
Abstract
The objective of this study was to investigate whether serum high-sensitivity C-reactive protein (hs-CRP) concentration varies with dietary fatty acid intake in Iranian adults free of any history of cardiovascular disease (CVD). This cross-sectional study involved 8105 adults (3142 men) aged 35–65 years. Dietary intake was assessed using 24-h dietary recalls. The relationship between anthropometric, cardiometabolic risk factors and dietary data and serum hs-CRP was assessed using SPSS software. Median crude dietary saturated fat decreased across hs-CRP quarters (P =0.009 for linear trend), whereas energy-adjusted total fat (P =0.017), trans-fat (P =0.016), monounsaturated fatty acids (P =0.030) and cholesterol (P =0.005) monotonically increased, with some evidence of statistical interactions by gender. In conclusion, serum hs-CRP concentrations were associated with some components of dietary fatty acid intake in our population of individuals without CVD, suggesting that dietary fat intake could be associated with subclinical inflammation.
Similar content being viewed by others

Introduction
Recent evidence supports a key role for inflammation in all stages of the development of atherosclerosis.1 Circulating markers of inflammation, such as C-reactive protein (CRP), tumor necrosis factor-α and some interleukins (IL-6 and IL- 1), are associated with high risk of cardiovascular events.2 There is growing evidence that the influence of diet on cardiovascular disease (CVD) is mediated through mechanisms that include subclinical inflammation.3 High-sensitivity CRP (hs-CRP) is a biomarker of low-grade inflammation, which has been shown to improve the prediction of the future risk of CVD and type 2 diabetes.4 It has been reported that saturated fatty acids (SFAs) are more prone to be stored in the adipose tissue than monounsaturated fatty acids (MUFAs) and thereby increase the inflammatory milieu of this tissue.5 Studies on the association of saturated fatty acids with hs-CRP3, 5 are conflicting. Some have reported positive associations between fatty acids and hs-CRP,5 whereas others have indicated no significant association.6, 7 Clarifying this relationship has relevance for public health strategies to improve CVD risk stratification and reduction.
In the current study, we have examined the association between dietary intake of trans fatty acids, MUFAs, SFAs, poly unsaturated fatty acids (PUFAs), total fat and the serum concentrations of hs-CRP in a large Iranian adult population who were free of any overt CVD or other inflammatory diseases.
Materials and methods
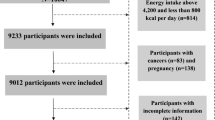
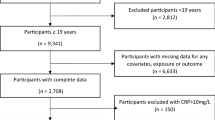
The Mashhad Stroke Heart Atherosclerosis Disorder (MASHAD) is an ongoing urban population-based, observational cohort study that was initiated by investigators of Mashhad University of Medical Sciences, using a stratified-cluster random sampling method.8 The age range of participants was 35 to 64 years, and none had a past history of cardiovascular event (unstable angina, myocardial infarction and stroke), heart failure, peripheral vascular disease including transient ischemic attack or amaurosis fugax, or a history of any previous cardiovascular intervention or surgery. Individuals with any major comorbidity such as cancer, autoimmune, infectious and inflammatory diseases were excluded. The study protocol was approved by the Ethical Committee in Research of Mashhad University of Medical Sciences, and all study participants provided a written informed consent.
For all individuals, anthropometric parameters including weight, height and waist circumference were measured using standard protocols.9 Fasting blood samples (after an overnight fast) were collected from each subject, and then centrifuged for 15 min to obtain serum. Sera were kept at −80 °C until analyzed. Blood pressure was measured using a stethoscope and mercury sphygmomanometer calibrated by the Iranian Institute of Standards and Industrial Research; with Korotkoff phase 1 and phase 5 sounds marked the systolic and diastolic blood pressure, respectively. Fasting blood glucose and lipid profile were measured using an auto-analyzer (Eppendorf, Hamburg, Germany). Biochemical analysis comprising total cholesterol and triglycerides was carried out using enzymatic-based methods (Pars Azmon Inc., Tehran, Iran). Low-density lipoprotein cholesterol was calculated from the serum total cholesterol, triglycerides and high-density lipoprotein cholesterol concentrations expressed in mg/dl using the Friedewald formula. hs-CRP was measured by using an auto-analyzer (Eppendorf).10
Dietary assessment
Dietary information was collected using a questionnaire for 24-h recall, administered by a trained dietary interviewer during a face-to-face interview, to collect information on food and beverage items consumed over the previous 24-h period.11 Individual nutritional intakes were assessed using Dietplan6 software (Forestfield Software Ltd., Horsham, UK). An adjustment was made for total energy intake through the residual method as an alternative to using nutrient densities to control for confounding by total energy intake and to remove extraneous variation due to total energy intake.
