
Abstract
Past research suggests that higher coherence between feelings and physiology under stress may confer regulatory advantages. Research and theory also suggest that higher resting vagal tone (rVT) may promote more adaptive responses to stress. The present study examines the roles of response system coherence (RSC; defined as the within-individual covariation between feelings and heart rate over time) and rVT in mediating the links between childhood adversity and later-life responses to acute stressors. Using data from 279 adults from the Second Generation Study of the Harvard Study of Adult Development who completed stressful public speaking and mental arithmetic tasks, we find that individuals who report more childhood adversity have lower RSC, but not lower rVT. We further find that lower RSC mediates the association between adversity and slower cardiovascular recovery. Higher rVT in the present study is linked to less intense cardiovascular reactivity to stress, but not to quicker recovery or to the subjective experience of negative affect after the stressful tasks. Additional analyses indicate links between RSC and mindfulness and replicate previous findings connecting RSC to emotion regulation and well-being outcomes. Taken together, these findings are consistent with the idea that uncoupling between physiological and emotional streams of affective experiences may be one of the mechanisms connecting early adversity to later-life affective responses. These findings also provide evidence that RSC and rVT are associated with distinct aspects of self-regulation under stress.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Adapting to the emotional twists and turns of everyday life is much like boating along a fast-moving river: having a clear view of the waves and being able to steer the boat through turbulent waters are both important for a smooth journey. Two largely independent lines of research shed light on individuals’ ability to notice their emotional, physiological, and behavioral responses to emotional challenges and to modify them effectively. First, an emerging body of work on Response System Coherence (RSC) suggests that tighter coherence between one’s subjective experience of emotions and physiology over time (e.g., the extent to which an increase in heart rate accompanies an increase in negative affect) may promote greater awareness of inner experiences and needs (Brown et al., 2020; Sommerfeldt et al., 2019; Sze et al., 2010). Such awareness may facilitate more effective responses to emotional challenges (e.g., by alerting an individual to the need to enact or discontinue a regulatory strategy; Brown et al., 2020). However, it is not in itself sufficient to ensure the success of one’s regulatory efforts. Individuals must also be able to calibrate their regulatory resources, such as arousal and attention, in ways that further their regulatory goals and meet the more general demands of the situation (Bonanno & Burton, 2013; Lazarus, 1991). A separate but related line of research suggests that this ability to self-regulate is indexed by resting vagal tone (rVT)—a marker of parasympathetic influences on cardiac activity (Holzman & Bridgett, 2017; Thayer et al., 2009).
Despite its conceptual importance, RSC’s link to rVT, as well as their joint roles in shaping responses to ongoing emotional challenges, has not been explored empirically. The sources of individual differences in RSC and rVT also remain poorly understood.
Childhood Adversity as a Source of Individual Differences in RSC and rVT
There are theoretical and empirical reasons to believe that both RSC and rVT may be shaped by the experience of adversity in childhood. Some forms of adversity have been linked to impairments in individuals’ ability to identify their own emotions (e.g., Brown et al., 2016; Matti et al., 2008). It has also been speculated that such impairments can contribute to “uncoupling” between experiential and physiological channels of emotion (e.g., Gunnar & Donzella, 2002; Repetti et al., 2002), but no studies to date have directly examined the links between childhood adversity and RSC. Similarly, early life stress and negative parenting practices have been linked to disruptions in the development and function of the parasympathetic nervous system prior to adulthood (e.g., Graham et al., 2017; Johnson et al., 2017). However, evidence for the longer-term associations between adverse childhood experiences and rVT has been inconsistent (e.g., Dale et al., 2018; Hagan et al., 2017).
