
Abstract
Background/Objectives:
Multiple studies have revealed an interaction between a variant in the FTO gene and self-reported physical activity on body mass index (BMI). Physical inactivity, such as time spent sitting (TSS) has recently gained attention as an important risk factor for obesity and related diseases. It is possible that FTO interacts with TSS to affect BMI, and/or that FTO’s putative effect on BMI is mediated through TSS.
Subjects/Methods:
We tested these hypotheses in two cohorts of the Framingham Heart Study (FHS) (Offspring: n=3430 and Third Generation: n=3888), and attempted to replicate our results in the Women’s Health Initiative (WHI; n=4756). Specifically, we examined whether an association exists between FTO and self-reported TSS, and whether an interaction exists between FTO and TSS on BMI, while adjusting for several important covariates such as physical activity.
Results:
In FHS, we find a significant positive association between the BMI-increasing FTO allele and TSS. We find a similar trend in WHI. Mediation analyses suggest that the effect of FTO on BMI is mediated through TSS. In FHS, we find a significant interaction of FTO and TSS on BMI, whereby the association of TSS with BMI is greatest among those with more FTO risk alleles. In WHI, we also find a significant interaction, although the direction is opposite to that in FHS. In a meta-analysis of the two data sets, there is no net interaction of FTO with TSS on BMI.
Conclusions:
Our study suggests that FTO exerts its effect on BMI, at least partly, through energy expenditure mechanisms such as TSS. Further research into the intersection of genetics, sedentary behavior and obesity-related outcomes is warranted.
Similar content being viewed by others

Introduction
Obesity, a major worldwide health problem, arises due to both genetic and environmental risk factors.1 A variant in the fat mass and obesity associated (FTO) gene is the most well-established genetic risk factor for obesity.2, 3 The exact mechanism through which this variant is linked to obesity is still unknown, although there is some indication that it involves the hypothalamus, and thus potentially operates through energy expenditure and/or food intake.4, 5, 6, 7, 8
Interaction analyses of FTO and physical activity (PA) have suggested that the putative effect of the FTO variant is diminished among individuals who are more physically active.9, 10 Although PA is an important lifestyle factor, another important factor that has received only recent attention is physical inactivity, such as time spent sitting (TSS).11, 12 Prolonged and sustained sitting behavior has been identified as an independent risk factor for metabolic and cardiovascular disease,13 possibly by deactivating large postural muscles of the back and legs,14 leading to decreased lipoprotein lipase activity.15, 16
Despite the growing recognition of physical inactivity as an important risk factor for obesity and related diseases, little is known regarding how it may be linked to FTO as either (1) a potential mechanism connecting FTO to obesity, or (2) a modifier of the putative effect of FTO variation as has been discovered in the case of PA. Several studies have examined the interaction of body mass index (BMI)-associated genetic variants with sedentary behavior. Qi et al.17 examined the interaction of overall genetic risk to obesity and television watching, and found that the association of genetic risk with obesity was accentuated among those who spent more time watching television. Graff et al.18 found two BMI-associated single nucleotide polymorphisms (SNPs) that interacted with screen time behavior, such that the association of these SNPs with BMI was accentuated among those who engaged in more screen time.
Although television watching is often used as a proxy for sedentary behaviors, this variable does not fully capture total daily sitting time. TSS is an important and comprehensive lifestyle risk factor which has not yet been assessed directly in a genetic interaction study. Furthermore, the extent to which FTO may be associated with TSS, and thus potentially mediate the FTO-BMI association, has not been examined. Here, we tested the association of FTO with TSS, and the interaction of FTO with TSS on BMI in two studies, and in multiple ethnic/racial groups. We also use mediation analysis to determine the extent to which TSS mediates the association between FTO and BMI.
