
Abstract
Background
This study aimed to demonstrate the differences in the way cell and gene therapy (CGT) products have been developed and reviewed for approval in Japan, the USA, and the EU by comparing regulations and successfully launched products in each region, and to examine the background to such differences.
Methods
Information on relevant regulations and approved CGT products were collected from the public source and compared by region.
Results
While regulations on CGT products are largely consistent among these regions, some differences could have a substantial impact on the practices defining CGT products, the timing of responses required to comply with the regulations for handling gene-modified organisms, and the acceptable validation processes under good manufacturing practice regulations. Although CGT products are given some preferential status in all regions, the preferential treatment given to CGT products varies across regions. The CGT products launched in each region also differ significantly in type, indications, the nature of the developers, and the clinical evidence submitted. While all the cellular products launched in Japan were approved based on small uncontrolled trials, most cellular products in the USA and EU were approved based on controlled studies. A trend was observed for companies to enter their home markets.
Conclusion
Our study showed differences of regulations on CGT products and of features in approved products as well as the trend of their home market entries, which may have been driven by a different context than that of traditional pharmaceuticals.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cell and gene therapies (CGTs) are expected to provide a new therapeutic approach in disease areas with no treatment options or where conventional therapies have failed to produce satisfactory therapeutic outcomes. Industries have invested heavily in these areas [1, 2]. The development of CGT products has been accelerating worldwide since 2000, and the number of approved CGT products has increased in the 2010s [3,4,5]. The industrial development of CGT products is a target for both regulations and industry support [6, 7].
CGTs are different from traditional drugs in that they involve processing living cells, administering genetically modified cells, and expressing genes of interest in the human body. Companies must take on many challenges in the research and development (R&D) stages of these products to achieve their expected quality and safety, some of which may involve high costs. Although developers follow the existing guidelines by International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) for biopharmaceuticals, they also refer to their own regional CGT regulations and consult with regulatory authorities on any requirements that are not explicitly stated. Owing to the lack of experience of developers and regulators and variations in requirements among regions, the resources and time required for development depend on the characteristics of the product and the market in which it is intended to be launched.
Apparent differences in regulations in different countries can be clarified through a careful comparison of their laws and regulatory guidelines. Furthermore, to examine the background factors that lead to such differences and their impact on global industries, it is necessary to analyze the differences in regulations to the differences in products actually developed and launched in each country. However, it is challenging to analyze the relationship between CGT product development and the relevant regulations because CGT products have diverse properties and applications. Furthermore, the number of approved CGT products remains small compared to other common drugs, and companies entering the market are different from traditional pharmaceutical companies. The endogenous nature of regulations in each country, as they arise and change in response to the importance of their own industries and healthcare needs, is another reason why analyzing the impact of regulations can be difficult.
The aim of this study is to demonstrate the differences in the way CGT products have been developed and reviewed for approval in Japan, the USA, and the EU by comparing regulations and successfully launched products in each region, and to examine the background to such differences. Specifically, we investigated how CGT products are positioned within the framework of pharmaceutical regulations and marketing approval review. The characteristics of the approved products (i.e., applicants and their corporate nationalities, product types, indications, development time, review time, main clinical study information, and applied regulatory frameworks) in each region were investigated to determine whether any characteristics differed by region. We also discussed if there is any relationship between country-specific regulations for CGT products and the characteristics of the products launched and whether the approval framework applied contributes to early access to the products in each country.
Methods
Information on regulations and review frameworks was obtained from the websites of regulatory authorities in Japan (PMDA/MHLW), the USA (FDA), and the EU (EMA). The cutoff date for information and data collection was set at December 31, 2020 at the submission of this article. During its review we updated the information to include data through June 30, 2022. The information collected included laws and regulations defining CGT products, review frameworks, the timing of clinical trials and application for marketing approval, and the requirements related to genetically modified organisms, manufacturing and quality control. We also referred to descriptions of these regulations in previous studies [7,8,9,10,11,12].
