
Abstract
Osteoid osteoma occurs in various locations in the human body, mostly in the metaphysis and diaphysis of long bones. This article describes a rare case of osteoid osteoma occurring in an intra-articular location, specifically in the lateral tibial plateau of a 40-year-old female patient. The challenge of diagnosing such a pathology in an atypical location was tackled in this article as well as different management options. Arthroscopic resection was opted in this case.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteoid osteoma, comprising about 10% of benign bone tumors, is a benign osteoblastic tumor with a size less than 2 cm [1]. It usually occurs between 10 and 25 years, predominating in males [1]. Most of the times, it is found on the metaphysis and diaphysis of the long bones and presents with pain that worsens at night and relieved by non-steroidal anti-inflammatory drug (NSAID) [2]. On radiographs, it appears as a radiolucent nidus that is surrounded by bone sclerosis [3].
When it has an intra-articular location such as around the knee, both the clinical and radiographic appearances may become atypical, a delay in the diagnosis of this tumor will be observed and it will most probably present a therapeutic problem [3]. We present a case of an osteoid osteoma of the lateral tibial plateau in the right knee.
Case Report
This is the case of a 40-year-old female suffering from a few months’ history of mechanical pain in the lateral compartment of the right knee. There was no traumatic cause. Radiographs of the knee were inconclusive. Therefore, the patient was treated with intra-articular steroid injection followed by a platelet-rich plasma injection without relief. The pain persisted for an additional few months and became worse at night. It was partly relieved by NSAIDS at first, but became resistant later on and the patient became unable to bear weight on the affected limb.
On physical examination, there was swelling and effusion around the knee that limited the patient’s range of motion, and on palpation of the Hoffa pad, there were both tenderness and swelling. Meniscus and patellofemoral signs were absent and laxity tests were normal. Both foot and hip were normal. There was pain of the postero-lateral space of the knee on palpation, forced flexion, distraction and compression.
MRI was done, which showed intra-osseous hypointense lesion with surrounding hyperintense rim measuring 6 mm at the level of the anteromedial epiphysis of the lateral tibial plateau (Fig. 1).

A Sagittal and B coronal views of right knee MRI showing intra-osseous formation at the level of anteromedial epiphysis of the lateral tibial plateau
These findings were suggestive of osteoid osteoma, but needed confirmation with a right knee CT scan. CT scan was done showing a lucent nidus surrounded by sclerotic bone (Fig. 2), and the diagnosis of osteoid osteoma was confirmed.

A Sagittal, B coronal and C axial views of the right knee CT scan showing a lucent nidus surrounded by sclerotic bone suggestive of osteoid osteoma
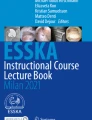
Treatment of this lesion consisted of arthroscopic resection of osteoid osteoma (Fig. 3). Localization of the lesion was achieved with the help of the MRI and CT scan findings in relation to adjacent anatomical landmarks including the distance from the ACL footprint on the medial aspect of the knee and the lateral meniscus.

Intra-operative arthroscopic views showing resection of the intra-osseous osteoid osteoma using an osteotome (A), a curette (B) and a burr (C)
The inflammatory pain symptoms completely resolved on the first day after the surgery and the patient was able to get back to daily life activities with no restrictions. Clinical follow-up done at 1 and 3 months post-operatively showed no residual or recurrent symptoms with patient satisfaction and stoppage of pain medications.
Discussion
In 50% of cases, osteoid osteomas are found in the femoral and tibial diaphysis and are cortical or paracortical in most cases, making it easier to detect and treat [4]. When it is intra-articular, both the diagnosis and treatment become more difficult due to the atypical presentation [5, 6]. This location is rare and affects mainly the hip [7, 8]. When comparing the time to reach the diagnosis of osteoid osteoma, the average was 26.6 months for the intra-articular location compared to 8.5 months for other locations [8]. Especially in the knee, the diagnosis is difficult due to the large number of differential diagnoses such as meniscal problems, tendon lesions, bursopathies, and chondromalacia [3]. When the diagnosis is delayed, effusion accompanies the pain suggesting a wider range of differential diagnoses such as monoarthritis or villonodular synovitis [9]. Also, when misdiagnosed, this tumor can be thought of as anterior gonalgia resistant to all treatments [4]. In fact, the case of our patient was, in the beginning, considered to be arthritis of the knee that was first treated with intra-articular injections without success. Diagnosis was made approximately 24 months later with an MRI, followed by a CT scan that showed typical features of osteoid osteoma, since simple radiographs of the knee were inconclusive.
