
Abstract
Background/Objectives:
The use of dietary supplements (DSs) by children and adolescents is increasing. The aim of this study was to identify the characteristics of DS users and examine the nutritional contributions of DSs to total nutrient intakes in children and adolescents, using data obtained from a national survey.
Subjects/Methods:
In total, 3134 subjects aged 9–18 years who participated in the 4th Korea National Health and Nutrition Examination Survey (2007–2009) were selected; the survey included 24-h recall questions on food intake and questions on DS use over the past year. Nutrient intakes from DSs were calculated using the aid of a label-based database on such supplements, and individual total nutrient intakes were derived by combining information on the foods and DSs consumed by each subject.
Results:
There were 895 DS users (28.5%), 85.2% of whom (n=577) had complete DS nutrient information and were therefore defined as identified-DS users. Identified-DS users were slightly younger and had a greater household income and better nutritional knowledge than did non-users. The most frequently consumed type of supplement was a ‘multivitamin and minerals’ complex. For total nutrient intake, identified-DS users had a significantly higher intake of most of the nutrients, except for macronutrient and sodium than non-users. In all identified-DS users, the contribution of vitamins and minerals from DSs to total nutrient intake was higher than energy and macronutrients.
Conclusions:
DS use by children and adolescents can improve micronutrient status, but it also increases the risk of excessive intake of certain vitamins and minerals.
Similar content being viewed by others


Introduction
The use of dietary supplement (DS) has increased substantially in Korea and other countries. Recent national surveys reported that the prevalence of DS use in adults was approximately 50% in the United States,1 33% in the United Kingdom,2 30–56% in the Netherlands3 and 34% in Korea.4 Children and adolescents also widely used DSs: 37% of US children and 34% of Korean children and adolescents reportedly taking DSs of any type.5, 6
Adult DS users are more likely to be female and to have higher levels of education and healthier lifestyles, compared with non-users.7, 8, 9, 10, 11 Although there are few studies of supplement use in children and adolescents, similar trends have been observed with respect to higher family socioeconomic status,5, 12 greater knowledge of nutrition,13 generally healthier diets and increased engagement in physical activity.12, 14
DSs are important sources of nutrients that can complement nutrients naturally occurring in foods.15, 16 They contribute substantially to total micronutrient intake, and the use of vitamin–mineral complexes is particularly common. Because of the absence of a Korean nutrient database for DS, very few studies have examined the effects of DSs on total nutrient intake (that is, from both foods and DSs). In the Multiethnic Cohort Study,17 the prevalence of nutrient adequacy was calculated based on food frequency questionnaire data; when DSs were included, it improved by an average of 8% for both sexes. Bailey et al. reported on the effects of DSs on micronutrient sufficiency in US adults,18, 19 as well as in children and adolescents,20 using data from the National Health and Nutrition Examination Survey (NHANES). In US adults, total vitamin and mineral intakes in supplement users were higher compared with non-users; furthermore, supplement use was associated with a lower prevalence of intakes below the estimated average requirement. Moreover, intakes of several nutrients, such as folic acid, vitamin A, vitamin B6, vitamin C, calcium, zinc, iron and magnesium, were above the tolerable upper intake levels.18, 19 Similar to adults, micronutrient supplement use in children and adolescents was associated with a lower prevalence of inadequate intake of many different vitamins and minerals; however, the prevalence of intakes above the upper intake level for several micronutrients including iron, zinc, folic acid and vitamin A was increased.20 Therefore, it is important to monitor the extent to which DSs influence adequate, as well as excessive, nutrient intakes. Children and adolescents are particularly susceptible to the effects of DSs, due to their relatively low body weights. To date, however, no study has examined the nutrient contribution from DS use to total nutrient intake in Asian adolescents.
The primary goal of this study was to examine the nutrient intake from DSs and evaluate total nutrient intake compared with dietary reference intakes for Korean children and adolescents using data from the 4th Korea NHANES (KNHANES).
