
Abstract
Background
Surgical antibiotic prophylaxis (SAP) has become the standard of care in orthopaedic surgery. Inappropriate usage of antibiotics (dosage, strength, and/or administration time and duration) can inadvertently result in superadded infections and antimicrobial resistance. The purpose of this study was to document and analyse the prescription patterns for SAP, and to investigate the factors associated with divergence from standard guidelines.
Methods
We conducted an online cross-sectional questionnaire-based study to collect information about the SAP practices of the members of the Indian Orthopaedic Association (IOA) using Google forms. A link to the questionnaire was sent by e-mails.
Results
The overall response rate was 5.73%. While 97.3% respondents practised SAP routinely, the practice was not aligned with standard guidelines’ recommendations. There was heterogeneity in the use of SAP in terms of choice of antibiotic(s), number of co-prescribed drugs, single- versus multiple-dose regimens, and the duration of therapy. The prescription practice patterns showed that orthopaedic surgeons almost always used broad-spectrum antibiotics for long durations, regardless of the type of surgery.
Conclusion
While Orthopaedic surgeons in India are practicing SAP, the pattern of antibiotic usage is heterogeneous. Variations were noted in the choice of antibiotics for different types of surgeries, time of administration, duration of usage in the postoperative period as well as co-prescriptions. This study highlights the urgent need for a comprehensive, rational, and robust national SAP policy for orthopaedic surgeries.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Surgical site infections (SSI) are associated with significant morbidity and mortality. Perioperative antibiotic prophylaxis, also frequently known as surgical antibiotic prophylaxis (SAP), is prescribed with the aim to reduce the infection risk in conditions when the internal tissues are exposed to the external environment and has become the standard of care in orthopaedic surgery especially for cases involving the insertion of orthopaedic implants, as the infection once established becomes difficult to eradicate due to biofilm formation over the implanted foreign material [1]. The development of SSI is multifactorial with the number of bacteria present in the surgical wound being an important factor. SAP tries to decrease and delay the bacterial growth allowing the host immune mechanisms to prevent establishment of any infection.
The choice of antimicrobial agent and its duration of administration, to an extent, remains a matter of personal choice as local community standards, bacterial resistance, and local bacterial flora alter the antibiotic prophylaxis that is required [2]. It has been reported that antibiotics are frequently administered inappropriately (strength, dosage, time/duration) which can then result in their increased usage, increased costs and prolonged hospitalisation. The risk of superadded infection and the possibility of antimicrobial resistance (AMR) are increased too [3]. With the limited availability of therapeutic choices, it is imperative to restrict usage of broad-spectrum antibiotics [2]. Administration of SAP is an important component of the WHO surgical safety check list which is used for the prevention of complications [4].
Establishing a rational antibiotic policy is the first step to tackle the imprudent use of antibiotics. In countries where no formal policy on prescription of prophylactic antibiotics exists, or its recommendations are not strictly adhered to, the choices are often driven by individual or treating team’s cumulative experiences. In some counties with existing SAP guidelines/policies, attempts are being made to assess the compliance to those guidelines [1, 5,6,7,8,9]. In India, there have been sporadic attempts limited to a few hospitals [2, 10,11,12]. In 2017, the ministry of health and family welfare, Government of India, puts forward its strategy to deal with increasing AMR [13]. However, its on-field implementation has not been visible due to various reasons, one of the factors being lack of involvement of the major stakeholders [14].
An increased national emphasis on AMR and antibiotic stewardship has driven re-evaluation of antibiotic use in all areas of medicine, including orthopaedic trauma [15]. Analysing the existing variability in prescription practices is the first step towards understanding ‘evidence–practice gap’. To explore this discrepancy, a nationwide survey among orthopaedic surgeons registered with the Indian Orthopaedic Association (IOA) regarding SAP prescription practices in routine clinical situations was conducted. The purpose of the survey was to document and analyse the prescription patterns for SAP, and to investigate the factors associated with divergence, if any, from standard guidelines.
