
Abstract
Introduction
Direct transport from the scene of injury to a trauma centre reduces saves lives. In Ontario, paramedics use the field trauma triage standard (FTTS) to determine if a patient meets trauma bypass criteria. Recent studies have questioned the efficacy of the FTTS in identifying severely injured patients. The objective of this study was to determine the predictive performance of the FTTS on the need for trauma center care in patients who were transported to a trauma center.
Methods
This was a single-center health records study of patients transported by ambulance directly to a level 1 trauma center. Hospital based trauma center need and injury severity score-based need were defined. Bivariate associations with one or more FTTS criteria were tested using the Wilcoxon two-sample test for continuous variables, and the Chi-square or Fisher’s exact test for categorical indicators. The sensitivity and specificity of each category of the FTTS were calculated.
Results
There were 1427 patients included in the study, with 76% men, mean age of 40, and 76% had a blunt mechanism. The overall sensitivity and specificity of the FTTS was 90.9% and 20.8% for hospital-based need and 91.6% and 20.3 for injury severity need. The most sensitive variable for hospital-based need was physiologic criteria (53.7). Mechanism of injury was the most sensitive criteria for injury severity need (54.8). Physiological criteria had the highest association with hospital-based and injury severity need (adjusted odds ratios 7.5 [95% CI 5.8–9.8] and 5.1 [95% CI 3.9–6.7]).
Conclusions
The FTTS has fair performance in identifying the need for hospital-based and injury severity need. Systolic blood pressure less than 90 mmHg, Glasgow Coma Scale (motor) less than 6, and falls greater than 6 m were most predictive of trauma center need. Improving prehospital trauma triage is critical to ensure timely transport to a trauma centre.
Résumé
Introduction
Le transport direct de la scène de la blessure à un centre de traumatologie permet de sauver des vies. En Ontario, les ambulanciers paramédicaux utilisent la norme de triage des traumatismes sur le terrain (FTTS) pour déterminer si un patient répond aux critères de pontage traumatique. Des études récentes ont remis en question l’efficacité du FTTS dans l’identification des patients gravement blessés. L’objectif de cette étude était de déterminer la performance prédictive du FTTS sur le besoin de soins en centre de traumatologie chez les patients qui ont été transportés dans un centre de traumatologie.
Méthodes
Il s’agissait d’une étude des dossiers médicaux d’un seul centre portant sur des patients transportés par ambulance directement à un centre de traumatologie de niveau 1. Les besoins des centres de traumatologie hospitaliers et les besoins basés sur le score de gravité des blessures ont été définis. Les associations bivariées avec un ou plusieurs critères FTTS ont été testées à l’aide du test à deux échantillons de Wilcoxon pour les variables continues et du test de Fisher pour les indicateurs catégoriels. La sensibilité et la spécificité de chaque catégorie du FTTS ont été calculées.
Résultats
Il y avait 1427 patients inclus dans l’étude, avec 76% d’hommes, âge moyen de 40, et 76% avaient un mécanisme émoussé. La sensibilité et la spécificité globales du FTTS étaient de 90,9 % et de 20,8 % pour les besoins hospitaliers et de 91,6 % et de 20,3 % pour les besoins de gravité des blessures. La variable la plus sensible pour les besoins hospitaliers était les critères physiologiques (53,7). Le mécanisme de blessure était le critère le plus sensible pour le besoin de gravité de la blessure (54,8). Les critères physiologiques étaient les plus associés aux besoins hospitaliers et aux besoins en matière de gravité des blessures (rapports de cotes ajustés de 7,5 [IC à 95 % 5,8-9,8] et 5,1 [IC à 95 % 3,9-6,7]).
Conclusion
Le FTTS a un rendement équitable pour ce qui est de déterminer le besoin de soins hospitaliers et de gravité des blessures. La pression artérielle systolique inférieure à 90mmHg, l’échelle de coma de Glasgow (moteur) inférieure à 6 et les chutes supérieures à 6m étaient les plus prédictives des besoins du centre de traumatologie. L’amélioration du triage des traumatismes avant l’hospitalisation est essentielle pour assurer un transport rapide vers un centre de traumatologie.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Direct transport from the scene to a trauma hospital, “trauma bypass”, reduces mortality severely injured patients [1,2,3]. Accurate identification in the field of patients who benefit from higher level care is essential for improving patient outcomes. Over-triage can result in reduced availability of prehospital and in-hospital resources, and increased costs to the system [4]. Under-triage may result in delays to definitive care, increasing morbidity and mortality [1,2,3].
