
Abstract
Background:
CXCL12 (SDF1) is reported to promote cancer progression in several preclinical models and this is corroborated by the analysis of human tissue specimens. However, the relationship between CXCL12 expression and cancer survival has not been systematically assessed.
Methods:
We conducted a systematic review and meta-analysis of studies that evaluated the association between CXCL12 expression and cancer survival.
Results:
Thirty-eight studies inclusive of 5807 patients were included in the analysis of overall, recurrence-free or cancer-specific survival, the majority of which were retrospective. The pooled hazard ratios (HRs) for overall and recurrence-free survival in patients with high CXCL12 expression were 1.39 (95% CI: 1.17–1.65, P=0.0002) and 1.12 (95% CI: 0.82–1.53, P=0.48) respectively, but with significant heterogeneity between studies. On subgroup analysis by cancer type, high CXCL12 expression was associated with reduced overall survival in patients with oesophagogastric (HR 2.08; 95% CI: 1.31–3.33, P=0.002), pancreatic (HR 1.54; 95% CI: 1.21–1.97, P=0.0005) and lung cancer (HR 1.37; 95% CI: 1.08–1.75, P=0.01), whereas in breast cancer patients high CXCL12 expression conferred an overall survival advantage (HR 0.5; 95% CI: 0.38–0.66, P<0.00001).
Conclusions:
Determination of CXCL12 expression has the potential to be of use as a cancer biomarker and adds prognostic information in various cancer types. Prospective or prospective–retrospective analyses of CXCL12 expression in clearly defined cancer cohorts are now required to advance our understanding of the relationship between CXCL12 expression and cancer outcome.
Similar content being viewed by others

Main
A feature of most cancers is heterogeneity with regard to treatment response, recurrence and propensity for metastasis. Biomarkers that decipher this heterogeneity, either independently or in addition to current staging systems can help to guide the suitability of radical surgery and chemoradiotherapy, as well as a tailored approach to follow-up. Despite the promise that prognostic biomarkers hold, relatively few have reached clinical practice. This is because of a failure to translate findings from preclinical models to the clinic, a lack of rigorous prospective biomarker validation studies and poor reproducibility between such studies.
In the past two decades, much scientific endeavour has focused on the role that the immune system has in cancer development (de Visser et al, 2006; Grivennikov et al, 2010). Immune cells contribute to cancer progression, preparation of the premetastatic niche (Psaila and Lyden, 2009) and outgrowth of cancer cells at distant sites. Cytokines are the master regulators of protumourigenic immune cells, orchestrating their recruitment from the bone marrow and blood to the tumour and polarising their phenotype once within the tumour microenvironment. These soluble mediators can also promote intravasation of tumour cells or their migration to metastatic sites, drive angiogenesis and inhibit cytotoxic T-cell activity (Balkwill, 2004; Mantovani et al, 2008; Chow and Luster, 2014). Certain cytokines may therefore be able to provide prognostic information by identifying tumours that are likely to metastasise or display therapeutic resistance (Ludwig and Weinstein, 2005).
The chemokine CXCL12 (SDF1) binds to the chemokine receptor CXCR4 and is constitutively expressed in tissues that serve as sites for metastasis including the lung, bone marrow and liver. Cancer cells migrate to these organs in a CXCL12-dependent manner (Taichman et al, 2002; Ray et al, 2015). Preclinical evidence suggests that migration of cancer cells towards CXCL12 in metastatic sites is dependent on simultaneous gain of CXCR4 expression and loss of CXCL12 in the tumour cell, enabling movement away from the primary tumour and towards the metastatic niche (Wendt et al, 2006, 2008; Murakami et al, 2013). However, this experimentally validated hypothesis is at odds with findings demonstrating that CXCL12 is upregulated in cancer tissues relative to their normal counterparts and that high CXCL12 expression in some human tumours correlates with cancer dedifferentiation and increased tumour grade and stage (Tsuboi et al, 2008; Jaafar et al, 2009; Machelon et al, 2011; Zhong et al, 2012).
Given the complex and multifaceted role that CXCL12 has in the progression of primary cancer to metastasis, the prognostic benefit of determining CXCL12 expression in cancer patients is unclear. In an attempt to address this issue, we have performed a meta-analysis of CXCL12 protein expression in the tumour or plasma of cancer patients with the primary independent variable being high vs low CXCL12 level. Our primary aims were to determine firstly whether CXCL12 expression predicts survival in cancer patients, and secondly, whether CXCL12 measurement can be considered a valid prognostic biomarker in cancer.
Materials and Methods
This meta-analysis was performed in accordance with the Meta-analysis of Observational studies in Epidemiology (MOOSE) group (Stroup et al, 2000) and Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidance (Moher et al, 2009).
Identification of relevant literature
MEDLINE (PubMed) and EMBASE (Ovid) were search on 10 November 2016 by a health-care librarian (TP) using the strategy shown in Supplementary Figures 1 and 2. All abstracts generated from the search strategy were read and the full text of selected publications was viewed to determine whether the inclusion criteria were met. References from included studies were also hand searched to identify further studies for inclusion.
