
Abstract
Background/Objectives:
The determination of dietary patterns in children examines the effects of the overall diet at early ages, instead of looking at individual foods or energy providing nutrients. The present analysis aims to identify the dietary patterns of preschool children and to examine their associations with multiple socio-economic and lifestyle characteristics.
Subjects/Methods:
Dietary data were collected for 1081 children participating in the Rhea mother–child cohort in Crete, Greece. Diet was assessed using a validated food frequency questionnaire, and dietary patterns were identified with principal component analysis. Multivariable linear regression models were used to examine factors associated with each dietary pattern.
Results:
Three dietary patterns were identified explaining 45.8% of the total diet variation. The ‘Mediterranean’ pattern was based on pulses, olive oil, vegetables, fish and fruits; the ‘Snacky’ pattern included potatoes and other starchy roots, salty snacks, sugar products and eggs; the ‘Western’ pattern contained cereals, cheese, added lipids, beverages and meat. Preschool attendance and increased time spent with the mother (⩾2 h/day) were positively associated with the ‘Mediterranean’ pattern, whereas watching TV was inversely associated with this pattern. Lower parental education, maternal age and earlier introduction to solid foods were positively associated with the ‘Snacky’ pattern. Higher scores on the ‘Western’ type diet were associated with exposure to passive smoking and watching TV. No variation in energy providing nutrient intake was observed across tertiles of the identified dietary patterns.
Conclusions:
The results from this analysis indicate the important role of socio-demographic factors on children’s dietary preferences in early age.
Similar content being viewed by others


Introduction
Dietary food preferences that are first established at preschool age encourage children to adopt healthy eating in adult life.1, 2 Dietary patterns in the first years of life have been associated with multiple health outcomes.3 Unhealthy dietary patterns in the first years of life, with high fat and low fiber foods, have been positively associated with greater risk of childhood obesity4 and negatively associated with cognitive development.5, 6 Understanding early life dietary choices is of great interest in terms of developing strategies that will ensure healthy nutrition in early childhood, as dietary patterns are possibly age specific.
A number of studies have examined dietary patterns in infancy and toddlerhood,7, 8, 9, 10, 11, 12, 13 with only a few focused at preschool age.14, 15, 16, 17 Although the type and number of identified patterns in preschoolers’ vary among studies, three main patterns have been observed. These patterns have been described as ‘healthy’, ‘less healthy’ and ‘traditional’. Several parental socio-demographic and lifestyle characteristics have been associated with the adoption of specific dietary patterns in early childhood. Lower levels of maternal education13, 14, 15, 16, 18 and the presence of older siblings14 have been associated with ‘less healthy’ diets. On the other hand, breastfeeding has been positively associated with the adoption of a ‘healthy’ dietary pattern in childhood.17
The use of dietary patterns allows the combination of foods usually eaten together and the exploration of the whole diet.19 Principal component analysis (PCA) is a statistical method that groups individual foods and nutrients and describes specific patterns. Pattern analysis can form the basis for the development of specific dietary guidelines and recommendations.20
To our knowledge, this is the first birth cohort study exploring the association of dietary patterns using PCA in Greek preschool children and the level of influence by several early life socio-demographic and lifestyle factors. As PCA method is data driven, results from the literature cannot be extrapolated to other populations. Thus, understanding dietary patterns at early ages is essential, given that Greece has the highest prevalence of overweight and obese preadolescent children in Europe, based on recent reports.21
Materials and methods
Study population
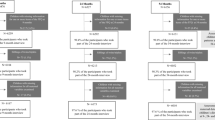
The ‘Rhea’ birth cohort study is a prospective cohort that started in February 2007 in Crete, Greece.22 Briefly, pregnant women, residents in the study area, aged 16 years or above, with no communication handicap were included in the study. Pregnant women (Greek and immigrant) who became pregnant within a 12-month period, starting in February 2007, were contacted and asked to participate in the study. The first contact was made before 15-week gestation, at the time of the first major ultrasound examination, and participants were invited to provide blood and urine samples and to participate in a face-to-face interview. Women were contacted again at various times during pregnancy, at birth, at 8–10 weeks after delivery and for children’s follow-up at 9th, 18th months and at 4 years of age. Face-to face completed questionnaires together with self-administered questionnaires and medical records were used to obtain information on dietary, environmental and psychosocial exposures during pregnancy and early childhood. The study was approved by the Ethical Committee of the University Hospital of Heraklion (Crete, Greece), and all participants provided written informed consent after complete description of the study.