Roles of RSC and rVT in Shaping Reactivity and Recovery
Past research demonstrates that both high RSC and rVT are linked to greater subjective well-being and lower levels of inflammatory markers (Brown et al., 2020; Kok & Fredrickson, 2010; Marsland et al., 2007; Sommerfeldt et al., 2019). It is possible that these links are at least partially driven by the accrued benefits of better responses to emotional challenges in day-to-day life (Brown et al., 2020; Diener et al., 2009; Luhmann et al., 2012). Consistent with this possibility, high rVT has been shown to predict less intense reactions to acute stressors and better post-stress recovery (Scott & Weems, 2014; Weber et al., 2010). Furthermore, experimentally induced increases in heart rate variability (HRV)—a commonly used measure of vagal tone—have been linked to reductions in stress and anxiety across a number of studies (see review by Goessl et al., 2017). Taken together, these findings raise an exciting possibility that rVT may play a causal role in shaping reactivity and recovery.
No studies to date have examined the links between RSC and responses to emotional challenges as they unfold in real time. It has been proposed that higher coherence between feelings and physiology promotes greater awareness of internal experiences, which, in turn, can help efficiently mobilize coping resources (Brown et al., 2020). However, whether such awareness has adaptive benefits or not may depend on the underlying motivations for paying attention to one’s experiences (Hayes, 2004; Mehling et al., 2009). Awareness that is driven by the need to feel in control and avoid potential threats might lead to increased negative affect as well as more negative long-term outcomes (Ginzburg et al., 2014). In contrast, awareness characterized by a nonjudgmental attitude—an attitude that has been linked to mindfulness (Shapiro et al., 2006)—has been shown to reduce negative emotional reactivity to stressors and facilitate better post-stress recovery (Crosswell et al., 2017; Lindsay et al., 2018). Nevertheless, the links between RSC and mindfulness have not been investigated directly.
Current Study
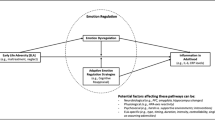
In the present study, we test a model that posits RSC and rVT as parallel mediators of links between childhood adversity and several components of the stress response (Fig. 1). Specifically, we focus on cardiovascular and emotional reactivity to and recovery from a social stressor (public speaking and mental arithmetic tasks in a context in which one is being evaluated). We hypothesize that greater adversity will be linked with lower RSC and rVT, which, in turn, will be connected with higher cardiovascularFootnote 1 reactivity to stress, slower recovery, and more negative affect. We conduct additional analyses aimed at furthering the existing understanding of RSC and its link to well-being and adaptive emotion regulation. We hypothesize that higher RSC will be associated with higher trait mindfulness. In addition, we seek to replicate recent findings showing that higher RSC is linked with higher self-reported indicators of subjective well-being and less suppression of negative emotions (Brown et al., 2020; Sommerfeldt et al., 2019).

Hypothesized theoretical model of the associations among childhood adversity, RSC, rVT, and responses to stress
Method
Participants
Three hundred and five men and women from the Second Generation Study of the Harvard Study of Adult Development (Morrill et al., 2019) participated in an in-person laboratory visit. Of those 305, only those participants who completed stressful public speaking and mental arithmetic tasks during the lab visit (n = 279) were included in the present study.Footnote 2 Participants came from 206 different families with an average of 1.35 (SD = .90) siblings per family. The sample was 47.3% male and 52.7% female, with a mean age of 61.90 years (SD = 8.13) and a median annual household income of $105,000. Reflecting the demographics of their parents who were recruited from Boston for the original Harvard Study of Adult Development in the 1930s and 1940s, 98.4% of participants were Caucasian. Participants who completed the lab visit did not differ from the larger Second Generation sample (total including lab visit participants = 1311) in their age, gender, race, income, trait mindfulness, or amount of childhood adversity.
Procedure
The lab visit took, on average, 2.5 h, and its purpose was to collect data on physical health and reactions to stress. Participants were paid $75 for completing the lab visit. Lab participants had already completed a survey that included childhood adversity questions as well as the short form of the Five Facets of Mindfulness Questionnaire (FFMQ-SF; Bohlmeijer et al., 2011). The average time between completion of the survey and participation in the lab visit was 1 year.