Inclusion/exclusion criteria
Studies in humans with any solid cancer reporting the effect of CXCL12 expression on absolute, cancer-specific and/or recurrence-free survival were included. We accepted publications reporting any means of CXCL12 protein quantification including ELISA of serum or tumour lysates, or histological analysis of tumour samples. Included studies must have analysed surgical resection histology rather than tumour biopsy. Studies were excluded if they analysed RNA only, or performed a synthesis of publicly available proteomics or RNA data, as were studies of <20 patients. Studies were also excluded if they were not published in English and duplicated data sets from the same institution were also excluded.
Authors were contacted via email if their publication met the inclusion/exclusion criteria, but reported insufficient information for inclusion in the analysis. If no response was obtained they were contacted a second time within 4 weeks.
Assessment of publication quality and risk of bias
The Quality in Prognostic Studies (QUIPS) tool was used to determine risk of bias (Hayden et al, 2013). Two authors (HS and AGW) independently assessed each publication meeting the inclusion criteria for the quality domains set out in the QUIPS tool and any discrepancies in their assessment were resolved by joint analysis of the quality domain in question. Risk of bias for each domain was reported using a traffic light system, with red, orange or green indicating a high, moderate or low risk of bias, respectively.
Data extraction and statistical analysis
Data was extracted by one author (AGW) into a spreadsheet and cross-checked by a second author (HS). In all included studies, the independent variable under observation was the level of CXCL12 expression classified as high vs low, as defined by each study. The natural logarithm and standard error of the hazard ratio were calculated for outcome measures in each study. Pooled estimates were presented as forest plots and analysed using the random-effects model (DerSimonian and Laird), performed using Review Manager Version 5.3 (Cochrane Collaboration, Oxford, UK). Heterogeneity between studies was assessed using the Cochran Q statistic (χ2 test) and I2. Heterogeneity was considered high, medium or low if ≥75%, 50–75% or <50%, respectively (Higgins et al, 2003). Funnel plots were constructed for overall, disease-specific and recurrence-free survival analyses and assessed by visual inspection. Subgroup analysis was performed to determine the relationship between CXCL12 expression and outcome in specific cancer types for overall survival. A P-value<0.05 throughout was considered statistically significant. We did not correct the P-value for multiple comparisons within our subgroup analysis as the Cochrane Handbook (V.5.1.0) (Higgins and Green, 2011) currently recommends against this.
Results
Search results
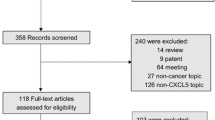
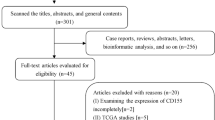
The study flow is shown in Figure 1. A total of 38 studies were included in the meta-analysis of one or more outcome measures totalling 5807 patients (Table 1). Twenty-eight studies reported absolute survival, 16 recurrence-free survival and 4 reported cancer-specific survival. A further 18 studies met the inclusion criteria, but failed to report sufficient data to be included. Of these studies, five authors responded to requests for further data. Of the 11 who failed to respond, 5 reported no association between CXCL12 expression and outcome in the original manuscript.

Study flow.
Study demographics
The demographics of included studies can be seen in Table 1. The total study period ranged from 1982 to 2014, although in 27% of publications, the study period was not identifiable. Forty-seven per cent of studies analysed patients from Australasia, 39% from Europe, 11% from North America and 3% from Africa and 30% of studies analysed data from more than 200 patients. Eighteen studies analysed patients with gastrointestinal cancer (49%), 7 with gynaecological cancer (19%), 4 with breast cancer (11%), 3 with urological cancer (8%) and 2 with lung cancer (5%). The proportion of patients considered to express high levels of CXCL12 varied widely from 18.9% (Wang et al, 2013) to 89.5% (Stanisavljević et al, 2016). The median follow-up period ranged from 4.9 months in a study of metastatic colorectal cancer (Tabernero et al, 2015) to 167 months in a study of ovarian cancer (Popple et al, 2012) and 13 studies (35%) did not provide the median follow-up period.
Study methodology and assessment of study quality
The technical detail for included studies, study methodology and technique for CXCL12 protein quantification is shown in Table 2, while an analysis of risk of bias as determined using the QUIPS tool is shown in Supplementary Table 1. There were 3 studies that analysed serum CXCL12 concentration and 34 studies that quantified tumour protein expression using IHC. We did not identify any study that quantified CXCL12 expression in protein from tumour lysate. Most studies simultaneously analysed the expression of other factors with CXCR4 analysed by 23 studies. The antigen retrieval technique and details of the antibody used, sufficient that the methodology could be repeated by readers, were documented by 16 studies (43%). Interestingly, one study reported the use of an antibody with specificity for CXCR4 for the analysis of CXCL12 (Ishigami et al, 2007).