Dietary information was available for 1081 children participating at the 4-year follow-up by completing a food frequency questionnaire (FFQ). Children following a specific diet for health purposes (n=20) were excluded from the analysis resulting to 1061 subjects. In total, 683 children with full information on dietary intake and multiple socio-demographic and lifestyle factors collected at different time points were included in this analysis.
Dietary assessment
Dietary assessment at 4 years of age was performed with the use of the ‘Rhea follow-up FFQ’, which is a validated semi-quantitative food frequency questionnaire designed to assess habitual dietary intake in preschool children.23 Primary caregivers were phone-interviewed by a dietitian trained in a standard protocol to complete the questionnaire. The questionnaire contained questions on 118 food items with the following components: food frequency, type of meals during the day (breakfast, morning snack, lunch, afternoon snack, dinner and evening snack), use of dietary supplements, type of fat used for cooking, frequency of meals consumed in restaurants or take away and television viewing during meals. The questions were hierarchical from general to more specific questions. The 118 food items were aggregated into 17 food groups (cereals and cereal products, meat and meat products, fish and seafood, milk and milk products, eggs, total added lipids, olive oil, potatoes and other starchy roots, pulses, vegetables, nuts, fruits, sugar preserves and confectionery, non-alcoholic beverages, olives, salty snacks and miscellaneous). Parents could choose from one or two portion sizes and report the child’s intake in terms of times per day, week, month and year or never. Seasonality of consumption was also reported in all food items.
The FFQ data were converted into daily intake of foods and nutrients using the UK food tables (McCance & Widdowson’s The Composition of Foods, 6th summary edition) and standard greek recipes for complex mixed dishes. The dietary intake data were analyzed by using a software program developed at the Department of Applied Information Technology and Multimedia, TEI-Crete, Heraklion, Crete, Greece.
Parental and child characteristics
Parents provided information on several socio-demographic and lifestyle characteristics from early pregnancy up to the age of 4 years through interviewer-administered questionnaires, including the following: (A) Parental characteristics: maternal age at 4 years of age (<31, 31–36, ⩾36 years); maternal residence (urban, rural) at 4 years of age; maternal and paternal origin at recruitment (Greek/Non-Greek); maternal and paternal education at recruitment (low level: ⩽6 years of school, medium level: 7–12 years of school, high level: university or technical college degree); maternal working status at 4 years of age (yes/no); marital status at 4 years of age (married-engaged/other); pre-pregnancy maternal body mass index (BMI, kg/m2) (number); type of delivery (caesarian/vaginal). (B) Child characteristics: gender (male/female); birth order (order number); birth weight (grams); preterm birth (<37 weeks of gestation; yes/no); breastfeeding duration (months); age of introduction to solid foods at 9 months (months); preschool attendance at 4 years of age (yes/no); hours/day spent with mother and father at 4 years of age (<1, 1–2, ⩾2); passive smoking at home at 4 years (yes/no); hours/day spending watching television at 4 years (almost never, 1–2, ⩾3); hours/day spent outside home at 4 years (<1, 1–3, ⩾3); child’s BMI z-scores based on cohort-specific, gender and age-adjusted growth curves. Child’s BMI cutoffs were based on the International Obesity Task Force (IOTF) criteria.24
Statistical analyses
Differences in distributions of normally distributed variables were tested with a t-test, non-normally distributed continuous variables were tested by using nonparametric tests (i.e., Mann–Whitney, Kruskal–Wallis and Spearman’s non-parametric statistical tests), whereas categorical variables were tested with the chi-square test (Pearson’s or Fisher’s exact test with Monte–Carlo correction).
PCA was used to identify the dietary patterns using the child’s daily intake (in grams) of the 17 food groups as input. This method reduces the data by forming linear combinations of the original observed variables, thereby grouping together correlated variables, which in its turn identifies any underlying dimensions in the data. The Kaiser-Mayer-Olkin measure was calculated to evaluate the level of intra-correlation between the variables (values >0.6 indicated good intra-correlation and, therefore, PCA could give interpretable results). To identify the number of components, we used the eigenvalue of >1 criterion and the visual representation by the scree plot25 and the interpretability of the factor loadings. Varimax rotation was applied to enhance the determination of the dietary components.26, 27 Rotation redistributes the explained variance for the individual components, thereby achieving a simpler structure, increasing the number of larger and smaller loadings. Factor loadings above 0.3 on a component were considered to have a strong association with that component. A score was attributed to every child for each of the components identified. The score was calculated for each of the components retained by summing the standardized values of the food items weighted by their scoring coefficients. Tertiles of the factor score of each component were used for cut offs.