Methods
Studies
We used data from 7318 European-American participants from the Offspring (Exam 4; n=3430) and Third Generation (exam 1; n=3888) cohorts of the Framingham Heart Study (FHS), which is a prospective cohort study to examine the causes of heart disease.19 The Offspring cohort initiated in 1971 includes the offspring of the Original cohort participants as well as the spouses of the offspring.20 Third Generation participants includes children of the Offspring cohort participants as well as their spouses.21 Our replication data set consisted of 4756 participants in the Women’s Health Initiative (WHI) study.22 Of these, 1542 are self-identified Hispanic-Americans (HA) and 3214 are self-identified African-Americans (AA). Based on the assumptions of our model described below, we have over 80% statistical power to detect an effect of FTO on a phenotype with an r2 as low as 0.35%, with a total sample size of 4000, at an alpha of 0.05. An r2 of 0.35% corresponds to the proportion of BMI variation explained by FTO among individuals of European descent.3 We have no a priori expectation regarding the proportion of variation in TSS that variation in FTO might explain. Approval for this study was obtained from the University of Arizona Institutional Review Board. Data were obtained from the database of Genotypes and Phenotypes.
Phenotypic and lifestyle measurements
BMI was measured at baseline as weight (kg) divided by squared height (m). TSS in FHS was measured through the following question: ‘Number of hours typically sitting in a typical day?’ In WHI, TSS was measured through the following question: ‘During a usual day and night, about how many hours do you spend sitting? Include the time you spend sitting at work, sitting at the table eating, driving or riding in a car or bus, and sitting up watching TV or talking.’ In WHI, TSS was recorded as one of eight categories ranging from <4 h to >16 h, with the rest being in 1-h increments. We chose the mean for each time-interval category for the purpose of our analyses. PA in FHS was measured using a questionnaire assessing the number of hours spent in slight, moderate and heavy PA on a typical day. As previously described,23 the slight, moderate and heavy activity were further multiplied by factors of 1.5, 2.4 and 5, respectively, to account for the contribution of these levels of PA in enhancing cardiovascular disease-free life expectancy in adults aged >50 years. These quantities were subsequently summed to create an overall measure of PA in FHS. In WHI, PA was derived by summing metabolic equivalent-hours per week of energy expenditure in mild, moderate and hard exercise activity. Examples of each of these types of activities were provided in the questionnaire. Metabolic equivalent-hours per week were calculated as the summed product of the frequency, duration and intensity of reported activities.24, 25 The intensity of the activity was assigned according to a standardized classification.26 Dietary intake was assessed in WHI through estimation of the amount of total dietary energy consumed (Kcal per day) on a normal day. Employment was dichotomized in both FHS (Third Generation) and WHI to reflect the current employment status of each individual (0 if not employed, 1 if employed). Education was recoded into years of education in FHS (Third Generation) and WHI. Cigarette smoking in both data sets was dichotomized to reflect any current or past smoking. Individuals with any missing values for the above variables were excluded from the analyses.
FTO genotype
We used a common variant, rs9939609 (A/T) repeatedly identified in many BMI genome-wide association studies in European-American and AA.27, 28, 29 Given the lack of association of the rs9939609 SNP in some studies of AA,30 we also considered other SNPs identified in fine-mapping efforts in AA: rs1421085, rs56137030, rs17817964 and rs8050136.31, 32 Genotyping was originally performed using the Affymetrix 500 SNP Array in FHS, and the Affymetrix 6.0 SNP Array in WHI (Affymetrix Inc., Santa Clara, CA, USA). In WHI, the DNA was extracted from blood samples collected at enrollment, and genotyping QC included concordance rates for blinded and unblended duplicates.33 To test multiple FTO SNPs in WHI, we used imputed genotypes that were available in the database of Genotypes and Phenotypes. In brief, genotypes were imputed using BEAGLE software,34 and 1000 Genomes data35 as reference. Individuals with missing values of FTO genotypes were excluded from all analyses.