Statistical analysis
SPSS software (version 11.5, Chicago, IL, USA) was used for statistical analysis. The Kolmogorov–Smirnov tests were used to assess the normal distribution of continuous variables. Data are expressed as mean±s.d. for normally distributed variables and median and 25th–75th percentiles for skewed variables. Changes in cardiometabolic profiles and dietary intake were investigated using the analysis of variance and Kruskal–Wallis tests. The association of dietary fat with hs-CRP was assessed by measuring the differences in dietary fat intake across subgroups of participants defined by increasing quarters of hs-CRP. A P-value ⩽0.05 was considered statistically significant.
Results
Of the 8105 participants, 39.8% (n =3142) were men. The mean age was 48.3 years overall, 49.1 years in men and 47.9 years in women (P =0.001). Compared with men, women were more likely to have a high body mass index (P =0.001), higher waist girth (P =0.001), higher high-density lipoprotein cholesterol, low-density lipoprotein cholesterol and total cholesterol (all P =0.001), and a higher rate of metabolic syndrome (P =0.001) based on the International Diabetes Federation (IDF) criteria but lower triglycerides, systolic blood pressure and lower smoking rate (all P<0.001), Table 1). The distribution of the same characteristics across quarters of hs-CRP is shown in Table 2, with significant differences (all P<0.001) in a linear manner (all P<0.001 for linear trends), always reflecting monotonically increasing trend (decreasing for high-density lipoprotein cholesterol) across increasing quarters of hs-CRP, with, in most cases, evidence of statistically significant gender*hs-CRP interactions.
The association of fatty acid intake with hs-CRP is summarized in Table 3. Crude saturated fat and MUFA, energy-adjusted total fat, MUFA and cholesterol intake were significantly different across quarters of hs-CRP (all P<0.05). Furthermore, median crude saturated fats monotonically decrease across hs-CRP quarters (P =0.009 for linear trend), whereas energy-adjusted total fat (P =0.017), trans-fat (P =0.016), MUFA (P =0.030) and cholesterol (P =0.005) monotonically increased. Significant but weak correlations were apparent between continuous hs-CRP levels and all components of fatty acid intake. These correlations were negative for crude total fat, saturated fat and trans-fat but positive for the other components (Table 3).
Discussion
This study investigated the association between dietary fat intake and serum hs-CRP concentrations in Iranian adults. The main findings were a weak correlation between various components of fat intake with the hs-CRP level suggesting that the effect, if any, of fat intake on subclinical inflammation in people with no history of CVD is likely to be small.
Consistent with our findings, data from the National Health and Nutrition Examination Survey (NHANES 99-00) have reported SFA consumption to be correlated with increased hs-CRP in US adults.3 Anti-inflammatory effects of Dietary Approaches to Stop Hypertension diet (DASH), which is low in cholesterol, saturated fat, total fat and increased consumption of fruits and vegetables, have been reported in the literature.12 However, Muka et al.13 reported that SFA intake was not significantly related with elevated hs-CRP (⩾1.0 mg/l) in Japanese women. The authors suggested that the absence of association could be due to the low baseline rate of elevated hs-CRP concentrations (5.6%). Moreover, a Swedish study of an elderly population failed to identify a significant relationship between levels of myristic, palmitic or stearic acids, measured in serum cholesteryl esters, and hs-CRP.7 However, these findings were limited to a small sample of older individuals. In line with these latter findings, in an Italian population, an increased SFA intake was not significantly associated with changes in hs-CRP. The authors hypothesized that, in dysmetabolic subjects, the role of dietary factors such as SFA on inflammation could be less evident than in healthy subjects.14
The suggested associations between SFA and serum hs-CRP, if any, could be supported by biological mechanisms. It seems that SFAs stimulate inflammatory signaling pathways by a process that involves Toll-like receptor-415 and subsequently nuclear factor kB, increasing the expression of a number of inflammatory genes.16 A novel mechanism by which SFA might greatly amplify macrophage inflammation through a Toll-like receptor-4-independent pathway has been proposed, which is dependent on the uptake and metabolic processing of SFA into ceramide.17
It has been reported that the intake of peanuts that are rich in MUFA is related with improved postprandial profiles of inflammatory markers and lipids.18, 19 In addition, it has been suggested that the Mediterranean diet, high in MUFAs and PUFAs, has an inverse correlation with inflammatory markers including CRP.12, 20 However, inconsistent findings have been reported in studying this association, with some reporting no significant differences in subjects with a MUFA-rich diet.21, 22, 23 These studies claimed that central adiposity is associated with increased CRP levels, and it is possible that participants with central adiposity may not show improvements in inflammatory markers without weight loss. Furthermore, recently Muke and coworkers in a prospective study analyzing 4707 participants found that high intakes of PUFAs (mainly n-6 PUFAs) were correlated with lower levels of CRP, which might reflect reduced chronic systemic inflammation.13 Julia et al.24 stated that the inverse relation found between total n-3 PUFAs and CRP was mostly driven by long-chain n-3 PUFAs.13
Limitations and strengths
The cross-sectional nature and the 24-h recall methodology are limitations of our study, although this approach has been widely used in previous surveys. Under-reporting of energy intake may be a problem when obese subjects are under investigation.25 A major strength of the present study is the large number of participants. The differences in mean dietary intake between under reporters and those who give valid records reduced by energy adjustment through the residual model.
