
Abstract
Purpose
The interaction between sleep and recovery is a fundamental issue for ultra-marathoners, especially after an ultra-trail, but literatures on this matter remains are scarce. The main objectives were (1) to describe sleep parameters during the nights following an ultra-endurance event in amateur trail runners, (2) to evaluate the recovery kinetics, and (3) to assess the relationship between sleep parameters and recovery.
Methods
Nineteen race finishers were tested daily, from 10 days before to 10 days after the Ultra-Trail du Mont-Blanc® (UTMB®). Hooper Index (HI) was used to assess recovery and sleep parameters (total sleep time, TST and wake after sleep onset, WASO) were monitored using a wrist-worn actigraph.
Results
HI was higher than baseline until day 5 after the race (P < 0.05) and younger athletes had a lower HI than older ones during the recovery period (P < 0.001). TST was not modified by the race, but there was a WASO peak on the second night after. Positive correlations were found between WASO and muscle soreness (P < 0.001) and between TST and HI (P < 0.05).
Conclusions
In conclusion, participants needed 6 days for recovery after UTMB® and younger runners seemed to recover faster than older ones. Post-race sleep quantity did not increase, but the second night was more fragmented, most likely due to muscle soreness. Correlations between sleep and recovery parameters highlighted the key role of sleep for recovery.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Ultramarathons have been growing more and more popular among runners for the past 10 years. The term ultramarathon refers to a running race longer than 42.195 km, on any type of ground surface [26]. More precisely, the International Trail Running Association defines ultra-trail running as a pedestrian competition held in a natural environment, longer than 80 km; nevertheless, the 100-mile-long races are the most coveted events, with or without elevation. The Ultra Trail du Mont-Blanc® (UTMB®, 170 km, 10,000 m elevation, time limit 46 h 30 min) is considered to be one of the world hardest mountain ultra-marathons (MUM).
The physiological effects of running are well documented for distance below 42 km [7, 12], but remain to be fully explored in MUM, due to the logistical issues involved in monitoring runners in remote ecological conditions. However, recent studies have significantly increased the knowledge about the impact of these ultra-endurance races on sleep deprivation [15, 16, 23], muscular and cardiorespiratory adaptations [24, 29] and physiological/psychological recovery [20, 21] in amateur and elite athletes. As recovery may be defined as an intra- and inter-individual multilevel (e.g., psychological, physiological and social) process for the restoration of performance abilities [18], a few papers highlighted 5–14 days as being necessary for recovery after an ultra-marathon, depending on the biological and physiological considered markers. Indeed, a 5-day rest is necessary for returning to basal subjective values of fatigue and muscle soreness after a 100-miles MUM (elevation 5500 m) [13]. After UTMB®, 9 days were needed for participants to recover maximum voluntary strength and to return to basal values of muscle integrity and inflammation; in the same manner, myoglobin concentration increased during race returned to normal values 5 days after [20, 21]. After a similar 24-h event, trail runners required 2 weeks post-race to return levels of perceived stress and recovery levels back to initial values [22]. Finally, heart rate variability, another marker for fatigue status, also remained lower for 2 weeks after the event, with a predominance of sympathetic activity [20, 21].
Hence, these studies show that, after a MUM, a long period of recovery is needed for a wide range of physiological and psychological functions to return to pre-race levels. In ultra-trail, participants must recover from a grueling physical effort, but also from a significant sleep deprivation. Unlike team sports in which players play a series of matches, quick physical recovery for an ultra-amateur trailer may not be the priority. However, a quick recovery of cognitive functions seems necessary for safety and health, for example to avoid road accidents, domestic or professional issues. In this matter, it takes several days and nights of recovery to get basal cognitive abilities back after sleep deprivation [3, 27]. However, to our knowledge, no study has described sleep parameters during this post-race period and its potential subsequent interactions with the recovery process. Two mechanisms might come into play. On one hand, the physiological strain of such a long race may have a negative impact on sleep quantity and quality during the nights post-race and an acute intensive period of exercise may produce concomitant fatigue and muscle soreness, inducing sleep disorders during recovery [17]. On the other hand, it is well established that a “sleep rebound” follows a period of sleep deprivation [1, 2], that is, an increase in sleep quantity during the nights following sleep deprivation. Considering the key role of sleep on sport recovery [10], a rise or a decrease in sleep quantity after an ultra-trail may influence recovery kinetics.