Materials and methods
Study design and study population
This study was based on data from the 4th KNHANES (2007–2009), a cross-sectional, nationally representative survey carried out by the Korea Centers for Disease Control and Prevention. The KNHANES uses a stratified, multistage probability sampling method and comprises the following three surveys: a health-related questions survey, a dietary survey and a health examination survey. Detailed information from each survey is available on the KNHANES website (http://knhanes.cdc.go.kr).21 KNHANES was approved by the Korea Centers for Disease Control and Prevention Institutional Review Board, and informed written consent was provided by every subject.
The study population comprised boys and girls between 9 and 18 years of age who had completed the nutrition survey. The nutrition survey consisted of 24-h recall and dietary-related questionnaire components, including items pertaining to DS use.
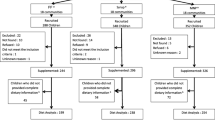
Of the 3134 eligible subjects between 9 and 18 years of age, 2239 subjects (71.4%) reported that they were not taking DS, compared with 895 subjects (28.5%) who were taking DSs. Of these 895 subjects, we excluded individuals who did not provide product names (n=218) or provided inaccurate product information (n=100). The remaining 577 subjects were defined as ‘identified-DS users’. The final study sample comprised 2816 subjects.
DS information
DS information was obtained using the following questions: ‘In the past year, have you consumed any vitamin or mineral supplements for at least 2 weeks on a continuous basis?’ and ‘In the past year, have you consumed any functional foods for health at least 2 weeks on a continuous basis?’. Subjects who answered ‘yes’ for either question were defined as ‘DS users’ and were then asked for more detailed information pertaining to consumption frequency, amount taken per serving and supplement type, brand and name. This information was used during searches of the nutrient composition of each product, as well as to calculate total nutrient intake from DSs.
Nutrient intake from DS was calculated using DS nutrient database based on product label information; details of this process are provided elsewhere.11 Briefly, DSs in the Korean market are classified as either functional foods for health or pharmaceutical drugs. Although nutrient information for health functional foods was directly obtained from nutrient labels, information for pharmaceutical drugs was calculated on the basis of the ingredients comprising their chemical formulae. DSs type was classified based upon the categories provided by the Korean Ministry of Food and Safety. Multivitamin and mineral supplements were defined as those that contained at least one vitamin and at least one mineral and vitamin or mineral supplements as those that contained more than one vitamin or mineral, respectively.
Estimation of usual intake from foods using a 24-h recall method
Dietary intake from food sources was obtained using a 24-h recall method. Because the 4th KNHANES provided 24-h recall data for only 1 day, we used the data for 2 days obtained during the KNHANES of 2001–2002. Murphy and Poos22 suggested that an estimate of within-person variation in nutrient intakes can be taken from other data sets if it is not available in the sample being studied. The usual intakes in the present study were therefore calculated by using an estimate of within-person variation derived from the 2001–2002 sub-data using the C-SIDE software package (Software for Intake Distribution Estimation; ver. 1.02, 1996; available from the Center for Survey Statistics and Methodology, Iowa State University, Ames, IA, USA). Estimation details have been described elsewhere.23 Briefly, within-person variations in the intake of each nutrient were estimated using the 2-day intake data of the 2001–2002 KNHANES. This within-person variation of each nutrient was applied in the estimation of the distribution of usual intake from the 24-h recall data. We also partially removed the effect of certain variables, such as age and gender, from the intake data using C-SIDE’s adjustment procedure as a covariate.
Total nutrient intake from foods and DSs
Nutrient intakes from DSs for each individual were calculated using the reported daily consumption frequency, amount of DS taken per serving and the nutrient profiles per standard serving of DS in database. After the usual intake—from food—of each nutrient was estimated, total nutrient intakes were combined from both foods and DSs for each individual.