Conclusion
The most obvious finding from this study is that hs-CRP concentrations are associated with some categories of dietary fatty acids in an Iranian population without the overt history of CVD, suggesting that hs-CRP concentrations could be modulated by dietary fatty acid intake. Furthermore, as the fatty acid intake has been a topic of interest in relation with CVD risk, understanding the effects of SFA, MUFA and PUFA on subclinical inflammation could bring new insights into this field.
References
Micallef MA, Garg ML . Anti-inflammatory and cardioprotective effects of n-3 polyunsaturated fatty acids and plant sterols in hyperlipidemic individuals. Atherosclerosis 2009; 204: 476–482.
DeBoer MD . Obesity, systemic inflammation, and increased risk for cardiovascular disease and diabetes among adolescents: a need for screening tools to target interventions. Nutrition 2013; 29: 379–386.
Santos S, Oliveira A, Casal S, Lopes C . Saturated fatty acids intake in relation to C-reactive protein, adiponectin, and leptin: A population-based study. Nutrition 2013; 29: 892–897.
Bian F, Yang X, Zhou F, Wu PH, Xing S, Xu G et al. C-reactive protein promotes atherosclerosis by increasing LDL transcytosis across endothelial cells. Br J Pharmacol 2014; 171: 2671–2684.
Kalogeropoulos N, Panagiotakos DB, Pitsavos C, Chrysohoou C, Rousinou G, Toutouza M et al. Unsaturated fatty acids are inversely associated and n-6/n-3 ratios are positively related to inflammation and coagulation markers in plasma of apparently healthy adults. Clin Chim Acta 2010; 411: 584–591.
Kong A, Neuhouser ML, Xiao L, Ulrich CM, McTiernan A, Foster-Schubert KE . Higher habitual intake of dietary fat and carbohydrates are associated with lower leptin and higher ghrelin concentrations in overweight and obese postmenopausal women with elevated insulin levels. Nutr Res 2009; 29: 768–776.
Petersson H, Lind L, Hulthe J, Elmgren A, Cederholm T, Riserus U . Relationships between serum fatty acid composition and multiple markers of inflammation and endothelial function in an elderly population. Atherosclerosis 2009; 203: 298–303.
Ghayour-Mobarhan M, Moohebati M, Esmaily H, Ebrahimi M, Parizadeh SM, Heidari-Bakavoli AR et al. Mashhad stroke and heart atherosclerotic disorder (MASHAD) study: design, baseline characteristics and 10-year cardiovascular risk estimation. Int J Public Health 2015; 60: 561–572.
Kazemi-Bajestani SM, Azarpazhooh MR, Ebrahimi M, Vedadian P, Esmaeili H, Parizadeh SM et al. Serum high sensitivity CRP concentrations predict the presence of carotid artery plaque in individuals without a history of cardiovascular events. Nutr Metab Cardiovasc Dis 2015; 25: 434–435.
Kelishadi R, Sharifi M, Khosravi A, Adeli K . Relationship between C-reactive protein and atherosclerotic risk factors and oxidative stress markers among young persons 10–18 years old. Clin Chem 2007; 53: 456–464.
Azarpazhooh MR, Kazemi-Bajestani SM, Esmaeili H, Vedadian P, Ebrahimi M, Parizadeh SM et al. Cardiovascular risk factors and nutritional intake are not associated with ultrasound-defined increased carotid intima media thickness in individuals without a history of cardiovascular events. Int J Prev Med 2014; 5: 1412–1421.
