group had higher intake of protein and fat intake than the hypertensive group in both cohorts (P<0.001; Table 2). Ca and K intake was higher in the normotensive group than the hypertensive group in both cohorts (P<0.01). Na intake was significantly higher in the hypertensive group than the normotensive group only in City-Rural cohort (P<0.0001) but it was not significantly different in Ansan/Ansung cohort. However, the ratio of Na/K intake was significantly higher in the hypertensive group than the normotensive group in both cohorts (P<0.0001).
Association of ATP2B1 rs17249754 variants with hypertension
Among the Korean population, 39.2% and 37.6% were homozygous for the major alleles, 49.8% and 47.8% for heterozygous, and 11.0% and 14.6% homozygous minor alleles in the Ansan/Ansung cohort and City-Rural cohort, respectively. ATP2B1 homozygous major allele carriers had an increased risk of hypertension by 1.436 and 1.381 folds for both cohorts, respectively, compared with homozygous minor allele carriers after adjusting for the covariates (Table 3). In addition, ATP2B1 homozygous major allele carriers had an increased risk of hypertension by 1.338 (confidence interval: 1.061–1.687, P=0.0206) when using a previous diagnosis of hypertension as the criteria. Thus, the ORs were not much different between the hypertension definitions. SBP and DBP also exhibited a higher association with ATP2B1 major alleles by 1.438 and 1.531 folds on the basis of its homozygote minor alleles in the Ansan/Ansung cohort (Table 3). However, in the City-Rural cohort SBP, but not DBP, had a positive association with the major allele. Serum creatine levels were not associated with ATP2B1 variants in either cohort, whereas serum BUN levels tended to show a higher association with ATP2B1 major alleles in the Ansan/Ansung cohort (P=0.0535), but there was no association between serum BUN and ATP2B1 variants in the City-Rural cohort. In addition, serum Na, Ca and K levels were not significantly associated with ATP2B1 variants in Ansan/Ansung cohort whereas the association was not examined in the City-Rural cohort since these parameters were not measured.
Interaction of ATP2B1 rs17249754 variants and macronutrient intakes in the risk of hypertension
There was no interaction between ATP2B1 variants and nutrient intakes such as energy, protein, CHO, fat, Ca and Na in determining the prevalence of hypertension in either of the cohorts (Table 4). The ATP2B1 major alleles were positively associated with the prevalence of hypertension regardless of the levels of energy, protein, fat and Ca intake in the Ansan/Ansung cohort. However, ATP2B1 variants had different relative associations with the risk of hypertension according to the levels of CHO and Na intake. Subjects with ATP2B1 major alleles exhibited a significant positive association with the risk of hypertension compared with minor alleles when consuming a low CHO diet whereas there was no significant difference in a high CHO diet in either cohort (Table 4). Subjects with the ATP2B1 minor allele and low Na consumption had a lower incidence of hypertension compared with major allele carriers with low Na intake in the Ansan/Ansung cohort (Table 4), suggesting that low Na intake is more protective against hypertension in people with the minor allele.
Unlike the results of the Ansan/Ansung cohort only ATP2B1 major alleles showed a positive association with hypertension regardless of Na and protein intake levels in the City-Rural cohort. However, other individual nutrients exhibited significant associations with hypertension in the City-Rural cohort. High intakes of energy, fat, and potassium in subjects with ATP2B1 minor alleles protected against the risk of hypertension in comparison to the major alleles in city/rural cohort. By contrast, ATP2B1 minor alleles reduced the hypertension risk in in subjects with a low intake of carbohydrate and a low ratio of Na/K intake.
Interactions of ATP2B1 rs17249754 variants and energy and protein intake in blood pressure
As hypertension is defined by SBP and DBP, the interaction of ATP2B1 variants and Ca, Na and K intake on the risk of elevated SBP and DBP was examined, as these nutrients play an important role in the risk of hypertension. In Ansan/Ansung and City-Rural cohorts ATP2B1 variants exhibited significant interactions with Na intake on increased risk of high SBP. In the Ansan/Ansung cohort, a low Na intake among subjects with ATP2B1 major alleles had a positive association with a greater risk of high SBP and DBP compared with minor alleles (Table 5). However, in the City-Rural cohort ATP2B1 major alleles were positively associated with the risk of increasing SBP regardless of Na intake but ATP2B1 major alleles had no significant association with the risk of high DBP in either low or high intake of Na. Low Na/K was associated with a lower risk of SBP for the minor allele in in both groups and DBP in the Ansan/Ansung cohort (Table 5). High K intake resulted in subjects with the ATP2B1 minor allele having much lower risk of high SBP and DBP in both Ansan/Ansung and City-Rural cohorts than the major allele (Table 5).