Information on approved products was collected from public sources, review reports, and PharmaProjects® (Informa PLC). Indications were classified using the International Classification of Diseases 11th revision (ICD 11). The Clinical Trial Notification (CTN) submission date was used for Japan and the Investigational New Drug (IND) submission date for the USA for the start date of clinical development. Since the date of clinical trial application (CTA) submission in the EU is not publicly available, the date when the first country approved the trial in the EU Clinical Trial Register was set as the start date. When these data were not available from public source, actual study start dates based on review reports or descriptions in clinical study database were applied. For multinational trials, we adopted the start date of the country in which the trial was initiated. Designations refer to rare diseases, priority reviews, and special designations for innovative products (e.g., Sakigake in Japan, Fast track/Breakthrough therapy/RMAT in the USA, and PRIME in the EU). The characteristics of the main clinical trials, including phase, single/multicenter, randomization, blinding, control arm setting, and the number of participants, were collected. Development time was defined as the time from the start of clinical development to the date of the marketing authorization application. Review time was calculated by subtracting the application date from the approval date. For applications that were withdrawn and then reapplied, the review time was the sum of these two periods, the application date from the withdrawal date and the reapplication date from the final approval date.
Due to the different regulatory definitions of CGT products in the three regions, we tentatively classified them in this study as follows: cell therapy products (CTP), ex vivo gene therapy products (GTPe), and in vivo gene therapy products (GTPi). GTPe and GTPi are collectively referred to as GTP. Since the production and treatment with heterologous hematopoietic stem cell transplantation (HSCT) products are currently handled in medical practice in hospitals in Japan and the EU, we excluded HSCT products from this study [4].
Results
Regulations on CGT Products in the Three Regions
Our comparison of the regulations regarding CGT products in the three regions revealed differences in the definition of CGT products, conditional approval system, designation of innovative products, procedures for initiation of clinical trials for GTP, and manufacturing and quality control regulation (Table 1, and detailed information is shown in Online Resource 1).
The legal and regulatory frameworks of CGT products in the three regions were distinctly different. The USA handles CGT products under regulations for pharmaceuticals and medical devices [13, 14]. The EU treats CGT products as pharmaceuticals but created a new category called “Advanced Therapy Medicinal Products (ATMP) [15]”. Japanese regulations define CGT products as “Regenerative Medical Products (RMP),” which are different from pharmaceuticals and medical devices [8, 16].
The basic principle for the review and approval of CGT products is common in all three regions: Approval is granted even with limited study results, priority review is available, and there are provisions for innovative products with a new mechanism of action, potential to address unmet medical needs or severe conditions, or a potential for significant efficacy. However, region-specific provisions exist. For example, conditional and time-limited approvals are applicable to CGT products in Japan without the need for serious conditions. In contrast, there are requirements of disease severity for accelerated approval and conditional approvals in the USA and EU.
The USA introduced the regenerative medicine advanced therapy (RMAT) designation as a special framework for advanced therapies, including CGT products. This is a measure to promote CGT development by supporting applications for accelerated approval [17]. The objective of conditional and time-limited approvals in Japan is to expedite access, especially for CTPs with heterogeneous quality, since using traditional statistical criteria would require a long time to confirm their efficacy. It is also referred to as “provisional” approval, and an application for formal approval is required within 7 years [16]. Japan has a system called “Sakigake (pioneer)” designation that aims to promote the development of innovative products. To qualify for the “Sakigake” designation, which gives various priorities in the review process, a new drug application (NDA) must be filed in Japan before (or at least at the same time as) an application is filed elsewhere [18, 19].