Smidowicz A, Regula J . Effect of nutritional status and dietary patterns on human serum C-reactive protein and interleukin-6 concentrations. Adv Nutr 2015; 6: 738–747.
Muka T, Kiefte-de Jong JC, Hofman A, Dehghan A, Rivadeneira F, Franco OH . Polyunsaturated fatty acids and serum C-reactive protein: the Rotterdam study. Am J Epidemiol 2015; 181: 846–856.
Bo S, Ciccone G, Guidi S, Gambino R, Durazzo M, Gentile L et al. Diet or exercise: what is more effective in preventing or reducing metabolic alterations? Eur J Endocrinol 2008; 159: 685–691.
Chait A, Kim F . Saturated fatty acids and inflammation: who pays the toll? Arterioscler Thromb Vasc Biol 2010; 30: 692–693.
Yeop Han C, Kargi AY, Omer M, Chan CK, Wabitsch M, O'Brien KD et al. Differential effect of saturated and unsaturated free fatty acids on the generation of monocyte adhesion and chemotactic factors by adipocytes: dissociation of adipocyte hypertrophy from inflammation. Diabetes 2010; 59: 386–396.
Schwartz EA, Zhang WY, Karnik SK, Borwege S, Anand VR, Laine PS et al. Nutrient modification of the innate immune response: a novel mechanism by which saturated fatty acids greatly amplify monocyte inflammation. Arterioscler Thromb Vasc Biol 2010; 30: 802–808.
McKiernan F, Lokko P, Kuevi A, Sales RL, Costa NM, Bressan J et al. Effects of peanut processing on body weight and fasting plasma lipids. Br J Nutr 2010; 104: 418–426.
Moreira Alves RD, Boroni Moreira AP, Macedo VS, Bressan J, de Cassia Goncalves Alfenas R, Mattes R et al. High-oleic peanuts: new perspective to attenuate glucose homeostasis disruption and inflammation related obesity. Obesity (Silver Spring, Md) 2014; 22: 1981–1988.
Ahluwalia N, Andreeva VA, Kesse-Guyot E, Hercberg S . Dietary patterns, inflammation and the metabolic syndrome. Diabetes Metab 2013; 39: 99–110.
Barbour JA, Howe PR, Buckley JD, Bryan J, Coates AM . Effect of 12 weeks high oleic peanut consumption on cardio-metabolic risk factors and body composition. Nutrients 2015; 7: 7381–7398.
Harvey KA, Walker CL, Xu Z, Whitley P, Pavlina TM, Hise M et al. Oleic acid inhibits stearic acid-induced inhibition of cell growth and pro-inflammatory responses in human aortic endothelial cells. J Lipid Res 2010; 51: 3470–3480.
Pai JK, Pischon T, Ma J, Manson JE, Hankinson SE, Joshipura K et al. Inflammatory markers and the risk of coronary heart disease in men and women. N Engl J Med 2004; 351: 2599–2610.
Julia C, Touvier M, Meunier N, Papet I, Galan P, Hercberg S et al. Intakes of PUFAs were inversely associated with plasma C-reactive protein 12 years later in a middle-aged population with vitamin E intake as an effect modifier. J Nutr 2013; 143: 1760–1766.
Scagliusi FB, Ferriolli E, Pfrimer K, Laureano C, Cunha CS, Gualano B et al. Underreporting of energy intake in Brazilian women varies according to dietary assessment: a cross-sectional study using doubly labeled water. J Am Diet Assoc 2008; 108: 2031–2040.
Acknowledgements
MM was supported by a TWAS studentship of the Chinese Academy of Sciences, during the preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Mazidi, M., Heidari-Bakavoli, A., Khayyatzadeh, S. et al. Serum hs-CRP varies with dietary cholesterol, but not dietary fatty acid intake in individuals free of any history of cardiovascular disease. Eur J Clin Nutr 70, 1454–1457 (2016). https://doi.org/10.1038/ejcn.2016.92
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejcn.2016.92
- Springer Nature Limited
This article is cited by
-
Level and trend of total plasma cholesterol in national and subnational of Iran: a systematic review and age-spatio-temporal analysis from 1990 to 2016
Journal of Diabetes & Metabolic Disorders (2022)
-
Low adherence to CKD-specific dietary recommendations associates with impaired kidney function, dyslipidemia, and inflammation
European Journal of Clinical Nutrition (2021)
-
Serum trans-fatty acids level are positively associated with lower food security among american adults
Nutrition & Diabetes (2018)
-
Association between plasma trans fatty acids concentrations and leucocyte telomere length in US adults
European Journal of Clinical Nutrition (2018)