Statistical analyses
For our main analysis, we used the rs9939609 FTO SNP. However, other genetic variants listed above were also tested and showed similar results. The rs9939609 was chosen to maintain consistency across studies. Linear multiple regression models were used to assess the association between (i) rs9939609 and BMI, adjusting for age, gender, smoking and PA. (ii) rs9939609 and TSS, adjusting for age, gender, BMI, smoking and PA. These models were also run in our replication data set of AA and HA in WHI, where we also adjusted for dietary intake. The distributions of all variables were visually examined to ensure no departure from normality. In WHI and the FHS Third Generation cohort, we also included employment and education as covariates. We performed a random-effects, inverse-variance weighted, meta-analysis of the association of rs9939609 with TSS, as well as for the interaction of rs9939609 with TSS, to combine estimates from FHS and WHI, using the metafor package in R.36 We also examined the possible mediation effect of TSS and PA on the association between rs9939609 and BMI, by performing a causal mediation analysis using the ‘mediation’ package in R.37 We included all covariates mentioned above in this analysis, and we included them additively, which is under the model assumption. Mediation analysis was carried out using a least squares regression to statistically test for the indirect effect or average causal mediation effect of TSS and PA (tested separately) on the association of rs9939609 with BMI, and of BMI on the association of rs9939609 with TSS. A non-parametric bootstrap (simulations=1000) method was adopted to estimate parameter uncertainty. A sensitivity analysis was also conducted on the significant mediation results obtained in European-American, with age, sex, PA, smoking and cohort type as covariates. Lastly, we also tested the interaction of TSS and rs9939609 on BMI by including in the regression model the product of these two variables. All analyses were conducted using R software (version 3.0.238) and two sided P-values <0.05 were considered statistically significant.
Results
Descriptive characteristics of the sample are shown in Table 1. The mean age of FHS participants is lower (mean≈45) than that of participants in WHI (mean≈61). Mean BMI is highest among AA in WHI (mean=30.1 kg m−2). The frequency of the rs9939609-A allele does not differ greatly across racial/ethnic groups (Table 1).
Association of rs9939609 with BMI and TSS
We first confirmed that the A allele of rs9939609 is associated with a higher BMI, after adjustment for age, sex and PA in the combined FHS (P=2.07 × 10−7) and WHI HA (P=8.79 × 10−3). Among AA, we do not observe a significant association of this allele with BMI (P=0.95; Table 2). The regression coefficient of rs9939609 with BMI is slightly smaller upon including TSS in the model (0.43 and 0.48 before inclusion of TSS, and 0.41 and 0.45 after inclusion of TSS, in the FHS Offspring and FHS Third Generation, respectively). In this same latter model, we also find that TSS is positively associated with BMI (P<1 × 10−6) in FHS. In WHI, the inclusion of TSS in the model with BMI as the outcome results in a decreased coefficient for rs9939609 in AA (0.01, before TSS inclusion vs −0.11, after TSS inclusion), but an increased coefficient in HA (0.39 vs 0.74). In the latter model, TSS is positively associated with BMI (P<1 × 10−6) in WHI.
The A allele is also associated with greater TSS in the combined FHS (P=9.94 × 10−4) after adjustment for multiple covariates, including BMI. In the combined WHI data set, we find a trend suggesting that the A allele is positively associated with TSS, although the association is not quite statistically significant (P=0.08), adjusting for all covariates, including employment and education (Table 2). The meta-analyzed estimate of the rs9939609 association with TSS shows a significant positive association of rs9939609 with TSS (β=0.11, P=2.3 × 10−4), as shown in Table 2.
Mediation analysis revealed that the association of rs9939609 with BMI is partly mediated by TSS in FHS (P=0.02 and P=0.03, respectively in Offspring and Third Generation), but not by PA (P=0.78 and P=0.85, respectively in Offspring and Third Generation; Tables 3 and 4). In WHI, we find a similar trend, although the results are not statistically significant (Tables 3 and 4). Table 5 shows the results of the mediation by BMI of rs9939609 on TSS. BMI appears to partly mediate the association between rs9939609 and TSS, although there also appears to be a direct effect of rs9939609 on TSS. As above, the results are stronger in FHS than in WHI.
Interaction of rs9939609 and TSS
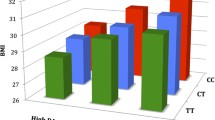
As shown in Table 6, we find a significant interaction of rs9939609 and TSS on BMI in both FHS (P=3.4 × 10−3) and WHI Hispanics (P=0.02). In FHS, the association of TSS with BMI is strongest among those homozygous for the rs9939609 risk allele (Table 7). Conversely, the association of rs9939609 with BMI is strongest among those with high TSS, and weakest among those with low TSS. However, in WHI, we observed the opposite pattern of interaction whereby the association of TSS with BMI is strongest among those homozygous for the rs9939609 protective allele. As shown in Table 6, upon meta-analysis of the interaction estimate in WHI and in FHS, we find no significant interaction of rs9939609 with TSS on BMI (βinteraction=−0.29 × 10−4, Pinteraction=0.99).