There are differences in the procedures used to initiate clinical trials using genetically modified organisms (GMOs). The environmental assessment of GMOs for GTPs is a common requirement in all regions, but the scope and operation of this requirement differ [10]. In the USA, a categorical exclusion is applied to GTPs for INDs because of their limited use, exempting these products from environmental assessments. In addition, GTPe can also be exempted as per the guideline for environmental assessments for gene therapies, even for BLAs [20]. In Japan, under the Cartagena Act, a full environmental impact assessment had to be submitted for review to obtain approval for the use of GMOs (Type I Use approval) before submitting CTNs [21]. Recently, this timeline has been slightly relaxed, that is, Type I Use approval is now necessary before the first patient enrolment in Japan instead of CTN submission [22]. Furthermore, domestic manufacturing sites must undergo the same review before starting the production of investigational products (Type II Use confirmation). For GTPe, genetically modified cells themselves are not regulated; however, in case infectious viral vectors remain in the final products, it should be noted that residual vectors are regulated in Japan [23]. In the EU, except for a few countries, the GMO review process is conducted in parallel in each country at the time of the CTA reviews [10].
Variations in the regulations for the manufacturing and quality control of CGT products also exist among the three regions. Good manufacturing practice (GMP) is applied to CGT products and pharmaceuticals. In Japan, when CGT products were introduced as a new category of products different from pharmaceuticals, GMP specifically for CGT products (Good Gene, Cellular, and Tissue-based Products Manufacturing Practice; GCTP) was established and has been applied ever since [24]. Subtle differences exist between GCTP and traditional GMP. For example, the verification approach, an alternative to conventional process validation (PV), can also be applied to GCTP. This enables a manufacturer to report their process validation results after evaluating the data accumulated during commercial manufacturing. For autologous CTPs, PV is very challenging because of the limited patient material. By applying a verification approach, applicants can start commercial manufacturing before completing PV to demonstrate process robustness in the future based on their accumulated commercial production data. The EU-GMP also has provisions for CGT products. An annex for ATMP has been created in the EU-GMP, which includes provisions that allow the release of out-of-specification products [25]. In autologous CTP and GTPe, out-of-specification tends to occur more commonly than in traditional pharmaceuticals because of the nature of living cells as source materials. Annex 4 of the EU-GMP contains provisions addressing medical needs for serious conditions when alternative products are not available.
CGT Products Approved in the Three Regions
The types and natures of approved products differed from region to region (Table 2, and the list of approved products is shown in Online Resource 2).
As of June 30, 2022, there were 16, 15, and 21 CGT products approved in Japan, the USA, and the EU, respectively. Observing the applicants’ nationalities for these products, we found that companies generally prefer to enter their home markets: 75% (12/16) in Japan, 87% (13/15) in the USA, and 43% (9/21) in the EU (Online Resource 2). The rest of the European entrants were US firms. Eight products made by Japanese companies were approved only in Japan. US companies received 27 approvals for 15 products. European companies obtained 13 approvals for 11 products.
Regarding the type of approved products, the proportion of CTPs was higher in Japan than in the USA and EU. The proportion of GTPe in the EU was relatively higher than that in Japan and the USA. Only three of the 18 CTPs had multi-regional approval, compared to 55% (6/11) for GTPe and 50% (3/6) for GTPi, showing that CTPs were less likely to be approved in multiple regions compared to GTPs. The proportion of products targeting tumors was higher in the USA and EU than in Japan. The proportion of products designated for innovative products (Japan: “Sakigake,” the USA: fast track/breakthrough therapy/RMAT, the EU: PRIME) tended to be higher in the USA.
The percentage of conditional approvals with limited evidence was lower in the USA. More than ten products were eligible for or applied for priority review in each region, but there was only one product whose review was completed within the target priority review time in the EU. Seven products were withdrawn from the EU while two products in the USA and no product in Japan were withdrawn.
Clinical Development and Approval Review of CGT Products in the Three Regions
The clinical data packages submitted for approval differed for each region (Table 3, and the comparison of CTP and GTP populations is shown in Online Resource 3). Overall, the CGT products approved in Japan were based on weaker evidence than those approved in the USA and EU.