Materials and Methods
This cross-sectional questionnaire-based study was conducted after Institutional Review Board and ethics committee approval (IHEC-LOP/2020/IM0243). The study was designed to be anonymous and no personal details like name, phone number or address were sought, to maintain data confidentiality and maximise participation. The inclusion criteria were consent from the responding surgeons. There were no exclusion criteria. The participation of the respondents was voluntary, and no incentives of any sort were offered in lieu of their participation.
A web-based questionnaire was developed using Google Forms (Google LLC, California) which is free for non-commercial use. It consisted of a total of 23 questions enquiring about the respondents’ age, experience, their workplace, major field of orthopaedic practice, preferred number and type of antibiotic for SAP for elective cases and for open fractures. Additionally, the pattern of prescription of antibiotics in the perioperative period as well as co-prescription of other drugs was enquired. The questionnaire was circulated internally within the department of Orthopaedics and among colleagues of other specialties to examine the comprehensibility of the questions and to iron out ambiguities. Trial runs were performed to ensure that the questionnaire could be filled without glitches. Once satisfied, the collected data was cleared from the database. A link to the questionnaire was generated and was sent by e-mail to the members of the IOA along with a participant information sheet detailing the objectives of the study, information on the confidentiality of the data and the details of investigators to be contacted for any clarification. The e-mails were sent by three of the investigators from their own e-mail addresses starting from 8th March 2020. Two reminder e-mails requesting for participation were sent at an interval of two weeks to maximise the responses. However, the exact timelines were not notified to the participants. The first question of the questionnaire requested for consent for participation and only those respondents who consented could proceed further with other questions. After the first question, there were 22 mandatory questions, of which two had branching options. While the respondents had the option to review their responses prior to submission, a further change of ones’ response was not possible after the final submission. The questionnaire could be submitted only when all the mandatory questions were answered.
The automatically collected data were exported as a Microsoft Excel spreadsheet (Microsoft corp., Redmond, PA). All the responses were scanned for their completeness, and those responses where the participant had not consented and where the responses were either inappropriate or were duplicate, were excluded. Entries with the exact same responses and consecutive time stamps were considered to be duplicates and only one entry was considered for further analysis, which was done using SPSS version 26 (IBM Corp., Armonk, NY) and R Studio desktop (free version, R Studio, Boston, MA). The frequency of responses of individual questions was reported as numbers (percentages). In case of continuous variables, the result was reported in terms of mean, median and standard deviation. Fisher's exact test and Chi-square test were used to examine the significance of the association (contingency) between categorical variables. Further, statistical tests used were ANOVA for continuous variables and Kruskal–Wallis test for categorical variables. Statistical significance was set at ‘p’ < 0.05.
Results
7469 members of the IOA were contacted though e-mails; 362 e-mails could not be delivered due to technical reasons from the e-mail hosting sites. The details of the methodology adopted for data collection and analysis are shown in Fig. 1. The overall response rate to the survey was 5.73%. Table 1 summarises the demographic details of the respondents. The details of prescription practices of the respondents for SAP are shown in Table 2. Table 3 shows the details of antibiotic prophylaxis for open fractures.

Summary of the details of email requests sent and the responses included for final analysis
An inclination was noted for using more than one antibiotic when implant surgery was performed. Of the respondents whose major field of practice was trauma surgery and arthroplasty, 73.54% and 83.33%, respectively, preferred using a single antibiotic for a non-implant surgery but this number fell to 42% and 50%, respectively, when performing an implant surgery. This difference was found to be statistically significant using the Chi-square test (p values 0.000 and 0.002, for major field of practice being trauma and arthroplasty, respectively) (Supplementary Table S1).
Univariate analysis to assess if age, number of years of experience, or the place of work of a respondent had any association with the antibiotic prescription practices was done using one-way ANOVA and Chi-square test (Table 4). The age of a respondent had statistically significant association with the preferred route of post-operative antibiotic administration. Their number of years of experience in orthopaedics was significantly associated with their preference of cephalosporin/penicillin, the route of post-operative antibiotic administration, and the preference of antibiotics used in Gustilo–Anderson (GA) type I and II fractures. The workplace had a significant association with the number of antibiotics used in non-implant and implant surgeries, preference for cephalosporin/penicillin, and the duration of post-operative antibiotic administration. The type of workplace was significantly associated with the preference for cephalosporin or penicillin. The workplace and its type had no association with the preference of antibiotic prescription for SAP in any of the GA types of open fractures. Supplementary table S2 shows further details of the factors which showed statistical significance in univariate analysis.