Hence, in this study, the main objectives were (1) to describe sleep parameters during the nights following an ultra-endurance event in amateur trail runners, (2) to evaluate the recovery kinetics and (3) to assess the relationship between sleep parameters and recovery. The hypotheses were, in amateur athletes, sleep quantity would be augmented (“sleep rebound”) after a 170 km MUM (elevation 10,000 m) and sleep would have an effect on recovery kinetics.
Methods
Experimental Design
This study took place during the 2019 UTMB®. The start was at 6:00 PM on August 30th in Chamonix, France and included cutoff time limits at 16 check points around the course (for nutrition and rest). Runners had 46.5 h to complete the race. Sleep monitoring started 10 days before the race using actigraph.
The study was approved by the UTMB® medical committee and by local ethics committee (no°2018220323) and all participants gave written informed consent in accordance with the Declaration of Helsinki [30].
Participants
Forty-four healthy male participants (age 43.1 ± 6.2 years old), all of whom had qualified for this event according to UTMB® regulations [28], volunteered for this study. Inclusion criteria for participant included being resident or domiciled around the Greenwich Meridian, ± 2 h and not taking medication which could impact sleep and cognitive function.
Of the 44 trail runners, 29 completed the race within the time limit and 19 were selected for further data analyses (age 44.2 ± 7.0 years old, height 176 ± 6 cm, weight 78 ± 6 kg, fat mass percentage 13% ± 2%, body mass index 25.2 ± 3.2 kg/m), as data were missing or lost for the ten remaining runners. These 19 athletes finished the race in 43.2 ± 1.8 h, with age group categories as follows: age 23–39 years: senior (S) (n = 6), age 40–49 years: veteran 1 (V1) (n = 8) and age 50–59 years: veteran 2 (V2) (n = 5).
Sleep Parameters (Quality and Quantity)
Participants were asked to wear, for 3 weeks (10 days pre-race, 10 days post-race and during race itself), a tri-axel accelerometer (wGT3X-BT, Actigraph, Pensacola, Florida) on the wrist of their non-dominant hand, to continuously monitor the sleep–wake cycle. The data were retrieved and analysed with Actilife 6.0 software, using Cole–Kripke algorithm [5]: total sleep time, as the duration from sleep onset to wake-up time (TST, min), wake after sleep onset, as the duration of awake time between bedtime and wake-up time (WASO, min), number of awaking as the number of awakenings longer than one minute (NOA) and sleep fragmentation index as the percentage of time spent moving during sleep, which is an indicator of night-time restlessness (SFI, %). Participants were also asked to complete a daily sleep–wake log, in which they would report wake-up time, bedtime, nap time and period when they did not wear the captor (shower, safety issue).
During the race, at seven check points (29 km, 49 km, 77 km, 101 km, 131 km, 160 km and finish line), participants were asked if they had slept at any point between the start line and the checkpoint, where the nap occurred and how long it was.
Physical and Psychological State: Hooper Index
Hooper index (HI) is a self-reported rating of well-being and provides an efficient assessment of monitoring recovery [14].
Participants were asked to complete the HI twice before race day (7 and 1 day before) and every day after the race, for 10 days, between 6:00 and 8:00 PM. It is the sum of four subtest indexes about sleep quality, stress amount, fatigue and muscle soreness. Each subtest consists of a scale from 1 (“very, very low” or “good”) to 7 (“very, very high” or “bad”). The Hooper Index score ranges from 4 to 28, 4 referring to optimal well being.