Other confounding variables
Demographic and lifestyle characteristics including age, gender, household income and physical activity and body shape self-awareness were also obtained. If a subject indicated engagement in vigorous physical activity for at least 20 min on 3 or more days per week, or moderate physical activity for at least 30 min on 5 or more days per week, then their answer to this question was coded as ‘yes’. The self-awareness of body shape was grouped into five categories, ‘underweight’, ‘slightly underweight’, ‘normal weight’, ‘a little overweight’ and ‘obese’. The use of nutritional labels and the awareness of dietary guidelines for Korean were also included to analyze the knowledge about diet.
Statistical analysis
Data were analyzed using the SAS software package (Statistical Analysis System; ver. 9.3, SAS Institute Inc., Cary, NC, USA). A value of P<0.05 was taken to indicate statistical significance. All analyses took into account the complex sampling design, such that appropriate sampling weights were employed according to the procedure used in the PROC SURVEY.21 Demographic and lifestyle characteristics were compared between identified-DS users and non-users using the chi-square test for categorical variables and the t-test for continuous variables. Total nutrient intake and intake from food sources alone were compared among identified-DS users and non-users using a multivariate regression analysis after adjusting for all potentially confounding variables.
Results
In the 4th KNHANES (2007–2009), 28.5% of subjects 9–18 years of age reported using DSs. The demographic and lifestyle characteristics of identified-DS users and non-users are presented in Table 1. The mean age of the identified-DS users was significantly lower than that of non-users (P=0.0106). No significant between-group difference was evident in terms of gender distribution. However, household income differed significantly by group (Table 1). The percentages of subjects aware of dietary guidelines and who exhibited nutritional knowledge were significantly higher among the identified-DS users. No significant between-group differences in demographic or lifestyle characteristics were evident between the identified-DS users and the non-users (data not shown).
Table 2 shows the DSs most commonly consumed by identified-DS users 9–18 years of age. ‘Multivitamin and mineral’ complexes ranked first. The six most frequently consumed types of DS, when considered together, were consumed by 94.9% of identified-DS users.
Nutrient intakes from food and DSs are shown in Table 3. Considering the nutrients from food only, the identified-DS users consumed higher intakes of energy, vitamin A, riboflavin, calcium, phosphorus and potassium, compared with non-users. Considering the nutrients from DSs, the intakes of vitamin C, thiamin, niacin and iron were higher among the identified-DS users.
Figure 1 illustrates contributions of DSs to total nutrient intake. In all identified-DS users, the percentage of nutrient intakes in vitamins and minerals from DSs to total nutrient intake was higher than energy and macronutrients. The contributions of DSs to total nutrient intake were 0.3–0.4% of energy and macronutrients (data not shown) and 20% or more for water-soluble vitamins and approximately 10% for calcium and iron. When considering identified-DS users who actually consumed each nutrient from DSs, the nutrient contributions of DSs increased 40% or more for water-soluble vitamins and 19% for calcium and 38% for iron.

Contribution of DSs on total nutrient intake among identified-DS users and users who actually obtained each nutrient from dietary supplements. ¶Percentage of nutrient intake from dietary supplement to total nutrient intake.
Discussion
We identified the characteristics of the DS users and examined nutrient contributions from DS to total nutrient intake in a large nationwide sample of Korean children and adolescents.
We found that 28.5% of sampled children and adolescents reported that they took DSs, including vitamin/mineral combinations and functional foods for health, regularly for at least 2 weeks over the past year. Our finding is in agreement with data from other studies, although different methods were used to assess DS intake. Among high school students in Texas,14 23.6% took DSs, as did 26.0% of children 8–11 years of age in Hawaii (on the day before the survey; this figure was 40.0% for the month before the survey).24 Among elementary school children in Taiwan, 22.0% of each sex took supplements.25
Identified-DS users were younger, had higher household incomes, had a greater awareness of dietary guidelines and read nutritional information on products more frequently than did non-users. These findings are similar to those of several other studies in children or adolescents, in which DS use varied by age, race/ethnicity, residential area and family socioeconomic status.5, 25, 26 Most previous studies were characterized by a lack of any between-gender differences, in agreement with our results.5, 14
The most frequently consumed forms of DS were multivitamins and minerals (41.9%). Of all users, 80.4% took specific vitamin- or mineral-related supplements, in agreement with the results of studies conducted in Italy, Japan, Taiwan and the United States.5, 25, 27, 28, 29 As vitamin–mineral complexes are thus the most frequently used supplements, the contributions of such supplement to micronutrient intakes are of particular interest.