The method for defining low and high CXCL12 expression level was reported in 89% of studies, with 65% using an arbitrary method not related to data distribution and only 22% of studies determining CXCL12 value cutoffs based on ROC curve analysis. In 10 studies (26%), the CXCL12 expression data was linked to follow-up data collected in a prospective manner.
Survival analysis
The pooled HR for overall survival in patients with high CXCL12 expression compared with low expression was 1.39 (95% CI: 1.17–1.65, P=0.0002), but with a significant degree of heterogeneity (I2=86%) (Figure 2), while the pooled HR for recurrence-free survival was 1.12 (95% CI: 0.82–1.53, P=0.48), again with a high degree of study heterogeneity (I2=85%) (Figure 3). The pool HR for cancer-specific survival, which was only analysed in four studies, was 1.67 (95% CI: 0.43–6.50, P=0.46) again with high study heterogeneity (I2=87%) (results not shown). Funnel plots for overall, recurrence-free and cancer-specific survival demonstrated no evidence of publication bias or small study effects (Figure 4).

Forrest plot of overall survival for all studies meeting the inclusion criteria listed in order of effect size.

Forrest plot of recurrence-free survival for all studies meeting the inclusion criteria in order of effect size.

Funnel plots for included studies reporting overall (left) and recurrence-free survival (right).
Subgroup analysis
Following subgroup analysis, high CXCL12 expression served as a marker of reduced overall survival in oesophagogastric (HR 2.08; 95% CI: 1.31–3.33, P=0.002), pancreatic (HR 1.54; 95% CI: 1.21–1.97, P=0.0005) and lung (HR 1.37; 95% CI: 1.08–1.75, P=0.01) cancers (Figure 5). For colorectal and ovarian cancer, however, there was no relationship between CXCL12 expression and overall survival (HR 1.21; 95% CI: 0.64–2.51, P=0.49) and (HR 1.23; 95% CI: 0.75–2.03, P=0.42), respectively. For breast cancer patients, high CXCL12 predicted better overall survival (HR 0.5; 95% CI: 0.38–0.66, P<0.00001). Of note, aside from colorectal cancer, statistical heterogeneity across studies was significantly lower in subgroup analyses compared with the analysis of all studies combined.

Subgroup analysis by cancer type demonstrating meta-analysis of high vs low CXCL12 expression for overall survival.
Relatively fewer studies published data for recurrence-free survival, but where sufficient data was available, it broadly supported the findings for absolute survival. We were able to identify at least two studies reporting recurrence-free survival for pancreatic, breast or colon cancer (Figure 6).

Subgroup analysis by cancer type demonstrating meta-analysis of high vs low CXCL12 expression for recurrence-free survival.
We also performed further subgroup analyses based on the nature of follow-up data collection (prospective vs retrospective), study size (>200 patients vs <200 patients) or method for defining CXCL12 expression cutoff, reasoning that such analysis might help differentiate studies with a higher level of bias. However, this approach failed to eliminate statistical heterogeneity, which was shared between study types evenly (data not shown).
Discussion
The primary objective of this meta-analysis was to determine whether CXCL12 expression was associated with survival in cancer patients. We found that high CXCL12 expression was associated with reduced absolute survival in patients with oesophagogastric, pancreatic or lung cancer, while the converse was the case for breast cancer patients. Indeed, the major cause of heterogeneity in our meta-analysis resulted from heterogeneity in the relationship between CXCL12 expression and outcome between breast and other cancer types. Our data indicate that determination of CXCL12 expression could be useful for predicting outcome in these cancer types. Although studies of RNA expression were excluded from this meta-analysis, published studies that have assessed CXCL12 mRNA expression in oesophageal (Goto et al, 2017) or breast cancer (Razis et al, 2012) support our findings, with an association between increased CXCL12 expression and adverse outcome in oesophageal cancer, but the converse in breast cancer.
The cause of the different effect of high CXCL12 expression and outcome in breast compared with other cancers is unclear. The publications of breast, pancreatic, lung and oesophagogastric cancer included in our study all analysed primary rather than metastatic tumours; thus, differences are unlikely to result from sampling differences between cancer types. However, they may result from clinicobiological differences between these cancers.
Thus, breast cancer is rarely fatal unless metastatic, whereas oesophagogastric, lung and pancreatic cancers often cause mortality through local invasion. CXCL12 is able to promote local invasion of cancer cells, while loss of CXCL12 promotes tumour cell migration to organs expressing high levels of CXCL12 such as the liver, bone marrow and lung. Breast cancers may therefore rely on downregulation of CXCL12 to metastasise, whereas in pancreatic, oesophagogastric and lung tumours, high CXCL12 expression may be associated with poor outcome because it promotes local invasion, in turn contributing to mortality.