Statistical Analysis
Basal values of TST, WASO and HI were defined as their respective pre-race values.
Normality and variance homogeneity of data were verified by Shapiro–Wilk and a Levene tests, respectively.
Multiple analyses of variance (ANOVA) and post hoc tests were then conducted to evaluate the effect of race on TST, WASO, HI and HI subitems (pre-race vs. post-race) and also to evaluate the evolution of each dependant variable during post-race period.
Additional ANOVAs were performed to evaluate the effect of age on each dependent variable. Finally, Pearson’s correlation analyses were performed to establish potential relationship between HI (and its subtests coefficients), sleep parameters pre-, per- and post-race (TST, WASO) and race performance.
The effect size was assessed for age group tests via η2 for ANOVA and Cohen’s d for t test. Statistical analyses were performed using R Studio 1.3.1093 (RStudio, Inc., Boston, USA), and statistical significance was set at P < 0.05.
Results
Race values (mean ± SD) of sleep and race performance by age group are presented in Table 1.
There was no effect of age group on race time and no effect of sleep quantity during race on race time.
Hooper Index (Figs. 1 and 2)

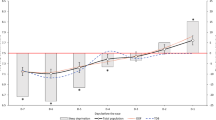
A (left). Values (mean ± SD) of daily Hooper Index after the race, for 10 days. B (right). Values of daily Hooper Index subitems after the race, for 10 days (sleep, black circles; fatigue, black triangles; soreness, black squares; stress, black rhombus). SD bars were removed for a better clarity. *P < 0.05 (vs. pre-race)
Post-race HI values were higher than pre-race (P < 0.001), until day 5 (P < 0.05) (Fig. 1A).
More precisely, the post-race values of fatigue subitem was higher until day 6 (P < 0.001) and soreness until day 4 (P < 0.001) than pre-race values (Fig. 1B).
There was an age effect on total HI score (P < 0.001; η2 = 0.076) and on each subitem during post-race HI (sleep, P < 0.05, η2 = 0.037; stress, P < 0.001, η2 = 0.114; fatigue, P < 0.05, η2 = 0.055; soreness, P < 0.001, η2 = 0.129). Senior group had a lower HI than V1 group at days 3 and 4 (P < 0.05, d = 0.67 and d = 0.55, respectively) and than the V2 group at days 6 and 7 (P < 0.05, d = 0.82 and d = 0.73, respectively) (Fig. 2). Soreness scores in the senior group were lower than V1 group for day 2 (P = 0.017, d = 0.55), day 3 (P = 0.026, d = 0.67) and day 4 (P = 0.049, d = 0.84). This subitem score was also lower for the senior group as compared to V2 group from day 3 (P = 0.048, d = 0.67) to day 10 (P = 0.004, d = 0.53).

Values of daily Hooper Index after the race, for 10 days, by age group (Senior, S, black circles; Veteran 1, V1, black triangles; Veteran 2, V2, black squares). SD bars were removed for a better clarity. *P < 0.05 (vs. V1 group at the same day). $P < 0.05 (vs. V2 group at the same day)
No difference was found between V1 and V2 groups.
Sleep Parameters (Fig. 3)

Values of total sleep time (TST, black triangles) and wake after sleep onset (WASO, black circles) during the 10 nights prior to and following UTMB. *P < 0.05 (vs. nights 8, 9 and 10)
There was no race effect on sleep parameters (TST, WASO, NOA and SFI).
During post-race analysis, there was a day effect on WASO (P < 0.01). More precisely, WASO on night 2 was higher than on night 8 (P < 0.05), night 9 (P < 0.05) and night 10 (P < 0.001) (Fig. 3).
Positive correlations were found between WASO and muscle soreness (r = 0.324, P < 0.001) and between WASO and HI (r = 0.195, P < 0.05). There were also negative correlations between TST and sleep (r = − 0.240, P < 0.001), between TST and stress (r = − 0.190, P < 0.05) and between TST and HI (r = − 0.1935, P < 0.05).