We found that the identified-DS users ingested higher amounts of riboflavin, vitamin A, calcium, phosphorus and potassium (compared with non-users), even when nutrients in food only were considered. When nutrients from DSs were included, the vitamin C, thiamin, niacin and iron intakes were also significantly higher in identified-DS users.
A few studies have evaluated nutrient intakes from DSs in children and adolescents, albeit in the context of food only.13, 20 In the Third CATCH (Child and Adolescent Trial for Cardiovascular Health) tracking study, DS users had significantly higher intakes of most vitamins and minerals (16 of 20) from food alone, compared with non-users.13 However, there was no significant differences among supplement users and non-users in terms of micronutrient intakes from food sources alone in children and adolescent of the 2003–2006 NHANES.20
As expected, the DS use was associated with increased vitamin and mineral intakes. Although the use of dietary reference intake values to assess nutrient intake as adequate or excessive is not optimal, particularly for children and adolescents, the proportion of subjects in whom total nutrient intakes, for the majority of vitamins and minerals, were below the estimated average requirement was lower among the identified-DS users. The proportion of subjects who consumed amounts above the upper intake level was 7.5 for vitamin A, 3.5% for vitamin C and 3.7% for iron (data not shown).
Regarding the effects of DSs on nutritional adequacy in children and adolescents, Bailey et al.20 also reported that calcium, iron, magnesium, vitamin A, vitamin C, vitamin D and vitamin E levels were increased, and there was also an association with excessive intakes of certain vitamins and minerals, including iron, zinc, copper, selenium, folic acid, vitamin A and vitamin C.
In Korea, intakes of calcium and iron in youth represent major areas of concern.30 Because the typical Korean diet is rice based and contains plentiful plant-based foods, the reported consumption of milk and dairy products is consistently low. Furthermore, because girls typically desire a slim body shape, anemia is prevalent in this population.31 To address calcium and iron inadequacies, DS use would be beneficial. There is a group of vitamins that accounts for almost half of the total nutrient intake in the youth population, in whom DS should be monitored because data on the long-term effects of high supplement doses in children are still lacking.
Although this study is the first to quantify the contributions of DSs to total nutrient intakes in Asian children and adolescents, several limitations are apparent. First, although we combined the nutrient intakes from food and DSs for each subject, the food data were obtained via 24 h-recall, and dietary supplementation over the past year was explored using a diet questionnaire. Although we calculated intakes using 2001–2002 KNHANES data, the difference between the methods used to derive the data may have biased the total nutrient figures; this possibility should be kept in mind. Nonetheless, it is important to evaluate the micronutrient contributions of several DSs, because children and adolescents are particularly susceptible to excessive intake.
Second, we used a label-based approach to obtain nutritional information on DSs. Label-based values are not as accurate as analytical data, and, our estimates could thus be somewhat inaccurate, in turn affecting our figures on the prevalence of inadequate and excessive nutrient intake. In addition, we could not evaluate the levels of folate, vitamin D or vitamin E, all of which are particularly important nutrients in children and adolescents, because no nutrient database on Korean foods is available.
Finally, we did not include all supplement users because of incomplete data on supplement use in some. However, the general characteristics of the identified and unidentified DS users did not differ (data not shown).
Despite these shortcomings, we used the national data and described nutrient contributions from DSs in Asian children and adolescents. The contribution of DSs for water soluble vitamins was almost half of total nutrient intakes among users who actually consumed each nutrient. This indicates that micronutrient intake from DSs should be monitored in young populations; little is known about the long-term effects of excessive dietary supplementation. Furthermore, methodology to achieve estimation of total nutrient intakes (in food and DSs combined) is required.