Alternatively, differences between breast and other cancer types may reflect systemic differences between the demographics of the studies, or the methodologies used. It should also be considered that the source of CXCL12 within the tumour may be important. The majority of included studies did not investigate the cellular source of CXCL12, and while the immunohistochemical images presented in most publications indicate the primary source of CXCL12 is the tumour cell, it is possible that stromal and tumour cell CXCL12 production have different roles in cancer progression. Finally, there is significant redundancy in the chemokine network such that analysis of a single chemokine alone may be insufficient. Thus, the relative ratio of CXCL12 to its receptors CXCR4 and/or CXCR7 may be a better indicator of CXCL12 activity (Luker et al, 2012; Wani et al, 2014) and there may be differences in these ratios between cancer types.
Our second objective was to determine whether CXCL12 measurement can be used as a prognostic biomarker in cancer patients. The gold standard evidence level for a prognostic biomarker study is a randomised controlled trial (RCT) designed in such a way that participants are randomised to the prognostic test or a standard prognostic factor and the treatment received dependent on the results of the prognostic test. This type of trial is difficult to perform, requires a very large sample size to be adequately powered and is at significant risk of confounding (Simon et al, 2009).
The retrospective analysis of archived tissue specimens collected as part of an RCT may provide as good an indication of the value of a prognostic marker as an RCT of the marker itself, as can the retrospective analysis of tissues linked to prospectively collected follow-up data (a prospective–retrospective design) (Simon et al, 2009). In contrast, truly retrospective biomarker studies, where follow-up data is generated retrospectively, are at high risk of bias. We were only able to identify one study that used RCT-generated follow-up data (Tabernero et al, 2015) and while a number of other studies were of a prospective–retrospective nature, a significant number were purely retrospective and therefore at risk of bias. This is supported by our analysis of bias using the QUIPS tool, which demonstrated that the majority of studies suffered from at least a moderate risk of bias.
It is however reassuring that the funnel plots generated from studies reporting absolute and recurrence-free survival demonstrate no evidence of publication bias. This is supported by the fact that of the 18 studies that met the inclusion criteria, but reported inadequate outcome data to be included in the meta-analysis, fewer than 50% found that CXCL12 was not associated with outcome; a figure lower than the percentage in the included literature. This suggests that nonsignificant findings with respect to association between CXCL12 expression and outcome are frequently published and were well represented in our analysis.
For a prognostic biomarker to be useful, it must display analytic and clinical validity, as well as clinical utility. Of the studies meeting the inclusion criteria, none robustly determined the validity of the quantification method used and several provided insufficient information such that the method could not be replicated. As a result, the proportion of patients in each study defined as displaying high CXCL12 expression varied considerably. Although such variation may represent true biological differences between tumour types or the patient populations being studied, these factors are unlikely to be the only explanation, as there were significant differences in the proportion of patients with high CXCL12 expression in studies of the same cancer types.
Furthermore, a range of antibodies were used with a sensitivity or specificity for CXCL12 that was not thoroughly determined by the research group, while only two studies repeated their analysis in an independent validation cohort. Based on these findings, although we have identified an association between CXCL12 expression and cancer survival, a standardised, agreed method for CXCL12 quantification has not been reached, and, therefore, CXCL12 can at best be considered an exploratory biomarker at the present time (Goodsaid and Frueh, 2007; Chau et al, 2008). Studies are now needed that accurately report the comparison of several methods for CXCL12 measurement in a prospective–retrospective manner in order that a consensus is reached as to the most appropriate test methodology to take forward for further investigation.
The potential clinical validity of CXCL12 is tested in the subgroup analysis presented here. These data indicate that CXCL12 has clinical validity as a biomarker for breast, pancreatic, lung and oesophagogastric cancer. Studies of colon cancer, whether primary or metastatic, demonstrated heterogenous results over a large number of patients, indicating that measuring CXCL12 alone in colon cancer patients is less likely to be useful for prognostication. Despite this, two colorectal cancer studies assessed the effect of the CXCL12:CXCR4 ratio on survival, with both finding that this approach provided prognostic information. Indeed, the publications by Stanisavljević et al (2016) and D’Alterio et al (2014) found that patients with a combination of low CXCL12 and high CXCR4 expression in the primary tumour experienced reduced recurrence-free or overall survival, respectively. Unfortunately, we were unable to identify other studies that combined the measure of CXCL12 and CXCR4 expression in this way, but the data from these studies indicate that this approach may provide more useful information than measuring either factor alone.
The data identified in our meta-analysis provide only limited information about the precise clinical utility of CXCL12 in specific groups of cancer patients. This is in part because of our broad inclusion criteria that identified a heterogeneous set of studies, and also because of a failure of many included studies to define adequately their cancer population. We found that even simple demographic data such as age, sex and tumour stage was not always reported. Future studies in this area should therefore clearly report the analysis of CXCL12 expression in a subset of cancer patients that are defined on the basis of clinical, histopathological and preferably genomic data such that the clinical utility of CXCL12 in clearly defined cancer patients can be better determined.
