
Abstract
Purpose
This study aimed to determine (1) does vertebral body tethering (VBT) produce differential growth modulation in individual vertebrae in patients with idiopathic scoliosis, (2) does VBT change disc shape, and (3) does VBT affect total spine length?
Methods
Patients with idiopathic scoliosis treated with VBT of the main thoracic curve and minimum 2-year follow-up were included. Vertebrae and discs were categorized as uninstrumented proximal thoracic, instrumented main thoracic, or uninstrumented thoracolumbar–lumbar. The left- and right-sided heights of each vertebra and disc were measured on subsequent radiographs to assess for differential growth. T1–T12 thoracic and T1–S1 thoracolumbar growth velocities were compared with standardized reference data.
Results
Fifty-one patients (764 vertebrae and 807 discs) were analyzed. The average major curve magnitude improved from 46° ± 11° to 17° ± 11° at 2-year follow-up. Differential growth was observed in MT vertebrae, in which the left/concave side grew 2.0 ± 2.2 mm compared with 1.5 ± 2.3 mm on the right/convex (tethered) side (p < 0.001). Differential height changes were observed for all discs, but were most pronounced in instrumented MT discs, in which the right/convex sides decreased by an average of 1.2 mm each, compared with no significant height change on the left/concave side. Total spinal growth velocities were not significantly different from standard reference data.
Conclusion
Vertebral body tethering limits convex spinal growth as designed while permitting concave growth. Curve correction results from differential vertebral growth and decreased convex disc height. Overall spinal growth continues at the expected rate.
Level of evidence
Level IV case series.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vertebral body tethering (VBT) as a treatment option for idiopathic scoliosis has gained popularity over the past decade. Vertebral body tethering offers the potential to harness remaining spinal growth, via the Hueter–Volkman principle, to correct scoliosis without fusion of the spinal column. Animal studies [1,2,3] and a case study [4] show proof of this concept. Clinical studies focus on early and mid-term outcomes, curve correction, and complication rates for patients treated with VBT [5,6,7,8,9,10,11,12,13,14]. These studies demonstrate that curve correction can occur; however, the effects of VBT on longitudinal growth of the spine, disc height changes, and whether differential growth of individual vertebrae occurs have not been reported. It is unclear whether the curve magnitude improvement in successful VBT cases occurs through differential vertebral growth, changes in convex- and/or concave-sided disc height, or both. In this study, we sought to answer the following research questions using multi-center retrospective data collected from patients with minimum 2-year follow-up: (1) does VBT produce differential growth modulation in individual vertebrae, (2) does VBT change disc shape, and (3) does VBT affect total spine length?
Methods
Patients with idiopathic scoliosis treated with thoracic VBT between April 2014 and October 2018 with minimum 2-year follow-up were identified from a retrospective multi-center database. This retrospective chart review study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Human Investigation Committee (IRB) of our institution approved this study. Demographic data included sex and age at surgery. Radiographs from preoperative and postoperative visits (first erect, 1 year, and 2 years) were reviewed. The first erect visits were typically 4–6 weeks postoperatively. The Sanders stage [15] was noted preoperatively.
The major curve magnitude of the instrumented curve was measured preoperatively and at the 2-year postoperative visit. We only included Lenke 1 patients whose main thoracic curves (defined as those with a thoracic apical vertebra or disc) were tethered, and excluded those who underwent tethering of a lumbar curve (apical vertebra or disc in the lumbar spine). To accurately assess the effect of VBT on growing thoracic vertebrae, patients with treatment failure (defined as final 2-year curve magnitude greater than 35°), tether breakage (defined as a greater than 5° increase in the angulation between an adjacent pair of screws on successive radiographs) [9], tethered curves other than a main thoracic curve (defined as those with a thoracic apical vertebra or disc), or preoperative Sanders score greater than 4 were excluded due to limited growth potential in the spine after this stage.