The data packages included single-center trials in all three regions and a few trials were blinded. The percentage of products for which phase III trial results were less than 50%. The number of CGT products approved that submitted data from randomized and controlled trials was lower in Japan than in the USA or the EU. Reflecting these differences, the sizes of the main studies, as the total number of subjects, submitted in Japan were much smaller than those submitted to the USA and EU. The smallest study submitted to Japan had a sample size of two. This contrast was even more pronounced for cell therapy products. While almost all CTPs in the USA and EU reported the use of controlled trials, no products in Japan had controlled trials. Comparing the study sizes between cell and gene therapies, we found that the study size was generally larger for CTPs than for GTPs in the USA and EU, but the reverse was true in Japan (Online Resource 3).
For ex vivo and in vivo gene therapy products approved only in the EU for the treatment of hereditary diseases (e.g., Strimvelis, Zynteglo, Libmeldy, and Glybera), it is not feasible to conduct clinical trials with appropriate control groups. The study sizes for these products ranged from 12 to 45 patients, with only 12 to 27 patients receiving therapies. Most CGT products approved in the USA are approved in the EU and utilize data from international collaborative studies. Four CTPs were approved only in the USA, and their study sizes are ranged from 71 to 421. Chimeric antigen receptor (CAR)-T cell products for relapsed and refractory cancer have been approved in Japan, the USA and EU (Kymriah, Yescarta, Tecartus, Breyanzi, Abecma). Most CAR-T products had study sizes of around 100 while Breyanzi had relatively large size of more than 300 in the USA and EU.
In Japan, eight autologous cell products have been approved for eye, skin, and joint diseases, cell sheets for heart failure, and mesenchymal stem cells for neurological symptoms and functional disorders associated with spinal cord injury. In addition, the allogeneic cell product Temcell HS has been approved for use in GVHD treatment. All the main studies for these products ranged from 2 to 33 subjects in size and had no control arm.
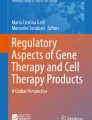
The distribution of the development and review times for each region is shown in Fig. 1a and b. We also checked whether changes occurred over time (Fig. 1c and d). The median development times (days) were 1885 in Japan, 2142 in the USA, and 1946 in the EU. Although the development time varied per product, the variation in Japan was smaller than that in the USA and EU. The development time for recently approved products seems to be short in the USA, although there are a few CTPs with exceptionally longer time.

Comparison of clinical development times and regulatory review times a Clinical development time in each region and b review time by each health authority are depicted. Plots of the development time c and review time d over the submission date of each product
Depending on the regulatory status of the product, the quality and quantity of the studies required to be submitted as evidence differed; the development time also differed accordingly (Table 4). For conditionally approved products, the study size and development times were smaller and shorter in the USA and EU compared to Japan. CGT products designated as innovative products generally had a small overall study size in the USA and short development time in the USA and EU. For orphan-designated products, the development time in the USA was short, but the development time in the EU and Japan was not necessarily shorter than that of non-orphan-designated products.
The median review time was 314, 334, and 481 days in Japan, the USA, and the EU, respectively. The review time in the USA was shorter and the variance was smaller without outliers, which may reflect differences in the time clock rules in that region. Regulators in Japan and the EU stop the time clock during review to allow applicants to take their time in responding to the questions and requests of the health authorities. The review times have been shortened in both Japan and the EU in recent years; however, the review time in the EU tends to be longer for conditional approvals.
Discussion
Our study showed that while the basic policies for the development and approval of CGT products in Japan, the USA, and Europe are generally consistent, there are some differences in specific regulatory definitions and provisions. Furthermore, the nature of CGT products launched in the three regions differ significantly. This study also found that companies marketing CGT products tended to enter their home markets and that the clinical evidence accepted by countries as the basis for approval varied considerably. These differences cannot be explained solely in terms of the regulations themselves or the regulatory processes required for new product development and marketing approvals. The differences observed seem to reflect the history and market characteristics of each region with respect to CGTs, including local medical needs, health insurance coverage, and the degree of maturity of the industry and academia in developing new products of this kind.
Types of Approved Products and Regulatory Environments
The number of approvals for all CGT products during the observation period was similar in the three regions; however, the types of products approved varied widely (Table 2).