In summary, the strengths of this meta-analysis are a wide search strategy identifying multiple studies from differing populations and a pragmatic subgroup analysis highlighting potential differences in the relationship between CXCL12 expression and prognosis between cancer types. Through critical and systematic appraisal, this review has led to guidance points that, if followed, will ensure the generation of higher quality data in the investigation of CXCL12 as a prognostic biomarker. These strengths need to be balanced against the fact that our conclusions are drawn from predominantly retrospectively analyses of survival data, which are by definition prone to bias. The majority of included studies also failed to blind the outcome assessor to participants CXCL12 status, leading to a risk of reporter bias in such studies. Overall, the quality of research in this field needs to improve if progress is to be made in better defining the role of CXCL12 as a prognostic biomarker.
Change history
27 June 2017
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Akishima-Fukasawa Y, Nakanishi Y, Ino Y, Moriya Y, Kanai Y, Hirohashi S (2009) Prognostic significance of CXCL12 expression in patients with colorectal carcinoma. Am J Clin Pathol 132: 202–210, ; quiz 307.
Amara S, Chaar I, Khiari M, Ounissi D, Weslati M, Boughriba R, Hmida AB, Bouraoui S (2015) Stromal cell derived factor-1 and CXCR4 expression in colorectal cancer promote liver metastasis. Cancer Biomark 15: 869–879.
Balkwill F (2004) Cancer and the chemokine network. Nat Rev Cancer 4: 540–550.
Chau CH, Rixe O, McLeod H, Figg WD (2008) Validation of analytical methods for biomarkers employed in drug development. Clin Cancer Res 14: 5967–5976.
Chow MT, Luster AD (2014) Chemokines in cancer. Cancer Immunol Res 2: 1125–1131.
de Cuba EMV, de Hingh IHJT, Sluiter NR, Kwakman R, Coupé VMH, Beliën JAM, Verwaal VJ, Meijerink WJHJ, Delis-van Diemen PM, Bonjer HJ, Meijer GA, Te Velde EA (2016) Angiogenesis-related markers and prognosis after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for metastatic colorectal cancer. Ann Surg Oncol 23: 1601–1608.
D’Alterio C, Avallone A, Tatangelo F, Delrio P, Pecori B, Cella L, Pelella A, D’Armiento FP, Carlomagno C, Bianco F, Silvestro L, Pacelli R, Napolitano M, Iaffaioli RV, Scala S (2014) A prognostic model comprising pT stage, N status, and the chemokine receptors CXCR4 and CXCR7 powerfully predicts outcome in neoadjuvant resistant rectal cancer patients. Int J Cancer 135: 379–390.
Fu Z, Wang F, Cai J (2015) Gene expression changes in residual advanced cervical cancer after radiotherapy: indicators of poor prognosis and radioresistance? Med Sci Monit 21: 1276–1287.
Gilbert DC, Chandler I, McIntyre A, Goddard NC, Gabe R, Huddart RA, Shipley J (2009) Clinical and biological significance of CXCL12 and CXCR4 expression in adult testes and germ cell tumours of adults and adolescents. J Pathol 217: 94–102.
Goodsaid F, Frueh F (2007) Biomarker qualification pilot process at the US Food and Drug Administration. AAPS J 9: E105–E108.
Goto M, Yoshida T, Yamamoto Y, Furukita Y, Inoue S, Fujiwara S, Kawakita N, Nishino T, Minato T, Yuasa Y, Yamai H, Takechi H, Seike J, Bando Y, Tangoku A (2017) CXCR4 expression is associated with poor prognosis in patients with esophageal squamous cell carcinoma. Ann Surg Oncol 24: 832–840.
Grivennikov SI, Greten FR, Karin M (2010) Immunity, inflammation, and cancer. Cell 140: 883–899.
Guo J-C, Li J, Zhou L, Yang J-Y, Zhang Z-G, Liang Z-Y, Zhou W-X, You L, Zhang T-P, Zhao Y-P (2016) CXCL12–CXCR7 axis contributes to the invasive phenotype of pancreatic cancer. Oncotarget 7 (38): 62006–62018.
Hassan S, Ferrario C, Saragovi U, Quenneville L, Gaboury L, Baccarelli A, Salvucci O, Basik M (2009) The influence of tumor–host interactions in the stromal cell-derived factor-1/CXCR4 ligand/receptor axis in determining metastatic risk in breast cancer. Am J Pathol 175: 66–73.
Hayden JA, van der Windt DA, Cartwright JL, Côté P, Bombardier C (2013) Assessing bias in studies of prognostic factors. Ann Intern Med 158: 280–286.
Higgins JPT, Green S (2011) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. Cochrane Collaboration: London, UK.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327: 557–560.
Hong TS, Ryan DP, Borger DR, Blaszkowsky LS, Yeap BY, Ancukiewicz M, Deshpande V, Shinagare S, Wo JY, Boucher Y, Wadlow RC, Kwak EL, Allen JN, Clark JW, Zhu AX, Ferrone CR, Mamon HJ, Adams J, Winrich B, Grillo T, Jain RK, DeLaney TF, Fernandez-del Castillo C, Duda DG (2014) A phase 1/2 and biomarker study of preoperative short course chemoradiation with proton beam therapy and capecitabine followed by early surgery for resectable pancreatic ductal adenocarcinoma. Int J Radiat Oncol Biol Phys 89: 830–838.
