
Abstract
Purpose
Pediatric emergency departments are overcrowded, in part due to many non-emergent visits. We aimed to assess the proportion of parents interested in leaving the pediatric emergency department (ED) prior to physician assessment if they could be offered a scheduled community healthcare appointment. We explored differences in care children received in the ED stratified by interest in a community healthcare appointment and parents’ reasons when they were not interested.
Methods
We conducted a 14-item survey within the pediatric ED at a Canadian tertiary care teaching hospital to assess parents’ interest if a program offered community healthcare appointments and we determined preferred appointment characteristics. All parents presenting with children triaged as CTAS 2–5 who met eligibility criteria were approached by a research assistant prior to physician assessment. Surveys were paired with the medical chart outlining the care received. Descriptive statistics and a regression model were used to describe characteristics of families and care received among those who were and were not interested in a community healthcare appointment.
Results
In total, 403 surveys were completed. Overall, 236 participants (58.6%; 95% CI 53.8–63.4) were interested in a community healthcare appointment. In general, parents who were interested in a community healthcare appointment were younger and presented with younger children compared to those who were not interested. Among those interested, there was a preference to have the appointment with a pediatrician or family physician, timely access to an appointment, and appointments scheduled outside of regular business hours.
Conclusion
Our study provides evidence that there is interest in an alternative care access model positioned to reduce pediatric ED congestion. We found that parents would be interested in leaving the pediatric ED in favor of a community healthcare appointment, provided it was with a physician and available in a timely manner.
Résumé
Objectif
Les services d’urgences pédiatriques sont surchargés, en partie à cause des nombreuses visites non urgentes. Nous avons cherché à évaluer la proportion de parents désireux de quitter le service des urgences pédiatriques avant l’évaluation du médecin si on leur proposait un rendez-vous dans un centre de soins de santé communautaire. Nous avons étudié les différences dans les soins reçus par les enfants aux urgences en fonction de leur intérêt pour un rendez-vous dans un centre de soins de santé communautaire et des raisons invoquées par les parents lorsqu’ils n’étaient pas intéressés.
Méthodes
Nous avons mené une enquête de 14 points au sein du service des urgences pédiatriques d’un hôpital universitaire canadien de soins tertiaires afin d’évaluer l’intérêt des parents pour un programme offrant des rendez-vous de soins de santé communautaires et nous avons déterminé les caractéristiques des rendez-vous préférés. Tous les parents se présentant avec des enfants triés selon l’ETG 2–5 et répondant aux critères d’éligibilité ont été approchés par un assistant de recherche avant l’évaluation par le médecin. Les questionnaires ont été associés au dossier médical décrivant les soins reçus. Des statistiques descriptives et un modèle de régression ont été utilisés pour décrire les caractéristiques des familles et les soins reçus parmi ceux qui étaient et n’étaient pas intéressés par un rendez-vous en soins de santé communautaire.
Résultats
Au total, 403 enquêtes ont été réalisées. Dans l’ensemble, 236 participants (58,6%; IC à 95% 53,8–63,4) étaient intéressés par un rendez-vous en soins de santé communautaires. En général, les parents intéressés par un rendez-vous dans les soins de santé communautaires étaient plus jeunes et se présentaient avec des enfants plus jeunes que ceux qui n’étaient pas intéressés. Parmi les personnes intéressées, on note une préférence pour un rendez-vous avec un pédiatre ou un médecin de famille, un accès rapide à un rendez-vous et des rendez-vous fixés en dehors des heures normales de bureau.
Conclusions
Notre étude montre qu’il existe un intérêt pour un modèle d’accès aux soins alternatif destiné à réduire l’engorgement des urgences pédiatriques. Nous avons constaté que les parents seraient intéressés à quitter le service d’urgence pédiatrique en faveur d’un rendez-vous de soins de santé communautaires pourvu qu’il soit avec un médecin et disponible en temps opportun.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
What is known about the topic? |
Overcrowding in pediatric emergency departments (ED) is often a result of high volumes of low-acuity visits. |
There is a need for novel strategies to reduce the impact of low-acuity visits on the pediatric ED. |
What did this study ask? |
What proportion of families within the pediatric ED would prefer a community healthcare appointment rather than waiting to receive care? |
What did this study find? |
Most parents surveyed indicated they would be interested in a community healthcare appointment. |
Why does this study matter to clinicians? |
We identify the feasibility of a novel initiative to reduce the impact of low-acuity visits to the pediatric ED. |
Introduction
The emergency department (ED) is designed to handle acute presentations, but round the clock availability also makes the ED a convenient and accessible point of care when there is limited access to other settings [1,2,3,4,5,6,7,8]. Volumes within pediatric EDs increased by 27% from 2010 to 2014 (9). Such increased demand in the face of fixed or unmatched growth in ED capacity places strain on the pediatric ED and contributes to crowding. Overcrowding is associated with increased morbidity, wait times, delays in care, patients leaving without being seen, increased hospital admissions, and decreased patient satisfaction [9,10,11,12,13,14,15,16].
