
Abstract
Background:
The association between eating rate and obesity has recently been reported. However, the findings remain inconclusive.
Objectives:
We undertook a systematic review with a meta-analysis of published epidemiological studies to provide a reliable close estimate of the association between eating rate and obesity.
Methods:
A comprehensive search of MEDLINE, EMBASE and CINAHL was conducted to identify studies that reported quantitative estimates for indices of obesity based on the category of eating rate. Interventional studies or studies conducted using children as subjects were excluded. Two independent researchers extracted the data. A summary estimate was calculated using a random-effects model, and subgroup analyses were conducted to identify sources of heterogeneity.
Results:
Data from 23 published studies were eligible for inclusion. The mean difference in body mass indices (BMIs) between individuals who ate quickly and those who ate slowly was 1.78 kg m−2 (95% confidence interval (CI), 1.53–2.04 kg m−2). The pooled odds ratio of eating quickly on the presence of obesity was 2.15 (95% CI, 1.84–2.51). There was evidence of significant quantitative heterogeneity in the magnitudes of the association across studies (I2=78.4%, P-value for heterogeneity <0.001 for BMI, I2=71.9%, P-value for heterogeneity <0.001 for obesity), which may be partially explained by differences in the type of study population (a weaker association was observed for BMI in diabetic patients).
Conclusions:
Eating quickly is positively associated with excess body weight. Further studies are warranted to determine whether interventions to slow the speed of eating are effective for weight control.
Similar content being viewed by others


Introduction
Overweight and obesity in humans have increased globally in both developed and developing countries. Worldwide, the percentage of men with a body mass index (BMI) ⩾25 kg m−2 increased from 28.8% in 1980 to 36.9% in 2013, whereas that of women increased from 29.8 to 38.0% during the same period.1 Similarly, the number of overweight and obese people increased from 857 million in 1980 to 2.1 billion in 2013.1 Given its adverse consequences,2, 3, 4 the obesity epidemic has become a major public health concern. Therefore, a practical and effective strategy for the prevention and treatment of obesity is crucial.
Diet therapy has an important role in the treatment of overweight and obesity. Recommendations on energy balance and macronutrient intake have been established,5 but appropriate eating behaviors for the prevention of obesity remains uncertain. Among eating behaviors, reducing eating rate is frequently advocated as a simple and effective method for control of food intake and thus body weight.6 Several epidemiological studies suggested that eating quickly was associated with an increased prevalence of obesity,7, 8, 9, 10 but their findings remained inconclusive.11, 12 Considering the epidemic and deleterious impact of obesity, a better understanding of the precise nature of the association between eating rate and obesity would be beneficial from both clinical and public healthcare perspectives. Herein, we report the results of a systematic review with a meta-analysis of published epidemiological studies undertaken to obtain a reliable and precise measure for the association between eating rate and obesity.
Materials and methods
Data sources and searches
The Meta-analysis of Observational Studies in Epidemiology guidelines for the conduct of meta-analyses of observational cohort studies were followed.13 Relevant published studies were identified with computerized searches of MEDLINE via Ovid (from 1946 through September 2014), EMBASE (from 1966 through September 2014), and CINAHL (from 1987 through September 2014) databases using relevant text words and medical subject headings, including all spellings of ‘eating rate,’ ‘eating speed,’ ‘eating time,’ ‘slow eating,’ ‘quick eating,’ ‘fast eating’ and ‘rapid eating’ and these words combined with all spellings of ‘body mass index,’ ‘body weight’ and ‘obesity’ (See Supplementary Appendix). The search was limited to cross-sectional studies, case-control studies and cohort studies without language restrictions. The reference lists from identified articles were manually scanned to identify other relevant studies.
Study selection and data extraction
Studies were included if they reported quantitative estimates and standard errors (SEs; or 95% confidence intervals (CIs)) of indices of obesity according to a category of some measure of eating rate, namely, the mean value of or the change in body weight or BMI, the frequency of obesity, the odds ratio (OR) for the presence of obesity or the relative risk for the development of obesity. The definition of eating rate was based on that presented in each study. Obesity was defined as BMI⩾25 kg m−2 in all included studies. Studies were excluded if they met the following criteria: (1) an interventional study; (2) a study population that included children; and (3) a study reporting the estimate of an effect without the ability to derive the SE. Two authors (TO and TN) independently conducted the literature search and data extraction using a standardized approach. Any discrepancies regarding eligibility or quality of a study were resolved by consensus after a third author (YH) reviewed the paper.