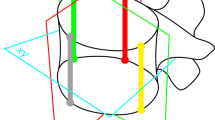
The upper instrumented vertebra and lower instrumented vertebra for each patient were noted. Individual vertebrae and discs were classified by location as follows: instrumented main thoracic (MT), uninstrumented proximal thoracic (PT), and uninstrumented thoracolumbar–lumbar (ThL–L). The upper instrumented vertebra and lower instrumented vertebra of each patient were excluded from analysis. We believed these vertebrae would behave variably between an instrumented and an uninstrumented vertebra, because only one of the two growth plates of the vertebra were subject to the tether’s compressive forces. On pre- and postoperative radiographs, the individual right- and left-sided heights of each vertebra and disc were measured (Fig. 1), as well as the linear height of the thoracic spine and entire thoracolumbar spine. The right- and left-sided vertebral height measurements were made on the right and left aspect of each vertebral body, between a line that traces the upper endplate and a line that traces the lower endplate. Disc height measurements were made in a similar fashion on the right and left lateral edges of the disc. For conceptual consistency, in the few patients with left thoracic curves, left-sided measurements were recorded as right and vice versa. Thoracic linear height was measured as a straight line from the midpoint of the superior endplate of T1 to the midpoint of the inferior endplate of T12. The thoracolumbar linear height was measured as a straight line from the midpoint of the superior endplate of T1 to the midpoint of the superior endplate of S1. Measurements were performed by four trained observers and verified for accuracy by the first author.

Representative example of methodology for measuring a left and right intervertebral disc heights, and b left and right vertebral heights
To determine if a change of individual segment shape occurred, the mean right- and left-sided height of each vertebra and disc within a given region of the spine (i.e., PT, MT, ThL–L) were compared between the various timepoints. To account for vertebral growth between the time that preoperative radiographs were taken before surgery, first erect, 1-year, and 2-year follow-up radiographs were compared to analyze vertebral growth. In this way, only growth under the influence of the tether forces was considered. For discs, based on the assumption that disc growth is no longer occurring [16] and height changes were due to the distribution of disc volume based on mechanical loads, preoperative and 2-year follow-up radiographs were compared. In this way, the change in right- and left-sided disc heights in response to the forces enacted by the tether could be calculated. Then, to determine if differential growth occurred, for each vertebral and disc category, the mean change in height on the left side was compared with the mean change in height on the right to see if there were significant differences in side-to-side height change. This analysis was also performed for instrumented vertebrae in patients split by Sanders stage to observe differential growth based on preoperative skeletal maturity.
To determine whether VBT affects total spine growth, growth velocities over the 2-year study were calculated for both the thoracic spine and the thoracolumbar spine using T1–T12 heights and T1–S1 heights, respectively, and compared with expected values. Expected growth velocities were calculated for each patient using Dimeglio’s standardized growth curve charts based on age and sex [17].
Statistical analysis was performed using IBM SPSS Statistics, version 27 (Armonk, NY). Paired sample t tests were used to compare vertebrae and disc heights, as well as the comparison between measured spine heights and expected spine heights. Significance was set at an α level of 0.01.
Results
Seventy-five patients were identified from our records as having been treated with VBT. Twenty-four were excluded (five for missing Sanders stage data, five for Sanders stage of 5 or greater, 10 for treatment failure, and four for curves other than a main thoracic curve tethered), leaving 51 patients who met the inclusion criteria (41 female, 10 male). The mean age at the time of surgery was 12.3 years (range, 10–15 years). Preoperatively, nine patients (18%) were Sanders 2, 26 (51%) were Sanders 3, and 16 (31%) were Sanders 4. The average major curve magnitude was 46° ± 11° preoperatively, which decreased to 17° ± 11° at 2-year follow-up. Overall, 764 vertebrae and 807 intervertebral discs were included in the analysis. There were 234 uninstrumented PT, 279 instrumented MT, and 251 uninstrumented ThL–L vertebrae. There were 226 uninstrumented PT, 326 instrumented MT, and 255 uninstrumented ThL–L discs.
Left- and right-sided growth/height change of individual segments
The mean heights of vertebrae from all three regions of the spine increased significantly on both the left and right sides when comparing 2-year follow-up radiographs with first erect, indicating that vertebral body growth occurred during the study period, even in the tethered MT vertebrae (Table 1). For discs, significant decreases in height during the study were observed on the convex side of each curve, i.e., left PT curve discs, right MT curve discs, and left ThL–L discs (Table 2). No significant concave-sided disc height changes were observed.