References
Bailey RL, Gahche JJ, Lentino CV, Dwyer JT, Engel JS, Thomas PR et al. Dietary supplement use in the United States, 2003-2006. J Nutr 2011; 141: 261–266.
Bates B, Lennox A, Bates C, Swan G . National Diet and Nutrition Survey: Headline Results from Years 1 and 2 (combined) of the Rolling Programme 2008/2009–2010/2011. Department of Health and Food Standards Agency: London, UK, 2011.
Van Rossum C, Fransen H, Verkaik-Kloosterman J, Buurma-Rethans E, Ocké M . Dutch National Food Consumption Survey 2007-2010: Diet of Children and Adults Aged 7 to 69 Years. National Institute of Public Health and the Environment, Ministry of Health, Welfare and Sport: Bilthoven, Netherlands, 2011.
Korea Centers for Disease Control and Prevention Korea Health Statistics 2009: Korea National Health and Nutrition Examination Survey (KNHANES IV-3). Korea Centers for Disease Control and Prevention, Ministry of Health and Welfare: Seoul, Korea, 2010.
Dwyer J, Nahin RL, Rogers GT, Barnes PM, Jacques PM, Sempos CT et al. Prevalence and predictors of children's dietary supplement use: the 2007 National Health Interview Survey. Am J Clin Nutr 2013; 97: 1331–1337.
Yoon JY, Park HA, Kang JH, Kim KW, Hur YI, Park JJ et al. Prevalence of dietary supplement use in Korean children and adolescents: insights from Korea National Health and Nutrition Examination Survey 2007-2009. J Korean Med Sci 2012; 27: 512–517.
Foote JA, Murphy SP, Wilkens LR, Hankin JH, Henderson BE, Kolonel LN . Factors associated with dietary supplement use among healthy adults of five ethnicities: The Multiethnic Cohort Study. Am J Epidemiol 2003; 157: 888–897.
Harrison R, Holt D, Pattison D, Elton P . Are those in need taking dietary supplements? A survey of 21 923 adults. Br J Nutr 2004; 91: 617–623.
Lee J-S, Kim J . Factors affecting the use of dietary supplements by Korean adults: data from the Korean National Health and Nutrition Examination Survey III. J Am Diet Assoc 2009; 109: 1599–1605.
Pouchieu C, Andreeva VA, Péneau S, Kesse-Guyot E, Lassale C, Hercberg S et al. Sociodemographic, lifestyle and dietary correlates of dietary supplement use in a large sample of French adults: results from the NutriNet-Sante cohort study. Br J Nutr 2013; 110: 1480–1491.
Kang M, Kim DW, Baek YJ, Moon SH, Jung HJ, Song YJ et al. Dietary supplement use and its effect on nutrient intake in Korean adult population in the Korea National Health and Nutrition Examination Survey IV (2007-2009) data. Eur J Clin Nutr 2014; 68: 804–810.
Bailey RL, Gahche JJ, Thomas PR, Dwyer JT . Why US children use dietary supplements. Pediatr Res 2013; 74: 737–741.
Dwyer JT, Garceau AO, EVANS M, Li D, Lytle L, Hoelscher D et al. Do adolescent vitamin-mineral supplement users have better nutrient intakes than nonusers? Observations from the CATCH tracking study. J Am Diet Assoc 2001; 101: 1340–1346.
George GC, Springer AE, Forman MR, Hoelscher DM . Associations among dietary supplement use and dietary and activity behaviors by sex and race/ethnicity in a representative multiethnic sample of 11th-grade students in Texas. J Am Diet Assoc 2011; 111: 385–393.
Block G, Sinha R, Gridley G . Collection of dietary-supplement data and implications for analysis. Am J Clin Nutr 1994; 59: 232S–239S.
Patterson RE, Kristal AR, Levy L, McLerran D, White E . Validity of methods used to assess vitamin and mineral supplement use. Am J Epidemiol 1998; 148: 643–649.