Unlike in the USA and Europe, more CTPs were approved than GTPs in Japan. There are some Japan-specific regulations that worked to the advantage of cell product development and to the disadvantage of gene therapy products. An advantage of CTP development in Japan is the GCTP ordinance, which allows a verification approach as an alternative to traditional process validation (PV) [24]. This makes it possible to shorten the time required for chemistry, manufacturing and control (CMC) development especially in autologous CTPs. One Japanese regulatory procedure that may work against the development of gene therapy products compared to other regions is compliance with the Cartagena Act [21]. Although the operation in Cartgena Act was slightly improved in 2021, the relatively burdensome procedure may have led to delay in GTP development in Japan.
Clinical Trial Data Submitted for the Approval of Cell and Gene Therapy Products
It is difficult to determine whether the clinical evidence required for the approval of CGT products differed among the three regions because the requirements for approval vary widely across products. However, a comparison of the three regions regarding the clinical evidence for product groups with the same therapeutic objective may be possible. For example, CTPs for ocular and knee cartilage diseases were approved in multiple regions, although these products were developed by different companies. Holoclar (EU) and Nepic (Japan) are autologous corneal epithelial cell products with a similar indication for limbal stem cell deficiency. Studies for both products did not have a control group, but there was a large difference in sample size (106 (Holoclar) vs. 12 (Nepic)). Several autologous cell products have been approved for knee cartilage defects in the three regions: Spherox and ChondroCelect (EU), Maci (EU and US), and JACC (Japan). Except for JACC, a phase 3 study with a control group (microfracture) was conducted with sample sizes ranging from 102 to 144. JACC was approved based on a single-arm trial with only 33 subjects. Hence, it appears that the requirements for clinical evidence for the approval of CGT products in the three regions are different.
Home Markets are Prioritized for Product Launches
Companies that developed CGT products showed a strong tendency to enter their home markets (Online Resource 2). Historically, home market entry has been generally observed in pharmaceuticals [26,27,28]. Advantages based on domestic experience, relatively high costs of entry into foreign markets, and price setting in healthcare systems have been suggested as factors contributing to home market entry for traditional pharmaceuticals [26, 29]. Many developers of CGT products are relatively new and small or do not have extensive experience in commercial development. They often do not think about obtaining overseas approval in the early stages of their business. Hence, it seems natural that they tend to launch their products in their home countries first because they are familiar with their local regulations and can easily consult with their local authorities.
Pricing strategies may also lead to entry into home markets. Because manufacturing and maintenance costs are sometimes extraordinarily high and the targets are often rare diseases, prices and pricing flexibility are critical for companies marketing CGT products. When launching a product in one country, the prices in other markets are mostly referenced. Global companies are likely to choose the USA as their first market, where pricing is less constrained than other countries, and then file applications in the EU and Japan. This global strategy in pharmaceuticals has also been observed in a few CTPs and half of GTPs launched in the multiple regions. However, CGT products developed by small companies are often launched only in a particular country, so the context of global development is not valid.
Each region has its regulatory framework and supporting programs to accelerate access to new promising therapies (Table 1). Frameworks relevant to CGT product approval include the conditional and time-limited approvals in Japan and RMAT designations in the USA. Most CGT products in the USA have received special designation for innovative products (Table 2). In the EU, 12 products have been filed since the PRIME system was introduced in 2016, nine of which have been designated as PRIME. Among the applications after introducing conditional and time-limited approvals for CGT products in Japan, four have been designated as such. Companies receive preferential regulatory treatment during the approval review of CGT products. In addition, there is considerable support for product development, from subsidies and tax incentives to consultation services, but the results of these efforts have not been fully examined.
Conclusion
While regulations on CGT products are largely consistent among Japan, the USA, and the EU, some differences have a substantive impact on practices in the definition of CGT products (i.e., their status as pharmaceutical products), the timing of compliance with regulations for handling GMOs, and the validation process under GMP regulations. Although CGT products are given some preferential status in all regions, the preferential treatment given to CGT products varies across regions, reflecting the background differences in traditional pharmaceutical regulations. For CGT products historically launched in each region, the number, type, indications, developers, and submitted clinical evidence varied. A trend was observed for companies to enter their home markets, and this may have been driven by a different context than that of traditional pharmaceuticals, for which global development is more commonly observed.