Differential growth of individual segments.
For vertebrae, differential growth was only observed in instrumented main thoracic vertebrae with the left (concave) side growing on average 0.5 mm more than the right (convex) tethered side over the 2-year study interval (2.0 ± 2.2 mm compared with 1.5 ± 2.3 mm, respectively) (Fig. 2). Figure 3 shows the differential growth of instrumented MT vertebrae split by preoperative Sanders stage. In all subgroups, growth on the left (concave) side was greater than that on the right (convex) side. Only differential growth for vertebrae in the Sanders 3 patients met statistical significance.

Mean vertebral growth over the 2-year study period for each vertebra category. The difference between left- and right-sided growth was only significant in MT vertebrae. *Reached statistical significance, MT main thoracic, NS not significant, PT proximal thoracic, ThL–L thoracolumbar–lumbar

Instrumented main thoracic vertebral growth split by preoperative Sanders stage. NS not significant
For discs, differential height changes were observed in all regions. The most significant differential change was observed in instrumented MT discs, in which the right (convex) side of the discs was decreased by an average of 1.2 mm each, compared with no significant height change on the left (concave) side (Fig. 4).

Mean intervertebral disc height changes for each disc category. Significant differences were seen when comparing the left- and right-sided height changes for each disc type over the 2-year study period. *Reached statistical significance, MT main thoracic, PT proximal thoracic, ThL–L thoracolumbar–lumbar
Regional and total spinal growth
Calculated and expected growth velocities for the thoracic spine and whole thoracolumbar spine are listed in Table 3. No significant differences were noted for calculated compared with expected growth velocities, indicating that overall spinal growth in those treated with VBT is not significantly different from that of normal (non-scoliotic) age- and sex-matched controls.
Discussion
Vertebral body tethering is a relatively new treatment option that theoretically harnesses remaining spine growth in skeletally immature scoliosis patients by differential growth modulation via the Hueter–Volkmann principle. Multiple case series [5,6,7,8,9,10,11,12,13,14] have demonstrated the ability of VBT to improve curve magnitude, but to our knowledge no study to date has specifically assessed whether differential growth is occurring clinically within individual vertebra as demonstrated in animal models. In the present series, we demonstrated a statistically significant difference between left and right vertebral height changes in tethered vertebrae, indicating that differential growth modulation does occur with concave outpacing convex growth by a factor of roughly 1.3 during the study period (Fig. 2).
We found that growth along the right (convex) side of the instrumented vertebrae still occurs, as the mean right-sided MT vertebral height was found to be statistically greater on 2-year follow-up radiographs compared with first erect radiographs (Table 1). Thus, although differential growth occurs in instrumented vertebrae, growth is not completely arrested on the tethered side. When the data are split by Sanders stage (Fig. 3), the overall growth appears to inversely correlate with Sanders stage, given that less growth remains with increasing skeletal maturity. Although mean left-sided vertebral body growth was greater than that of right-sided growth for Sanders 2 and Sanders 4 patients, these differences did not reach statistical significance in this study. This is likely because of a loss of power due to low numbers—there were only nine patients at Sanders 2 and 16 patients at Sanders 4.
Discs in all three regions of the spine exhibited differential changes in height due to significant decreases on the convex side of each disc (Table 2, Fig. 4). In the uninstrumented PT and ThL–L curves, disc height decreased on the left, convex side and was statistically unchanged on the right, concave side. In the instrumented MT curve, disc height decreased on the right, convex side by a greater magnitude than the decreases seen in the convex sides of the uninstrumented PT and ThL–L curves. The left, concave-side height of MT discs remained statistically unchanged. Disc growth is essentially completed prior to age 10 years [16], and given their viscoelastic properties, changes in height are expected to be secondary to mechanical forces across the disc and volumetric shifts. Our data support the predictable behavior of the intervertebral discs in response to changes in force distribution and vertebral body shape within the instrumented MT segment of the spine. During surgery, the tether compresses the discs on the convex side as the cord is tensioned, and the initial correction of the curve seen immediately postoperatively occurs through the changes in the shape of the discs within the MT curve. Because the PT and ThL–L curves are minor, compensatory curves, the spine maintains balance in these uninstrumented segments by invoking changes in the uninstrumented discs. From differential vertebral growth in the instrumented vertebrae and disc shape changes, the mean major curve magnitude in the present cohort improved from 46° to 17°.
