
Abstract
The role of dietary factors on chronic diseases seems essential in the potentially adverse or preventive effects. However, no evidence of dose–response meta-analysis of prospective cohort studies has verified the association between the intake of fruit and/or vegetables and the risk of developing hypertension. The PubMed and Embase were searched for prospective cohort studies. A generic inverse-variance method with random effects model was used to calculate the pooled relative risks (RRs) and 95% confidence intervals (CIs). Generalized least squares trend estimation model was used to calculate the study-specific slopes for the dose–response analyses. Seven articles comprised nine cohorts involving 185 676 participants were assessed. The highest intake of fruit or vegetables separately, and total fruit and vegetables were inversely associated with the incident risk of hypertension compared with the lowest level, and the pooled RRs and 95% CIs were 0.87 (0.79, 0.95), 0.88 (0.79, 0.99) and 0.90 (0.84, 0.98), respectively. We also found an inverse dose–response relation between the risk of developing hypertension and fruit intake, and total fruit and vegetables consumption. The incident risk of hypertension was decreased by 1.9% for each serving per day of fruit consumption, and decreased by 1.2% for each serving per day of total fruit and vegetables consumption. Our results support the recommendation to increase the consumption of fruit and vegetables with respect to preventing the risk of developing hypertension. However, further large prospective studies and long-term high-quality randomized controlled trials are still needed to confirm the observed association.
Similar content being viewed by others

Introduction
As a concomitant risk factor of cardiovascular disease and kidney disease, hypertension remains one of the most common causes of morbidity and mortality in many populations.1, 2, 3 Overall, more than a quarter of adults were hypertensive patients in 2000, and this proportion had been estimated to increase by about 60% in 2025.1 Therefore, primary prevention of hypertension has been considered an important public health issue around the world.
The role of dietary factors in chronic disease seems essential in the potentially adverse or preventive effects.4, 5, 6, 7, 8, 9, 10 Among these dietary factors, previous meta-analyses have demonstrated that fruit and vegetables consumption has a specific powerful association with the incident risk of many chronic diseases, such as type 2 diabetes, stroke and coronary heart disease.11, 12, 13, 14 However, no evidence of dose–response meta-analysis of prospective cohort studies has verified the association between the intake of fruit and/or vegetables and the risk of developing hypertension. Previous cross-sectional studies and case–control studies have ascertained the effect of increasing fruit and vegetables consumption on the decreased risk of hypertension and on the blood pressure reduction; however, these studies leave much uncertainty regarding the causal mechanism of the association.15, 16, 17, 18 Moreover, due to the heterogeneous geographical ethnic backgrounds and various methods of diet assessment and outcome ascertainment among studies, the magnitude of associations were inconsistent in the above findings.15, 16, 17, 18 To date, a number of clinical trials have shown that a diet high in fruit and vegetables has beneficial effect on blood pressure reduction. The duration of intervention ranged from 6 weeks to 8 months among these trials, and thus the long-term effect of fruit and vegetables intake was still unclear.19, 20, 21
In the present study, we performed a systematic review and meta-analysis to summarise the evidences from prospective cohort studies on fruit and vegetables consumption, fruit consumption or vegetables consumption separately, and the risk of incident hypertension. Furthermore, we also quantified the dose–response patterns of fruit and/or vegetables intake on the risk of developing hypertension.
Materials and methods
Literature search
The present study was carried out in adherence with the Cochrane Handbook for Systematic Reviews22 and the meta-analysis of observational studies in epidemiology guidelines.23 We searched the PubMed (1950 to 4 November 2015) and the Embase (1974 to 4 November 2015) databases for records to report fruit and/or vegetables consumption and the risk of incident hypertension with no language restriction. Our search included both free-text and Medical Subject Headings (MeSH) terms, such as ‘fruit*’, ‘vegetable*’, ‘fruit[MeSH Terms]’, ‘vegetables[MeSH Terms]’, ‘hypertension[MeSH Terms]’, ‘hypertensi*’, ‘HBP’ and ‘high blood pressure*’. Details of the search strategy are shown in Supplementary Table 1. When multiple publications from the same study were identified, we included the one with the longest duration of follow-up. Furthermore, the reference lists of relevant articles were manually searched to identify more potentially eligible articles.