The timeline of tasks and measures during the lab visit is summarized in Fig. 2. Following an informed consent procedure, heart rate was measured and stored continuously throughout the entire lab visit via an eMotion Faros 180o device (Mega Electronics Ltd., Kuopio, Finland) with 2-electrode cable placement sampled at 1000 Hz. Questions regarding caffeine and alcohol use just prior to the session were recorded. During HRV intervals, subjects were instructed to maintain a relaxed but upright posture and asked to watch a low-demand cognitive “Vanilla Task” (Jennings et al., 1992) to improve accuracy and provide for a stable baseline. After the initial baseline HRV and blood pressure measurements, a series of functional measures (e.g., hand strength, walking speed, etc.) were collected for the larger study. Following an optional break, participants completed the Trier Social Stress Test (TSST; Kirschbaum et al., 1993). As part of the TSST, participants were asked to prepare (3 min) and present (5 min) a speech about themselves, and to complete a series of challenging mental arithmetic tasks (5 min). Participants reported on their momentary emotions immediately before (T1) and after (T2) the TSST. Participants were debriefed on the purposes of the TSST and offered a break before proceeding to an Expressive Writing task. The Writing Task, in which participants were asked to write for 10 min about a low point in their lives, was designed to simulate a more private (compared to the TSST) emotional challenge (see Petrova et al., 2021). Participants reported on their momentary emotions immediately before (T3) and after (T4) the writing task. The only data from the writing task that were used in the present study (to calculate RSC coefficients) are (1) participants’ self-reports of negative affect after the writing task and (2) participants’ heart rate after the writing task. After the writing task, participants completed an interview that included questions about participants’ experience in the writing task, as well as questions about positive experiences in their lives. Participants were debriefed and offered an opportunity to ask questions about the lab visit or the study before departing from the lab.

Timeline of the relevant part of the lab visit. Cardiovascular measures are shown as hearts. Negative affect measures are shown as emoticons. RSC measure was based on heart rate and negative affect from T1, T2, and T4. The outcome measure of post-TSST negative affect was based on T2 negative affect
Measures
Cardiovascular Reactivity and Recovery
All heart rate data were processed using Kubios HRV Premium (Version 3.1, Tarvainen et al., 2014). Each participant’s heart rate data were carefully examined for ectopic beats, noise, and other irregularities.
Cardiovascular reactivity to the TSST was operationalized as the difference score between the average heart rate during the first 60 s of the speech part of the TSST and average heart rate during the 60 s immediately before the preparation part of the TSST (see Fig. 2). Because the magnitude of cardiovascular responses is known to be influenced by baseline heart rate (Berntson et al., 1994), we controlled for pre-TSST heart rate in all analyses that included the heart rate reactivity score.
Cardiovascular recovery was operationalized as the exponential rate of decay in heart rate during the 2 min immediately after the TSST. Heart rate recovery is a complex process that unfolds over time, and past research demonstrates that an initial sharp decrease in heart rate following exercise-induced increases in cardiac output is followed by a slower, steadier decrease (Imai et al., 1994). A first-order exponential decay curve has been shown to be a reasonable model of HR recovery (Bartels-Ferreira et al., 2015; Pierpont et al., 2000). In addition to better capturing the shape of the recovery trajectory, the exponential decay approach has important computational advantages. Namely, it relies on substantially more data points compared to the more traditional difference score approaches, thus strengthening the reliability of the measure (see Berntson et al., 1994; Willett, 1994). Importantly, it also makes it less likely that the intensity of individuals’ initial responses to the TSST or their baseline levels of HR will drive the index of recovery.