Multiple linear regression models were fitted for each of the retained components to determine which of the early life socio-demographic and lifestyle characteristics were significantly associated with the dietary components. Estimated associations were described with β-coefficients and 95% confidence interval (CI). Potential determinants related with dietary components in the bivariate models with a P-value of <0.10 were included in the multivariable linear models. Age, sex and pre-pregnancy maternal BMI were included a priori in the analyses of dietary components.
All hypotheses testing were conducted assuming a 0.05 significance level and a two-sided alternative hypothesis. Stata S.E. version 13 was used for the statistical analyses (StataCorp, College Station, TX, USA).
Results
A description of the population characteristics is presented in Table 1. The mean maternal age when children were 4 years old was 33.4 (s.d.: 4.96) years. The majority of parents had Greek origin and medium education. Most mothers were working and were married and/or engaged. Dietary data were provided for 551 (51.9%) boys and 510 (48.1%) girls at the age of 4 years. Children had mean birth weight 3.17 (s.d.: 0.47) kg, the majority attended preschool (n=703, 85.4%), were not exposed to passive smoking (n=508, 61.7%) and spent 1–2 h/day watching TV (n=513, 62.3%).
Three dietary patterns were extracted at 4 years of age (Table 2). We have chosen to give each factor a label (‘Mediterranean’, ‘Snacky’ and ‘Western’); these do not perfectly describe each underlying pattern but correspond to current views on health diet and aid in the report and discussion of results. The ‘Mediterranean’ dietary pattern comprised mainly vegetables, fruits, pulses, olive oil, fish and seafood. The second pattern included foods that require minimum preparation such as potatoes and other starchy roots, salty snacks, sugar preserves and confectionery and eggs with the description ‘Snacky’ being the most suitable. The last pattern named ‘Western’ loaded highly for cereals and bakery products, cheese, lipids of animal and vegetable origin, sweetened beverages, (soft drinks, packed fruit juices) and meat products. The eigenvalues were 3.72, 1.48 and 1.21 for the ‘Mediterranean’, the ‘Snacky’ and the ‘Western’ factors, respectively. Collectively, these factors explained 45.79% of total variance.
Table 3 presents the multivariable associations between several maternal and child socio-demographic and lifestyle characteristics and the three identified dietary patterns.
The ‘Mediterannean’ pattern
Increased number of siblings (β=0.24; 95% CI: 0.01, 0.47), longer breastfeeding duration (β= 0.02; 95% CI: 0.001, 0.04), preschool attendance (β= 0.28; 95% CI: 0.06, 0.50) and time spent with mother (β=0.24; 95% CI: 0.01, 0.47) were positively associated with the adherence to the ‘Mediterranean’ pattern at 4 years of age, whereas watching TV at 4 years of age (hours/day) was inversely associated with this pattern (β=−0.31; 95% CI:−0.60, −0.03).
The ‘Snacky’ pattern
Higher scores on the ‘Snacky’ pattern were associated with rural residence (β=0.18; 95% CI: 0.03, 0.34), increasing number of older siblings (β=0.28; 95% CI: 0.07, 0.49) and hours spent with the mother (β= 0.22; 95% CI: 0.01, 0.43). Children who were later introduced to solid foods and whose mothers were older and with higher pre-pregnancy BMI scored lower on this pattern. Lower scores were also observed for children of the more educated parents.
The ‘Western’ pattern
Higher scores on the ‘Western’ pattern were observed for children with increasing number of siblings, exposed to passive smoking and for those spent more than 3 h per day watching TV and less than 1 h per day outside home. Negative associations were found between maternal Greek origin (β=−0.39; 95% CI: −0.70, −0.08), preschool attendance (β=−0.23; 95% CI: −0.44, −0.03) and the ‘Western’ pattern.
Analyses of associations between mean energy and energy-adjusted nutrient intake showed no overall variation among the three identified dietary patterns (Supplementary Table 1).
Discussion
The aim of the present study was to identify the dietary patterns in Greek preschool children and to examine their associations with multiple socio-demographic and lifestyle factors.