The radiologic characteristics of osteoid osteoma are absent most of the times when in an articular location. It either shows no signs of osteoid osteoma, or localized osteopenia [7, 8]. To confirm or even detect it, most of the times, a CT scan and MRI are needed [4,5,6]. These examinations will aid in both differentiating this tumor from other diagnoses and in positioning it before the surgery [3, 10]. On CT scan, the contouring sclerosis is often insignificant and central calcifications become denser with the age of the lesion [11]. On MRI, the nidus is not very well defined in half of the cases with variable intensity of peri-nidus and bone marrow edema that can reach surrounding soft tissue, enhancing variably after injection of gadolinium [7, 12]. This bone marrow signal, observed best on T2 images, reflects the age of the tumor being highest in the beginning [11]. Sometimes, scintigraphy is needed to confirm the diagnosis, but it can also miss this tumor if the classical image of “double density” is absent [11]. The advantage of this technique is to find multiple locations of osteoid osteoma in exceptional cases [13]. Although a study by Georgoulis et al. showed that in 40% of cases there was unnecessary arthroscopic investigations [3], Szendroi et al. reported that it was possible to confirm the diagnosis of intra-articular osteoid osteoma in 80% of cases when a careful diagnostic approach was implemented [8]. In our case, we only needed CT scan and MRI to confirm the diagnosis of intra-articular osteoid osteoma, since both imaging modalities showed specific images.
To choose the treatment, one must consider the localization of the nidus to define the nature and size of the lesion [14]. Radiofrequency thermoablation (RFT) is the treatment of choice for osteoid osteomas reporting high rates of success [7]. In addition, higher rates of infection, cartilage destruction and synovial reactions were reported when RFT was used to treat osteoid osteoma in transarticular locations [11]. The patient must also be warned about the degenerative lesions resulting from intra-articular treatment [11]. Depending on the location of the tumor, the use of RFT may cause damage to the cartilage explained by its higher sensitivity to heat than bone [11]. When the heat source is more than 1 cm away from the cartilage, chondrocyte death does not occur [15], which is why in practice it is advised to remain at least 1 cm away from the cartilage. This risk must be compared to other surgical treatments which are more invasive and can affect the cartilage [11]. Krause et al. chose to perform arthroscopic excision of the tumor to prevent any cartilage damage [16], as good outcomes of this surgery has already been described [17]. When it comes to CT-guided percutaneous resection with K-wire, this procedure causes local destruction, does not preserve tissue for histologic examination and sometimes needs revision [18]. Some complications associated with this technique are skin necrosis and burns, osteomyelitis, neuropraxia, and fractures [18]. The en bloc resection technique can guarantee a histologic diagnosis, but it will need bone transplant or osteosynthesis depending on the location due to its requirement of a bigger bone excision than the lesion itself [14]. The location being in a weight-bearing area, it is recommended to fill the bone defect and this graft is mainly taken from the proximal tibial metaphysis [19]. In the above described case, excision of osteoid osteoma was done arthroscopically without any per- or post-operative complications.
Conclusion
Intra-articular osteoid osteoma is a rare entity. Its presentation is atypical and creates a diagnostic and therapeutic problem. The presentation may be atypical, with plain radiographs, MRI and scintigraphy lacking the specific appearance of osteoid osteoma. The treatment options are various and it should be chosen pre-operatively depending on the location and size of the nidus to prevent any cartilage damage.
References
Mastrokalos, D. S., Pässler, H. H., Tibesku, C. O., & Wrazidlo, W. (2001). Computed tomography-guided endoscopic removal of an osteoid osteoma from the femur. Arthroscopy : The Journal of Arthroscopic & Related Surgery, 17(1), 62–66. https://doi.org/10.1053/jars.2001.8023
Chai, J. W., Hong, S. H., Choi, J.-Y., Koh, Y. H., Lee, J. W., Choi, J.-A., et al. (2010). Radiologic diagnosis of osteoid osteoma: From simple to challenging findings. Radiographics, 30(3), 737–749. https://doi.org/10.1148/rg.303095120
Georgoulis, A. D., Soucacos, P. N., Beris, A. E., & Xenakis, T. A. (1995). Osteoid osteoma in the differential diagnosis of persistent joint pain. Knee Surgery, Sports Traumatology, Arthroscopy, 3(2), 125–128. https://doi.org/10.1007/BF01552389
Franceschi, F., Marinozzi, A., Rizzello, G., Papalia, R., Rojas, M., & Denaro, V. (2005). Computed tomography-guided and arthroscopically controlled en bloc retrograde resection of a juxta-articular osteoid osteoma of the tibial plateau. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 21(3), 351–359. https://doi.org/10.1016/j.arthro.2004.10.004
Kartus, J., Ejerhed, L., Sernert, N., Brandsson, S., & Karlsson, J. (2000). Comparison of traditional and subcutaneous patellar tendon harvest: A prospective study of donor site-related problems after anterior cruciate ligament reconstruction using different graft harvesting techniques. The American Journal of Sports Medicine, 28(3), 328–335. https://doi.org/10.1177/03635465000280030801
Eriksson, K., Anderberg, P., Hamberg, P., Löfgren, A. C., Bredenberg, M., Westman, I., et al. (2001). A comparison of quadruple semitendinosus and patellar tendon grafts in reconstruction of the anterior cruciate ligament. The Journal of Bone & Joint Surgery British Volume, 83(3), 348–354. https://doi.org/10.1302/0301-620x.83b3.11685
Allen, S. D., & Saifuddin, A. (2003). Imaging of intra-articular osteoid osteoma. Clinical Radiology, 58(11), 845–852. https://doi.org/10.1016/s0009-9260(03)00213-7
Szendroi, M., Köllo, K., Antal, I., Lakatos, J., & Szoke, G. (2004). Intraarticular osteoid osteoma: Clinical features, imaging results, and comparison with extraarticular localization. The Journal of Rheumatology, 31(5), 957–964.