Crowding in pediatric EDs is largely due to a high volume of visits for low acuity concerns, which are estimated to represent as many as 58–82% of presentations [1, 15,16,17,18,19]. Approximately 55% of all children presenting to Ontario EDs were triaged using Canadian Triage and Acuity Scale (CTAS) as low acuity (level 4 or 5), with 90% of children discharged home from the ED [20]. This problem may be amplified in the wake of recent public health events; following COVID-19, the rate of children age 0–4 visiting the ED has almost doubled from pre-pandemic rates [21]. Further, many pediatric visits to the ED require only a history and physical examination. When investigations do occur, they are commonly those readily accessible to community healthcare providers (such as X-ray, urinalysis, or throat swab) [22]. Studied interventions, focusing on reducing the number of non-emergent visits presenting to the pediatric ED, have aimed to divert non-emergent visits by educating parents about what conditions represent an emergency and sought to improve the access to community healthcare settings [21, 23,24,25,26,27]. So far no strategy has consistently demonstrated an improvement in measures of pediatric ED performance—wait time, length of stay, or the rate of ‘left without being seen’—likely because these interventions rely on families self-determination of urgency and underestimate their needs for external reassurance when making healthcare utilization choices [21, 28, 29].
Combining the nature of most pediatric ED presentations and the need for support in assessing urgency of needs for families, redirecting non-emergent visits to community healthcare settings after triage in an ED may be a strategy that both reassures families, overcomes barriers to access community care, and reduces the impact on pediatric ED congestion. Similar programs have been trialed in adult EDs with mixed results and study quality but this strategy has not been considered in a pediatric setting where reassurance may be more important [30,31,32,33,34]. In this study, we sought to determine the proportion of parents who would be interested in leaving the pediatric ED, prior to being seen by a physician, in favor of a scheduled community healthcare appointment.
Methods
Study design and time period
This cross-sectional study was conducted between May 2021 and September 2021 at the BC Children’s Hospital ED, a Canadian tertiary care teaching hospital whose pediatric ED receives nearly 50,000 visits annually. All parents or guardians (herein parents) who presented to the ED with a child (age < 18) and assigned a CTAS category 2–5 by our triage nurses were considered for inclusion. Exclusion criteria were: (1) families of children who presented with an obvious need for ED services (respiratory distress, visible extremity deformity, lacerations, and those requiring immediate resuscitation); (2) presenting concern which involved mental health or behavioral issues; (3) the patient was transferred or directly referred to the ED by another physician or healthcare facility; (4) no parent was present; (5) the family was not able to provide informed consent or complete the survey in English.
Participants were recruited using random cluster sampling, approaching all eligible patients presenting to the ED between 1000 and 2200 h during a specified 2-h period each day on a rotating cycle to capture time and day variability (ex: Monday 0800–1000 h, Tuesday 1000–1200 h, Wednesday 1200–1400 h with this pattern continuing onwards).
Research assistants approached eligible parents after triage, once they had been moved from the waiting area to an examination room, prior to physician assessment. If consent was provided, surveys were completed electronically and after the visit, paired with the medical chart documenting the ED visit. We developed our 14-item survey by adapting a survey used to assess parent perspectives about neonatal visits to the ED, survey questions focused on parent interest and preferred characteristics of community healthcare appointments [35].
Outcome measures
The primary outcome measure was the proportion of parents who indicated they would be interested in a scheduled community healthcare appointment as an alternative to waiting for care in the ED, (herein referred to as ‘community healthcare appointment’). We were focused on the proportion of parents who indicated they would be interested in a community healthcare appointment and identifying the preferred characteristics of these visits. Additional variables of interest included characteristics of the concern prompting an ED visit, care received within the ED, and reasons provided when a community healthcare appointment was not preferred.