The total variance (45.8%), explained by the three dietary patterns identified in the present analysis was higher compared with other studies in the Mediterranean region. Studies in Greece and Spain have identified dietary patterns with a lot smaller variance 12.5 and 22.5%, respectively,16, 28 whereas in a Portuguese study where 48% of variance was explained by a total of eight dietary patterns only 9.9% of the variance was explained by the first dietary pattern.18
In the present analysis, the ‘Mediterranean’ dietary component was the principal pattern that explained the higher percentage of variability, 26.6%. Even though traditional Greek diet has undergone many changes the last years,29, 30, 31, 32 it seems that the Mediterranean pattern still reflects the main dietary choice for children. At the same time, it is important to highlight that the other two ‘less healthy’ patterns also explain a high percentage of the children’s dietary variation (19.2%).
Regarding our findings on the determinants of dietary patterns, other studies have also found an association between lower parental educational levels,14, 16, 17, 18, 33 the presence of older siblings, exposure to passive smoking8, 14 and earlier introduction to solid foods9, 12 with less ‘healthy’ patterns. Similarly, higher scores on ‘healthier’ patterns have been observed for children with longer breastfeeding duration9, 11, 12, 13, 14, 15, 16, 17 and for those attending preschool.34 It has been supported that attending pre- and elementary school lunch is associated with healthier eating habits and lower sedentary behavior.34 When giving children the option to a single meal proposed at school may encourage them to taste more foods and therefore improve their dietary diversity.35
Overall, there is little evidence on the underlying mechanisms of the previously mentioned determinants on the configuration of preschoolers’ dietary patterns. However, the observed associations of earlier or later introduction to solid foods and breastfeeding duration with dietary patterns can be possibly explained by early feeding practices. There are mechanisms involving genetic determinants that modulate the perception of flavor, the food acceptance and taste preferences.36, 37 Flavors can be transmitted prenatally through amniotic fluid and postnatally through breast milk, depending on maternal diet.38 Therefore, maternal choices are essential for children’s future eating habits.
Comparing our findings with other studies is rather complex mainly because of multiple methodological approaches including study design, dietary assessment tools, food variability across countries and different statistical techniques used. Factor analysis is a sample-specific method, and its results cannot be extrapolated to the general population.39 The main reservation of PCA is that it introduces researcher’s subjectivity in the analysis, when determining the number of components and their interpretation. However, these subjective decisions derive from previous scientific knowledge on nutritional epidemiologic research.
Strengths of the present study include the population-based prospective design and the high participation rate (82%). Diet was assessed using a validated FFQ for this population,23 although parental misreporting should always be counted in.40 PCA is also a validated method for the determination of dietary patterns.41 The use of this method gives the opportunity to gain deep understanding of the whole diet instead of isolated foods and nutrients and thus design valuable interventions and health policies.42 A limitation of our analysis is that we found no variation in nutrient intake underpinning each dietary pattern, which could have provided us with useful information on the association between diet and health.
The findings of the present study clearly indicate that dietary patterns followed from preschoolers’ are associated with multiple socio-demographic factors and lifestyle choices. As dietary and other lifestyle choices are formed early in life, it is essential to enforce policies targeting the whole family and encouraging healthy behaviors from pregnancy onward.
References
Ventura AK, Worobey J . Early influences on the development of food preferences. Curr Biol 2013; 23: R401–R408.
Birch L, Savage JS, Ventura A . Influences on the development of children's eating behaviours: from infancy to adolescence. Can J Diet Pract Res 2007; 68: s1–s56.
Smithers LG, Golley RK, Brazionis L, Lynch JW . Characterizing whole diets of young children from developed countries and the association between diet and health: a systematic review. Nutr Rev 2011; 69: 449–467.
Ambrosini GL . Childhood dietary patterns and later obesity: a review of the evidence. Proc Nutr Soc 2014; 73: 137–146.
Smithers LG, Golley RK, Mittinty MN, Brazionis L, Nortstone K, Emmett P et al. Do dietary trajectories between infancy and toddlerhood influence IQ in childhood and adolescence? Results from a prospective birth cohort study. PLoS One 2013; 8: e58904.
Northstone K, Joinson C, Emmett P, Ness A, Paus T . Are dietary patterns in childhood associated with IQ at 8 years of age? A population-based cohort study. J Epidemiol Community Health 2012; 66: 624–628.
Ystrom E, Niegel S, Vollrath ME . The impact of maternal negative affectivity on dietary patterns of 18-month-old children in the Norwegian Mother and Child Cohort Study. Matern Child Nutr 2009; 5: 234–242.
Smithers LG, Brazionis L, Golley RK, Mittinty MN, Nortstone K, Emmett P et al. Associations between dietary patterns at 6 and 15 months of age and sociodemographic factors. Eur J Clin Nutr 2012; 66: 658–666.