There was no significant difference in SBP (Ansan/Ansung cohort), and SBP and DBP (City-Rural cohort) between the subjects with major and minor alleles especially in a high Na/K intake ratio (Figures 1a and b), indicating that a minor allele was not very protective against the risk of hypertension in the intake of high Na/K ratio. Although subjects had higher SBP (129–130 versus 122–125 mm Hg, respectively) and DBP (80.8–81.9 versus 77.9–79.4 mm Hg, respectively) in high Na/K intake than low Na/K intake in the City-Rural cohort (Figures 1a and b), a significant association of ATP2B1 variants with higher SBP and DBP was shown only in subjects with low Na/K intakes (Figures 1a and b). SBP and DBP were higher in subjects with high Na/K ratio intake than those with low ratio in Ansan/Ansung cohort (Figures 1a and c). However, there was a significant association of ATP2B1 variants with DBP in subjects with high Na/K intakes in Ansan/Ansung cohort (Figure 1c). The subjects with ATP2B1 major alleles exhibited higher SBP and DBP with low Na/K intake indicating that a low Na/K intake improved the protective effects of minor alleles, but not in high Na/K intake in Ansan/Ansung cohorts (Figure 1a and c) and City-Rural cohort (Figures 1b and d).

Blood pressure of subjects with ATP2B1 rs17249754 genotypes according to the intake of Na and K ratio. (a) SBP and DBP of the subjects with intake of low ratio of Na and K in Ansan/Ansung cohort. (b) SBP and DBP of the subjects with intake of low ratio of Na and K in City-Rural cohort. (c) SBP and DBP of the subjects with intake of high ratio of Na and K in Ansan/Ansung cohort. (d) SBP and DBP of the subjects with intake of high ratio of Na and K in City-Rural cohort Bars and error bars represented adjusted means and s.e. after adjusting for age, gender, residence area body mass index, daily energy intake, smoking status and physical activity. a,b,cDifferent alphabets on the bars indicate significant differences at P<0.05.
Discussion
It has previously been demonstrated that ATP2B1 variants can modulate the risk of hypertension in the Asian population.9, 10, 18, 19 Nutritional status of the mineral electrolytes are known to be involved in vascular smooth muscle cell contraction and relaxation that modulate the risk of hypertension. Although both gene variants and mineral electrolytes are well established factors in the etiology of hypertension, the interaction of the genetic variants with mineral status in humans is poorly understood. It is important that these interactions be clearly characterized to facilitate dietary recommendations according to genotype for preventing hypertension in at-risk patients. The present study clearly showed different dietary needs for protecting carries of the major and minor alleles of ATP2B1 against hypertension.
It is well known that Na, K and Ca are important for the regulation of blood pressure however this study has added additional information about how genetic variants can influence the best approach to preventing hypertension. A previous study has also shown that high Na excretion, used as indicator of high Na consumption, is linked to a greater incidence of hypertension among Koreans who express the major allele of ATP2B1.20 Furthermore, high urinary excretion of Na, low excretion of potassium, and a high Na/K ratio were all shown to increase the incidence of hypertension among carriers of the major allele of C-terminal Src kinase rs1378942 and C-terminal Src kinase-microRNA 4513 rs3784789 genes.21 The C-terminal Src kinase gene encodes a tyrosine kinase that inactivates Src by phosphorylation. Src is important for increasing blood pressure by mediating angiotensin II-related vasoconstriction and increased blood volume.22 This process operates in counter to the activity of the ATP2B1 Ca pump.