Ishigami S, Natsugoe S, Okumura H, Matsumoto M, Nakajo A, Uenosono Y, Arigami T, Uchikado Y, Setoyama T, Arima H, Hokita S, Aikou T (2007) Clinical implication of CXCL12 expression in gastric cancer. Ann Surg Oncol 14: 3154–3158.
Izumi D, Ishimoto T, Miyake K, Sugihara H, Eto K, Sawayama H, Yasuda T, Kiyozumi Y, Kaida T, Kurashige J, Imamura Y, Hiyoshi Y, Iwatsuki M, Iwagami S, Baba Y, Sakamoto Y, Miyamoto Y, Yoshida N, Watanabe M, Takamori H, Araki N, Tan P, Baba H (2016) CXCL12/CXCR4 activation by cancer-associated fibroblasts promotes integrin β1 clustering and invasiveness in gastric cancer. Int J Cancer 138: 1207–1219.
Jaafar F, Righi E, Lindstrom V, Linton C, Nohadani M, Van Noorden S, Lloyd T, Poznansky J, Stamp G, Dina R, Coleman DV, Poznansky MC (2009) Correlation of CXCL12 expression and FoxP3+ cell infiltration with human papillomavirus infection and clinicopathological progression of cervical cancer. Am J Pathol 175: 1525–1535.
Kadota K, Nitadori J, Ujiie H, Buitrago DH, Woo KM, Sima CS, Travis WD, Jones DR, Adusumilli PS (2015) Prognostic impact of immune microenvironment in lung squamous cell carcinoma: tumor-infiltrating CD10+ neutrophil/CD20+ lymphocyte ratio as an independent prognostic factor. J Thorac Oncol 10: 1301–1310.
Kobayashi T, Tsuda H, Moriya T, Yamasaki T, Kikuchi R, Ueda S, Omata J, Yamamoto J, Matsubara O (2010) Expression pattern of stromal cell-derived factor-1 chemokine in invasive breast cancer is correlated with estrogen receptor status and patient prognosis. Breast Cancer Res Treat 123: 733–745.
Lee HJ, Lee K, Lee DG, Bae K-H, Kim J-S, Liang ZL, Huang SM, Suk OhY, Kim HY, Jo DY, Min J-K, Kim J-M, Lee HJ (2012) Chemokine (C–X–C motif) ligand 12 is associated with gallbladder carcinoma progression and is a novel independent poor prognostic factor. Clin Cancer Res 18: 3270–3280.
Liang JJ, Zhu S, Bruggeman R, Zaino RJ, Evans DB, Fleming JB, Gomez HF, Zander DS, Wang H (2010) High levels of expression of human stromal cell-derived factor-1 are associated with worse prognosis in patients with stage II pancreatic ductal adenocarcinoma. Cancer Epidemiol Biomarkers Prev 19: 2598–2604.
Ludwig JA, Weinstein JN (2005) Biomarkers in cancer staging, prognosis and treatment selection. Nat Rev Cancer 5: 845–856.
Luker KE, Lewin SA, Mihalko LA, Schmidt BT, Winkler JS, Coggins NL, Thomas DG, Luker GD (2012) Scavenging of CXCL12 by CXCR7 promotes tumor growth and metastasis of CXCR4-positive breast cancer cells. Oncogene 31: 4750–4758.
Machelon V, Gaudin F, Camilleri-Broët S, Nasreddine S, Bouchet-Delbos L, Pujade-Lauraine E, Alexandre J, Gladieff L, Arenzana-Seisdedos F, Emilie D, Prévot S, Broët P, Balabanian K (2011) CXCL12 expression by healthy and malignant ovarian epithelial cells. BMC Cancer 11: 97.
Mantovani A, Allavena P, Sica A, Balkwill F (2008) Cancer-related inflammation. Nature 454: 436–444.
Martinetti A, Miceli R, Sottotetti E, Di Bartolomeo M, de Braud F, Gevorgyan A, Dotti KF, Bajetta E, Campiglio M, Bianchi F, Bregni G, Pietrantonio F (2014) Circulating biomarkers in advanced colorectal cancer patients randomly assigned to three bevacizumab-based regimens. Cancers 6: 1753–1768.
Mirisola V, Zuccarino A, Bachmeier BE, Sormani MP, Falter J, Nerlich A, Pfeffer U (2009) CXCL12/SDF1 expression by breast cancers is an independent prognostic marker of disease-free and overall survival. Eur J Cancer 45: 2579–2587.
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339: b2535.
Murakami T, Kawada K, Iwamoto M, Akagami M, Hida K, Nakanishi Y, Kanda K, Kawada M, Seno H, Taketo MM, Sakai Y (2013) The role of CXCR3 and CXCR4 in colorectal cancer metastasis. Int J Cancer 132: 276–287.