Kattapuram, S. V., Kushner, D. C., Phillips, W. C., & Rosenthal, D. I. (1983). Osteoid osteoma: An unusual cause of articular pain. Radiology, 147(2), 383–387. https://doi.org/10.1148/radiology.147.2.6836118
Donley, B. G., Philbin, T., Rosenberg, G. A., Schils, J. P., & Recht, M. (2000). Percutaneous CT guided resection of osteoid osteoma of the tibial plafond. Foot & Ankle International, 21(7), 596–598. https://doi.org/10.1177/107110070002100713
Eggel, Y., Theumann, N., & Lüthi, F. (2007). Intra-articular osteoid osteoma of the knee: Clinical and therapeutical particularities. Joint, Bone, Spine, 74(4), 379–381. https://doi.org/10.1016/j.jbspin.2006.10.007
McGrath, B. E., Bush, C. H., Nelson, T. E., & Scarborough, M. T. (1996). Evaluation of suspected osteoid osteoma. Clinical Orthopaedics and Related Research, 327, 247–252. https://doi.org/10.1097/00003086-199606000-00030
Niamane, R., Lespessailles, E., Deluzarches, P., Vialat, J.-F., Maitre, F., & Benhamou, L. C. (2002). Osteoid osteoma multifocally located and recurrent in the carpus. Joint, Bone, Spine, 69(3), 327–330. https://doi.org/10.1016/s1297-319x(02)00402-5
Lindner, N. J., Ozaki, T., Roedl, R., Gosheger, G., Winkelmann, W., & Wörtler, K. (2001). Percutaneous radiofrequency ablation in osteoid osteoma. The Journal of Bone & Joint Surgery British Volume, 83(3), 391–396. https://doi.org/10.1302/0301-620x.83b3.11679
Caffey, S., McPherson, E., Moore, B., Hedman, T., & Vangsness, C. T. (2005). Effects of radiofrequency energy on human articular cartilage: An analysis of 5 systems. The American Journal of Sports Medicine, 33(7), 1035–1039. https://doi.org/10.1177/0363546504271965
Krause, M., Oheim, R., Meenen, N. M., Frosch, K. H., & Amling, M. (2016). Intra-articular osteoid osteoma in the proximal tibia and its imaging characteristics. The Knee, 23(5), 915–919. https://doi.org/10.1016/j.knee.2016.05.005
Abnousi, F., Saliman, J. D., & Fanton, G. S. (2008). Arthroscopic visualization and assisted excision of osteoid osteoma at the knee. The American Journal of Sports Medicine, 36(2), 375–378. https://doi.org/10.1177/0363546507307865
Sans, N., Galy-Fourcade, D., Assoun, J., Jarlaud, T., Chiavassa, H., Bonnevialle, P., et al. (1999). Osteoid osteoma: CT-guided percutaneous resection and follow-up in 38 patients. Radiology, 212(3), 687–692. https://doi.org/10.1148/radiology.212.3.r99se06687
Fukuda, Y., Takai, S., Yoshino, N., Murase, K., Tsutsumi, S., Ikeuchi, K., et al. (2000). Impact load transmission of the knee joint-influence of leg alignment and the role of meniscus and articular cartilage. Clinical Biomechanics (Bristol, Avon), 15(7), 516–521. https://doi.org/10.1016/s0268-0033(00)00013-9
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Standard Statement
This article does not contain any studies with human or animal subjects performed by any of the authors.
Informed Consent
For this type of study informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Daher, M., Aouad, D., Ghanem, W. et al. Intra-articular Lateral Tibial Plateau Osteoid Osteoma: Case Report and Arthroscopic Management. JOIO 57, 983–986 (2023). https://doi.org/10.1007/s43465-023-00886-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43465-023-00886-7