Data analysis
We used descriptive statistics to summarize and compare demographics, survey responses, and clinical variables stratified by those who were and were not interested in a community healthcare appointment. Pearson χ2 or Fisher’s exact tests were completed to assess differences between groups where appropriate. Two-sided p values < 0.05 were considered statistically significant. A logistic regression was completed to assess if the visit day/time or the time from triage to survey completion was associated with parent interest in a community healthcare appointment. Analyses were completed using R statistical software.
Results
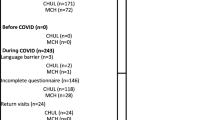
During the times our team was recruiting participants, 1165 individuals visited the ED and 696 were eligible to participate. Among those eligible, 403 individuals were interested in the study, provided consent, and completed the survey. In 391 cases, the survey could be paired with the medical chart documenting the ED visit. Overall, 167 participants (41.4%; 95% CI 36.6–46.2) indicated that they would prefer to complete their assessment and care in the ED and declined a community healthcare appointment, and 236 participants (58.6%; 95% CI 53.8–63.4) indicated that they would favor a community healthcare appointment in lieu of waiting to receive care in the ED.
Table 1 summarizes the characteristics of children visiting the pediatric ED and parent respondents. In general, those who were interested in a community healthcare appointment were younger parents (< 35 years) and those presenting with younger children. Parents coming to the pediatric ED with a male child were less likely to be interested in a community healthcare appointment.
Table 2 describes the characteristics of pediatric ED visits, and parents’ expectations at this visit. Parent interest or lack of interest in a community healthcare appointment was not distinguishable by reason for the ED visit. The reason for ED visit was parent reported. In general, parents had been concerned about the medical problem for < 24 h and majority expected to wait between 1 and 4 h before seeing a doctor in the ED.
A logistic regression model was completed to determine if there was an association between parent interest in a community healthcare appointment and covariates of interest. Covariates included variables that were significant in our univariate analyses (child age, child sex, and parent age) as well as the time/day a visit occurred and the length of time from triage completion to survey completion. Regression results are summarized in Table 3. When adjusting for other covariates, child gender was associated with parent interest in a community healthcare appointment. Specifically, the odds that a parent will be interested in a community healthcare appointment are 54% higher for female children when adjusting for child age, parent age, visit time, and time from triage to survey completion.
Table 4 summarizes interventions received by patients during the ED visit. The proportion of children who received oral medications or required a procedure during their pediatric ED visit was significantly higher among those who declined a community healthcare appointment. Few children in our sample required IV fluids. Among those who were and were not interested in a community healthcare appointment, there were no significant differences in how frequently children required laboratory investigations, imaging, or a hospital specialist consultation/admission to hospital.
Parents who indicated they would be interested in a community healthcare appointment were asked about preferred characteristics of this visit, responses are summarized in Table 5. Most parents indicated that a community healthcare appointment would only be acceptable if it was on the day of, or the day following, their presentation in the ED (63.1% and 26.3%, respectively). Parents expressed a preference to receive care from a pediatrician (82.2%) or family doctor (59.7%) compared to appointments with a nurse practitioner (28.0%). While many parents (65.7%) indicated that appointment times within business hours (Monday–Friday 8 am–5 pm) would be acceptable, more parents (81.4%) indicated that a convenient appointment time would be outside of business hours.
Parents who declined the community healthcare appointment option were asked about their reason for choosing to wait in the pediatric ED; 149 (89.2%) provided a response. Parents indicated that they were not interested in a community healthcare appointment because the pediatric ED was convenient (44.3%), they perceived a need for emergent care (31.5%), they perceived a need for hospital-based management (16.1%), or they believed the ED to be a superior location to receive care (8.1%).