Finally, to assess whether or not VBT affects total overall spinal growth, growth velocities were calculated from our data and compared with those of age- and sex-matched controls from Dimeglio’s standardized data set of normal adolescent spine growth (Table 3) [17]. We found that neither the total thoracic spine nor the total thoracolumbar spine growth was significantly influenced by the tether compared with expected growth velocities.
There are several limitations of this study. First, only patients with tethered thoracic curves were included. Thus, it is possible that the findings reported herein are not generalizable to patients with tethered lumbar curves or with two tethered curves. Second, since we excluded patients with “treatment failure” and those with tether breakages, the behavior of the individual vertebra and discs in such patients is unknown. We opted to exclude these patients to avoid introducing inconsistencies in the data set. We aimed to keep the scope of this investigation concise—that is, when VBT is successful, what is happening at the individual vertebral and disc level? Third, because of the rotational differences in vertebrae in the scoliotic spine and the normal sagittal regional differences in the thoracic and lumbar spine, different individual vertebra are oriented in different planes relative to the plane of a two-dimensional radiograph. Thus, linear measurements on vertebrae that are more out of plane may be inherently more variable, increasing measurement error and decreasing precision. This is especially true with measuring L5, which tends to be tipped fairly caudad as most lumbar lordosis occurs at the L5–S1 segment [18]. This inherent variability could potentially be reduced using three-dimensional data to perform linear measurements on individual vertebrae, with the ability to differentially orient each vertebra to the desired plane of measurement. Future analysis using three-dimensional data may decrease this error and provide more precise measurements. Fourth, the fact that the standard deviation is relatively high compared with the mean values is likely because of multiple different vertebrae included in the means, which are inherently different sizes. Fifth, there was no control group of patients with normal or untreated scoliotic spines for direct comparisons. This is an especially salient limitation when evaluating whether VBT affects total spine growth. Future investigations should aim to answer this question with a well-defined control group; however, with the present study design, historic controls were the best available comparison. Finally, while this study’s endpoint was at the 2-year follow-up visit, some additional spinal growth may be seen past the 2-year postoperative mark, especially in the more skeletally immature patients at the time of surgery.
In conclusion, when successful, VBT produces differential growth modulation in the instrumented vertebrae (growth maintenance on the concavity and relatively slower growth on the convexity). Intervertebral disc shape also changes with VBT, with decreases observed on the convex sides of discs. These changes are most pronounced in the main thoracic discs within the tether construct. Finally, it does not appear that VBT has an adverse effect on total spine length, as thoracic and thoracolumbar spinal growth velocities noted in the present study were not significantly different from expected values for normal age- and sex-matched controls [17]. Findings from this study may form the basis for predictive modeling and future VBT strategies in skeletally immature scoliosis patients so that we may be able to more accurately select who to tether and when, to optimize patient outcomes.
Availability of data and materials
Data are available upon reasonable request.
Code availability
Not applicable.