Selection criteria and data extraction
The initial search was conducted by Wu and Sun independently. Duplicate records were deleted, and the titles and abstracts of each article were screened. We independently identified each article as excluded or requiring further assessment. Any disagreements were resolved by consensus.
We included articles that met the following criteria: (1) the studies reported relative risks (RRs) or hazard ratios and their corresponding 95% confidence intervals (CIs) of incident hypertension in relation to total fruit and vegetables intake, and fruit or vegetables intake separately; (2) the study design was based on prospective cohort; (3) the participants were adults aged 18 years or above. Studies were excluded if: (1) the data described the effect of individual fruit and vegetables, such as garlic, beans and soybeans; (2) the data described the surrogate nutrients of fruit and vegetables, such as fruit juice, vegetable protein and fibre; (3) the participants were pregnant or lactating females.
Data extraction was independently performed by Wu and Sun. Disagreements were resolved by discussing with He. The following data were extracted from each article: the first author, the year of publication, the study location, the number of participants, the characteristics of participants, the number of cases, baseline blood pressure, method of exposure and outcome measurements, the duration of follow-up, the RRs or hazard ratios with corresponding 95% CIs of the incident hypertension for all categories of fruit and/or vegetables consumption (the largest number of covariates in the adjusted model). Risks were estimated from the published beta-coefficients if possible.
Quality assessment
We used the Newcastle-Ottawa quality scale to assess the quality of the included cohorts. A quality of ‘high’ (6–9 points) or ‘low’ (0–6 points) were assigned according to the following domains: the basis of the cohort selection (0–4 points), the comparability of the cohort design and analysis (0–2 points), and the adequacy of the exposure and outcome measurements (0–3 points). Disagreements were resolved by consensus with the third author (He).
Statistical analysis
We calculated the pooled RRs (95% CIs) for the highest compared with the lowest category of fruit and/or vegetables consumption. A generic inverse-variance method with random effects model was used to pool the outcome data. Between-study heterogeneity was examined by the Q-test and I2 statistic; an I2 statistic >50% indicated significant heterogeneity.24 Subgroup analyses and meta-regression were conducted to explore potential sources of heterogeneity by pre-specified characteristics (study location, duration of follow-up, gender, sample size, assessment method of exposure and outcome ascertainment). Sensitivity analysis was performed to estimate the influence of a single study on the overall pooled results by omitting one study at every turn. Begg’s and Egger’s tests were used to evaluate the presence of publication bias.25, 26
Generalized least squares trend estimation model was used to calculate the study-specific slopes for the dose–response analysis based on method reported by Orsini et al.27, 28 We extracted data on all (at least three) categories of total fruit and vegetables intake and fruit or vegetables intake separately, the distribution of cases and person-years, and hazard ratios or RRs with 95% CIs of incident hypertension. Doses reported as gram per day were converted to serving per day, using a standard portion size of 106 g.29 For categories of the fruit and vegetables consumption that were open (for example, 1–2 servings per day), we assigned the median value as the corresponding dose of consumption. If the highest category was open-ended (for example, >2 servings per day), we assumed that the boundary had the same amplitude as the preceding category.30 The dose–response results in the forest plots were presented for every one serving per day increment in fruit and vegetables consumption. We used a four-knot-restricted cubic spline model to test for nonlinearity hypothesis in the association between fruit and vegetables consumption and the incident risk of hypertension. We verified that the regression coefficients of the last two spline transformations both equal to zero (the joint null hypothesis).27, 28 Simple generalized least squares trend estimation model (without the restricted cubic spline model) was used to test the linear hypothesis, if the test for the non-linear association was not statistically significant.
Stata software, version 12.0 (StataCorp LP, College Station, TX, USA) and Review Manager software, version 5.2 (The Nordic Cochrane Centre, Copenhagen, Denmark) were used for the statistical analyses. P-values <0.05 were considered statistically significant.