Discussion
In a large sample of European-Americans, we find that rs9939609 in FTO is associated with TSS, that TSS partly mediates the association of rs9939609 with BMI, and that the putative effect of sitting on BMI is greatest in those homozygous for the rs9939609 risk allele. In a replication sample of HA and AA, we find a similar, albeit not statistically significant, association of rs9939609 with TSS. In a meta-analysis of the two data sets we find a significant association of the rs9939609 with TSS that is independent of BMI, PA and other covariates. The weaker findings in WHI may be related to the smaller sample size in HA as well as our finding of no association of FTO variants with BMI in AA. As mentioned, we tried other FTO variants previously found to be associated with BMI in AA, but we did not find any association in this cohort with these SNPs. Mediation analyses provided support for a model in which TSS mediates the association of rs9939609 with BMI, but also for a model in which in which BMI mediates the association of rs9939609 with TSS.
The mechanism through which FTO increases BMI is still unclear, although there is evidence from knockout mice models suggesting FTO could be functionally involved in energy homeostasis via regulation of energy expenditure.39 FTO is also found to be strongly expressed in satiety centers within the hypothalamus region,40, 41, 42 where it could potentially influence increased energy intake,8, 43 dietary preferences for increased intake of dietary fats,41, 44 or protein,7, 45 increased appetite and reduced satiety,46 as well as loss of control over eating.47 However, the evidence that the FTO variant is associated with dietary intake is mixed, raising the alternative scenario in which FTO increases BMI through prolonged sedentary behavior. Previous studies of TSS and energy intake have shown that dramatic reductions in energy expenditure due to experimentally induced sitting do not lead to a reduction in appetite or a reduction in food intake.48, 49 Thus, it is possible that individuals with the higher-risk alleles are not modulating energy intake following long periods of reduced energy expenditures associated with high TSS.
Our results of interaction are in agreement with other studies suggesting that the effect of FTO is contingent on lifestyle factors such as PA.50 The direction of the interaction in FHS is consistent with previous studies on PA interactions,9, 10 in that the putative effect of FTO is reduced among those who report low TSS. The inconsistent direction of the interaction in the FHS and WHI data sets makes it difficult to draw any firm conclusions. However, our results do suggest that further exploration of interactions of FTO and/or other genetic factors with sedentary behavior is warranted, especially in diverse populations.
The strengths of our study include the use of overall sitting behavior as opposed to only screen/television time, a replication data set, the use of mediation analysis, and the inclusion of many potential confounders as covariates in the statistical models. Limitations include the observational nature of the study, and the subjective and self-reported measurements of TSS, PA and dietary intake. Another limitation is that the replication data set is comprised of a different ethnic/racial group than the discovery data set, as genetic and other risk factors may differ across these groups.
Further efforts in other data sets with objectively measured sitting behavior are needed to confirm our findings and to contribute to our understanding of the physiological mechanisms underlying specific genetic variants, and how these interact with our lifestyle.
References
Stunkard AJ, Sorensen TI, Hanis C, Teasdale TW, Chakraborty R, Schull WJ et al. An adoption study of human obesity. N Engl J Med 1986; 314: 193–198.
Frayling TM, Timpson NJ, Weedon MN, Zeggini E, Freathy RM, Lindgren CM et al. A common variant in the FTO gene is associated with body mass index and predisposes to childhood and adult obesity. Science 2007; 316: 889–894.
Speliotes EK, Willer CJ, Berndt SI, Monda KL, Thorleifsson G, Jackson AU et al. Association analyses of 249,796 individuals reveal 18 new loci associated with body mass index. Nat Genet 2010; 42: 937–948.
Willer CJ, Speliotes EK, Loos RJ, Li S, Lindgren CM, Heid IM et al. Six new loci associated with body mass index highlight a neuronal influence on body weight regulation. Nat Genet 2009; 41: 25–34.