Discussion
Interpretation of findings
Our study provides insight into a novel approach to manage the high volume of visits to the pediatric ED by determining parents’ interest in accepting a scheduled community healthcare appointment in lieu of waiting. We found that, if this offering was available, most parents (58.6%; 95% CI 53.8–63.4) would be interested in accepting a community healthcare appointment and forgo pediatric ED assessment. Preferred characteristics for these visits included care provided by a pediatrician or family physician, timely access to these appointments, and appointments outside of business hours. Interest in a community healthcare appointment was significantly higher among parents < 35 years (33.4% and 19.8% respectively, p value = 0.04) and among those presenting with younger children (average child age among those interested was 3 years, average age of those not interested was 6 years, p value = 0.01). The majority of children whose parents were not interested in a community healthcare appointment required only oral medications in the ED, which could have been provided in an outpatient setting; however, 10.8% did receive a procedure (such as casting or suture placement) in the ED.
Comparison to previous studies
Most (63.1%) parents indicated community healthcare appointments would need to be provided the same day; 26.3% of parents indicated that they would be interested in an appointment if it was offered by the following day. This finding aligns with those found in a survey of parents of neonates which found that 44% of ED visits would have been prevented by a same day appointment with a healthcare provider [35]. When parents indicated they were not interested in a community healthcare appointment, the most common reasons parents declined a community healthcare appointment was the belief that their child required emergent care; this echoes other research exploring parents motives for bringing their child to the ED [36,37,38,39]. Interestingly, while there were few children in our sample who required a procedure in the pediatric ED, we did find that children of parents who were interested in leaving the ED were less likely to have a procedure completed (5.3% vs. 10.8% respectively, p value = 0.03).
The pediatric literature is currently divided about the impact of parent and child age on care seeking behavior. For example, some studies find that older parents are more likely to view their child’s health unfavorably and believe the ED is the best location to receive care [38, 40]. Meanwhile, other studies have found that parents more commonly view a younger child’s illness as an emergency [41] and younger parents are more likely to prefer the pediatric ED [42]. Importantly, our work considers parents who have already determined that their child requires care and have already arrived in the ED. We find there is significantly higher interest in community healthcare appointments among younger parents and parents presenting with younger children. These findings suggest that community healthcare appointments may be viewed by this group as an even more convenient option compared to waiting for care in the pediatric ED. It is also possible that once younger parents are triaged in the ED they are reassured about their child’s health and become interested in alternative care locations.
Strengths and limitations
This study took place at a single center in an affluent urban neighborhood, and our results may not be representative an all parents who access the pediatric ED with their children. Parent responses to this hypothetical program may not reflect the true uptake if this program was operational, meaning the impact of this program on ED volumes is not yet known. Additionally, seasonal variability in the types of presenting concerns and pediatric ED volume may influence parents’ interest in an alternative appointment but was not controlled for as our enrollment period was limited to 5 months (May–September). We also did not assess if parents had a primary care provider or if they attempted to access alternate care for their child prior to presenting to the pediatric ED. It is possible that a subset of parents who declined to accept a community healthcare appointment did so as they had previously accessed alternative care, making them less interested in a community healthcare appointment. However, this did not emerge as a common reason for declining to accept a community appointment. Finally, our research team approached parents once they had been moved to an examination room meaning parents had already waited in the ED. However, regression results show that the time from triage to survey completion was not associated with parent responses.
Clinical implications
The substantial interest in community healthcare appointments expressed by parents indicates that a program with this offering may be a feasible way to meaningfully reduce the number of patients requesting treatment within the pediatric ED. If this program became available in pediatric EDs, we anticipate that crowding in the pediatric ED would reduce and care may improve for both patients who remain in the pediatric ED and those who receive a community healthcare appointment.
Research Implications
Knowing that there is substantial parent interest in community healthcare appointments, additional investigations are needed to better understand how to design and implement this program. Our team is currently designing studies to assess who could safely be offered community healthcare appointments, the logistics of providing this service, and the impact this may have on operations within the pediatric ED.
Conclusion
We identified that parents were interested in leaving the pediatric ED in favor of accepting a timely community healthcare appointment with a physician. Based on these responses, our work highlights an opportunity to develop a new program with potential to reduce the impact of overcapacity problems within the pediatric ED.
References
Berry A, Brousseau D, Brotanek JM, Tomany-Korman S, Flores G. Why do parents bring children to the emergency department for nonurgent conditions? A qualitative study. Ambul Pediatr. 2008;8(6):360–7.
Affleck A, Parks P, Drummond A, Rowe BH, Ovens HJ. Emergency department overcrowding and access block. Can J Emerg Med. 2013;15(6):359–70.