References
Braun JT, Ogilvie JW, Akyuz E et al (2006) Creation of an experimental idiopathic-type scoliosis in an immature goat model using a flexible posterior asymmetric tether. Spine 31:1410–1414. https://doi.org/10.1097/01.brs.0000219869.01599.6b
Newton PO, Fricka KB, Lee SS et al (2002) Asymmetrical flexible tethering of spine growth in an immature bovine model. Spine 27:689–693. https://doi.org/10.1097/00007632-200204010-00004
Newton PO, Farnsworth CL, Faro FD et al (2008) Spinal growth modulation with an anterolateral flexible tether in an immature bovine model: disc health and motion preservation. Spine 33:724–733. https://doi.org/10.1097/BRS.0b013e31816950a0
Crawford CH 3rd, Lenke LG (2010) Growth modulation by means of anterior tethering resulting in progressive correction of juvenile idiopathic scoliosis: a case report. J Bone Jt Surg Am 92:202–209. https://doi.org/10.2106/JBJS.H.01728
Baker CE, Kiebzak GM, Neal KM (2021) Anterior vertebral body tethering shows mixed results at 2-year follow-up. Spine Deform 9:481–489. https://doi.org/10.1007/s43390-020-00226-x
Ergene G (2019) Early-term postoperative thoracic outcomes of videothoracoscopic vertebral body tethering surgery. Turk Gogus Kalp Damar Cerrahisi Derg 27:526–531. https://doi.org/10.5606/tgkdc.dergisi.2019.17889
Hoernschemeyer DG, Boeyer ME, Robertson ME et al (2020) Anterior vertebral body tethering for adolescent scoliosis with growth remaining: a retrospective review of 2 to 5-year postoperative results. J Bone Jt Surg Am 102:1169–1176. https://doi.org/10.2106/JBJS.19.00980
Miyanji F, Pawelek J, Nasto LA et al (2020) Safety and efficacy of anterior vertebral body tethering in the treatment of idiopathic scoliosis. Bone Jt J 102-B:1703–1708. https://doi.org/10.1302/0301-620X.102B12.BJJ-2020-0426.R1
Newton PO, Kluck DG, Saito W et al (2018) Anterior spinal growth tethering for skeletally immature patients with scoliosis: a retrospective look two to four years postoperatively. J Bone Jt Surg Am 100:1691–1697. https://doi.org/10.2106/JBJS.18.00287
Newton PO, Bartley CE, Bastrom TP et al (2020) Anterior spinal growth modulation in skeletally immature patients with idiopathic scoliosis: a comparison with posterior spinal fusion at 2 to 5 years postoperatively. J Bone Jt Surg Am 102:769–777. https://doi.org/10.2106/JBJS.19.01176
Pehlivanoglu T, Oltulu I, Ofluoglu E et al (2020) Thoracoscopic vertebral body tethering for adolescent idiopathic scoliosis: a minimum of 2 years’ results of 21 patients. J Pediatr Orthop 40:575–580. https://doi.org/10.1097/BPO.0000000000001590
Samdani AF, Ames RJ, Kimball JS et al (2014) Anterior vertebral body tethering for idiopathic scoliosis: two-year results. Spine 39:1688–1693. https://doi.org/10.1097/BRS.0000000000000472
Samdani AF, Ames RJ, Kimball JS et al (2015) Anterior vertebral body tethering for immature adolescent idiopathic scoliosis: one-year results on the first 32 patients. Eur Spine J 24:1533–1539. https://doi.org/10.1007/s00586-014-3706-z
Wong HK, Ruiz JNM, Newton PO et al (2019) Non-fusion surgical correction of thoracic idiopathic scoliosis using a novel, braided vertebral body tethering device: minimum follow-up of 4 years. JBJS Open Access 4:e0026. https://doi.org/10.2106/JBJS.OA.19.00026
Sanders JO, Khoury JG, Kishan S et al (2008) Predicting scoliosis progression from skeletal maturity: a simplified classification during adolescence. J Bone Jt Surg Am 90:540–553. https://doi.org/10.2106/JBJS.G.00004
Stokes IA, Windisch L (2006) Vertebral height growth predominates over intervertebral disc height growth in adolescents with scoliosis. Spine 31:1600–1604. https://doi.org/10.1097/01.brs.0000222008.15750.1f
Dimeglio A, Canavese F, Bonnel F (2016) Normal growth of the spine and thorax. In: Akbarnia BA, Yazici M, Thompson GH (eds) The growing spine: management of spinal disorders in young children, 2nd edn. Springer, Heidelberg, pp 47–82
Bernhardt M, Bridwell KH (1989) Segmental analysis of the sagittal plane alignment of the normal thoracic and lumbar spines and thoracolumbar junction. Spine 14:717–721. https://doi.org/10.1097/00007632-198907000-00012
Acknowledgements
The authors would like to thank Stefan Parent (Sainte-Justine University Hospital, Montreal, QC and Department of Surgery, Université de Montréal, Montréal, QC) and Firoz Miyanji (BC Children’s Hospital, Vancouver, BC) for their valuable insight and assistance with the design and analysis of our data for this study.
Funding
The authors received study support from Setting Scoliosis Straight Foundation for the submitted work.