Ock C-Y, Nam A-R, Lee J, Bang J-H, Lee K-H, Han S-W, Kim T-Y, Im S-A, Kim T-Y, Bang Y-J, Oh D-Y (2017) Prognostic implication of antitumor immunity measured by the neutrophil-lymphocyte ratio and serum cytokines and angiogenic factors in gastric cancer. Gastric Cancer 20 (2): 254–262.
Pils D, Pinter A, Reibenwein J, Alfanz A, Horak P, Schmid BC, Hefler L, Horvat R, Reinthaller A, Zeillinger R, Krainer M (2007) In ovarian cancer the prognostic influence of HER2/neu is not dependent on the CXCR4/SDF-1 signalling pathway. Br J Cancer 96: 485–491.
Popple A, Durrant LG, Spendlove I, Rolland P, Scott IV, Deen S, Ramage JM (2012) The chemokine, CXCL12, is an independent predictor of poor survival in ovarian cancer. Br J Cancer 106: 1306–1313.
Psaila B, Lyden D (2009) The metastatic niche: adapting the foreign soil. Nat Rev Cancer 9: 285–293.
Rave-Fränk M, Tehrany N, Kitz J, Leu M, Weber HE, Burfeind P, Schliephake H, Canis M, Beissbarth T, Reichardt HM, Wolff HA (2016) Prognostic value of CXCL12 and CXCR4 in inoperable head and neck squamous cell carcinoma. Strahlenther Onkol 192: 47–54.
Ray P, Stacer AC, Fenner J, Cavnar SP, Meguiar K, Brown M, Luker KE, Luker GD (2015) CXCL12-γ in primary tumors drives breast cancer metastasis. Oncogene 34: 2043–2051.
Razis E, Kalogeras KT, Kotoula V, Eleftheraki AG, Nikitas N, Kronenwett R, Timotheadou E, Christodoulou C, Pectasides D, Gogas H, Wirtz RM, Makatsoris T, Bafaloukos D, Aravantinos G, Televantou D, Pavlidis N, Fountzilas G (2012) Improved outcome of high-risk early HER2 positive breast cancer with high CXCL13-CXCR5 messenger RNA expression. Clin Breast Cancer 12: 183–193.
Sakai N, Yoshidome H, Shida T, Kimura F, Shimizu H, Ohtsuka M, Takeuchi D, Sakakibara M, Miyazaki M (2012) CXCR4/CXCL12 expression profile is associated with tumor microenvironment and clinical outcome of liver metastases of colorectal cancer. Clin Exp Metastasis 29: 101–110.
Sasaki K, Natsugoe S, Ishigami S, Matsumoto M, Okumura H, Setoyama T, Uchikado Y, Kita Y, Tamotsu K, Hanazono K, Owaki T, Aikou T (2009) Expression of CXCL12 and its receptor CXCR4 in esophageal squamous cell carcinoma. Oncol Rep 21: 65–71.
Schrevel M, Karim R, ter Haar NT, van der Burg SH, Trimbos JBMZ, Fleuren GJ, Gorter A, Jordanova ES (2012) CXCR7 expression is associated with disease-free and disease-specific survival in cervical cancer patients. Br J Cancer 106: 1520–1525.
Simon RM, Paik S, Hayes DF (2009) Use of archived specimens in evaluation of prognostic and predictive biomarkers. J Natl Cancer Inst 101: 1446–1452.
Stanisavljević L, Aßmus J, Storli KE, Leh SM, Dahl O, Myklebust MP (2016) CXCR4, CXCL12 and the relative CXCL12–CXCR4 expression as prognostic factors in colon cancer. Tumour Biol 37: 7441–7452.
Sterlacci W, Saker S, Huber B, Fiegl M, Tzankov A (2016) Expression of the CXCR4 ligand SDF-1/CXCL12 is prognostically important for adenocarcinoma and large cell carcinoma of the lung. Virchows Arch 468: 463–471.
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 283: 2008–2012.
Tabernero J, Lenz H-J, Siena S, Sobrero A, Falcone A, Ychou M, Humblet Y, Bouché O, Mineur L, Barone C, Adenis A, Yoshino T, Goldberg RM, Sargent DJ, Wagner A, Laurent D, Teufel M, Jeffers M, Grothey A, Van Cutsem E (2015) Analysis of circulating DNA and protein biomarkers to predict the clinical activity of regorafenib and assess prognosis in patients with metastatic colorectal cancer: a retrospective, exploratory analysis of the CORRECT trial. Lancet Oncol 16: 937–948.
Taichman RS, Cooper C, Keller ET, Pienta KJ, Taichman NS, McCauley LK (2002) Use of the stromal cell-derived factor-1/CXCR4 pathway in prostate cancer metastasis to bone. Cancer Res 62: 1832–1837.
Tang W, Wang X, Chen Y, Zhang J, Chen Y, Lin Z (2015) CXCL12 and CXCR4 as predictive biomarkers of glioma recurrence pattern after total resection. Pathol Biol (Paris) 63: 190–198.