Discussion
Firstly, as expected, sleep deprivation during UTMB® was significant, as previously observed [16, 23]. Secondly, the combination of sleep deprivation and the long and strenuous demand of a MUM produced a heavy physical and psychological impact for several days after the race, illustrated by the duration of recovery. Hence, the evolution of post-race Hooper Index highlighted a long subjective recovery (Fig. 1A) in which muscle soreness and fatigue played a key role. However, our data did not show the usual sleep rebound consistent with such a long sleep deprivation (Fig. 3) and indicated a positive correlation between WASO and muscle soreness. Indeed, the Hooper Index and some of its subitems, the fatigue and the muscle soreness, were augmented by the race (Fig. 1A, B) and athletes required 6 days to return to baseline values, hereby showing the deep and multidimensional fatigue encountered by runners in ultra-endurance events. This is in accordance with previous studies that focused on muscle damage and inflammation after a MUM, where athletes needed 9 days for a physiological recovery, although no data were collected between the 5th and the 9th days [20, 21]. Therefore, these data extracted from a subjective marker, the Hooper Index, are consistent with objective data and would even suggest a shorter recovery period.
These results also indicate an age effect on recovery kinetics, especially on perceived muscle soreness: seniors recovered faster than veterans V1 and V2, whereas there was no significant difference before the race or during the preparation phase. Indeed, the post-race Hooper Index was higher in V1 and V2 than in the Senior group following the race, whereas there was no difference before. The muscle soreness component presented a similar trait, as V1 and V2 runners were exhibiting a higher level of muscle pain after the race. This findings also corroborate recent works suggesting that athletes age should be taken into account for recovery kinetics [4]: aging may produce an increased depletion of energy substrates, greater muscle damage and an altered feeling of fatigue after a race [8, 9, 25]. The rate of muscle protein synthesis, measured 72 h after a MUM, is lower in older athletes, suggesting less efficient “repair and remodelling” mechanisms in these athletes [6]. Age is; therefore, an essential factor to consider when monitoring runners’ recovery during training and post-race recovery phases.
The current literature surrounding sleep parameters after long and strenuous exercise and its impact on sleep deprivation is scarce. Both acute and chronic sleep deprivation negatively impact on reaction time and vigilance [3, 15]. During the UTMB® also, Hurdiel et al. [15] showed that combined acute lack of sleep and strenuous exercise had marked adverse effects on cognitive performances ranging from mere lengthening of response time to serious symptoms, such as visual hallucinations independently of rest duration in race and time in race. The following nights will be important to recover of this sleep deprivation. This study shows that total sleep time (TST) and wake after sleep onset (WASO) were not significantly affected by participating in the UTMB® trail event, despite a WASO peak on the second night after race. Surprisingly, the amount of sleep in trail runners was not increased over the ten nights following the race despite sleep deprivation during the event (Fig. 3), whereas several studies showed an associated “sleep rebound”, including longer phases of slow-wave and REM sleep [1, 2]. In our study, sleep was measured by accelerometer. Although actigraphic assessment of sleep parameters is reliable, the accuracy for some sleep parameters is limited [19]. Also, it is possible that “social synchronizers”, such as professional duties and family commitments, did not allow participants in this study to pay off this sleep debt as fast as professional athletes would, with a more flexible daily time schedule; unfortunately, social data are lacking to enable this to be further investigated. Moreover, it is interesting to note that during nights 6 and 7, corresponding to the first weekend after the race, a small, albeit nonsignificant, increase in TST was observed. It is unlikely that the minor WASO increase observed on the second post-race night was caused by the race-related circadian desynchronization [15]. Nevertheless, these data highlight a correlation between WASO and the level of muscle soreness: the latter may be the main cause of sleep disturbance and the consecutive decline in sleep quality during the second post-race night. In elite rugby players, the use of probiotics decreased muscle soreness and enhanced sleep quantity and quality [11], hereby confirming the negative impact of muscle pain on sleep and its subsequent consequence on recovery process.