Author information
Authors and Affiliations
Consortia
Contributions
1a. Conception or design of the work OR: TCM, SAS, MEB, KN, BSL, ANL, BY, PON, DGH. 1b. Acquisition, analysis, or interpretation of data for the work OR: TCM, JBH, JV, MEB, MP, ANL, PON, DGH, Harms. 1c. Creation of new software used in the work: none. 2a. Drafting the work OR: TCM. 2b. Revising the work critically for important intellectual content: TCM, SAS, JBH, JV, MEB, MP, KN, BSL, ANL, BY, PON, DGH, Harms. 3. Final approval of the version to be published: TCM, SAS, JBH, JV, MEB, MP, KN, BSL, ANL, BY, PON, DGH, Harms. 4. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: TCM, SAS, JBH, JV, MEB, MP, KN, BSL, ANL, BY, PON, DGH, Harms.
Corresponding author
Ethics declarations
Conflict of interest
Authors TCM, JBH, JV, MEB, and MP have no relevant financial or non-financial interests to disclose. Author SAS reports grants from the Setting Scoliosis Straight Foundation, during the conduct of the study and personal fees from DePuy Synthes Spine, outside the submitted work. Author KN reports personal fees from OrthoPediatrics, outside the submitted work. Author BSL reports grants from Grant from DePuy Synthes to Setting Scoliosis Straight Foundation in Support of Harms Study Group, personal fees and non-financial support from Depuy Synthes, personal fees from Zimmer Biomet, personal fees and non-financial support from ApiFix, other from Spine Search, other from Paradigm Spine, other from SRS Spine Deformity Journal, outside the submitted work. Author ANL reports other from Depuy, Globus, Orthopediatrics, Medtronic, outside the submitted work. Author BY reports grants from Setting Scoliosis Straight, during the conduct of the study and grants and personal fees from Stryker, grants and personal fees from Depuy Synthes, personal fees from Nuvasive, personal fees from Medtronic, personal fees from Biogen, personal fees from Orthopediatrics, personal fees from Globus, outside the submitted work. Author PON reports grants from Setting Scoliosis Straight Foundation, during the conduct of the study; grants and other from Setting Scoliosis Straight Foundation, other from Rady Children's Specialists of San Diego; grants, personal fees and non-financial support from DePuy Synthes Spine; grants and other from Scoliosis Research Society; grants from EOS imaging; personal fees from Thieme Publishing, grants from NuVasive; other from Electrocore; other from International Pediatric Orthopedic Think Tank; grants, non-financial support and other from Orthopediatrics; grants, personal fees, and non-financial support from Stryker K2M; grants and non-financial support from Alphatech; grants from Mazor Robotics; personal fees from Pacira; personal fees from Globus Medical; personal fees from Medtronic, outside the submitted work. In addition, Dr. Newton has a patent “Anchoring Systems and Methods for Correcting Spinal Deformities” (8540754) with royalties paid to DePuy Synthes Spine, a patent “Low Profile Spinal Tethering Systems” (8123749) licensed to DePuy Spine, Inc., a patent “Posterior Spinal Fixation” licensed to Stryker/K2M, and a patent “Posterior Cervical Fixation” with royalties paid to Stryker/K2M. Author DGH has a patent regarding tethering pending. Author HNFSG reports grants from Setting Scoliosis Straight Foundation, during the conduct of the study: SSSF receives funding from DePuy Synthes Spine, EOS imaging, K2M, Medtronic, NuVasive, Zimmer Biomet and the FDA in support of Harms Non-Fusion Study Group research; grants and other from Setting Scoliosis Straight Foundation: SSSF received educational grants from Orthopediatrics, Mazor Robotics, Stryker, Ellipse, Globus & SpineGuard, to support Setting Scoliosis Straight educational activities.
Ethical approval
Approval was obtained from the Nemours Institutional Review Board. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
McDonald, T.C., Shah, S.A., Hargiss, J.B. et al. When successful, anterior vertebral body tethering (VBT) induces differential segmental growth of vertebrae: an in vivo study of 51 patients and 764 vertebrae. Spine Deform 10, 791–797 (2022). https://doi.org/10.1007/s43390-022-00471-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43390-022-00471-2