Robinson S, Marriott L, Poole J, Crozier S, Borland S, Lawrence W et al. Dietary patterns in infancy: the importance of maternal and family influences on feeding practice. Br J Nutr 2007; 98: 1029–1037.
Okubo H, Miyake Y, Sasaki S, Tanaka K, Murakami K, Hirota Y . Dietary patterns in infancy and their associations with maternal socio-economic and lifestyle factors among 758 Japanese mother-child pairs: the Osaka Maternal and Child Health Study. Matern Child Nutr 2014; 10: 213–225.
Kiefte-de Jong JC, de Vries JH, Bleeker SE, Jaddoe VW, Hofman A, Raat H et al. Socio-demographic and lifestyle determinants of 'Western-like' and 'Health conscious' dietary patterns in toddlers. Br J Nutr 2013; 109: 137–147.
Bell LK, Golley RK, Daniels L, Magarey AM . Dietary patterns of Australian children aged 14 and 24 months, and associations with socio-demographic factors and adiposity. Eur J Clin Nutr 2013; 67: 638–645.
Northstone K, Emmett P . The associations between feeding difficulties and behaviours and dietary patterns at 2 years of age: the ALSPAC cohort. Matern Child Nutr 2013; 9: 533–542.
North K, Emmett P . Multivariate analysis of diet among three-year-old children and associations with socio-demographic characteristics. The Avon Longitudinal Study of Pregnancy and Childhood (ALSPAC) Study Team. Eur J Clin Nutr 2000; 54: 73–80.
Wall CR, Thompson JM, Robinson E, Mitchell EA . Dietary patterns of children at 3.5 and 7 years of age: a New Zealand birth cohort study. Acta Paediatr 2013; 102: 137–142.
Aranceta J, Perez-Rodrigo C, Ribas L, Serra-Majem L . Sociodemographic and lifestyle determinants of food patterns in Spanish children and adolescents: the enKid study. Eur J Clin Nutr 2003; 57: S40–S44.
Grieger JA, Scott J, Cobiac L . Dietary patterns and breast-feeding in Australian children. Public Health Nutr 2011; 14: 1939–1947.
Moreira P, Santos S, Padrao P, Cordeiro T, Bessa M, Valente H et al. Food patterns according to sociodemographics, physical activity, sleeping and obesity in Portuguese children. Int J Environ Res Public Health 2010; 7: 1121–1138.
Smith AD, Emmett PM, Newby PK, Northstone K . Dietary patterns obtained through principal components analysis: the effect of input variable quantification. Br J Nutr 2013; 109: 1881–1891.
Krauss RM, Eckel RH, Howard B, Appel LJ, Daniels SR, Deckelbaum RJ et al. AHA Dietary Guidelines: revision 2000: a statement for healthcare professionals from the Nutrition Committee of the American Heart Association. Circulation 2000; 102: 2284–2299.
Cole TJ, Lobstein T . Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes 2012; 7: 284–294.
Chatzi L, Plana E, Daraki V, Karakosta P, Alegkakis D, Tsatsanis C et al. Metabolic syndrome in early pregnancy and risk of preterm birth. Am J Epidemiol 2009; 170: 829–836.
Leventakou V, Georgiou V, Chatzi L, Sarri K . Relative validity of an FFQ for pre-school children in the mother-child 'Rhea' birth cohort in Crete, Greece. Public Health Nutr 2014; 18: 421–427.
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH . Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 2000; 320: 1240–1243.
Cattell RB . The scree test for the number of factors. Multivariate Behav Res 1966; 1: 245–276.
Gorsuch RL . Factor Analysis. WB Saunders Company: Philadelphia, PA, USA, 1974.
Kline P . An Easy Guide to Factor Analysis. Routledge: London, UK; New York, USA, 1994.
Manios Y, Kourlaba G, Grammatikaki E, Androutsos O, Ioannou E, Roma-Giannikou E . Comparison of two methods for identifying dietary patterns associated with obesity in preschool children: the GENESIS study. Eur J Clin Nutr 2010; 64: 1407–1414.
Lazarou C, Panagiotakos DB, Matalas AL . Level of adherence to the Mediterranean diet among children from Cyprus: the CYKIDS study. Public Health Nutr 2009; 12: 991–1000.
Kontogianni MD, Vidra N, Farmaki AE, Koinaki S, Belogianni K, Sofrona S et al. Adherence rates to the Mediterranean diet are low in a representative sample of Greek children and adolescents. J Nutr 2008; 138: 1951–1956.