Blood pressure is increased by vasoconstriction as a consequence depolarization of the vascular smooth muscle cell, which involves opening of Ca channels allowing Ca to flow into the cell with the concentration gradient, which in turns opens calcium-activated K channels allowing K to exit the cell along the concentration gradient for K, resulting in hyperpolarization.23 Blood pressure is decreased as the calcium channels are closed prohibiting further influx of calcium and intracellular calcium is decreased by the active pumping of Ca from the cell (via Ca pumps such as is encoded by ATP2B1) resulting in repolarization and vasorelaxation.23, 24 The most common drugs for treating hypertension target depolarization by blocking calcium channels or modulating the rennin–angiotensin system, which stimulates Ca influx and increases Na and fluid retention.24, 25, 26 However, the ATP2B1 calcium pump is an important part of the counter to the depolarization process. The finding of this study that increased Ca is especially important to the carriers of the major allele carriers of ATP2B1 would at first seem paradoxical, as ATP2B1 is involved in lowering intracellular calcium concentrations. It is a logical assumption that as the minor alleles of ATP2B1 are protective against hypertension, they, in some way, encode more efficient Ca pumps and are more efficient at removing intracellular Ca. This is supported by the observation that ATP2B1 heterozygous knockout mice (ATP2B1+/− mice) are hypertensive and that vasorelaxation of vascular rings from the ATP2B1+/− mice was significantly attenuated.27
Several mechanisms could explain why increasing dietary calcium would help lower intracellular Ca and therefore maintain vasorelaxation and lower blood pressure. First, the membrane potential is maintained by the difference between intracellular and extracellular Ca. Increasing dietary intake of Ca could keep make the potential greater if it increased extracellular Ca with little or no effect on intracellular Ca.7 Second, low Ca status stimulates the production of the calcitrophic hormone calcitriol (1,25 dihydroxyvitamin D3). Calcitriol causes an influx of calcium into the cell, which explains how poor Ca status can increase intracellular Ca and cause a concomitant increase in blood pressure.28 These mechanisms may in part explain the importance of dietary calcium for maintaining normal blood pressure and why it is especially important for carriers of the ATP2B1 major allele, which encodes a less effective Ca pump for removal of intracellular Ca.
The Na/K consumption ratio has been the subject of much less research than just Na intake itself, but this and other studies suggest that it may be more important than Na alone. Interestingly, one of the first dietary treatments for hypertension was the ‘Rice Diet’, developed by the Duke University physician Walter Kempner in 1939, which included just rice and fruit.29 The rice diet was very low in sodium at about 150 mg per day, but high in potassium. Even thought it was highly effective at lowering blood pressure at a time when there were limited blood pressure lowering drugs, it was a highly restrictive diet that was difficult to maintain. However, several more recent studies have reported the importance of a low intake ratio of Na/K.21, 30 The potential mechanisms of Na and K on hypertension has been comprehensively reviewed.31
The major limitation of this study was the diagnosis of hypertension. As blood pressure was measured in a single visit, the blood pressure may not reflect the real blood pressure of some the subjects. However, only 27% of the subjects were identified as hypertensive for the first time in this study, with the majority having a history of hypertension. Second, the accuracy of the estimation of dietary intakes is a limitation of this study, as in all other large studies. The spot estimations of sodium intake in previous studies have been seriously questioned for accuracy and reliability.32, 33 However, the SQFFQ developed for Korean Genome and Epidemiology Study was used for measuring daily nutrient intake and the SQFFQ was especially designed and validated for this population. As the SQFFQ included 103 Korean dishes, not foods themselves, the intake of even micronutrients such as sodium would be proper to use for the study. Furthermore, the relatively high salt consumption among Koreans is largely due to high salt-containing fermented foods that are remarkably consistent in their salt content because the salt content is a major factor in fermentation. Therefore, the dietary data should be acceptably reliable.
Despite the known roles of Na, K and Ca in maintaining normal blood pressure, there is no evidence that hypertension can be fully reversed in most people by manipulating dietary intakes of these minerals alone. It has been estimated that up to 80% of hypertension is attributable to overweight and obesity.34, 35 In this study, as expected, higher body mass index and waist circumference were associated with hypertension. This study also found that hypertension was associated with a low carbohydrate diet in the general population. However, low carbohydrate diet was associated with higher risk of hypertension in the major allele group compared with the minor allele group. Other studies have found that in Koreans, a high carbohydrate diet is associated with metabolic syndrome including obesity and dyslipidemia but hypertension had no positive association with a high carbohydrate diet.36, 37 Therefore, the effect of carbohydrate in this study is difficult to interpret. The traditional Korean diet is based largely on rice and vegetables (a high carbohydrate diet and a very low fat diet) and has no association with the risk of hypertension in majority of people with ATP2B1 major allele. It is possible that the simple classification of high or low carbohydrate is unable to separate the differential effects of a high sugar diet versus diets rich in complex carbohydrates from grains and vegetables.