Results
Study identification and selection
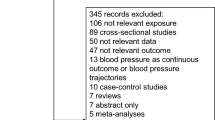
Figure 1 presents the detailed flow diagram of articles included in the present meta-analysis. A total of 1570 articles were identified from the initial database search (Pubmed: 824 articles, Embase: 746 articles). Of those studies, 304 articles were excluded for duplicates. After reading the titles and abstracts, 1233 articles were excluded. The remaining 33 articles were reviewed in full for eligibility. No additional records were identified from the reference lists of included articles. Finally, seven prospective cohort studies which comprised nine independent cohorts were selected for the present meta-analysis.31, 32, 33, 34, 35, 36, 37 One study31 consisted of three separate cohorts, that is, the NHS (Nurses’ Health Study) cohort, the NHSII cohort, and the HPFS (Health Professionals Follow-up Study) cohort, and they were entered as three independent cohorts.

Flow diagram of articles included in the meta-analysis.
Study characteristics
Table 1 shows the main characteristics of the included studies. These studies were published between 2004 and 2015. Three of the included studies were performed in the United States,31, 35, 37 three studies were performed in the European countries (Spain, Greece and Portugal),32, 33, 34 and the other study was conducted in Japan.36 The range of follow-up duration ranged from 3.8 to 28 years. Five articles included both male and female participants,32, 33, 34, 35, 36 and one article included only female participants.37 In an article by Borgi et al.,31 participants in the NHS cohort and the NHSII cohort were women, and the HPFS cohort included only men. The sample size ranged from 549 to 63 885 for a total number of 185 676. The fruit and/or vegetables intake was assessed by food-frequency questionnaire (FFQ) in all articles. The incident of hypertension was diagnosed from self-reported31, 33, 37 or measurement.32, 34, 35, 36 Participants who reported a diagnosis of hypertension at baseline were excluded from the analysis in all included studies. Six of the seven studies included studies reported fruit or vegetables intake separately,31, 33, 34, 35, 36, 37 and four of seven studies reported intake of total fruit and vegetables.31, 32, 33, 37
Quality assessment
All studies met the quality score of 7–8 stars (Supplementary Table 2). The main quality issues were listed as follows. Two articles measured the fruit and vegetables intake by self-administered.36, 37 The diagnosis of hypertension was based on self-reported.31, 33, 37 The follow-up duration was <10 years.32, 33, 34, 36 Two articles did not adjust for potential covariate of BMI.32, 34
Association between fruit or vegetable intake separately, and total fruit and vegetable intake and incident hypertension
Highest vs lowest
Six studies comprised eight cohorts reported an association between fruit or vegetables intake separately and incident risk of hypertension (Figures 2a and b). The highest intake of fruit or vegetables separately was inversely associated with the incident risk of hypertension compared to the lowest level, and the pooled RR and 95% CI was 0.87 (0.79, 0.95) for fruit consumption and 0.88 (0.79, 0.99) for vegetables consumption, both with an evidence of significant heterogeneity among included articles (I2=64% and I2=68%, respectively).

Meta-analysis of the association between (a) fruit, (b) vegetables and (c) total fruit and vegetables consumption (highest vs lowest) and the risk of incident hypertension.
Four studies comprised six cohorts reported an association between total fruit and vegetables intake and incident risk of hypertension. Figure 2c shows that the highest intake of total fruit and vegetables was inversely associated with the incident risk of hypertension compared with the lowest level, and the pooled RR and 95% CI was 0.90 (0.84, 0.98), with an evidence of heterogeneity (I2=68%, P=0.007).
Subgroup analysis and meta-regression
As shown in Table 2, subgroup analysis and meta-regression were performed to explore the potential sources of heterogeneity between fruit or vegetables intake separately, and total fruit and vegetables intake and incident hypertension. Analyses stratified by duration of follow-up (P-value for meta-regression=0.037), gender (P-value for meta-regression=0.017) and method of outcome ascertainment (P-value for meta-regression=0.009) gave some clues to explain the heterogeneity between fruit intake and incident hypertension. Analysis stratified by duration of follow-up (P-value for meta-regression=0.015) might explain the heterogeneity between vegetables intake and incident hypertension. No statistically significant source of heterogeneity was found for the association between total fruit and vegetables consumption and incident hypertension in the subgroup and meta-regression analysis (P>0.05 for each).