257 (64.1%) respondents routinely co-prescribed other drugs with antibiotics. While the respondents reported prescribing drugs of varied classes, the most common co-prescription was of a proton pump inhibitor or an H-2 receptor blocker (n = 257), followed by calcium (n = 163), multivitamins (n = 152) and probiotics like spores of Bacillus clausii or lactic acid bacillus (n = 95). With regard to the question of keeping oneself updated on prophylactic antibiotic prescription practices, 62, 52, 16, and 11 respondents kept themselves updated based on scientific papers, conferences, textbooks and information from pharmaceutical representatives, respectively; the rest depended on two or more sources. The preferred source for most was scientific papers (n = 222, 55.4%) (Table 2).
Discussion
Even though the achieved response rate of the present survey was quite low, this was probably the first attempt to ascertain the antibiotic prescription practices of members of the Indian Orthopaedic Association. While we noted heterogeneity in many of the responses, an overwhelming number of orthopaedic surgeons (97.3%) practised SAP routinely.
Elective Surgery/Closed Trauma Surgery
International guidelines recommend that the agent used for SAP should be non-toxic, low cost, having a narrow spectrum with rapid action to be administered as an intravenous single-dose bolus within 30–60 min before the incision; in case the blood loss during surgery is > 1500 ml or if the duration of the surgery is > 240 min, additional doses of antibiotics are recommended. However, the recommended duration of SAP is for no > 24 h postoperatively [16, 17]. In this study, > 90% of surgeons stated administering SAP within one hour of incision and an equal number also reported re-administering antibiotics intra-operatively. However, the timing of the repeat dose and duration of therapy in the postoperative period was diverse (Table 2).
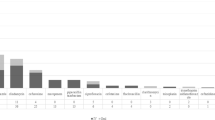
A first- or second-generation cephalosporin is recommended as the antibiotic of first choice, with vancomycin or fluoroquinolone being recommended in cases of beta-lactam allergy; metronidazole is added when prophylaxis against anaerobic bacteria is needed [16, 17]. Although single-dose antibiotic is also at times recommended for clean, non-implant surgery, the strength of evidence for this recommendation is low [16]. The National Centre for Disease Control (NCDC), India has broadly recommended on similar lines while leaving the choice of the prophylaxis to be based on the local antibiogram [18]. For routine orthopaedic surgery, it has recommended intravenous cefuroxime 1.5 g bolus followed by 12-hourly administration for 24 h (maximum) or intravenous cefazolin 2 g bolus; for trauma surgery, the recommendations are either intravenous cefuroxime 1.5 g bolus followed by 12-hourly administration for 24 h or intravenous ceftriaxone 2 g once daily. Figure 2 shows the compliance of the SAP practice of the respondents with NCDC recommendations.

Depicting the concordance of responses with the National centre for disease control (NCDC) guidelines
Most international clinical practice guidelines for SAP recommend the use of cefazolin as the first choice of antibiotic unless contraindicated [16]. In this study, cefazolin was used by < 6% of the respondents. Cefuroxime (39.1%), which is a second-generation cephalosporin, was the most common SAP agent followed by ceftriaxone–sulbactam combination (25.9%). Though we did not specifically enquire the reason for the choice of agent for SAP, availability of cefazolin could be a factor apart from the broader antimicrobial cover (both Gram-positive and -negative) afforded by cefuroxime [2]. Both cefuroxime and ceftriaxone have been reported to reduce the incidence of SSI in orthopaedic surgery [1, 2]. Aminoglycosides (65.8%) were the most common co-prescribed second antibiotic when preferring a combination of antibiotics. When comparing the prescription practice for non-implant versus implant surgery, the majority of respondents (76.6%) preferred using a single drug SAP for the former; while for the latter, 50.9% respondents preferred a combination of two antibiotics of different groups. Almost 60% respondents reported continuing antibiotic prophylaxis in the postoperative period beyond 24 h. Ambiguity in the recommendations in the available literature on single- or multiple-dose antibiotic prophylaxis regimen could be the reason for this practice [19]. Multiple-dose regimens have the potential risk of promoting AMR, while adding to the cost of treatment. The duration of SAP was quite varied with few respondents continuing antibiotics for up to 2 weeks empirically.