References
Smith DM, Culme-Seymour EJ, Mason C. Evolving industry partnerships and investments in cell and gene therapies. Cell Stem Cell. 2018;22(5):623–6.
Moody J, Milligan WD, St Onge M, et al. Cell and gene therapy: a snapshot of investor perspectives. Cytotherapy. 2021;23(3):256–60.
Atilla E, Kilic P, Gurman G. Cellular therapies: day by day, all the way. Transfus Apher Sci. 2018;57(2):187–96.
Coppens DGM, de Wilde S, Guchelaar HJ, et al. A decade of marketing approval of gene and cell-based therapies in the United States, European Union and Japan: an evaluation of regulatory decision-making. Cytotherapy. 2018;20(6):769–78.
Ramezankhani R, Torabi S, Minaei N, et al. Two decades of global progress in authorized advanced therapy medicinal products: an emerging revolution in therapeutic strategies. Front Cell Dev Biol. 2020;8:547653.
Coppens DGM, De Bruin ML, Leufkens HGM, et al. Global regulatory differences for gene- and cell-based therapies: consequences and implications for patient access and therapeutic innovation. Clin Pharmacol Ther. 2018;103(1):120–7.
Kusakabe T. Regulatory perspectives of Japan. Biologicals. 2015;43(5):422–4.
Fujiwara Y, Maruyama Y, Honda F. Balancing safety and efficacy with early availability in the regulation of regenerative medicine product. Clin Pharmacol Ther. 2020. https://doi.org/10.1002/cpt.2034.
Gee AP. Regulation of regenerative medicine products. Adv Exp Med Biol. 2018;1098:189–98.
Bachtarzi H, Farries T. The genetically modified organism medicinal framework in Europe, United States, and Japan: underlying scientific principles and considerations toward the development of gene therapy and genetically modified cell-based products. Hum Gene Ther Clin Dev. 2019;30(3):114–28.
Cox EM, Edmund AV, Kratz E, et al. Regulatory affairs 101: introduction to expedited regulatory pathways. Clin Transl Sci. 2020;13(3):451–61.
Tanaka M, Idei M, Sakaguchi H, et al. Achievements and challenges of the Sakigake designation system in Japan. Br J Clin Pharmacol. 2021. https://doi.org/10.1111/bcp.14807.
Public Health Service Act, Section 351. 42 U.S.C. §262.
Federal Food, Drug, and Cosmetic Act. 21 U.S.C. § 321–399i.
Commission Directive 2009/120/EC of 14 September 2009 amending Directive 2001/83/EC of the European Parliament and of the Council on the Community code relating to medicinal products for human use as regards advanced therapy medicinal products (OJ L 242, 15.9.2009, p. 3–12).
The Act on Securing Quality, Efficacy, and Safety of Products, including Pharmaceuticals and Medical Devices. Act No. 145 of August 10, 1960, and its amendments.
FDA Guidance for Industry, Expedited Programs for Regenerative Medicine Therapies for Serious Conditions. 2019.
Trial Implementation of SAKIGAKE review designation. Notification No. 0401 (dated on 1 April 2015) issued by the Director of Evaluation and Licensing Division, Pharmaceutical Safety and Environmental Health Bureau, MHLW.
Handling of the Designation for Pioneering Medical devices, IVDs, Regenerative Medical Products, etc. Notification No. 6 (dated on 31 August 2020) issued by the Director of Medical Device Evaluation Division, Pharmaceutical Safety and Environmental Health Bureau, MHLW.
FDA Guidance For Industry, Determining the Need for and Content of Environmental Assessments for Gene Therapies, Vectored Vaccines, and Related Recombinant Viral or Microbial Products. 2015.
Act on the Conservation and Sustainable Use of Biological Diversity through Regulations on the Use of Living Modified Organisms. Act No. 97 of June 18, 2003, and its amendments.