Finally, additional correlations between Hooper Index and sleep parameters were observed: the higher the HI, the lower the TST and the higher the WASO. These factors underline the key role of sleep on subjective recovery, already well reported [18]. Sleep quality and quantity should be carefully monitored in amateur trail runners due to their impact on recovery and on the capacity to properly complete a training program over several weeks or months.
This study has some limitations. First, it was based on a single UTMB® involving specific environmental conditions (elevation, temperature, weather conditions); therefore, conclusions are difficult to generalize for all MUM events. Second, the limited number of participants in each age group may explain a high effect size in these results. Third, the presence of a control group would help to distinguish fatigue from strenuous exercise and fatigue from sleep deprivation. Further studies will benefit from the inclusion of female athletes which may reveal potential differences in sleep and recovery between men and women. The sole measure of Hooper Index cannot fully and accurately assess the multidimensional aspects of recovery. The use of additional strategies during recovery period (e.g. compression garments) and the clothes worn during the race were not controlled. Lastly, these results on post-race sleep are interesting and innovative, but must be taken with caution due to strong individual variability. In addition, although actigraphic sleep measurements are validated, the gold standard for measuring sleep parameters remains polysomnography. Accelerometry is not able to retrieve information on sleep stages, especially slow wave and REM sleep; despite its impractical use in extreme environmental conditions, polysomnography, polygraphy or EEG devices would provide valuable information on the relationship between sleep and recovery after UTMB®. Moreover, in this study, information about latency and sleep efficiency was missing because participants filled a sleep diary with subjective bed and wake up hours and no objective data was collected to confirm these declarations.
Conclusion
Performing a 100-mile MUM such as UTMB® produces deep physiological and subjective impact on ultra-trail runners. A 6-day recovery seems necessary to return to pre-race values, but is modulated by age, with recovery appearing to be faster for younger athletes. Despite a substantial lack of sleep accumulated during the race, participants did not quickly pay off their sleep debt by sleeping longer or better; sleep quality was even negatively impacted by muscle soreness. It may be possible that social constraints did not allow participants to pay off this sleep debt and can explain the absence of sleep rebound. Correlations between sleep parameters and Hooper Index then confirm a key role of sleep in a proper recovery.
This study provides some practical implications. On one hand, from a performance point of view, ultra-trail generates a high physical fatigue which requires an adaptation of training modalities during the weeks after the event. The week immediately following the race should be devoted to recovery. On the other hand, participating in an ultra-trail can have an impact on personal and professional life during the post-race weeks. Finally, it would be interesting to use recovery strategies to limit muscle pain and thus improve sleep.
References
Akerstedt T, Kecklund G, Ingre M, Lekander M, Axelsson J. Sleep homeostasis during repeated sleep restriction and recovery: support from EEG dynamics. Sleep. 2009;32(2):217–22. https://doi.org/10.1093/sleep/32.2.217.
Banks S, Van Dongen HPA, Maislin G, Dinges DF. Neurobehavioral dynamics following chronic sleep restriction: dose–response effects of one night for recovery. Sleep. 2010;33(8):1013–26. https://doi.org/10.1093/sleep/33.8.1013.
Belenky G, Wesensten NJ, Thorne DR, Thomas ML, Sing HC, Redmond DP, Russo MB, Balkin TJ. Patterns of performance degradation and restoration during sleep restriction and subsequent recovery: a sleep dose–response study. J Sleep Res. 2003;12(1):1–12. https://doi.org/10.1046/j.1365-2869.2003.00337.x.
Borges NR, Driller MW. Wearable lactate threshold predicting device is valid and reliable in runners. J Strength Cond Res. 2016;30(8):2212–8. https://doi.org/10.1519/JSC.0000000000001307.