Open Trauma Surgery
The responses for looking at the pattern of SAP for open fractures were interesting. While 9% respondents reported that their SAP regimen remained the same as for clean orthopaedic surgery, 78.5% respondents reported variation in SAP regimens depending on the grade of injury. For GA types I, II and III fractures, 57.9%, 51.3% and 9.5% respondents, respectively, preferred using a cephalosporin or penicillin along with an aminoglycoside. Notably, 41.2% and 84.0% respondents preferred using a combination of cephalosporin/penicillin along with an aminoglycoside and metronidazole in GA types II and III fractures, respectively. Five respondents preferred using linezolid along with an aminoglycoside and metronidazole, while one respondent preferred using meropenem alone, in all GA type III fractures.
Globally, the management of open fractures is evolving not only with respect to improved wound management techniques but also with the SAP regimens adapting to emerging evidence, to optimise treatment outcomes. Over the years, routine use of expanded gram-negative coverage with aminoglycosides has decreased in popularity and has been challenged for its utility, efficacy, and tolerability for all patients [15, 20]. There appears to be a trend towards considering only first-generation cephalosporins for GA types I and II fractures as the contamination in these fractures commonly reflects normal skin flora, which are generally covered by a first-generation cephalosporin [15]. These organisms are not the infecting organisms identified in subsequent SSI [21]. For GA type III fractures, treatment with a third-generation cephalosporin is recommended [20, 22]. For soil or potential clostridial contamination, addition of penicillin is recommended [15, 20, 22]. While the use of metronidazole for GA type III fractures was quite frequent among the respondents there appears a need for clear evidence for its use. Another trend regarding the duration of therapy is not to extend it beyond 24–72 h after definitive coverage or debridement and coverage with a sterile dressing [15, 20].
Effect of Age, Years of Experience and Place of Work on Prescription Practice
Respondents younger than 45 years preferred to use intravenous (IV) followed by oral route more commonly than IV route alone (ratio being 2.3:1). However, this ratio was 1.27:1 for those who were older than 45 years. Also, the majority of respondents with ≤ 15 years of experience preferred administering SAP through the IV route followed by oral drugs over IV route alone (2.5:1) in the post-operative period. This ratio for those with > 15 years of experience was 1.25:1. Antibiotic prescription for elective orthopaedic surgery was as per the NCDC guidelines in 45.6% and 43.9% of respondents with experience of ≤ 15 years and > 15 years, respectively.
Of the 307 respondents who preferred a single antibiotic in elective non-implant cases, 139 (45.3%) worked in a private/corporate/trust hospital, 104 (33.9%) worked in a government hospital/institution, while 64 (20.8%) respondents worked in their own hospitals/nursing homes. Among all the respondents working in a private/corporate/trust hospital, 82.2% preferred a single antibiotic for non-implant cases. In cases where an implant was to be used, a greater number of respondents who worked in private/corporate/trust hospitals preferred using a single antibiotic when compared to those who worked in government hospitals (98 and 58, respectively). The preferred cephalosporin was as per the NCDC recommendations in 44.8% (61/136) and 53.8% (91/169) of respondents working in government hospitals and private/corporate/trust hospitals, respectively. Of the 162 participants who administered SAP usually up to 24 h, 88 (54.3%) and 38 (23.5%) worked in private/corporate/trust and government hospitals, respectively, while the rest worked in their own hospitals/nursing homes. The cephalosporin/penicillin of choice was as per NCDC recommendations in 52% and 37.9% of respondents working in a teaching and a non-teaching hospital, respectively.