Partial revision of "Revised procedures under Act on the Conservation and Sustainable Use of Biological Diversity through Regulations on the Use of Living Modified Organisms". Notification No. 5 (dated on 30 September 2021) issued by the Director-general of Pharmaceutical Safety and Environmental Health Bureau, MHLW. (To supplement “Questions and answers on administrative procedures, etc. for application for approval based on the law concerning the conservation of biodiversity through regulations on use of living modified organisms, etc. Administrative Notification issued by Pharmaceutical Evaluation Division and Medical Device Evaluation Division, Pharmaceutical Safety and Environmental Health Bureau, MHLW, dated on 3 February 2022.” is also referred.)
Concept of residual non-proliferative recombinant viruses used in the production of gene transduced cells. Administrative Notification issued by Evaluation and Licensing Division, Pharmaceutical Safety and Environmental Health Bureau, MHLW, dated on 10 December 2020.
Ministerial Ordinance on Standards for Manufacturing Control and Quality Control for Regenerative Medical Products. Ordinance of Ministry of Health, Labour and Welfare, No. 93, August 6, 2014.
Good Manufacturing Practice for Advanced Therapy Medicinal Products. EudraLex Volume 4 Part IV. 2017.
Kyle MK. The role of firm characteristics in pharmaceutical product launches. Rand J Econ. 2006;37(3):602–18.
Danzon PM, Wang YR, Wang L. The impact of price regulation on the launch delay of new drugs—evidence from twenty-five major markets in the 1990s. Health Econ. 2005;14(3):269–92.
Dranove D, Meltzer D. Do important drugs reach the market sooner. Rand J Econ. 1994;25(3):402–23.
Kyle MK. Pharmaceutical price controls and entry strategies. Rev Econ Stat. 2007;89(1):88–99.
FDA. What is Gene Therapy? https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products/what-gene-therapy. Accessed 25 July 2018.
Regulation (EC) No 1394/2007 of the European Parliament and of the Council of 13 November 2007 on advanced therapy medicinal products and amending Directive 2001/83/EC and Regulation (EC) No 726/2004.
Directive 2001/18/EC on the deliberate release into the environment of genetically modified organisms and repealing Council Directive 90/220/EEC.
Salmikangas P, Menezes-Ferreira M, Reischl I, et al. Manufacturing, characterization and control of cell-based medicinal products: challenging paradigms toward commercial use. Regen Med. 2015;10(1):65–78.
Handling of Priority Review. Notification No. 1 (dated on 31 August 2020) issued by the Directors of Pharmaceutical Evaluation Division and of Medical Device Evaluation Division, Pharmaceutical Safety and Environmental Health Bureau, MHLW.
FDA Guidance For Industry, Expedited Programs for Serious Conditions – Drugs and Biologics. 2014.
PMDA. Timeline for Standard Process of New Drug Review. https://www.pmda.go.jp/review-services/drug-reviews/about-reviews/p-drugs/0014.html. Accessed 14 Nov 2021.
MHLW. SAKIGAKE Package Strategy – Promotion of Commercializing Innovative Medicines 2014. https://www.mhlw.go.jp/seisakunitsuite/bunya/kenkou_iryou/iyakuhin/topics/tp140729-01.html. Accessed 26 Jan 2021
Funding
This study was funded by a Japanese government-based grant-in-aid from the Ministry of Education, Culture, Sports, Science and Technology, Tokyo, Japan (KAKEN-HI: 19K07215).
Author information
Authors and Affiliations
Contributions
YS and SO wrote the manuscript; YS and SO designed the research; YS analyzed the data.
Corresponding author
Ethics declarations
Conflict of interest
YS is an employee of Novartis Pharma K.K. The other author declared no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sato, Y., Ono, S. Regulatory Environment and Approvals in Cell and Gene Therapy Products Between Japan, the USA, and the EU. Ther Innov Regul Sci 57, 227–237 (2023). https://doi.org/10.1007/s43441-022-00455-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43441-022-00455-4