Berthoud H-R, Morrison C .. The brain, appetite, and obesity. Annu Rev Psychol 2008; 59: 55–92.
Heni M, Kullmann S, Veit R, Ketterer C, Frank S, Machicao F et al. Variation in the obesity risk gene FTO determines the postprandial cerebral processing of food stimuli in the prefrontal cortex. Mol Metab 2014; 3: 109–113.
Qi Q, Kilpeläinen TO, Downer MK, Tanaka T, Smith CE, Sluijs I et al. FTO genetic variants, dietary intake, and body mass index: insights from 177,330 individuals. Hum Mol Genet 2014; 23: 6961–6972.
Qi Q, Downer MK, Kilpelainen TO, Taal HR, Barton SJ, Ntalla I . Dietary intake, FTO genetic variants and adiposity: a combined analysis of over 16,000 children and adolescents. Diabetes 2015; 64: 2467–2476.
Kilpeläinen T, Qi L, Brage S, Sharp S, Sonestedt E, Demerath E et al. Physical activity attenuates the influence of FTO variants on obesity risk: a meta-analysis of 218,166 adults and 19,268 children. PLoS Med 2011; 8: e1001116.
Vimaleswaran KS, Li S, Zhao JH, Luan J, Bingham SA, Khaw KT et al. Physical activity attenuates the body mass index-increasing influence of genetic variation in the FTO gene. Am J Clin Nutr 2009; 90: 425–428.
Van der Ploeg HP, Chey T, Korda RJ, Banks E, Bauman A . Sitting time and all-cause mortality risk in 222 497 Australian adults. Arch Intern Med 2012; 172: 494–500.
Yates T, Khunti K, Wilmot EG, Brady E, Webb D, Srinivasan B et al. Self-reported sitting time and markers of inflammation, insulin resistance, and adiposity. Am J Prev Med 2012; 42: 1–7.
Dunstan DW, Thorp AA, Healy GN . Prolonged sitting: is it a distinct coronary heart disease risk factor? Curr Opin Cardiol 2011; 26: 412–419.
Hamilton MT, Hamilton DG, Zderic TW, Syndrome M, Diabetes T . Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes 2007; 56: 2655–2667.
Hamilton MT, Hamilton DG, Zderic TW . Exercise physiology versus inactivity physiology: an essential concept for understanding lipoprotein lipase regulation. Exerc Sport Sci Rev 2004; 32: 161–166.
Bey L, Hamilton MT . Suppression of skeletal muscle lipoprotein lipase activity during physical inactivity: a molecular reason to maintain daily low-intensity activity. J Physiol 2003; 551: 673–682.
Qi Q, Li Y, Chomistek AK, Kang JH, Curhan GC, Pasquale LR et al. Television watching, leisure time physical activity, and the genetic predisposition in relation to body mass index in women and men. Circulation 2012; 126: 1821–1827.
Graff M, North KE, Richardson AS, Young KM, Mohlke KL, Lange LA et al. Screen time behaviours may interact with obesity genes, independent of physical activity, to influence adolescent BMI in an ethnically diverse cohort. Pediatr Obes 2013; 8: e74–e79.
Dawber TR, Meadors GF, Moore FE Jr . Epidemiological approaches to heart disease: the Framingham Study. Am J Public Health Nations Health 1951; 41: 279–281.
Feinleib M, Kannel WB, Garrison RJ, McNamara PM, Castelli WP . The framingham offspring study. Design and preliminary data. Prev Med 1975; 4: 518–525.
Splansky GL, Corey D, Yang Q, Atwood LD, Cupples LA, Benjamin EJ et al. The third generation cohort of the national heart, lung, and blood Institute’s Framingham Heart Study: design, recruitment, and initial examination. Am J Epidemiol 2007; 165: 1328–1335.
Anderson GL, Cummings SR, Freedman LS, Furberg C, Henderson MM, Johnson SR et al. Design of the Women’s Health Initiative clinical trial and observational study. Control Clin Trials 1998; 19: 61–109.
Franco OH, de Laet C, Peeters A, Jonker J, Mackenbach J, Nusselder W . Effects of physical activity on life expectancy with cardiovascular disease. Arch Intern Med 2005; 165: 2355–2360.