Co-prescriptions with Antibiotics
Almost 64% of respondents replied in the affirmative regarding co-prescription of other drugs with antibiotics (Table 2). Caution needs to be exercised when co-prescribing proton pump inhibitors or H2-receptor blockers, as these are known to increase the risk of Clostridium difficile infection; while antacids, minerals, and calcium supplements could affect the absorption of oral antibiotics [23, 24]. Multivitamins are found to have a synergistic action with antibiotics and have been suggested as tools to treat multi-drug resistant superbugs [25]. Probiotics help to replenish the natural gastrointestinal flora with non-pathogenic organisms and are frequently promoted as co-prescriptions with antibiotics for the prevention and treatment of antibiotic-associated diarrhoea; however, care needs to be exercised in immunosuppressed patients as sepsis and fungemia associated with their use has been reported [26]. Co-prescriptions of vitamin D have been reported to decrease antibiotic consumption and seem to protect patients from respiratory tract infections [27]. There are mixed reports regarding the use of vitamin C along with antibiotics with synergy as well antagonism reported with various antibiotics and due caution should be exercised in co-prescribing vitamin C with antibiotics [28, 29].
Limitations
We acknowledge the limitations of this study. The overall response rate to the survey was quite poor. One probable reason was the survey being online only and surgeons who are not tech-savvy could not participate. As the e-mails were sent from a pre-existing list of addresses, there is a possibility that some of them were sent to addresses not being actively used by some members which could have affected the response rate. However, we believe that we have served the important purpose of sensitisation of orthopaedic surgeons to this issue of SAP practice. Second, this being a survey also suffered with the inherent limitations of this methodology like non-responder bias, as the prescription patterns of the responders may not reflect the variation within the orthopaedic fraternity, and self-reporting bias, with respondents possibly answering in a way that is a positive reflection of their practice.
Recommendations
The usual fear in the mind of orthopaedic surgeons in India is that ours being a hot and humid country, the risk of co-infection with both gram-positive and -negative organisms is high, and that the prophylactic antibiotics should continue till the epithelisation of a wound occurs [30]. However, in this era of increasing AMR, antimicrobial stewardship from the orthopaedic fraternity is needed to address the challenge of AMR. Discussion on SAP protocols need to be an integral part of our national and state chapter conferences so that broad guidelines may be formulated, which can then be used for expanding the NCDC guidelines.
Conclusion
This survey has brought out the antibiotic prescription practices of members of the IOA. While most of the respondents administer SAP; there is heterogeneity in terms of choice of antibiotic, number of co-prescribed drugs, single- versus multiple-dose regimens, and the duration of therapy. The study shows that orthopaedic surgeons prefer using broad-spectrum antibiotics for a long duration, regardless of the type of surgery.
In this era of increasing AMR, it is high time that the orthopaedic fraternity come together to conduct large, multicentre, well-designed randomised controlled trials to create the evidence for best practice. We believe, with this survey, we have served twin purposes of sensitizing the orthopaedic fraternity to this critical issue and building the database of current practice.
References
Yeap, J. S., Lim, J. W., Vergis, M., Au Yeung, P. S., Chiu, C. K., & Singh, H. (2006). Prophylactic antibiotics in orthopaedic surgery: guidelines and practice. Medical Journal of Malaysia, 61(2), 181–188.
Mathur, P., Trikha, V., Farooque, K., Sharma, V., Jain, N., Bhardwaj, N., et al. (2013). Implementation of a short course of prophylactic antibiotic treatment for prevention of postoperative infections in clean orthopaedic surgeries. Indian Journal of Medical Research, 137(1), 111–116.
Hawn, M. T., & Knowlton, L. M. (2019). Balancing the risks and benefits of surgical prophylaxis: timing and duration do matter. JAMA Surgery, 154(7), 598–599.
Sewell, M., Adebibe, M., Jayakumar, P., Jowett, C., Kong, K., Vemulapalli, K., et al. (2011). Use of the WHO surgical safety checklist in trauma and orthopaedic patients. International Orthopaedics, 35(6), 897–901.