In Ontario, Canada paramedics should bypass the closest emergency department (ED) and transport patients directly to a trauma center if a patient meets specific criteria. These criteria are outlined in the Basic Life Support Standards–Field Trauma Triage Standard (FTTS) (Appendix) [5]. The last update to the Ontario FTTS was in 2014 and was performed through expert consensus from various emergency medical services (EMS) and trauma centre stakeholders. During the last revision in 2014, the FTTS adapted by the Ontario Ministry of Health was aligned with the Center for Disease Control and Prevention (and American College of Surgeons Committee on Trauma Field Triage Decision Scheme [6]. There is considerable variability in regional operations which makes the field triage of trauma patients difficult to compare. Additionally, the lack of standardization in prehospital trauma triage makes it difficult to find consistent performance data. Previously these field triage criteria have been found to under triage 14–34% and over triage 12–31% of patients [7]. An under-triage rate of less than 5% and an over-triage rate of greater than 35% are considered acceptable according to the American College of Surgeons [7, 8]. Understanding the accuracy of the current FTTS can identify areas for improvement in future iterations.
Trauma centre need can be based on the hospital resources required or the injury severity score. Hospital-based need has been defined as a patient requiring one or more of the following: need for blood transfusion, need for surgical interventions on arrival, admission to intensive care unit, or in-hospital mortality [9,10,11]. Injury severity need has been defined as an injury severity score of greater than 15 [12].
The objective of this study was to determine the accuracy and predictive performance of the FTTS to determine the need for trauma centre care for patients transported to a level one trauma center.
Methods
Study design
This was a single-center health records study of all patients who were transported by ambulance to a level 1 trauma center, St. Michael’s Hospital between January 1, 2020 and December 31, 2021. The study was approved by the hospital Research Ethics Board.
Setting
St. Michael’s Hospital is one of two adult level one trauma centers for the Greater Toronto Area, supporting a population of almost 6.5 million residents [13]. St. Michael’s Hospital is a 500-bed, urban, academic lead trauma center in the downtown Toronto core with ~ 1500 trauma activations per year (including both direct from scene and interfacility transfers). Injured patients that meet trauma bypass criteria or trauma activation criteria are treated by the trauma team and have their data collected in the trauma registry. Injured patients that are not trauma team activations are treated solely by the emergency medicine physician in the emergency department. Patients are transported by five paramedic services from the surrounding municipalities as well as the provincial air ambulance provider which transports patients from up to 240 km away via helicopter. All paramedic services provide electronic patient call reports for patients transported to the trauma center reviewed for this study.
Participants
Data were gathered from the St. Michael’s Hospital trauma registry and manual review of paramedic records. All patients presenting as trauma team activation or trauma admissions have demographic and outcomes data collected and stored in the hospital trauma registry as mandated by level 1 accreditation standards. Patients were included if they were a trauma team activation and transported directly from the scene of injury by paramedics. Patients were excluded if they were brought to hospital by police, as an interfacility transfer, or walked in, or did not have a paramedic record available in their hospital records.
Variables: the FTTS criteria
The Ontario FTTS is comprised of 20 distinct criteria. The criteria are divided into physiological, anatomical, mechanism of injury, and special criteria (Appendix). According to the standard, patients meeting any one of the 20 criteria should be transported directly to a trauma center from the field if they are a 30–60 min drive depending on regional policies and procedures. Patients that meet the FTTS that are greater than this drive time should request an air ambulance response to facilitate more timely transfer.
Data sources and measurement
Patients were identified through the trauma registry and patient demographic, injury characteristics, and outcome data were abstracted from this database. At present there is no formal variable collected as to whether a patient meets FTTS or not in the current paramedic records. Thus, a manual review of the paramedic records was performed to assess for the presence or absence of any of the FTTS criteria. Patients were scored at three levels of detail: (1) the presence of any FTTS criteria, (2) the category met (physiological, anatomical, mechanism or injury, special criteria), and (3) the specific criteria met. We relied solely on paramedic documentation of their physical exam findings to support concern for anatomic injuries (i.e. presence of pelvic fracture, depressed skull fracture, flail chest). All paramedic records were reviewed by a single rater with worked experience as a paramedic. The study team met after 10, 50, and 200 charts and then as needed to review and assess any issues on data collection. Due to the large sample size of the study, it was decided to maintain a single reviewer with clinical expertise for consistency, thus no inter-rater reliability calculations were performed.
Primary and secondary outcomes
The primary outcome for our study was hospital-based need. Hospital-based need was defined as a patient requiring one or more of the following:
-
1.
transfusion of blood products in the trauma bay,
-
2.
admission to the operating room or intensive care unit from the trauma bay, or,
- 3.