Cole RJ, Kripke DF, Gruen W, Mullaney DJ, Gillin JC. Automatic sleep/wake identification from wrist activity. Sleep. 1992;15(5):461–9. https://doi.org/10.1093/sleep/15.5.461.
Doering TM, Jenkins DG, Reaburn PR, Borges NR, Hohmann E, Phillips SM. Lower integrated muscle protein synthesis in masters compared with younger athletes. Med Sci Sports Exerc. 2016;48(8):1613–8. https://doi.org/10.1249/MSS.0000000000000935.
Dyer JB, Crouch JG. Effects of running and other activities on moods. Percept Mot Skills. 1988;67(1):43–50. https://doi.org/10.2466/pms.1988.67.1.43.
Fell J, Reaburn P, Harrison GJ. Altered perception and report of fatigue and recovery in veteran athletes. J Sports Med Phys Fit. 2008;48(2):272–7.
Fell J, Williams D. The effect of aging on skeletal–muscle recovery from exercise: possible implications for aging athletes. J Aging Phys Act. 2008;16(1):97–115. https://doi.org/10.1123/japa.16.1.97.
Halson SL. Nutrition, sleep and recovery. Eur J Sport Sci. 2008;8(2):119–26. https://doi.org/10.1080/17461390801954794.
Harnett JE, Pyne DB, McKune AJ, Penm J, Pumpa KL. Probiotic supplementation elicits favourable changes in muscle soreness and sleep quality in rugby players. J Sci Med Sport. 2020. https://doi.org/10.1016/j.jsams.2020.08.005.
Hillman CH, Erickson KI, Kramer AF. Be smart, exercise your heart: exercise effects on brain and cognition. Nat Rev Neurosci. 2008;9(1):58–65. https://doi.org/10.1038/nrn2298.
Hoffman MD, Badowski N, Chin J, Stuempfle KJ, Parise CA. Determinants of recovery from a 161-km ultramarathon. J Sports Sci. 2017;35(7):669–77. https://doi.org/10.1080/02640414.2016.1183808.
Hooper SL, Mackinnon LT, Howard A, Gordon RD, Bachmann AW. Markers for monitoring overtraining and recovery. Med Sci Sports Exerc. 1995;27(1):106–12.
Hurdiel R, Pezé T, Daugherty J, Girard J, Poussel M, Poletti L, Basset P, Theunynck D. Combined effects of sleep deprivation and strenuous exercise on cognitive performances during The North Face® Ultra Trail du Mont Blanc® (UTMB®). J Sports Sci. 2015;33(7):670–4. https://doi.org/10.1080/02640414.2014.960883.
Hurdiel R, Riedy SM, Millet GP, Mauvieux B, Pezé T, Elsworth-Edelsten C, Martin D, Zunquin G, Dupont G. Cognitive performance and self-reported sleepiness are modulated by time-of-day during a mountain ultramarathon. Res Sports Med. 2018;26(4):482–9. https://doi.org/10.1080/15438627.2018.1492401.
Jürimäe J, Mäestu J, Purge P, Jürimäe T. Changes in stress and recovery after heavy training in rowers. J Sci Med Sport. 2004;7(3):335–9. https://doi.org/10.1016/s1440-2440(04)80028-8.
Kellmann M, Bertollo M, Bosquet L, Brink M, Coutts AJ, Duffield R, Erlacher D, Halson SL, Hecksteden A, Heidari J, Kallus KW, Meeusen R, Mujika I, Robazza C, Skorski S, Venter R, Beckmann J. Recovery and performance in sport: consensus statement. Int J Sports Physiol Perform. 2018;13(2):240–5. https://doi.org/10.1123/ijspp.2017-0759.