Argaw, N. A., Shumbash, K. Z., Asfaw, A. A., & Hawaze, S. (2017). Assessment of surgical antimicrobial prophylaxis in Orthopaedics and Traumatology Surgical Unit of a Tertiary Care Teaching Hospital in Addis Ababa. BMC Research Notes, 10(1), 160.
Andersson, A. E., Bergh, I., Karlsson, J., Eriksson, B. I., & Nilsson, K. (2012). The application of evidence-based measures to reduce surgical site infections during orthopedic surgery—report of a single-center experience in Sweden. Patient Safety in Surgery, 6(1), 11.
Queiroz, R., Grinbaum, R. S., Galvão, L. L., Tavares, F. G., & Bergsten-Mendes, G. (2005). Antibiotic prophylaxis in orthopedic surgeries: the results of an implemented protocol. Brazilian Journal of Infectious Disease, 9(4), 283–287.
İnan, A. (2011). Antibiotic use and cost in a teaching hospital in İstanbul. Journal of Microbiology and Infectious Disease, 1(3), 128–133.
Şengel, B. E., Bilgin, H., Bilgin, B. Ö., Gidener, T., Saydam, S., Pekmezci, A., et al. (2019). The need for an antibiotic stewardship program in a hospital using a computerized pre-authorization system. International Journal of Infectious Diseases, 82, 40–43.
Bhatnagar, N., Sural, S., Arora, S., Lingaiah, P., & Dhal, A. (2017). Efficacy of single dose versus multiple dose injectable antibiotics in hip joint surgery. Journal of Orthopaedics Trauma Surgery and Related Research, 12(2), 62–65.
Jaggi, N., Nirwan, P., & Chakraborty, M. (2018). Adherence to surgical antibiotic prophylaxis guidelines in an Indian tertiary care hospital. Journal of Patient Safety and Infection Control, 6, 13–18.
Kumari, P., Siddegowda, J. B., & Krishnaiah, V. (2019). Appropriateness and pharmacoeconomics of surgical antimicrobial prophylaxis in open reduction internal fixation surgery practiced in a tertiary hospital compared to recommendations in the national center for disease control guidelines. Perspectives in Clinical Research, 10(4), 172–176.
National Action Plan on Antimicrobial Resistance (NAP-AMR) 2017–2021 [Internet]. National Centre for Disease Control (NCDC); 2017. https://www.ncdc.gov.in/WriteReadData/linkimages/AMR/File645.pdf. Accessed 08 Oct 2020
Ranjalkar, J., & Chandy, S. J. (2019). India’s National Action Plan for antimicrobial resistance—an overview of the context, status, and way ahead. Journal of Family Medicine and Primary Care, 8(6), 1828–1834.
Hand, T. L., Hand, E. O., Welborn, A., & Zelle, B. A. (2020). Gram-negative antibiotic coverage in Gustilo–Anderson type-III open fractures. Journal of Bone and Joint Surgery, 102(16), 1468–1474.
Bratzler, D. W., Dellinger, E. P., Olsen, K. M., Perl, T. M., Auwaerter, P. G., Bolon, M. K., et al. (2013). Clinical practice guidelines for antimicrobial prophylaxis in surgery. American Journal of Health System Pharmacy, 70(3), 195–283.
World Health Organization. Global guidelines for the prevention of surgical site infection. 2016. https://apps.who.int/iris/bitstream/handle/10665/250680/9789241549882-eng.pdf?sequence=8. Accessed 08 Oct 2020
National treatment guidelines for antimicrobial use in infectious diseases version 1.0. National Centre for Disease Control (NCDC); 2016. https://www.ncdc.gov.in/WriteReadData/l892s/File622.pdf. Accessed 08 Oct 2020
Gans, I., Jain, A., Sirisreetreerux, N., Haut, E. R., & Hasenboehler, E. A. (2017). Current practice of antibiotic prophylaxis for surgical fixation of closed long bone fractures: a survey of 297 members of the Orthopaedic Trauma Association. Patient Safety in Surgery, 11(1), 2.