The secondary outcome was an injury severity score greater than 15, which we have labelled as injury severity need [12].
Statistical methods
The patient sample was described using mean (standard deviation), median (interquartile range), and counts (proportions). Bivariate associations with one or more FTTS criteria were tested using the Wilcoxon two-sample test for continuous variables, and the Chi-square or Fisher’s exact test for categorical indicators. The sensitivity and specificity of each categories of the FTTS criteria (“Physiologic Criteria”, “Anatomical Criteria”, “Mechanism of Injury Criteria”, and “Special Criteria”) were calculated for hospital-based need and injury severity need. Two separate multivariable logistic regression models for hospital-based need and injury severity need included variables considered clinically important as potential predictors. The first model included all four categories of the FTTS criteria. The second model included the presence of specific criteria of the FTTS (Appendix). Burns and pregnancy were not included due to low number of events (4 and 1, respectively). Adjusted odds ratios with 95% confidence intervals were estimated for each model. All tests were two-tailed and statistical significance was defined if the p value was less than 0.05 (Table 1). All analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
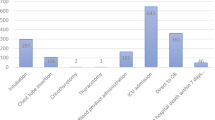
A total of 1427 patients were included, with 1186 (83.1%) patients meeting at least one of the FTTS criteria (Fig. 1). The mean age was 44.8 years and 76% were male. Hospital-based need was met in 482 (33.8%) of patients and 405 (28.4%) patients met injury severity need (Table 2).

Cohort creation flow diagram
Sensitivity, specificity, and adjusted odds ratios for FTTS criteria categories are reported in Table 3. Overall, physiologic criteria were strongly associated with both hospital-based need and injury severity need with adjusted odds ratio of 7.5 (95% CI 5.8–9.8) and 5.1 (95% CI 3.9–6.7) respectively. Physiologic criteria also had the highest specificity for both hospital-based need and injury severity need (86.2 and 82.1). Physiologic criteria were most sensitive (53.7) for hospital-based need, but mechanism was most sensitive for injury severity need (54.8). Overall, the FTTS had an area under the curve of 0.78 for hospital-based need and 0.74 for injury severity need. Overall, the FTTS had a sensitivity of 90.9 and specificity of 20.8 for hospital-based need and a sensitivity of 91.6 and a specificity of 20.3 for injury severity need.
Adjusted odds ratios for the association between each specific FTTS criteria and hospital-based need and injury severity need are reported in Table 4. Systolic blood pressure < 90 mmHg and Glasgow Coma Scale (GCS) motor were associated with the highest odds of hospital-based need with respective adjusted odds ratios of 7.1 (95% CI 4.5–11.5), 5.5 (95% CI 3.9–7.8). Paralysis (adjusted odds ratio 6.8 [95% CI 2.1–21.8]), GCS motor < 6 (adjusted odds ratio 3.8 [95% CI 2.8–5.4]), and fall > 6 m (adjust odds ratio 3.0 [95% CI 1.9–4.9]) were most strongly associated with injury severity need.
Discussion
Interpretation of findings
This study found that the FTTS had fair accuracy in predicting both hospital-based need and injury severity need (AUCs 0.75 and 0.73). The physiological criteria of the FTTS had the strongest association with both hospital-based need and injury severity need. The specific criteria most strongly associated with hospital-based need were systolic blood pressure < 90 mmHg and GCS(motor) < 6. The specific criteria most strongly associated with injury severity need need were paralysis, GCS(motor) < 6 and fall greater than 6 m.
Many of the anatomic criteria of the FTTS that are challenging diagnoses to make in the prehospital environment are the least predictive of TCN. Penetrating injury, chest wall deformity, pelvic fracture, and open or depressed skull fracture were not associated with trauma center need. Injury patterns, while highly specific, often lack sensitivity and are challenging to correctly diagnose in the absence of diagnostic imaging [7]. This study relied on paramedic assessment and documentation of concern for possible injuries to identify the anatomic FTTS criteria. Given the austere prehospital environment, it can be difficult to reliably identify some anatomic criteria. Additionally, paramedic documentation for these anatomic injuries was limited, which may explain why they were not found to be predictive of trauma center need.
Comparison to previous studies
Two studies within the Ontario trauma system identified that approximately 80% of all interfacility transfers to a trauma center met at least one of the FTTS criteria, suggesting that adherence to FTTS is a challenge [14]. The American College of Surgeons Committee on Trauma recently revised their field triage guidelines in 2021 [7]. The biggest change was a departure from the current step-wise approach to the creation of two “high risk” categories (injury patterns and mental status/vital signs) and two “moderate risk” categories (mechanism of injury and EMS judgement) (Appendix). Our study supports this approach as we found that many of the current FTTS criteria that now fall within the new high-risk categories were associated with trauma center need.