Antonogeorgos G, Panagiotakos DB, Grigoropoulou D, Papadimitriou A, Anthracopoulos M, Nicolaidou P et al. The mediating effect of parents' educational status on the association between adherence to the Mediterranean diet and childhood obesity: the PANACEA study. Int J Public Health 2013; 58: 401–408.
Farajian P, Risvas G, Karasouli K, Pounis GD, Kastorini CM, Panagiotakos DB et al. Very high childhood obesity prevalence and low adherence rates to the Mediterranean diet in Greek children: the GRECO study. Atherosclerosis 2011; 217: 525–530.
Nobre LN, Lamounier JA, Franceschini SC . Preschool children dietary patterns and associated factors. J Pediatr (Rio J) 2012; 88: 129–136.
Dubuisson C, Lioret S, Dufour A, Volatier JL, Lafay L, Turck D . Associations between usual school lunch attendance and eating habits and sedentary behaviour in French children and adolescents. Eur J Clin Nutr 2012; 66: 1335–1341.
Nelson M, Lowes K, Hwang V . The contribution of school meals to food consumption and nutrient intakes of young people aged 4-18 years in England. Public Health Nutr 2007; 10: 652–662.
Beauchamp GK, Mennella JA . Early flavor learning and its impact on later feeding behavior. J Pediatr Gastroenterol Nutr 2009; 48: S25–S30.
Harris G . Development of taste and food preferences in children. Curr Opin Clin Nutr Metab Care 2008; 11: 315–319.
Mennella JA, Jagnow CP, Beauchamp GK . Prenatal and postnatal flavor learning by human infants. Pediatrics 2001; 107: E88.
Schulze MB, Hoffmann K, Kroke A, Boeing H . An approach to construct simplified measures of dietary patterns from exploratory factor analysis. Br J Nutr 2003; 89: 409–419.
Treiber FA, Leonard SB, Frank G, Musante L, Davis H, Strong WB et al. Dietary assessment instruments for preschool children: reliability of parental responses to the 24-hour recall and a food frequency questionnaire. J Am Diet Assoc 1990; 90: 814–820.
Hu FB, Rimm E, Smith-Warner SA, Feskanich D, Stampfer MJ, Ascherio A et al. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am J Clin Nutr 1999; 69: 243–249.
Newby PK, Tucker KL . Empirically derived eating patterns using factor or cluster analysis: a review. Nutr Rev 2004; 62: 177–203.
Acknowledgements
The Rhea study was financially supported by European projects (EU FP6-2003-Food-3-A NewGeneris, EU FP6. STREP Hiwate, EU FP7 ENV.2007.1.2.2.2. Project No 211250 Escape, EU FP7-2008-ENV-1.2.1.4 Envirogenomarkers, EU FP7-HEALTH-2009- single-stage CHICOS, EU FP7 ENV.2008.1.2.1.6. Proposal No 226285 ENRIECO) and the Greek Ministry of Health (Program of Prevention of obesity and neurodevelopmental disorders in preschool children, in Heraklion district, Crete, Greece: 2011-2014). We thank all the cohort participants for their generous collaboration
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on European Journal of Clinical Nutrition website
Supplementary information
Rights and permissions
About this article

Cite this article
Leventakou, V., Sarri, K., Georgiou, V. et al. Early life determinants of dietary patterns in preschool children: Rhea mother–child cohort, Crete, Greece. Eur J Clin Nutr 70, 60–65 (2016). https://doi.org/10.1038/ejcn.2015.93
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejcn.2015.93
- Springer Nature Limited
This article is cited by
-
Use of a hybrid method to derive dietary patterns in 7 years olds with explanatory ability of body mass index at age 10
European Journal of Clinical Nutrition (2021)
-
High adherence to a mediterranean diet at age 4 reduces overweight, obesity and abdominal obesity incidence in children at the age of 8
International Journal of Obesity (2020)
-
A traditional dietary pattern is associated with lower odds of overweight and obesity among preschool children in Lebanon: a cross-sectional study
European Journal of Nutrition (2019)
-
Dietary patterns are associated with attention-deficit/hyperactivity disorder (ADHD) symptoms among preschoolers in mainland China
European Journal of Clinical Nutrition (2018)
-
Dietary patterns of early childhood and maternal socioeconomic status in a unique prospective sample from a randomized controlled trial of Prenatal DHA Supplementation
BMC Pediatrics (2016)