Ainsworth BE, Haskell WL, Leon AS, Jacobs DR, Montoye HJ, Sallis JF et al. Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc 1993; 25: 71–80.
Ware JE, Sherbourne CD . The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992; 30: 473–483.
Sims ST, Larson JC, Lamonte MJ, Michael YL, Martin LW, Johnson KC et al. Physical activity and body mass: changes in younger versus older postmenopausal women. Med Sci Sports Exerc 2012; 44: 89–97.
Grant SF, Li M, Bradfield JP, Kim CE, Annaiah K, Santa E et al. Association analysis of the FTO gene with obesity in children of Caucasian and African ancestry reveals a common tagging SNP. PLoS One 2008; 3: e1746.
Do R, Bailey SD, Desbiens K, Belisle A, Montpetit A, Bouchard C et al. Genetic variants of FTO influence adiposity, insulin sensitivity, leptin levels, and resting metabolic rate in the Quebec family study. Diabetes 2008; 57: 1147–1150.
Liu G, Zhu H, Lagou V, Gutin B, Stallmann-Jorgensen IS, Treiber FA et al. FTO variant rs9939609 is associated with body mass index and waist circumference, but not with energy intake or physical activity in European- and African- American youth. BMC Med Genet 2010; 11: 57.
Hennig BJ, Fulford AJ, Sirugo G, Rayco-Solon P, Hattersley AT, Frayling TM et al. FTO gene variation and measures of body mass in an African population. BMC Med Genet 2009; 10: 21.
Adeyemo A, Chen G, Zhou J, Shriner D, Doumatey A, Huang H et al. FTO genetic variation and association with obesity in West Africans and African Americans. Diabetes 2010; 59: 1549–1554.
Gong J, Schumacher F, Lim U, Hindorff LA, Haessler J, Buyske S et al. Fine mapping and identification of BMI loci in African Americans. Am J Hum Genet 2013; 93: 661–671.
Carty CL, Johnson NA, Hutter CM, Reiner AP, Peters U, Tang H et al. Genome-wide association study of body height in African Americans: The Women’s Health Initiative SNP Health Association Resource (SHARe). Hum Mol Genet 2012; 21: 711–720.
Browning BL, Browning SR . A unified approach to genotype imputation and haplotype-phase inference for large data sets of trios and unrelated individuals. Am J Hum Genet 2008; 84: 210–223.
Consortium GP, Abecasis GR, Auton A, Brooks LD, DePristo MA, Durbin RM et al. An integrated map of genetic variation from 1,092 human genomes. Nature 2012; 491: 56–65.
Viechtbauer W . Conducting meta-analyses in R with the metafor package. J Stat Softw 2010; 36: 1–48.
Tingley D, Yamamoto T, Hirose K, Keele L, Imai K . Mediation: R Package for Causal Mediation Analysis. J Stat Softw 2014; 59: 1–38.
R Core Team R: A Language and Environment for Statistical Computing R Foundation for Statistical Computing: Vienna, Austria, 2015. Available from https://www.R-project.org.
Fischer J, Koch L, Emmerling C, Vierkotten J, Peters T, Brüning JC et al. Inactivation of the Fto gene protects from obesity. Nature 2009; 458: 894–898.
Olszewski PK, Fredriksson R, Olszewska AM, Stephansson O, Alsiö J, Radomska KJ et al. Hypothalamic FTO is associated with the regulation of energy intake not feeding reward. BMC Neurosci 2009; 10: 129.
Tung YCL, Rimmington D, O’Rahilly S, Coll AP . Pro-opiomelanocortin modulates the thermogenic and physical activity responses to high-fat feeding and markedly influences dietary fat preference. Endocrinology 2007; 148: 5331–5338.
Gerken T, Girard CA, Tung Y-CL, Webby CJ, Saudek V, Hewitson KS et al. The obesity-associated FTO gene encodes a 2-oxoglutarate-dependent nucleic acid demethylase. Science 2007; 318: 1469–1472.