Vital signs have long been used to predict the mortality of trauma patients [16]. Our study showed that systolic blood pressure < 90 mmHg, GCS(motor) < 6, and respiratory rate (< 10 or > 30) were some of the most predictive for trauma center need. Shock index is another useful tool that incorporates heart rate divided by systolic blood pressure, with a shock index greater than 1.0 being associated with higher mortality [16,17,18]. The use of shock index as a sole predictor of trauma center need remains unknown, however, the importance of vital sign assessment and consideration of shock index have been included in the updated American College of Surgeons field triage guidelines [7]. The overall mortality of our study is similar to previous large system level trauma studies [19, 20].
Strengths and limitations
One of the strengths of this study was the extensive review of paramedic documentation to identify FTTS performance based on the initial paramedic assessment. By using paramedic documentation as opposed to only registry data, we were able to identify FTTS criteria not captured in any health administrative databases. The primary limitation of this study is that we only included patients who were transported to a trauma center. Therefore, the performance may be different on an entire trauma population. We likely overestimate sensitivity because we have no true assessment of the false negative rate of trauma patients. Likewise, we likely underestimate the specificity as the true negatives never come to the trauma centre. The use of a single, paramedic rater for auditing paramedic records could potentially introduce provider bias into the analysis of the patients’ conditions.
Clinical implications
We identified the individual FTTS criteria associations with trauma center need. This could lead to the development of a more parsimonious iteration of the FTTS by removing non-significant criteria. A more concise tool may reduce the cognitive load for paramedics in making decisions to transport patients to a trauma center in a high acuity, chaotic prehospital environment [15]. Additionally, removing criteria not predictive of TCN may reduce over-triage. The sensitivity of the FTTS was low, indicating there are a number of patients who do not meet the current FTTS that have trauma center need. Identification of additional factors that predict trauma center need is important to reduce under-triage and delays to care. For example, a study within the Ontario trauma setting identified recreational vehicle collisions such as all-terrain vehicles and snowmobiles to be associated with trauma center need [14]. Emergency physicians working at non-trauma centres must be familiar with their regional trauma triage practices. Poor adherence to FTTS can cause undertriage of severely injured patients [14]. Local hospitals, EMS, and trauma centres should ensure a robust quality assurance process to review patients that met trauma bypass criteria but were not brought to a trauma centre.
Research implications
Further investigation should explore paramedic decision making in prehospital trauma triage to understand how and why paramedics make triage decisions, along with insights into these triage decisions, including concordance versus discordance with guidelines [7, 16]. This may help inform triage performance optimization. Additionally, future investigations should explore the removal of variables that are non-predictive of trauma center need and/or addition of new criteria on sensitivity and specificity.
Conclusion
The FTTS as used by paramedics in Ontario to triage trauma patients demonstrated fair performance in identifying trauma center need. The specific criteria most strongly associated with hospital-based need were systolic blood pressure less than 90 mmHg, and GCS (motor) less than 6. The specific criteria most strongly associated with injury severity need need were paralysis, GCS (motor) less than 6, and falls greater than 6 m. Improving the precision of prehospital trauma triage is critical to ensure that severely injured patients are identified and have timely transport to a trauma center.
Data availability
The data that support the findings of this study are available upon reasonable request from the corresponding author.
References
Wright CA. A national evaluation of the effect of trauma-center care on mortality. J Trauma Nurs. 2006;13(3):150. https://doi.org/10.1097/00043860-200607000-00018.
Piontek FA, Coscia R, Marselle CS, Korn RL, Zarling EJ. Impact of American college of surgeons verification on trauma outcomes. J Trauma. 2003;54(6):1041–7. https://doi.org/10.1097/01.ta.0000061107.55798.31.
Demetriades D, Martin M, Salim A, et al. Relationship between American College of Surgeons Trauma Center designation and mortality in patients with severe trauma (injury severity score > 15). J Am Coll Surg. 2006;202(2):212–5. https://doi.org/10.1016/j.jamcollsurg.200509.027.
Cost of Injury in Canada—Parachute. parachute.ca. https://parachute.ca/en/professional-resource/cost-of-injury-in-canada/. Accessed 15 May 2024.
Basic Life Support Patient Care Standards. Emergency Health Regulatory and Accountability Branch Ministry of Health. 2023. https://www.health.gov.on.ca/en/pro/programs/emergency_health/edu/docs/bls_pcs_v3.4.pdf. Accessed 15 May 2024.