Publication bias and sensitivity analysis
As shown in Supplementary Figure 1, visual inspection of the funnel plot suggests an evidence of publication bias among the articles for fruit consumption (Egger’s test, P=0.035; Begg’s test, P=0.009), but not for vegetables consumption (Egger’s test, P=0.108; Begg’s test, P=0.127), and total fruit and vegetables consumption (Egger’s test, P=0.707; Begg’s test, P=0.518). However, the low power with <10 articles limited the interpretability of the finding.22
Further exclusion of any single article did not significantly alter the overall combined RR, which ranged from 0.84 (0.75, 0.93) to 0.90 (0.83, 0.97) for fruit consumption and 0.89 (0.80, 0.98) to 0.92 (0.85, 1.00) for total fruit and vegetables consumption. However, exclusion of an article by Psaltopoulou et al.34 significantly altered the overall combined RR, which ranged from 0.86 (0.74, 0.99) to 0.96 (0.91, 1.02) for vegetables consumption.
Dose–response analysis
After excluding one study32 reported less than three categories of fruit or vegetables consumption separately, and one study34 did not report the detailed data of fruit or vegetables consumption separately, five studies with seven cohorts were included in the dose–response analyses of fruit or vegetables consumption separately and the risk of incident hypertension.31, 33, 35, 36, 37 Four studies31, 32, 33, 37 with six cohorts were included in the dose–response analysis of total fruit and vegetables consumption and the risk of hypertension. The test for the non-linear association between fruit consumption (P for nonlinearity=0.434), vegetables consumption (P for nonlinearity=0.464), and total fruit and vegetables consumption (P for nonlinearity=0.098) and the incident risk of hypertension were not significant. Under the linear hypothesis, a higher consumption of fruit consumption and total fruit and vegetables consumption were significantly associated with a decreased risk of incident hypertension, and the summary RR (95% CI) was 0.981 (0.973, 0.989) and 0.988 (0.985, 0.991), respectively. Vegetables consumption was not associated with incident hypertension, and the summary RR (95% CI) was 1.00 (0.989, 1.011) (Figure 3).

Dose–response association between (a) fruit, (b) vegetables and (c) total fruit and vegetables consumption and the risk of incident hypertension. Solid line, best-fitting restricted cubic spine; dotted line, 95% CI.
Discussion
This meta-analysis identified nine cohorts involving a total of 185 676 participants. The pooled analysis showed that highest level of fruit or vegetables consumption separately and total fruit and vegetables consumption were inversely associated with the occurrence of hypertension after adjustment for potential confounding factors. We also found an inverse dose–response relation between the risk of developing hypertension and fruit intake, and total fruit and vegetables consumption. The incident risk of hypertension was decreased by 1.9% for each serving per day of fruit consumption, and decreased by 1.2% for each serving per day of total fruit and vegetables consumption.
The protective effect of fruit and/or vegetables consumption against hypertension is biologically plausible. Clinical and biological investigations have reported that the micro- and macro-constituents of fruit and vegetables, such as vitamin C, vitamin E, fibre and potassium are effective in lowering blood pressure.38, 39, 40 In consistence with the results of our study, diets rich in plant foods have been demonstrated to lower blood pressure and to reduce the prevalence of hypertension in both normotensive and hypertensive patients.41, 42, 43, 44, 45, 46, 47 No evidence from long-term randomized controlled trials has investigated the effect of fruit consumption and/or vegetables consumption on the prevention of hypertension occurrence, but the Dietary Approaches to Stop Hypertension (DASH) trial has shown that a diet high in fruit and vegetables, low in sodium, and low in saturated and total fat significantly reduced blood pressure.19
The pooled results of our study found that the highest level of vegetables intake was significantly associated with hypertension occurrence compared with the lowest level, but the dose–response analysis showed non-significant result. One possible explanation for the absence of the beneficial effect might be attributed to the added of fats and seasonings (sauce and salt), and the method of cooking (such as deep frying).36, 48 These unhealthy dietary styles might dilute the beneficial effect of vegetables consumption. In addition, the small number of included cohorts might also cause non-significant finding.