Continuous heart rate recordings from these 120 s were divided into twelve 10-s long epochs, and the average heart rate for each epoch was calculated. The resulting 12 epochs of heart rate for each participant were then used to estimate a nonlinear latent growth curve model with the rate of exponential decay in heart rate modeled as a random coefficient varying across individuals (model and code adapted from Grimm et al., 2011):
where π0i is the initial heart rate for individual i; si is the amount of change in heart rate from the intercept to the lower asymptote for individual i; αi is the exponential rate of change for individual i (with higher, more positive coefficients indicating faster decay rates), and εit is the time-varying residual. The model was estimated in Mplus (Version 8.3, Muthén & Muthén, 1998-2017), and exponential decay coefficients (αi) for all participants were exported for use in the main analyses. Extreme observations (> 3 standard deviations above the average decay rate; n = 2) were winsorized to equal the highest observed rate of decay below 3 standard deviations from the mean. Key model parameters are reported in the online supplement (Supplementary Table 1).
Negative Affect
A self-report measure developed by Tamir et al., (2007) was used to assess participants’ experience of negative affect at four points during the lab visit (only three of the four time points were used in the present study; see “Procedures” and Fig. 2 for additional details). Participants were presented with 7 triplets of negative emotions: anxious/worried/fearful, lonely/distant/isolated, sad/depressed/down, rejected/put down/hurt/, judged/scrutinized/evaluated, angry/irritated/provoked, and embarrassed/humiliated/ashamed. Participants were asked to indicate the extent to which they felt each triplet at the time of assessment using a scale ranging from 1 = not at all to 7 = very much. Visual inspection of the group trajectories of the 7 triplets indicated that the judged/scrutinized/evaluated triplet had a unique trajectory. Moreover, inclusion of this triplet reduced the overall internal consistency of the negative affect measure, so it was dropped from the scale. The scores on the remaining 6 triplets were averaged at each of the three time points to derive indices of overall negative affect at key points in the lab visit for each participant. Internal consistency ranged from α = .82 to α = .86 across the three time points.
Response System Coherence
We operationalize response system coherence (RSC) as the within-person covariation between negative affect and heart rate over time (i.e., the extent to which an increase in heart rate accompanies an increase in negative affect). Following procedures used in prior research (e.g., Sommerfeldt et al., 2019), RSC was quantified as the within-person slope of the relationship between heart rate and person-mean-centered negative affect over time. Participants’ heart rate (HR) during the first 30 s of filling out the negative emotions self-reports at times T1 (pre-TSST baseline), T2 (post-TSST), and T4 (after the expressive writing task) was used (see Fig. 2).Footnote 3 Following an established procedure (Bolger et al., 1989; Cohen et al., 2005), individual RSC coefficients were estimated using a two-level random intercepts and slopes linear regression model with negative affect (NA) as a person-mean-centered predictor of heart rate (HR):
Unstandardized slopes (π1i) for all participants were then exported for use as RSC coefficients in the main analyses. Key model parameters are reported in the online supplement (Supplementary Table 2). A total of 34 participants (12% of the sample) had no variation in self-reported negative affect across the three time points that were used to calculate RSC, which precluded obtaining reliable coherence coefficients for these participants. We found that all 34 of these participants reported experiencing none of the five negative emotions across any of the three time points (M = 1.00, SD = 0.00). The 34 excluded participants also had lower variability in heart rate across the three time points, though that difference was not significant (excluded, variance = 3.45; not excluded, variance = 6.67, p = .134). Finally, we compared the 34 excluded participants to the rest of the sample on key variables of interest. Interestingly, we found that participants with no variability in negative affect did not differ from the rest of the sample on any of the key study variables with the exception of trait mindfulness. Surprisingly, excluded participants had higher trait mindfulness compared to those who had some variability in negative affect (excluded M = 94.95, SD = 11.72; not excluded M = 89.04, SD = 11.93, p < .05, d = .50).
Half of the participants had negative coherence coefficients. Consistent with the view that negative scores indicate a lack of positive coherence, and that variation in negative coherence coefficients is not meaningful, all RSC coefficients were censored from below (that is, all negative coefficients were recoded as “0”).Footnote 4 The positive skew that resulted from this conversion was reduced using a standard square root transformation.