Conclusion
Carrying the major allele of ATP2B1 rs17249754 was associated with increased risk of hypertension. Furthermore, in people with the major alleles this study showed that it is especially important to have a high intake of Ca to reduce the risk of hypertension by genetic background. However, people with minor alleles are more salt sensitive and it is especially important for them to consume low Na/ high K diets to protect against increasing blood pressure. The results of this study can help nutritionists develop individualized dietary programs for maintaining a healthy blood pressure based on genotype.

References
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380: 2224–2260.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289: 2560–2572.
Shin J, Park JB, Kim KI, Kim JH, Yang DH, Pyun WB et al2013 Korean Society of Hypertension guidelines for the management of hypertension: part I-epidemiology and diagnosis of hypertension. Clin Hypertens 2015; 21: 1.
Ndanuko RN, Tapsell LC, Charlton KE, Neale EP, Batterham MJ . Dietary patterns and blood pressure in adults: a systematic review and meta-analysis of randomized controlled trials. Adv Nutr 2016; 7: 76–89.
2010 Korean National Health Statistics 2010 Korean National Health and Nutrition Examination Survey. National Department of Public Health: Seoul: Korea, 2010.
Geleijnse JM, Kok FJ, Grobbee DE . Impact of dietary and lifestyle factors on the prevalence of hypertension in Western populations. Eur J Public Health 2004; 14: 235–239.
Park J, Lee JS, Kim J . Relationship between dietary sodium, potassium, and calcium, anthropometric indexes, and blood pressure in young and middle aged Korean adults. Nutr Res Pract 2010; 4: 155–162.
Kim BK, Lim YH, Kim SG, Kim YM, Shin J . Relationship between sodium intake and blood pressure according to metabolic syndrome status in the Korean National Health and Nutrition Examination Survey. Blood Press Monit 2012; 17: 120–127.
Levy D, Ehret GB, Rice K, Verwoert GC, Launer LJ, Dehghan A et al. Genome-wide association study of blood pressure and hypertension. Nat Genet 2009; 41: 677–687.
Xi B, Tang W, Wang Q . Polymorphism near the ATP2B1 gene is associated with hypertension risk in East Asians: a meta-analysis involving 15 909 cases and 18 529 controls. Blood Press 2012; 21: 134–138.
Hong KW, Go MJ, Jin HS, Lim JE, Lee JY, Han BG et al. Genetic variations in ATP2B1, CSK, ARSG and CSMD1 loci are related to blood pressure and/or hypertension in two Korean cohorts. J Hum Hypertens 2010; 24: 367–372.
Kim Y, Han BG . Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int J Epidemiol 2017; 46: e20.
Park S, Daily JW, Zhang X, Jin HS, Lee HJ, Lee YH . Interactions with the MC4R rs17782313 variant, mental stress and energy intake and the risk of obesity in Genome Epidemiology Study. Nutr Metab 2016; 13: 38.
Rabbee N, Speed TP . A genotype calling algorithm for Affymetrix SNP arrays. Bioinformatics 2006; 22: 7–12.
Ahn Y, Kwon E, Shim JE, Park MK, Joo Y, Kimm K et al. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur J Clin Nutr 2007; 61: 1435–1441.
Daily JW, Park S . Interaction of BDNF rs6265 variants and energy and protein intake in the risk for glucose intolerance and type 2 diabetes in middle-aged adults. Nutrition 2017; 33: 187–194.
Prevention KCfDCa The Report of the Third Korea National Health and Nutrition Survey Control KCfD (ed.). Ministry of Health and Welfare: Seoul, 2005.
Cho YS, Go MJ, Kim YJ, Heo JY, Oh JH, Ban HJ et al. A large-scale genome-wide association study of Asian populations uncovers genetic factors influencing eight quantitative traits. Nat Genet 2009; 41: 527–534.