A substantial heterogeneity across studies was apparent in our study. Stratified analysis and meta-regression for fruit or vegetables intake separately revealed that the heterogeneity was associated with duration of follow-up, gender and method of outcome ascertainment. The non-significant source of heterogeneity for total fruit and vegetables consumption and incident hypertension may result from other unreported factors, such as different types of fruit and vegetables, various therapy methods of hypertensive patients and statistical model. More studies are warranted to investigate the potential difference in various subgroups.
To the best of our knowledge, this is the first dose–response meta-analysis of prospective cohort studies evaluated the association between fruit and/or vegetables intake and the occurrence of hypertension. We obtained an important finding of the significantly inverse association between fruit or vegetables intake separately, total fruit and vegetables intake and incident hypertension. In addition, we also detected a linear association of hypertension risk with fruit intake and total fruit and vegetables intake, which help to quantify the association and to examine the shape of the possible association. Epidemiological studies have consistently reported that hypertension is one of the important risk factors for various negative health outcomes. Minor changes in blood pressure can have a substantial impact on cardiovascular events.49 Previous meta-analyses have demonstrated the beneficial effects of fruit and/or vegetables on diabetes, cancer, and cardiovascular outcomes12, 13, 50, 51, 52, and these findings were in accordance with our results. Wu et al.12 reported that vegetables and fruit intake linked with a lower risk of type 2 diabetes mellitus. Gan et al.13 demonstrated that fruit or vegetables consumption separately, and total fruit and vegetables consumption were significantly associated with the lower incident of coronary heart disease. Zhan et al.50 provided strong support for the recommendation to consume a higher amount of fruit and vegetables to reduce the risk of cardiovascular disease.
Admittedly, the present meta-analysis has several limitations. First, the finding of a possible publication bias suggested that the pooled RR was probably overestimated. One possible explanation is that several smaller studies showing non-significant association may be underreported in the literature. In addition, the low power with only seven articles limits the interpretability of the finding. Second, most of the included articles were conducted in the western developed countries, and thus our findings seemed difficult to generalise to a broader range of population. Third, the majority of the included studies used the food-frequency questionnaire (FFQ) to assess levels of dietary consumption. Although previous studies have showed that FFQ was a reasonable tool to assess the fruit and vegetables intake, measurement bias might also exist in the present meta-analysis.53 Fourth, the dietary factor is dynamic, changes in fruit and/or vegetables intake may have taken place during the long follow-up periods. Lastly, all of the included studies adjusted for multiple potential confounding variables; however, the possibility of other unmeasured covariates might have affected the results of the present analysis. For example, participants who consumed more fruit and vegetables tend to follow other healthier lifestyles, and thus it is difficult to identify the independent effects of fruit consumption or vegetables consumption separately from other lifestyle and dietary factors.
Conclusions
In conclusion, the results from the present meta-analysis of seven studies comprised nine independent cohorts showed an inverse association between fruit or vegetables consumption separately, and total fruit and vegetable consumption and the incident risk of hypertension. Although the association was statistically significant, the present study is limited by its possible publication bias and its small number of included articles. Our results support the recommendation to increase the consumption of fruit and vegetables with respect to preventing the risk of developing hypertension. However, further large prospective studies and long-term high-quality randomized controlled trials are still needed to confirm the observed association.
References
Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J . Global burden of hypertension: analysis of worldwide data. Lancet 2005; 365 (9455): 217–223.
Meng XJ, Dong GH, Wang D, Liu MM, Lin Q, Tian S et al. Prevalence, awareness, treatment, control, and risk factors associated with hypertension in urban adults from 33 communities of China: the CHPSNE study. J Hypertens 2011; 29 (7): 1303–1310.
Wolf-Maier K, Cooper RS, Banegas JR, Giampaoli S, Hense HW, Joffres M et al. Hypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United States. JAMA 2003; 289 (18): 2363–2369.
Jayalath VH, de Souza RJ, Ha V, Mirrahimi A, Blanco-Mejia S, Di Buono M et al. Sugar-sweetened beverage consumption and incident hypertension: a systematic review and meta-analysis of prospective cohorts. Am J Clin Nutr 2015; 102 (4): 914–921.