Resting Vagal Tone
Resting high frequency heart rate variability (hf-HRV) is commonly used as an index of resting vagal tone (see Laborde et al., 2017). In the present study, HRV was measured over two 5-min periods before the TSST. An autoregressive (AR) spectral analysis was used to derive high frequency (HF) HRV from R-R interval segments with a normal sinus rhythm. The parameter for the HF band was set at 0.15–0.4 Hz. A standard log-transformation was applied to reduce the skew. Normalized HF-HRV scores measured over two 5-min baseline periods were highly correlated (r = .78) and were averaged into one combined score to improve reliability. Following the same procedure that was used to process heart rate reactivity and recovery data, the raw inter-beat intervals were manually inspected and corrected for missed and false R-peaks, as well as nonsinus beats and other technical artifacts using Kubios HRV analysis package 3.1 (Tarvainen et al., 2014). Manual inspection and correction did not use the deletion method as this may introduce step-like shapes into R-R interval time series (Peltola, 2012). Next, automated correction via Kubios utilizing cubic spline interpolation was performed using the lowest automated level necessary for a given sample. Given that short-term HRV analyses are more sensitive to artifacts and editing, we rejected samples in which greater than 5% of the R-R intervals required correction as per published recommendations (Peltola, 2012; Quintana et al., 2016).
Childhood Adversity
Childhood adversity was measured by 28 items drawn from the Adverse Childhood Experiences scale (ACE; Felitti et al., 1998) and the Risky Family Environment measure (Repetti et al., 2002; Taylor et al., 2004), as well as 11 additional events, including financial, school, and neighborhood stressors, bullying, violence outside of home, prolonged separation from primary caregivers, death and physical illness of caregivers and other family members, and stressful family transitions. Participants were asked to indicate whether each event had occurred (yes or no) at any point before they turned 19. A previous study (Morrill et al., 2019) established a multilevel factor structure with 22 out of the 28 adverse events that was replicated in the present study (Fig. 3). At the within-family level, the 6 factors were Family Conflict, Impaired Caregiving, Parental Dysfunction, Financial Insecurity, Poor Child-Environment Fit, and Household Dysfunction. The three between-family factors were Chaotic Families, Stressful Environment, and Poor Family-Environment Fit. In the present study, the 6 within-family factors were modeled as indicators of a superordinate childhood adversity factor. The full multilevel factor structure with overall childhood adversity as a superordinate level-1 factor was used in the main analyses.

Multilevel factor structure of childhood adversity. Standardized factor loadings and correlations are shown. Dashed lines removed from the model. A aggregated to level 2
The binary nature of the childhood adversity data poses a computational challenge for MSEM (for more information, see Morrill et al., 2019). Bayesian estimation is an effective approach for modeling binary outcomes in multilevel confirmatory factor analysis (CFA) models (Muthén & Asparouhov, 2012). We used Bayesian estimation (in Mplus v. 8.3) with two parallel chains of 20,000 iterations each to estimate the MSEM models. Default non-informative priors (N(0, 1010) for intercepts, factor loadings, and slopes of normally distributed continuous variables, and N(0, 5) for categorical variables) were used in all analyses (Asparouhov & Muthén, 2010). The 95% credibility intervals (CrIs) were used to assess the statistical significance of individual model parameters. The posterior predictive p value (PPP) for the chi-square values generated by posterior predictive checking can be interpreted as the probability that replicated data are as extreme or more extreme than the observed data (Scheines et al., 1999). The PPP was used as an index of the overall model fit, with values above .05 providing evidence of model fit (Muthén & Asparouhov, 2012).