Sasser M, et al. Guidelines for Field Triage of Injured Patients: Recommendations of the National Expert Panel on Field Triage. CDC MMWR. 2011
Newgard CD, Fischer PE, Gestring M, et al. National Guideline for the field triage of injured patients: recommendations of the National Expert Panel on Field Triage, 2021. J Trauma Acute Care Surg. 2022;93(2):49–60.
van Rein EAJ, Houwert RM, Gunning AC, Lichtveld RA, Leenen LPH, van Heijl M. Accuracy of prehospital triage protocols in selecting severely injured patients. J Trauma Acute Care Surg. 2017;83(2):328–39. https://doi.org/10.1097/ta.0000000000001516.
Newgard CD, Hedges JR, Diggs B, Mullins RJ. Establishing the need for trauma center care: anatomic injury or resource use? Prehosp Emerg Care. 2008;12(4):451–8. https://doi.org/10.1080/10903120802290737.
Mercier E, Nadeau A, Le Sage N, et al. A Canadian consensus-based list of urgent and specialized in-hospital trauma care interventions to assess the accuracy of prehospital trauma triage protocols: a modified Delphi study. Can J Surg. 2023;66(2):E181–8. https://doi.org/10.1503/cjs.019920.
Tillmann BW, Nathens AB, Guttman MP, et al. Hospital resources do not predict accuracy of secondary trauma triage: a population-based analysis. J Trauma Acute Care Surg. 2019;88(2):230–41. https://doi.org/10.1097/ta.0000000000002552.
Kang BH, Jung K, Kim S, et al. Accuracy and influencing factors of the field triage decision scheme for adult trauma patients at a level-1 trauma center in Korea. BMC Emerg Med. 2022. https://doi.org/10.1186/s12873-022-00637-1.
Economic Research Unit, Economic Development & Culture Division. Toronto at a Glance. Toronto (ON); 2022. https://www.toronto.ca/city-government/data-research-maps/toronto-at-a-glance/. Accessed 2023 Nov 13.
Bischoff T, Briton J, Baumber B, Lewell M, Nolan B. A review of secondary interfacility trauma transfers meeting provincial Prehospital Trauma Triage Guidelines. CJEM. 2021;23(6):837–41. https://doi.org/10.1007/s43678-021-00192-x.
Reay G, Rankin JA, Smith-MacDonald L, Lazarenko GC. Creative adapting in a fluid environment: an explanatory model of paramedic decision making in the pre-hospital setting. BMC Emerg Med. 2018. https://doi.org/10.1186/s12873-018-0194-1.
Kim DK, Jeong J, Shin SD, et al. Association between prehospital field to emergency department delta shock index and in-hospital mortality in patients with torso and extremity trauma: a multinational, observational study. PLoS One. 2021;16(10): e0258811. https://doi.org/10.1371/journal.pone.0258811.
Iirola T, Björkman J, Laaksonen M, Nurmi J. Predictive value of shock index variants on 30-day mortality of trauma patients in helicopter emergency medical services: a nationwide observational retrospective multicenter study. Sci Rep. 2022. https://doi.org/10.1038/s41598-022-24272-9.
Assessing Trauma: The Shock Index—JEMS: EMS, Emergency Medical Services—Training, Paramedic, EMT News. 2023. https://www.jems.com/patient-care/assessing-trauma-the-shock-index/#:~:text=In%20trauma%20patients%20with%20a. Accessed May 2024.
MacKenzie EJ, Rivara FP, Jurkovich GJ, Nathens AB, Frey KP, Egleston BL, Salkever DS, Scharfstein DO. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354(4):366–78. https://doi.org/10.1056/NEJMsa052049.
Gomez D, Alali AS, Haas B, Xiong W, Tien H, Nathens AB. Temporal trends and differences in mortality at trauma centres across Ontario from 2005 to 2011: a retrospective cohort study. CMAJ Open. 2014;2(3):E176–82. https://doi.org/10.9778/cmajo.20140007.
Funding
No funding was received for the writing of this paper. BN receives salary support from Physician Services Incorporated. Physician Services Incorporated did not have any role in the study design, data collection, analysis or writing of this paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gold-Bersani, D., Drennan, I.R., McGowan, M. et al. Field trauma triage criteria associated with need for dedicated trauma center care: a single-center retrospective cohort study. Can J Emerg Med 26, 499–506 (2024). https://doi.org/10.1007/s43678-024-00722-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43678-024-00722-3