Wu Y, Qian Y, Pan Y, Li P, Yang J, Ye X et al. Association between dietary fiber intake and risk of coronary heart disease: a meta-analysis. Clin Nutr 2015; 34 (4): 603–611.
Hu EA, Pan A, Malik V, Sun Q . White rice consumption and risk of type 2 diabetes: meta-analysis and systematic review. BMJ 2012; 344: e1454.
Rong Y, Chen L, Zhu T, Song Y, Yu M, Shan Z et al. Egg consumption and risk of coronary heart disease and stroke: dose-response meta-analysis of prospective cohort studies. BMJ 2013; 346: e8539.
Lairon D, Arnault N, Bertrais S, Planells R, Clero E, Hercberg S et al. Dietary fiber intake and risk factors for cardiovascular disease in French adults. Am J Clin Nutr 2005; 82 (6): 1185–1194.
Hirayama F, Lee AH, Binns CW, Zhao Y, Hiramatsu T, Tanikawa Y et al. Soy consumption and risk of COPD and respiratory symptoms: a case-control study in Japan. Respir Res 2009; 10: 56.
Tielemans SM, Altorf-van der Kuil W, Engberink MF, Brink EJ, van Baak MA, Bakker SJ et al. Intake of total protein, plant protein and animal protein in relation to blood pressure: a meta-analysis of observational and intervention studies. J Hum Hypertens 2013; 27 (9): 564–571.
Wang X, Ouyang Y, Liu J, Zhu M, Zhao G, Bao W et al. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2014; 349: g4490.
Wu Y, Zhang D, Jiang X, Jiang W . Fruit and vegetable consumption and risk of type 2 diabetes mellitus: a dose-response meta-analysis of prospective cohort studies. Nutr Metab Cardiovasc Dis 2015; 25 (2): 140–147.
Gan Y, Tong X, Li L, Cao S, Yin X, Gao C et al. Consumption of fruit and vegetable and risk of coronary heart disease: A meta-analysis of prospective cohort studies. Int J Cardiol 2015; 183: 129–137.
Larsson SC, Virtamo J, Wolk A . Total and specific fruit and vegetable consumption and risk of stroke: a prospective study. Atherosclerosis 2013; 227 (1): 147–152.
Chen Y, Factor-Litvak P, Howe GR, Parvez F, Ahsan H . Nutritional influence on risk of high blood pressure in Bangladesh: a population-based cross-sectional study. Am J Clin Nutr 2006; 84 (5): 1224–1232.
Gadgil MD, Anderson CA, Kandula NR, Kanaya AM . Dietary patterns are associated with metabolic risk factors in South Asians living in the United States. J Nutr 2015; 145 (6): 1211–1217.
Kim MK, Kim K, Shin MH, Shin DH, Lee YH, Chun BY et al. The relationship of dietary sodium, potassium, fruits, and vegetables intake with blood pressure among Korean adults aged 40 and older. Nutr Res Pract 2014; 8 (4): 453–462.
Li B, Li F, Wang L, Zhang D . Fruit and vegetables consumption and risk of hypertension: a meta-analysis. J Clin Hypertens (Greenwich) 2016; 18: 468–476.
Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med 1997; 336 (16): 1117–1124.
Rocha-Goldberg Mdel P, Corsino L, Batch B, Voils CI, Thorpe CT, Bosworth HB et al. Hypertension Improvement Project (HIP) Latino: results of a pilot study of lifestyle intervention for lowering blood pressure in Latino adults. Ethn Health 2010; 15 (3): 269–282.
John JH, Ziebland S, Yudkin P, Roe LS, Neil HA . Effects of fruit and vegetable consumption on plasma antioxidant concentrations and blood pressure: a randomised controlled trial. Lancet 2002; 359 (9322): 1969–1974.
Higgins JPT, Green S (eds). Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 (updated March 2011). Available http://handbook.cochrane.org/.
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000; 283 (15): 2008–2012.
Higgins JP, Thompson SG, Deeks JJ, Altman DG . Measuring inconsistency in meta-analyses. BMJ 2003; 327 (7414): 557–560.