Statistical analysis
The difference in the mean values of BMI (or body weight) and the ORs for the presence of obesity in the categories for the fastest versus slowest eating rates were calculated for each study. Summary estimates of the mean difference or the OR, and their 95% CIs, were obtained using a random-effects model. Multiple estimates of subgroups (for example, sex or diabetes status) from one study8, 10, 14, 15, 16, 17, 18 were combined using a fixed-effects model to create a single pairwise comparison.19 Heterogeneity across the included studies was analyzed using Cochran’s Q test and the I2 statistic, which approximates the proportion of total variation in the estimates caused by between-study heterogeneity. The possible sources of heterogeneity were investigated by comparing the summary results obtained from subsets of studies grouped by the characteristics of the included studies. Tests of heterogeneity between subgroups were estimated using a meta-regression analysis. Graphic representations of the potential publication bias were generated using a funnel plot of the mean differences or natural logarithms of the ORs versus their SEs and were assessed visually as well as using Egger’s test and Begg’s test, which performed a linear regression and a rank correlation between the observed effect estimates and observed standard errors for the statistical evaluation of funnel plot asymmetry, respectively. A two-sided P-value of <0.05 was considered statistically significant for all analyses. All analyses were performed using Stata software (release 13; StataCorp, College Station, TX, USA).
Results
Literature search and characteristics of included studies
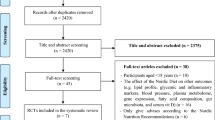
A flow chart detailing the process of study identification and selection is shown in Figure 1, and characteristics of the included studies are listed in Table 1. The literature search yielded 3925 articles, of which 61 were reviewed in full. Finally, 23 published studies7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31 were eligible for inclusion in the analysis, of which 20 were cross-sectional studies,7, 8, 9, 10, 11, 14, 15, 16, 17, 18, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30 two were longitudinal studies20, 31 and one provided results from both study designs.26 The eating rate was evaluated using self-reporting in 22 studies 7, 8, 9, 10, 11, 14, 15, 16, 17, 18, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31 and using an eating monitor in one study.12 In one study, the data from only male subjects were included in the analysis, because no data from female subjects were reported.22 Seventeen studies7, 8, 10, 14, 15, 16, 17, 20, 22, 23, 24, 25, 26, 27, 29, 30, 31 provided an estimate of the association between eating rate and indices of excess body weight that was adjusted for confounding factors, whereas six studies9, 11, 12, 18, 21, 28 reported the unadjusted analysis.

Identification process for eligible studies.
Association of eating rate with BMI: cross-sectional study
Fifteen cross-sectional studies7, 9, 10, 11, 12, 14, 17, 18, 22, 25, 26, 27, 28, 29, 30 investigated the association between eating rate and the mean value of BMI, 12 of which were included in the meta-analysis. Subjects eating quickly had a significantly higher mean value of BMI than those eating slowly: the pooled estimate of the mean differences in BMIs between those eating quickly and slowly was 1.78 kg m−2 (95% CI, 1.53–2.04 kg m−2; Figure 2a). There was evidence of significant heterogeneity in the magnitudes of the associations across the included studies (I2=78.4%, P-value for heterogeneity<0.001), although all point estimates were located on the right side of the forest plot. The sensitivity analysis excluding two studies that used medium eating rate as a reference group14, 27 had little effect on the finding, although the heterogeneity in the association across the studies was attenuated: a pooled mean difference in BMI of 1.92 kg m−2 (95% CI, 1.71–2.13 kg m−2; I2=58.0%, P-value for heterogeneity=0.01).

Forest plot of the mean differences in BMIs (a) and the odds ratios for obesity (b) in association with eating rate. CI, confidence interval.
Three studies11, 12, 25 were excluded from the meta-analysis because they had no available data: two studies11, 12 provided correlation coefficients between eating rate and BMI or body weight that were not significant, and one study25 revealed a positive association between eating rate and BMI (Table 2A).
Association of eating rate with obesity: cross-sectional study
Ten studies8, 9, 10, 15, 16, 17, 21, 23, 24, 26 reported on the association of eating rate with the presence of obesity. After excluding one study that did not report the value of the OR and its 95% CI,17 the remaining nine studies were included in the meta-analysis. All of the included studies demonstrated that eating quickly was significantly associated with a greater likelihood of obesity, but the magnitude of the association was heterogeneous across the studies (I2=71.9%, P value for heterogeneity<0.001; Figure 2b). The pooled OR for eating quickly with the presence of obesity was 2.15 (95% CI, 1.84–2.51).