Kushida CA, Chang A, Gadkary C, Guilleminault C, Carrillo O, Dement WC. Comparison of actigraphic, polysomnographic, and subjective assessment of sleep parameters in sleep-disordered patients. Sleep Med. 2001;2(5):389–96. https://doi.org/10.1016/S1389-9457(00)00098-8.
Millet G, Verney J, Joassard O, Bankole C, Millet G. Acute cardiovascular responses induced by an ultra-trail. 4th International congress mountain, sport, and health, Rovereto, 2011.
Millet GY. Can neuromuscular fatigue explain running strategies and performance in ultra-marathons?: The flush model. Sports Medicine (Auckland, NZ). 2011;41(6):489–506. https://doi.org/10.2165/11588760-000000000-00000.
Nicolas M, Banizette M, Millet GY. Stress and recovery states after a 24 h ultra-marathon race: a one-month follow-up study. Psychol Sport Exerc. 2011;12(4):368–74. https://doi.org/10.1016/j.psychsport.2011.03.005.
Poussel M, Laroppe J, Hurdiel R, Girard J, Poletti L, Thil C, Didelot A, Chenuel B. Sleep management strategy and performance in an extreme mountain ultra-marathon. Res Sports Med. 2015;23(3):330–6. https://doi.org/10.1080/15438627.2015.1040916.
Robach P, Boisson R-C, Vincent L, Lundby C, Moutereau S, Gergelé L, Michel N, Duthil E, Féasson L, Millet GY. Hemolysis induced by an extreme mountain ultra-marathon is not associated with a decrease in total red blood cell volume. Scand J Med Sci Sports. 2014;24(1):18–27. https://doi.org/10.1111/j.1600-0838.2012.01481.x.
Roth SM, Martel GF, Ivey FM, Lemmer JT, Metter EJ, Hurley BF, Rogers MA. High-volume, heavy-resistance strength training and muscle damage in young and older women. J Appl Physiol. 2000;88(3):1112–8. https://doi.org/10.1152/jappl.2000.88.3.1112.
Scheer V, Basset P, Giovanelli N, Vernillo G, Millet GP, Costa RJS. Defining off-road running: a position statement from the ultra sports science foundation. Int J Sports Med. 2020;41(5):275–84. https://doi.org/10.1055/a-1096-0980.
Tucker AM, Whitney P, Belenky G, Hinson JM, Van Dongen HPA. Effects of sleep deprivation on dissociated components of executive functioning. Sleep. 2010;33(1):47–57. https://doi.org/10.1093/sleep/33.1.47.
UTMB. UTMB®—regulations. 2019. https://utmbmontblanc.com/en/page/16/Regulations.html. Accessed 26 Aug 2019
Vitiello D, Rupp T, Bussière J-L, Robach P, Polge A, Millet GY, Nottin S. Myocardial damages and left and right ventricular strains after an extreme mountain ultra-long duration exercise. Int J Cardiol. 2013;165(2):391–2. https://doi.org/10.1016/j.ijcard.2012.08.053.
World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–4. https://doi.org/10.1001/jama.2013.281053.
Funding
Not applicable. We thank the organization of the Ultra Trail du Mont Blanc® and the Ultra Sports Science foundation for making this study feasible.
Author information
Authors and Affiliations
Contributions
Not applicable.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to declare.
Ethics approval
The study was approved by the UTMB® medical committee and by local ethic committee (no 2018220323).
Consent to participate
All participants gave written informed consent in accordance with the Declaration of Helsinki [30].
Consent for publication
Not applicable (anonymous data).
Availability of Data and Material
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Code Availability
Not applicable.
Rights and permissions
About this article

Cite this article
Baron, P., Hermand, É., Elsworth-Edelsten, C. et al. Sleep and Subjective Recovery in Amateur Trail Runners After the Ultra-Trail du Mont Blanc® (UTMB®). J. of SCI. IN SPORT AND EXERCISE 5, 123–129 (2023). https://doi.org/10.1007/s42978-021-00154-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42978-021-00154-w