Haltiwanger KA, Pines JM, Martin ML. The pediatric emergency department: a substitute for primary care? Calif J Emerg Med. 2006;2:26.
Bazaraa HM, Houchi SE, Rady HI. Profile of patients visiting the pediatric emergency service in an Egyptian University Hospital. Pediatr Emerg Care. 2012;28(2):148–52.
Bhat I, Wani M, Jogi M, Qazi I, Gurgani S, Hassan Z. Demographic profile of paediatric patients and their parents visiting paediatric emergency in urban tertiary care Hospital and parental reasons for nonemergency visits. Int J Med Sci Curr Res IJMSCR. 2020;3(1):32–42.
Akbayram HT, Coskun E. Paediatric emergency department visits for non-urgent conditions: can family medicine prevent this? Eur J Gen Pract. 2020;26(1):134–9.
Kubicek K, Liu D, Beaudin C, Supan J, Weiss G, Lu Y, et al. A profile of nonurgent emergency department use in an Urban Pediatric Hospital. Pediatr Emerg Care. 2012;28(10):977–84.
Phelps K, Taylor C, Kimmel S, Nagel R, Klein W, Puczynski S. Factors associated with emergency department utilization for nonurgent pediatric problems. Arch Fam Med. 2000;9:1086–92.
Doan Q, Wong H, Meckler G, Johnson D, Stang A, Dixon A, et al. The impact of pediatric emergency department crowding on patient and health care system outcomes: a multicentre cohort study. Can Med Assoc J. 2019;191(23):E627–35.
Tekwani KL, Kerem Y, Mistry CD, Sayger BM, Kulstad EB. Emergency department crowding is associated with reduced satisfaction scores in patients discharged from the emergency department. West J Emerg Med. 2013;14(1):11–5.
Singer AJ, Thode HC, Viccellio P, Pines JM. The association between length of emergency department boarding and mortality. Acad Emerg Med. 2011;18(12):1324–9.
Sun BC, Hsia RY, Weiss RE, Zingmond D, Liang LJ, Han W, et al. Effect of emergency department crowding on outcomes of admitted patients. Ann Emerg Med. 2013;61(6):605–11.
Guttmann A, Schull MJ, Vermeulen MJ, Stukel TA. Association between waiting times and short term mortality and hospital admission after departure from emergency department: Population based cohort study from Ontario Canada. BMJ. 2011;342:d2983.
Simon HK, Hirsh DA, Rogers AJ, Massey R, DeGuzman MA. Pediatric emergency department overcrowding: electronic medical record for identification of frequent, lower acuity visitors. Can we effectively identify patients for enhanced resource utilization? J Emerg Med. 2009;36(3):311–6.
Depinet HE, Iyer SB, Hornung R, Timm NL, Byczkowski TL. The effect of emergency department crowding on reassessment of children with critically abnormal vital signs. Acad Emerg Med. 2014;21(10):1116–20.
Chan M, Meckler G, Doan Q. Paediatric emergency department overcrowding and adverse patient outcomes. Paediatr Child Health. 2017;22(7):377–81.
Alele FO, Emeto TI, Callander EJ, Watt K. Non-urgent paediatric emergency department presentation: a systematic review. J Paediatr Child Health. 2019;55(3):271–7.
Sinclair D. Emergency department overcrowding-implications for paediatric emergency medicine. Paediatr Child Health. 2007;12(6):491–4.
Pileggi C, Raffaele G, Angelillo IF. Paediatric utilization of an emergency department in Italy. Eur J Public Health. 2006;16(5):565–9.
Ehrlich N, Tasmin F, Safi H, Barnett J, Lasley B. Pilot study of ER utilization at Tulsa hospitals. J Okla State Med Assoc. 2004;97(2):64–8.
NACRS emergency department visits and lengths of stay [release summary]. [Internet]. Canadian Institute for Health Information. 2023. https://www.cihi.ca/en/nacrs-emergency-department-visits-and-lengths-of-stay.
Canadian Institute for Health Information. Emergency departments and children in Ontario [Internet]. Canadian Institute of Health Information; 2008. https://secure.cihi.ca/free_products/aib_apr24_08_en.pdf.
Farion KJ, Wright M, Zemek R, Neto G, Karwowska A, Tse S, et al. Understanding low-acuity visits to the pediatric emergency department. PLoS ONE. 2015;10(6):e0128927.