Subgroup analysis
The subgroup analysis indicated that the type of study population was one of the sources for between-study heterogeneity in the association between a faster eating rate and a higher mean BMI (Figure 3a); the mean difference in BMI from the 3 studies having participants with diabetes was lower than that in the 11 studies having participants without diabetes (mean difference 1.32 kg m−2 (95% CI, 0.90–1.74 kg m−2) versus mean difference 1.89 kg m−2 (95% CI, 1.64–2.15 kg m−2), respectively; P value for heterogeneity=0.038). In the subgroup analysis for the presence of obesity, however, no significant heterogeneity in the association between types of study population was detected (Figure 3b). There was no evidence for a significant difference in the association between subgroups of sex, level of adjustment, adjustment for energy intake or number of participants (Figures 3a and b).

Subgroup analysis for the association of eating rate with BMI (a) and the odds ratio for obesity (b) based on study characteristics. CI, confidence interval.
Publication bias
A funnel plot showed a symmetric pattern (Figures 4a and b), without significant evidence of the presence of publication bias in statistical tests for funnel plot asymmetry (for BMI: Egger’s test P=0.08, Begg’s test P=0.68; for obesity: Egger’s test P=0.22, Begg’s test P=0.17).

Funnel plot of the mean differences in BMIs versus the standard errors (a) and the natural logarithms of the odds ratios for obesity versus the standard error (b) OR, odds ratio; SE, standard error.
Association of eating rate with obesity: longitudinal study
Three studies longitudinally examined the association of eating rate with the increase in body weight20, 26 and the risk of developing obesity.31 Gerace et al.20 found that firefighters who ate faster at the station than elsewhere gained 9.9 pounds over 7 years, whereas firefighters with a constant eating speed gained 6.8 pounds (P<0.006). This relationship persisted after adjustment for race/ethnicity, smoking status, age, percentage of ideal weight, marital status and worry over financial security. Tanihira et al.26 reported that after adjusting for confounders, participants eating quickly gained 1.10 kg (95% CI, 0.23–1.97 kg) more over 8 years than those eating moderately and slowly. Yamane et al.31 showed that fast eating was significantly associated with an increased risk of developing obesity in a 3-year follow-up study conducted in Japanese university students (OR, 4.40; 95% CI, 2.22–8.75; Table 2B).
Discussion
In the present meta-analysis, we showed a significant positive association between eating quickly and excess body weight. People who ate quickly were shown to have a significantly higher BMI and to be obese. This relationship was consistent for several subgroups, including sex, level of adjustment, adjustment for energy intake and number of participants, whereas the magnitude of the association between eating speed and BMI was weaker in individuals with diabetes than in those without the disease. These findings highlight that the speed of eating is an important factor for weight control.
There are several plausible pathophysiologic mechanisms to explain the association between eating quickly and excess body weight. Several epidemiologic studies7, 14, 17, 28, 30 and a recent meta-analysis32 showed that people who ate quickly tended to have more energy intake than those who ate slowly. This may be because fast eaters ingest more energy before the brain recognizes the satiety signal, which is triggered by nutrient ingestion, gastric distension and the release of gut factors, including cholecystokinin.33 Lower postprandial levels of the anorexigenic gut hormones peptide YY and glucagon-like peptide-1 after a meal short in duration34 may also contribute to the association. However, the results of our subgroup analysis with an adjustment for energy intake did not indicate significant heterogeneity (Figures 3a and b), which suggests the presence of a mechanism other than energy intake. Another plausible explanation for the association between eating quickly and excess body weight may be a decrease in mastication in the fast eaters and subsequent inactivation of neuronal histamine. In rats, activation of histamine neurons suppressed food intake physiologically through H1-receptors in the satiety centers.35 In addition, histamine neuronal activation accelerated lipolysis, particularly in visceral adipose tissue, and upregulated gene expression for the uncoupling protein family through sympathetic efferent nerves.35
In the present study, there was evidence of heterogeneity in the magnitude of the association between eating rate and BMI and the OR for obesity across the included studies. One potential source for this heterogeneity may be the differences in the definition of the categories of eating rates among the included studies. For example, the sensitivity analysis excluding two studies that used medium eating rate as a reference group reduced the heterogeneity in the association among the studies. In the subgroup analysis, we found significant heterogeneity in the association of eating rate with the mean differences in BMIs between groups of diabetes status. Studies conducted with diabetic patients showed a weaker association than those conducted with nondiabetic individuals. However, this is likely owing to chance because no difference was observed in the OR for the presence of obesity between diabetes statuses, although impaired insulin secretion in diabetic patients36 may also account for the association. The obesogenic effect of eating quickly may be weakened in diabetic patients because of the decreased anabolic action of insulin. Thus, we could not clarify the source of the heterogeneity in this study. Nevertheless, this heterogeneity does not alter our conclusion because heterogeneity was related only to the strength of the positive association and not with the direction of this association.