Garner, M. R., Sethuraman, S. A., Schade, M. A., & Boateng, H. (2020). Antibiotic prophylaxis in open fractures: evidence, evolving issues, and recommendations. Journal of American Academy of Orthopaedic Surgeons, 28(8), 309–315.
Lingaraj, R., Santoshi, J. A., Devi, S., Najimudeen, S., Gnanadoss, J. J., Kanagasabai, R., et al. (2015). Predebridement wound culture in open fractures does not predict postoperative wound infection: A pilot study. Journal of Natural Science Biology and Medicine, 6(Suppl 1), S63–S68.
Carver, D. C., Kuehn, S. B., & Weinlein, J. C. (2017). Role of systemic and local antibiotics in the treatment of open fractures. Orthopedic Clinics of North America, 48(2), 137–153.
Kandel, C. E., Gill, S., McCready, J., Matelski, J., & Powis, J. E. (2016). Reducing co-administration of proton pump inhibitors and antibiotics using a computerized order entry alert and prospective audit and feedback. BMC Infectious Diseases, 16, 355.
Ogawa, R., & Echizen, H. (2011). Clinically significant drug interactions with antacids: An update. Drugs, 71(14), 1839–1864.
Shahzad, S., Ashraf, M. A., Sajid, M., Shahzad, A., Rafique, A., & Mahmood, M. S. (2018). Evaluation of synergistic antimicrobial effect of vitamins (A, B1, B2, B6, B12, C, D, E and K) with antibiotics against resistant bacterial strains. Journal of Global Antimicrobial Resistance, 13, 231–236.
Rodgers, B., Kirley, K., & Mounsey, A. (2013). Prescribing an antibiotic? Pair it with probiotics. Journal of Family Practice, 62(3), 148–150.
Norlin, A. C., Hansen, S., Wahren-Borgström, E., Granert, C., Björkhem-Bergman, L., & Bergman, P. (2016). Vitamin D3 supplementation and antibiotic consumption—results from a prospective, observational study at an Immune-Deficiency Unit in Sweden. PLoS ONE, 11(9), e0163451.
Cursino, L., Chartone-Souza, E., & Nascimento, A. M. A. (2005). Synergic interaction between ascorbic acid and antibiotics against Pseudomonas aeruginosa. Brazilian Archives of Biology and Technology, 48(3), 379–384.
Kwiecińska-Piróg, J., Skowron, K., Bogiel, T., Białucha, A., Przekwas, J., & Gospodarek-Komkowska, E. (2019). Vitamin C in the presence of sub-inhibitory concentration of aminoglycosides and fluoroquinolones alters proteus mirabilis biofilm inhibitory rate. Antibiotics, 8(3), 116.
Dhammi, I. K., Ul Haq, R., & Kumar, S. (2015). Prophylactic antibiotics in orthopedic surgery: Controversial issues in its use. Indian Journal of Orthopaedics, 49(4), 373–376.
Author information
Authors and Affiliations
Contributions
Conceptualisation: JAS, PB. Methodology: JAS, MN, RS. Formal analysis and investigation: PB, AC. Writing—original draft preparation: JAS, PB, MN. Writing—review and editing: RS. Funding acquisition: not applicable. Resources: AC (software for statistical analysis). Supervision: RS.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standard statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Human Ethics Committee, All India Institute of Medical Sciences, Bhopal, MP, India, IHEC-LOP/2020/IM0243, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
43465_2020_306_MOESM1_ESM.pdf
Supplementary file1 Shows the relation of the age of the respondent and the years of experience in relation to their major field of orthopaedic practice (PDF 153 KB)
Rights and permissions
About this article

Cite this article
Santoshi, J.A., Behera, P., Nagar, M. et al. Current Surgical Antibiotic Prophylaxis Practices: A Survey of Orthopaedic Surgeons in India. JOIO 55, 749–757 (2021). https://doi.org/10.1007/s43465-020-00306-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43465-020-00306-0