Begg CB, Mazumdar M . Operating characteristics of a rank correlation test for publication bias. Biometrics 1994; 50 (4): 1088–1101.
Egger M, Davey Smith G, Schneider M, Minder C . Biasin meta-analysis detected by a simple, graphical test. BMJ 1997; 315 (7109): 629–634.
Orsini N, Bellocco R, Greenland S . Generalized least squares for trend estimation of summarized dose-response data. Stata J 2006; 6: 40–57.
Orsini N, Li R, Wolk A, Khudyakov P, Spiegelman D . Meta-analysis for linear and nonlinear dose–response relations: examples, an evaluation of approximations, and software. Am J Epidemiol 2012; 175 (1): 66–73.
Carter P, Gray LJ, Troughton J, Khunti K, Davies MJ . Fruit and vegetable intake and incidence of type 2 diabetes mellitus: systematic review and meta-analysis. BMJ 2010; 341: c4229.
Grøntved A, Hu FB . Television viewing and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: a meta-analysis. JAMA 2011; 305 (23): 2448–2455.
Borgi L, Muraki I, Satija A, Willett WC, Rimm EB, Forman JP . Fruit and vegetable consumption and the incidence of hypertension in three prospective cohort studies. Hypertension 2016; 67 (2): 288–293.
Camões M, Oliveira A, Pereira M, Severo M, Lopes C . Role of physical activity and diet in incidence of hypertension: a population-based study in Portuguese adults. Eur J Clin Nutr 2010; 64 (12): 1441–1449.
Nuñez-Cordoba JM, Alonso A, Beunza JJ, Palma S, Gomez-Gracia E, Martinez-Gonzalez MA . Role of vegetables and fruits in Mediterranean diets to prevent hypertension. Eur J Clin Nutr 2009; 63 (5): 605–612.
Psaltopoulou T, Naska A, Orfanos P, Trichopoulos D, Mountokalakis T, Trichopoulou A . Olive oil, the Mediterranean diet, and arterial blood pressure: the Greek European Prospective Investigation into Cancer and Nutrition (EPIC) study. Am J Clin Nutr 2004; 80 (4): 1012–1018.
Steffen LM, Kroenke CH, Yu X, Pereira MA, Slattery ML, Van Horn L et al. Associations of plant food, dairy product, and meat intakes with 15-y incidence of elevated blood pressure in young black and white adults: the Coronary Artery Risk Development in Young Adults (CARDIA) Study. Am J Clin Nutr 2005; 82 (6): 1169–1177.
Tsubota-Utsugi M, Ohkubo T, Kikuya M, Metoki H, Kurimoto A, Suzuki K et al. High fruit intake is associated with a lower risk of future hypertension determined by home blood pressure measurement: the OHASAMA study. J Hum Hypertens 2011; 25 (3): 164–171.
Wang L, Manson JE, Gaziano JM, Buring JE, Sesso HD . Fruit and vegetable intake and the risk of hypertension in middle-aged and older women. Am J Hypertens 2012; 25 (2): 180–189.
Dauchet L, Amouyel P, Hercberg S, Dallongeville J . Fruit and vegetable consumption and risk of coronary heart disease: a meta-analysis of cohort studies. J Nutr 2006; 136 (10): 2588–2593.
Bazzano LA, Serdula MK, Liu S . Dietary intake of fruits and vegetables and risk of cardiovascular disease. Curr Atheroscler Rep 2003; 5 (6): 492–499.
Savica V, Bellinghieri G, Kopple JD . The effect of nutrition on blood pressure. Annu Rev Nutr 2010; 30: 365–401.
Dauchet L, Kesse-Guyot E, Czernichow S, Bertrais S, Estaquio C, Péneau S et al. Dietary patterns and blood pressure change over 5-y follow-up in the SU.VI.MAX cohort. Am J Clin Nutr 2007; 85 (6): 1650–1656.
Masala G, Bendinelli B, Versari D, Saieva C, Ceroti M, Santagiuliana F et al. Anthropometric and dietary determinants of blood pressure in over 7000 Mediterranean women: the European Prospective Investigation into Cancer and Nutrition-Florence cohort. J Hypertens 2008; 26 (11): 2112–2120.