Murphy SP, White KK, Park S-Y, Sharma S . Multivitamin-multimineral supplements' effect on total nutrient intake. Am J Clin Nutr 2007; 85: 280S–284S.
Bailey RL, Fulgoni VL III, Keast DR, Dwyer JT . Examination of vitamin intakes among US adults by dietary supplement use. J Acad Nutr Diet 2012; 112: 657–663.
Bailey RL, Fulgoni VL III, Keast DR, Dwyer JT . Dietary supplement use is associated with higher intakes of minerals from food sources. Am J Clin Nutr 2011; 94: 1376–1381.
Bailey RL, Fulgoni VL III, Keast DR, Lentino CV, Dwyer JT . Do dietary supplements improve micronutrient sufficiency in children and adolescents? J Pediatr 2012; 161: 837–842.
Korea Centers for Disease Control and Prevention The Fourth Korea National Health and Nutrition Examination Survey (KNHANES IV). Korea Centers for Disease Control and Prevention, Ministry of Health and Welfare: Seoul, Korea, 2010.
Murphy SP, Poos MI . Dietary reference intakes: summary of applications in dietary assessment. Public Health Nutr 2002; 5: 843–849.
Kim DW, Shim JE, Paik HY, Song WO, Joung H . Nutritional intake of Korean population before and after adjusting for within-individual variations: 2001 Korean National Health and Nutrition Survey Data. Nutr Res Pract 2011; 5: 266–274.
Martin CL, Murphy SP, Novotny R . Contribution of dietary supplements to nutrient adequacy among children in Hawaii. J Am Diet Assoc 2008; 108: 1874–1880.
Chen S, Lin J, Kao M, Hang C, Cheng L, Pan W . Dietary supplement usage among elementary school children in Taiwan: their school performance and emotional status. Asia Pac J Clin Nutr 2007; 16: 554–563.
Wilson KM, Klein JD, Sesselberg TS, Yussman SM, Markow DB, Green AE et al. Use of complementary medicine and dietary supplements among US adolescents. J Adolesc Health 2006; 38: 385–394.
Radimer K, Bindewald B, Hughes J, Ervin B, Swanson C, Picciano MF . Dietary supplement use by US adults: data from the National Health and Nutrition Examination Survey, 1999–2000. Am J Epidemiol 2004; 160: 339–349.
Sato Y, Yamagishi A, Hashimoto Y, Virgona N, Hoshiyama Y, Umegaki K . Use of dietary supplements among preschool children in Japan. J Nutr Sci Vitaminol 2009; 55: 317–325.
Giammarioli S, Boniglia C, Carratu B, Ciarrocchi M, Chiarotti F, Mosca M et al. Use of food supplements and determinants of usage in a sample Italian adult population. Public Health Nutr 2013; 16: 1768–1781.
The Korean Nutrition Society Dietary Reference Intakes for Koreans, 1st revision. The Korean Nutrition Society: Seoul, Korea, 2010.
Lee JO, Lee JH, Ahn S, Kim JW, Chang H, Kim YJ et al. Prevalence and risk factors for iron deficiency anemia in the Korean population: Results of the fifth Korea National Health and Nutrition Examination Survey. J Korean Med Sci 2014; 29: 224–229.
Acknowledgements
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology (grant number NRF-2013R1A1A3010359).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Kang, M., Kim, D., Lee, H. et al. The nutrition contribution of dietary supplements on total nutrient intake in children and adolescents. Eur J Clin Nutr 70, 257–261 (2016). https://doi.org/10.1038/ejcn.2015.156
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejcn.2015.156
- Springer Nature Limited
This article is cited by
-
Questionable advisability of vitamin and mineral dietary supplement use in adolescents
BMC Nutrition (2023)
-
Höchstmengen für Vitamine und Mineralstoffe in Nahrungsergänzungsmitteln
Journal of Consumer Protection and Food Safety (2018)