The strengths of the present review are its inclusion of a large number of participants, immediate applicability to a clinical question, and clear results. The findings have direct implications for the clinical management of weight control, highlighting the importance of how to eat in addition to the traditional dietary instructions for what and how much to eat. Some limitations of our study should be noted. First, eating rate was evaluated using a self-reported questionnaire in most of the included studies. However, a high level of concordance between self-reported eating rate and friend-reported eating rate as a standard has been demonstrated.7 Other validation studies also indicated a correlation of self-reported eating rate with measured eating rate in the laboratory37 and recalled duration of eating.38 Second, most studies included in this review were conducted with a Japanese population. Considering the difference in dietary habits across racial or regional backgrounds, the generalizability of the current findings may be limited. In addition, the present studies focused on the influence of eating speed on obesity in adults, but recent cross-sectional and longitudinal studies conducted in children have also shown a positive association between eating fast and childhood obesity.39, 40 Further studies to ascertain the association in other races and children may be needed. Third, all the studies included in the meta-analysis were from cross-sectional studies, which do not allow the deduction of causal relationships. However, three longitudinal studies showed that a faster eating rate was associated with increased BMI and a higher risk of obesity over time. In addition, a prior randomized controlled trial retraining eating behavior to slow the speed of eating and reduce portion size was beneficial for weight reduction.41 Further longitudinal observational studies or randomized controlled trials will be required to test the causal relationship. Fourth, the definitions of the categories for the eating rate differed across the studies included in this analysis, which may be a source of heterogeneity in the association. Fifth, we could not include two studies reporting no significant correlation between eating rate and BMI in the analysis.11, 12 Excluding these studies may tend toward biasing an overestimation of the association. However, these two limitations are unlikely to change our conclusion, because almost all included studies showed a positive association between eating rate and BMI, and the two excluded studies had much smaller sample sizes than those in the included studies. Finally, there may be other unmeasured confounding factors in addition to those evaluated in the present meta-analysis.
In conclusion, the findings of the present meta-analysis clearly showed that eating quickly was associated with increased BMI and obesity. This study provides a critical contribution to weight-management practices because the importance of how to eat was clearly demonstrated, adding to prior evidence regarding what and how much to eat. Instructions to eat slowly may be widely efficacious because of the simple nature of this weight-management practice both in public health and clinical settings. Although further interventional studies are needed to conclude a causal relationship between eating rate and obesity, more emphasis may be placed in clinical practice on slowing the speed of eating.
Author contributions
TO and TN designed and conducted the research, analyzed the data and wrote the paper. YH, UN, YK and TK helped with the data interpretation, contributed to the discussion and revised the paper. TN had primary responsibility for the final content of the manuscript. All authors participated in critically revising and approving the final manuscript.
References
Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014; 384: 766–781.
Bogers RP, Bemelmans WJ, Hoogenveen RT, Boshuizen HC, Woodward M, Knekt P et al. Association of overweight with increased risk of coronary heart disease partly independent of blood pressure and cholesterol levels: a meta-analysis of 21 cohort studies including more than 300 000 persons. Arch Intern Med 2007; 167: 1720–1728.
Strazzullo P, D'Elia L, Cairella G, Garbagnati F, Cappuccio FP, Scalfi L . Excess body weight and incidence of stroke: meta-analysis of prospective studies with 2 million participants. Stroke 2010; 41: e418–e426.
Flegal KM, Kit BK, Orpana H, Graubard BI . Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA 2013; 309: 71–82.
Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014; 129: S102–S138.
Bellack AS . Behavior therapy for weight reduction. Addict Behav 1975; 1: 73–82.
Sasaki S, Katagiri A, Tsuji T, Shimoda T, Amano K . Self-reported rate of eating correlates with body mass index in 18-y-old Japanese women. Int J Obes Relat Metab Disord 2003; 27: 1405–1410.