Tielemans SM, Kromhout D, Altorf-van der Kuil W, Geleijnse JM . Associations of plant and animal protein intake with 5-year change in blood pressure: The Zutphen Elderly Study. Nutr Metab Cardiovasc Dis 2014; 24 (11): 1228–1233.
Pettersen BJ, Anousheh R, Fan J, Jaceldo-Siegl K, Fraser GE . Vegetarian diets and blood pressure among white subjects: results from the Adventist Health Study-2 (AHS-2). Public Health Nutr 2012; 15 (10): 1909–1916.
Krupp D, Shi L, Egert S, Wudy SA, Remer T . Prospective relevance of fruit and vegetable consumption and salt intake during adolescence for blood pressure in young adulthood. Eur J Nutr 2015; 54 (8): 1269–1279.
Jiang J, Liu M, Parvez F, Wang B, Wu F, Eunus M et al. Association of major dietary patterns and blood pressure longitudinal change in Bangladesh. J Hypertens 2015; 33 (6): 1193–1200.
Sarri K, Linardakis M, Codrington C, Kafatos A . Does the periodic vegetarianism of Greek Orthodox Christians benefit blood pressure? Prev Med 2007; 44 (4): 341–348.
Anderson CA, Appel LJ, Okuda N, Brown IJ, Chan Q, Zhao L et al. Dietary sources of sodium in China, Japan, the United King dom,and the United States, women and menaged 40 to 59 years: the INTERMAP study. J Am Diet Assoc 2010; 110 (5): 736–745.
MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J et al. Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 1990; 335 (8692): 765–774.
Zhan J, Liu YJ, Cai LB, Xu FR, Xie T, He QQ . Fruit and vegetable consumption and risk of cardiovascular disease: a meta-analysis of prospective cohort studies. Crit Rev Food Sci Nutr, (e-pub ahead of print 26 June 2015; doi:10.1080/10408398.2015.1008980).
Wang M, Qin S, Zhang T, Song X, Zhang S . The effect of fruit and vegetable intake on the development of lung cancer: a meta-analysis of 32 publications and 20,414 cases. Eur J Clin Nutr 2015; 69 (11): 1184–1192.
He FJ, Nowson CA, MacGregor GA . Fruit and vegetable consumption and stroke: meta-analysis of cohort studies. Lancet 2006; 367 (9507): 320–326.
Sauvageot N, Alkerwi A, Albert A, Guillaume M . Use of food frequency questionnaire to assess relationships between dietary habits and cardiovascular risk factors in NESCAV study: validation with biomarkers. Nutr J 2013; 12 (1): 143.
Acknowledgements
This study was supported by research grants from the National Natural Science Foundation of China, 81072355, 81373080; Beijing Municipal Science and Technology Commission, D121100004912003; Military Medicine Innovation Fund, 13CXZ029.
Author contributions
LW and YH were responsible for the conception and design. LW, DS and YH took part in the acquisition, analysis and interpretation of data. All authors have read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on the Journal of Human Hypertension website
Supplementary information
Rights and permissions
About this article

Cite this article
Wu, L., Sun, D. & He, Y. Fruit and vegetables consumption and incident hypertension: dose–response meta-analysis of prospective cohort studies. J Hum Hypertens 30, 573–580 (2016). https://doi.org/10.1038/jhh.2016.44
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhh.2016.44
- Springer Nature Limited
This article is cited by
-
Fruit and vegetable consumption and the risk of hypertension: a systematic review and meta-analysis of prospective studies
European Journal of Nutrition (2023)
-
Association between dietary total antioxidant capacity and hypertension in Iranian Kurdish women
BMC Women's Health (2022)
-
Dietary phytochemical index associated with cardiovascular risk factor in patients with type 1 diabetes mellitus
BMC Cardiovascular Disorders (2021)
-
Predictive value of women’s weight trajectories in determining familial cardiovascular disorders: a family-based longitudinal study
Scientific Reports (2021)
-
Association between dietary acid load and the risk of hypertension among adults from South China: result from nutrition and health survey (2015–2017)
BMC Public Health (2019)