Franco SM, Mitchell CK, Buzon RM. Gatekeeping: a key to reducing emergency department use. Clin Pediatr (Phila). 1997;36:63–8.
Derlet RW, Richards JR. Overcrowding in the Nation’s Emergency Departments: complex causes and disturbing effects. Ann Emerg Med. 2000;35(1):63–8.
Herman AD, Mayer GG. Reducing the use of emergency medical resources among Head Start families: a pilot study. J Community Health. 2004;29(3):197–208.
Wang C, Villar ME, Mulliganm DA, Hansem T. Cost and utilization analysis of a pediatric emergency department diversion project. Pediatrics. 2005;116(5):1075–9.
Gadomski AM, Perkis V, Horton L, Cross S, Stanton B. Diverting managed care Medicaid patients from pediatric emergency department use. Am Acad Pediatr. 1995;95(2):170–8.
Canadian Institute for Health Information. Annual Report 2020 [Internet]. Canadian Institute for Health Information; 2020. https://secure.cihi.ca/free_products/how-canada-compares-cmwf-survey-2020-chartbook-en.pdf.
Washington DL, Stevens CD, Shekelle PG, Baker DW, Fink A, Brook RH. Safely directing patients to appropriate levels of care: guideline-driven triage in the emergency service. Ann Emerg Med. 2000;36(1):15–22.
Washington DL, Stevens CD, Shekelle CG, Henneman PL. Next-day care for emergency department users with nonacute conditions: a randomized, controlled trial. Ann Intern Med. 2002;137(9):707.
Doran KM, Colucci AC, Hessler RA, Ngai CK, Williams ND, Wallach AB, et al. An intervention connecting low-acuity emergency department patients with primary care: effect on future primary care linkage. Ann Emerg Med. 2013;61(3):312-321.e7.
Ellbrant J, Åkeson J, Åkeson PK. Pediatric emergency department management benefits from appropriate early redirection of nonurgent visits. Pediatr Emerg Care. 2015;31(2):95–100.
Kirkland SW, Soleimani A, Rowe BH, Newton AS. A systematic review examining the impact of redirecting low-acuity patients seeking emergency department care: is the juice worth the squeeze? Emerg Med J. 2019;36:207045.
Herman A, Young KD, Espitia D, Fu N, Farshidi A. Impact of a health literacy intervention on pediatric emergency department use. Pediatr Emerg Care. 2009;25(7):434–8.
Chande VT, Wyss N, Exum V. Educational interventions to alter pediatric emergency department utilization patterns. Arch Pediatr Adolesc Med. 1996;150:525–8.
Harrold JA, Langevin M, Barrowman N, Sprague AE, Fell DB, Moreau KA, et al. Parental characteristics and perspectives pertaining to neonatal visits to the emergency department: a multicentre survey. CMAJ Open. 2018;6(3):E423–9.
Costet Wong A, Claudet I, Sorum P, Mullet E. Why do parents bring their children to the emergency department? A systematic inventory of motives. Int J Fam Med. 2015;4(2015):1–10.
Cheek JA, Braitberg G, Craig S, West A. Why do children present to emergency departments? Exploring motivators and measures of presentation appropriateness for children presenting to a paediatric emergency department. J Paediatr Child Health. 2017;53(5):451–7.
Burokienė S, Raistenskis J, Burokaitė E, Čerkauskienė R, Usonis V. Factors Determining parents’ decisions to bring their children to the pediatric emergency department for a minor illness. Med Sci Monit. 2017;28(23):4141–8.
Ogilvie S, Hopgood K, Higginson I, Ives A, Smith JE. Why do parents use the emergency department for minor injury and illness? A cross-sectional questionnaire. JRSM Open. 2016;7(3):205427041562369.
Kurt F, Beğde F, Oğuz S, Tekin D, Suskan E. How important are parental age and educational level in nonurgent admissions to the pediatric emergency department? Pediatr Emerg Care. 2020;36(9):414–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest and no financial relationships relevant to this study.
Additional information
Communicated by Simon Berthelot.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Leung, S., McDonald, E., Watson, A. et al. Community healthcare appointments as an alternative to emergency department assessment: an exploration of family acceptability and preferences. Can J Emerg Med 25, 984–991 (2023). https://doi.org/10.1007/s43678-023-00605-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43678-023-00605-z