Teng F, Tian W-Y, Wang Y-M, Zhang Y-F, Guo F, Zhao J, Gao C, Xue F-X (2016) Cancer-associated fibroblasts promote the progression of endometrial cancer via the SDF-1/CXCR4 axis. J Hematol Oncol 9: 8.
Tsuboi K, Kodera Y, Nakanishi H, Ito S, Mochizuki Y, Nakayama G, Koike M, Fujiwara M, Yamamura Y, Nakao A (2008) Expression of CXCL12 and CXCR4 in pT3-stage gastric cancer does not correlate with peritoneal metastasis. Oncol Rep 20: 1117–1123.
Uchi Y, Takeuchi H, Matsuda S, Saikawa Y, Kawakubo H, Wada N, Takahashi T, Nakamura R, Fukuda K, Omori T, Kitagawa Y (2016) CXCL12 expression promotes esophageal squamous cell carcinoma proliferation and worsens the prognosis. BMC Cancer 16: 514.
de Visser KE, Eichten A, Coussens LM (2006) Paradoxical roles of the immune system during cancer development. Nat Rev Cancer 6: 24–37.
Walentowicz-Sadlecka M, Sadlecki P, Bodnar M, Marszalek A, Walentowicz P, Sokup A, Wilińska-Jankowska A, Grabiec M (2014) Stromal derived factor-1 (SDF-1) and its receptors CXCR4 and CXCR7 in endometrial cancer patients. PloS One 9: e84629.
Wang L, Chen W, Gao L, Yang Q, Liu B, Wu Z, Wang Y, Sun Y (2012) High expression of CXCR4, CXCR7 and SDF-1 predicts poor survival in renal cell carcinoma. World J Surg Oncol 10: 212.
Wang Q, Diao X, Sun J, Chen Z (2013) Stromal cell-derived factor-1 and vascular endothelial growth factor as biomarkers for lymph node metastasis and poor cancer-specific survival in prostate cancer patients after radical prostatectomy. Urol Oncol 31: 312–317.
Wang X, Zhang H, He H, Shen Z, Tang Z, Xu J, Sun Y (2014) Prognostic value of stromal cell-derived factor 1 expression in patients with gastric cancer after surgical resection. Cancer Sci 105: 1447–1456.
Wani N, Nasser MW, Ahirwar DK, Zhao H, Miao Z, Shilo K, Ganju RK (2014) C–X–C motif chemokine 12/C–X–C chemokine receptor type 7 signaling regulates breast cancer growth and metastasis by modulating the tumor microenvironment. Breast Cancer Res 16: R54.
Wendt MK, Cooper AN, Dwinell MB (2008) Epigenetic silencing of CXCL12 increases the metastatic potential of mammary carcinoma cells. Oncogene 27: 1461–1471.
Wendt MK, Johanesen PA, Kang-Decker N, Binion DG, Shah V, Dwinell MB (2006) Silencing of epithelial CXCL12 expression by DNA hypermethylation promotes colonic carcinoma metastasis. Oncogene 25: 4986–4997.
Yan M, Jene N, Byrne D, Millar EKA, O’Toole SA, McNeil CM, Bates GJ, Harris AL, Banham AH, Sutherland RL, Fox SB (2011) Recruitment of regulatory T cells is correlated with hypoxia-induced CXCR4 expression, and is associated with poor prognosis in basal-like breast cancers. Breast Cancer Res 13: R47.
Zhong W, Chen W, Zhang D, Sun J, Li Y, Zhang J, Gao Y, Zhou W, Li S (2012) CXCL12/CXCR4 axis plays pivotal roles in the organ-specific metastasis of pancreatic adenocarcinoma: a clinical study. Exp Ther Med 4: 363–369.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 4.0 Unported License.
Supplementary Information accompanies this paper on British Journal of Cancer website
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/4.0/
About this article

{kind=link}
{kind=link}
Cite this article
Samarendra, H., Jones, K., Petrinic, T. et al. A meta-analysis of CXCL12 expression for cancer prognosis. Br J Cancer 117, 124–135 (2017). https://doi.org/10.1038/bjc.2017.134
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2017.134
- Springer Nature Limited
Keywords
This article is cited by
-
High density of CXCL12-positive immune cell infiltration predicts chemosensitivity and recurrence-free survival in ovarian carcinoma
Journal of Cancer Research and Clinical Oncology (2023)
-
Canine transmissible venereal tumour established in immunodeficient mice reprograms the gene expression profiles associated with a favourable tumour microenvironment to enable cancer malignancy
BMC Veterinary Research (2022)
-
Associations of CXCL12 polymorphisms with clinicopathological features in breast cancer: a case-control study
Molecular Biology Reports (2022)
-
Prognostic significance of CD8+ T-cells density in stage III colorectal cancer depends on SDF-1 expression
Scientific Reports (2021)
-
Expression and prognostic value of CXCL12/CXCR4/CXCR7 axis in clear cell renal cell carcinoma
Clinical and Experimental Nephrology (2021)