Maruyama K, Sato S, Ohira T, Maeda K, Noda H, Kubota Y et al. The joint impact on being overweight of self reported behaviours of eating quickly and eating until full: cross sectional survey. BMJ 2008; 337: a2002.
Sakurai M, Nakamura K, Miura K, Takamura T, Yoshita K, Nagasawa SY et al. Self-reported speed of eating and 7-year risk of type 2 diabetes mellitus in middle-aged Japanese men. Metabolism 2012; 61: 1566–1571.
Ohkuma T, Fujii H, Iwase M, Kikuchi Y, Ogata S, Idewaki Y et al. Impact of eating rate on obesity and cardiovascular risk factors according to glucose tolerance status: the Fukuoka Diabetes Registry and the Hisayama Study. Diabetologia 2013; 56: 70–77.
Mochizuki K, Misaki Y, Miyauchi R, Takabe S, Shimada M, Kuriki K et al. A higher rate of eating is associated with higher circulating interluekin-1beta concentrations in Japanese men not being treated for metabolic diseases. Nutrition 2012; 28: 978–983.
Kral JG, Buckley MC, Kissileff HR, Schaffner F . Metabolic correlates of eating behavior in severe obesity. Int J Obes Relat Metab Disord 2001; 25: 258–264.
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000; 283: 2008–2012.
Otsuka R, Tamakoshi K, Yatsuya H, Murata C, Sekiya A, Wada K et al. Eating fast leads to obesity: findings based on self-administered questionnaires among middle-aged Japanese men and women. J Epidemiol 2006; 16: 117–124.
Hsieh SD, Muto T, Murase T, Tsuji H, Arase Y . Eating until feeling full and rapid eating both increase metabolic risk factors in Japanese men and women. Public Health Nutr 2011; 14: 1266–1269.
Ekuni D, Furuta M, Tomofuji T, Irie K, Azuma T, Iwasaki Y et al. Effects of eating behaviors on being overweight in japanese university students: a cross-sectional survey at the Okayama University. Asia Pac J Public Health 2013; 25: 326–334.
Lee KS, Kim DH, Jang JS, Nam GE, Shin YN, Bok AR et al. Eating rate is associated with cardiometabolic risk factors in Korean adults. Nutr Metab Cardiovasc Dis 2013; 23: 635–641.
Nagahama S, Kurotani K, Pham NM, Nanri A, Kuwahara K, Dan M et al. Self-reported eating rate and metabolic syndrome in Japanese people: cross-sectional study. BMJ open 2014; 4: e005241.
Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 March 2011. Available from: http://handbook.cochrane.org/front_page.htm (accessed on 1 October 2014).
Gerace TA, George VA . Predictors of weight increases over 7 years in fire fighters and paramedics. Prev Med 1996; 25: 593–600.
Shigeta H, Shigeta M, Nakazawa A, Nakamura N, Yoshikawa T . Lifestyle, obesity, and insulin resistance. Diabetes Care 2001; 24: 608.
Takayama S, Akamine Y, Okabe T, Koya Y, Haraguchi M, Miyata Y et al. Rate of eating and body weight in patients with type 2 diabetes or hyperlipidaemia. J Int Med Res 2002; 30: 442–444.
Nishitani N, Sakakibara H, Akiyama I . Eating behavior related to obesity and job stress in male Japanese workers. Nutrition 2009; 25: 45–50.
Kimura Y, Nanri A, Matsushita Y, Sasaki S, Mizoue T . Eating behavior in relation to prevalence of overweight among Japanese men. Asia Pac J Clin Nutr 2011; 20: 29–34.
Leong SL, Madden C, Gray A, Waters D, Horwath C . Faster self-reported speed of eating is related to higher body mass index in a nationwide survey of middle-aged women. J Am Diet Assoc 2011; 111: 1192–1197.
Tanihara S, Imatoh T, Miyazaki M, Babazono A, Momose Y, Baba M et al. Retrospective longitudinal study on the relationship between 8-year weight change and current eating speed. Appetite 2011; 57: 179–183.
Saito A, Kawai K, Yanagisawa M, Yokoyama H, Kuribayashi N, Sugimoto H et al. Self-reported rate of eating is significantly associated with body mass index in Japanese patients with type 2 diabetes. Japan Diabetes Clinical Data Management Study Group (JDDM26). Appetite 2012; 59: 252–255.