Xu J, Qian HX, Hu SP, Liu LY, Zhou M, Feng M et al. Gender-specific association of ATP2B1 variants with susceptibility to essential hypertension in the han chinese population. Biomed Res Int 2016; 2016: 1910565.
Lee S, Kim SH, Shin C . Interaction according to urinary sodium excretion level on the association between ATP2B1 rs17249754 and incident hypertension: the Korean genome epidemiology study. Clin Exp Hypertens 2016; 38: 352–358.
Park YM, Kwock CK, Kim K, Kim J, Yang YJ . Interaction between single nucleotide polymorphism and urinary sodium, potassium, and sodium-potassium ratio on the risk of hypertension in Korean adults. Nutrients 2017; 9: 235.
Lee HJ, Kang JO, Kim SM, Ji SM, Park SY, Kim ME et al. Gene silencing and haploinsufficiency of Csk increase blood pressure. PLoS ONE 2016; 11: e0146841.
Hu XQ, Zhang L . Function and regulation of large conductance Ca(2+)-activated K+ channel in vascular smooth muscle cells. Drug Discov Today 2012; 17: 974–987.
Hirawa N, Fujiwara A, Umemura S . ATP2B1 and blood pressure: from associations to pathophysiology. Curr Opin Nephrol Hypertens 2013; 22: 177–184.
Ko EA, Han J, Jung ID, Park WS . Physiological roles of K+ channels in vascular smooth muscle cells. J Smooth Muscle Res 2008; 44: 65–81.
Brozovich FV, Nicholson CJ, Degen CV, Gao YZ, Aggarwal M, Morgan KG . Mechanisms of vascular smooth muscle contraction and the basis for pharmacologic treatment of smooth muscle disorders. Pharmacol Rev 2016; 68: 476–532.
Fujiwara A, Hirawa N, Fujita M, Kobayashi Y, Okuyama Y, Yatsu K et al. Impaired nitric oxide production and increased blood pressure in systemic heterozygous ATP2B1 null mice. J Hypertens 2014; 32: 1415–1423.
Zemel MB . Calcium modulation of hypertension and obesity: mechanisms and implications. J Am Coll Nutr 2001; 20: 428S–435S.
Kempner W . Treatment of hypertensive vascular disease with rice diet. Am J Med 1948; 4: 545–577.
Cook NR, Obarzanek E, Cutler JA, Buring JE, Rexrode KM, Kumanyika SK et al. Joint effects of sodium and potassium intake on subsequent cardiovascular disease: the Trials of Hypertension Prevention follow-up study. Arch Intern Med 2009; 169: 32–40.
Adrogue HJ, Madias NE . Sodium and potassium in the pathogenesis of hypertension. N Engl J Med 2007; 356: 1966–1978.
Titze J . Estimating salt intake in humans: not so easy!. Am J Clin Nutr 2017; 105: 1253–1254.
Zhou L, Tian Y, Fu JJ, Jiang YY, Bai YM, Zhang ZH et al. Validation of spot urine in predicting 24-h sodium excretion at the individual level. Am J Clin Nutr 2017; 105: 1291–1296.
Hall JE, do Carmo JM, da Silva AA, Wang Z, Hall ME . Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms. Circ Res 2015; 116: 991–1006.
Schutten MT, Houben AJ, de Leeuw PW, Stehouwer CD . The link between adipose tissue renin-angiotensin-aldosterone system signaling and obesity-associated hypertension. Physiology 2017; 32: 197–209.
Park S, Ahn J, Kim NS, Lee BK . High carbohydrate diets are positively associated with the risk of metabolic syndrome irrespective to fatty acid composition in women: the KNHANES 2007-2014. Int J Food Sci Nutr 2017; 68: 479–487.
Park S, Ahn J, Lee BK . Very-low-fat diets may be associated with increased risk of metabolic syndrome in the adult population. Clin Nutr 2016; 35: 1159–1167.
Acknowledgements
We acknowledge funding from the Korean Research Foundation in Korea (NRF-2015R1D1A3A01019577).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Daily, J., Kim, B., Liu, M. et al. People with the major alleles of ATP2B1 rs17249754 increases the risk of hypertension in high ratio of sodium and potassium, and low calcium intakes. J Hum Hypertens 31, 787–794 (2017). https://doi.org/10.1038/jhh.2017.72
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhh.2017.72
- Springer Nature Limited