Speakman JR, Rance KA, Johnstone AM . Polymorphisms of the FTO gene are associated with variation in energy intake, but not energy expenditure. Obesity (Silver Spring) 2008; 16: 1961–1965.
Timpson NJ, Emmett PM, Frayling TM, Rogers I, Hattersley AT, McCarthy MI et al. The fat mass- and obesity-associated locus and dietary intake in children. Am J Clin Nutr 2008; 88: 971–978.
Ahmad T, I-Min LEE, Paré G, Chasman DI, Rose L, Ridker PM et al. Lifestyle interaction with fat mass and obesity-associated (FTO) genotype and risk of obesity in apparently healthy U.S. women. Diabetes Care 2011; 34: 675–680.
Wardle J, Carnell S, Haworth CMA, Farooqi IS, O’Rahilly S, Plomin R . Obesity associated genetic variation in FTO is associated with diminished satiety. J Clin Endocrinol Metab 2008; 93: 3640–3643.
Tanofsky-Kraff M, Han JC, Anandalingam K, Shomaker LB, Columbo KM, Wolkoff LE et al. The FTO gene rs9939609 obesity-risk allele and loss of control over eating. Am J Clin Nutr 2009; 90: 1483–1488.
Thivel D, Metz L, Aucouturier J, Brakoniecki K, Duche P, Morio B . The effects of imposed sedentary behavior and exercise on energy intake in adolescents with obesity. J Dev Behav Pediatr 2013; 34: 616–622.
Granados K, Stephens BR, Malin SK, Zderic TW, Hamilton MT, Braun B . Appetite regulation in response to sitting and energy imbalance. Appl Physiol Nutr Metab 2012; 37: 323–333.
Kilpeläinen TO, Qi L, Brage S, Sharp SJ, Sonestedt E, Demerath E et al. Physical activity attenuates the influence of FTO variants on obesity risk: a meta-analysis of 218,166 adults and 19,268 children. PLoS Med 2011; 8: e1001116.
Acknowledgements
The authors would like to thank the participants and organizers of the FHS, and WHI studies. Data from these studies was obtained from database of Genotypes and Phenotypes through accession numbers: phs000007.v23.p8 and phs000200.v9.p3.c1. YCK was supported by NIH Grant K01DK095032. FHS: The FHS is conducted and supported by the National Heart, Lung and Blood Institute (NHLBI) in collaboration with Boston University (Contract No. N01-HC-25195). This manuscript was not prepared in collaboration with investigators of the FHS and does not necessarily reflect the opinions or views of the FHS, Boston University or NHLBI. Funding for SHARe Affymetrix genotyping was provided by NHLBI Contract N02-HL-64278. SHARe Illumina genotyping was provided under an agreement between Illumina and Boston University. WHI: The WHI program is funded by the National Heart, Lung and Blood Institute, National Institutes of Health, U.S. Department of Health and Human Services through Contracts N01WH22110, 24152, 32100-2, 32105-6, 32108-9, 32111-13, 32115, 32118-32119, 32122, 42107-26, 42129-32 and 44221. This manuscript was not prepared in collaboration with investigators of the WHI, has not been reviewed and/or approved by the WHI, and does not necessarily reflect the opinions of the WHI investigators or the NHLBI. SHARe: Funding for WHI SHARe genotyping was provided by NHLBI Contract N02-HL-64278.
Author contributions
YCK designed the study and wrote the manuscript. AA, AC and YCK performed data management and analysis. YCK, AA, AC, JZ and DR contributed to discussion, helped write the manuscript and reviewed/edited the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Klimentidis, Y., Arora, A., Chougule, A. et al. FTO association and interaction with time spent sitting. Int J Obes 40, 411–416 (2016). https://doi.org/10.1038/ijo.2015.190
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijo.2015.190
- Springer Nature Limited
This article is cited by
-
Do gene–environment interactions have implications for the precision prevention of type 2 diabetes?
Diabetologia (2022)
-
Quantile-dependent heritability of computed tomography, dual-energy x-ray absorptiometry, anthropometric, and bioelectrical measures of adiposity
International Journal of Obesity (2020)
-
Neurobiology of food choices—between energy homeostasis, reward system, and neuroeconomics
e-Neuroforum (2016)