Mochizuki K, Miyauchi R, Hariya N, Misaki Y, Kasezawa N, Tohyama K et al. Self-reported rate of eating is associated with higher circulating ALT activity in middle-aged apparently healthy Japanese men. Eur J Nutr 2013; 52: 985–990.
Mochizuki K, Hariya N, Miyauchi R, Misaki Y, Ichikawa Y, Goda T . Self-reported faster eating associated with higher ALT activity in middle-aged, apparently healthy Japanese women. Nutrition 2014; 30: 69–74.
Mochizuki K, Yamada M, Miyauchi R, Misaki Y, Kasezawa N, Tohyama K et al. Self-reported faster eating is positively associated with accumulation of visceral fat in middle-aged apparently healthy Japanese men. Eur J Nutr 2014; 53: 1187–1194.
Yamane M, Ekuni D, Mizutani S, Kataoka K, Sakumoto-Kataoka M, Kawabata Y et al. Relationships between eating quickly and weight gain in Japanese university students: A longitudinal study. Obesity 2014; 22: 2262–2266.
Robinson E, Almiron-Roig E, Rutters F, de Graaf C, Forde CG, Tudur Smith C et al. A systematic review and meta-analysis examining the effect of eating rate on energy intake and hunger. Am J Clin Nutr 2014; 100: 123–151.
Morton GJ, Cummings DE, Baskin DG, Barsh GS, Schwartz MW . Central nervous system control of food intake and body weight. Nature 2006; 443: 289–295.
Kokkinos A, le Roux CW, Alexiadou K, Tentolouris N, Vincent RP, Kyriaki D et al. Eating slowly increases the postprandial response of the anorexigenic gut hormones, peptide YY and glucagon-like peptide-1. J Clin Endocrinol Metab 2010; 95: 333–337.
Sakata T, Yoshimatsu H, Masaki T, Tsuda K . Anti-obesity actions of mastication driven by histamine neurons in rats. Exp Biol Med (Maywood) 2003; 228: 1106–1110.
DeFronzo RA, Bonadonna RC, Ferrannini E . Pathogenesis of NIDDM. A balanced overview. Diabetes Care 1992; 15: 318–368.
Petty AJ, Melanson KJ, Greene GW . Self-reported eating rate aligns with laboratory measured eating rate but not with free-living meals. Appetite 2013; 63: 36–41.
Oshida H, Muneyuki T, Suwa K, Nakajima K . Potential relationship between self-assessed eating speed and recalled duration of eating meals in apparently healthy adults. Br J Med Med Res 2013; 4: 257–262.
Llewellyn CH, van Jaarsveld CH, Boniface D, Carnell S, Wardle J . Eating rate is a heritable phenotype related to weight in children. Am J Clin Nutr 2008; 88: 1560–1566.
Berkowitz RI, Moore RH, Faith MS, Stallings VA, Kral TV, Stunkard AJ . Identification of an obese eating style in 4-year-old children born at high and low risk for obesity. Obesity 2010; 18: 505–512.
Ford AL, Bergh C, Sodersten P, Sabin MA, Hollinghurst S, Hunt LP et al. Treatment of childhood obesity by retraining eating behaviour: randomised controlled trial. BMJ 2010; 340: b5388.
Acknowledgements
This study was supported in part by Health and Labour Sciences Research Grants: Research on Food Safety (Study for Yusho; H24-Designated Research-014).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on International Journal of Obesity website
Supplementary information
Rights and permissions
About this article

Cite this article
Ohkuma, T., Hirakawa, Y., Nakamura, U. et al. Association between eating rate and obesity: a systematic review and meta-analysis. Int J Obes 39, 1589–1596 (2015). https://doi.org/10.1038/ijo.2015.96
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijo.2015.96
- Springer Nature Limited
This article is cited by
-
Eating behaviors and depressive symptoms among Japanese workers: the Furukawa Nutrition and Health Study
European Journal of Clinical Nutrition (2024)
-
Ultra-processed Food and Obesity: What Is the Evidence?
Current Nutrition Reports (2024)
-
Eating speed and abdominal adiposity in middle-aged adults: a cross-sectional study in Vietnam
BMC Public Health (2023)
-
The prevalence and determinant of overweight and obesity among residents aged 40–69 years in high-risk regions for upper gastrointestinal cancer in southeast China
Scientific Reports (2023)
-
Mindful Eating as a Tool for Diabetes Prevention and Management: A Review of Potential Mechanisms of Action
Mindfulness (2023)