Standardized factor loadings at the within-family level ranged from .41 to .96 (M = .75) and were highly similar to those reported by Morrill et al. in the full sample (n = 1311) from which the 279 participants who took part in the lab visit were drawn. Standardized factor loadings for the level-1 superordinate Childhood Adversity factor ranged from .39 to .94 (M = .72). At the between-family level, severe sexual maltreatment and unsafe neighborhood loaded poorly, with standardized factor loadings of − .19 and .13, respectively. Based on the guidelines proposed by Comrey and Lee (1992), the decision was made to remove these items from the level-2 model. Overall, factor loadings at level 2 ranged from .32 to .91 (M = .66). The resulting factor structure provided an excellent fit to the data, posterior predictive p value (PPP) = .380. Key descriptive statistics for each of the 22 binary items are presented in the online supplement (Supplementary Table 3).
Trait Mindfulness
Trait mindfulness was assessed with the short form of the Five Facets of Mindfulness Questionnaire (FFMQ-SF, Bohlmeijer et al., 2011). The FFMQ-SF measures five facets of mindfulness: Observing, Describing, Acting with Awareness, Non-Judging, and Non-Reactivity (Bohlmeijer et al., 2011). Each facet is measured with 5 items, except for Observing, which is measured with 4 items. Each item (e.g., When I have distressing thoughts or images I am able just to notice them without reacting—Non-Reactivity) is accompanied by a response scale ranging from 1 = never or very rarely true to 5 = very often or always true, with higher scores corresponding to higher levels of trait mindfulness. In the present study, the total trait mindfulness score for each participant was calculated by summing (after reverse scoring as needed) scores on all 24 items across the 5 facets. The FFMQ-SF had a high level of internal reliability, α = .87, in this study.
Emotion Regulation: Reappraisal and Expressive Suppression
The Emotion Regulation Questionnaire (ERQ; Gross & John, 2003) was used to assess a tendency to use reappraisal and expressive suppression. The questionnaire consists of 10 statements rated on a scale of 1 = disagree strongly to 7 = agree strongly. Reappraisal is measured by 6 items, e.g., When I want to feel more positive emotion (such as joy or amusement), I change what I am thinking about. The internal consistency of the reappraisal subscale in this sample was high, α = .88. Expressive suppression is measured by 4 items, e.g., I keep my emotions to myself. The suppression subscale also had a high level of internal consistency, α = .81. Participants’ responses to both scales were reversed prior to data analyses so that higher scores corresponded to higher levels of reappraisal and suppression.
Life Satisfaction
Life satisfaction was measured with a single item (Prenda & Lachman, 2001): Using a 0 to 10 scale, where 0 means “the worst possible life overall” and 10 means “the best possible life overall,” how would you rate your life overall these days?
Data Analysis
The data in this study present several statistical challenges. The first challenge is posed by the nested nature of the sample and the possibility that nesting will bias estimates of standard errors. Participants in the present study consist of siblings nested in 206 families. The intraclass correlations (ICCs) for variables of interest ranged widely (from .01 to .65; see Table 1 and Supplementary Table 3), indicating that, at the high end, close to two-thirds of the total variation was due to family factors and at the low end, only 1% of the total variation was due to family factors. To address the potential biasing effects of the nested nature of the sample, we used multilevel structural equation modeling (MSEM), implemented in Mplus (Version 8.3, Muthén & Muthén, 1998-2017). All regression and correlation coefficients reported throughout the paper are individual (within-family) estimates.
It is important to note the implications of having such a wide range of ICCs for interpretation of key outcomes. Unsurprisingly, individual childhood adversity items had the highest ICCs, indicating that two or more members of the same family tended to be relatively more similar (in the kinds of adverse events they report) to one another than to other participants in the sample. Of greater conceptual importance is the variability in the ICCs of the endogenous (outcome) variables. ICCs for endogenous variables ranged from .01 to .24 (average = .10), indicating that, on average, 90% of the total variance in these variables was due to variation at the individual (within-family) level. This means that the model we used (controlling for family level variance) can explain up to 99% of the total (across all levels) variation in variables of interest at the high end (rVT), and up to 76% (RSC) at the low end.
There was a complex pattern of missing data in the sample. Full-information Bayesian estimation (or maximum likelihood for analyses that were conducted outside of the main MSEM model) was used in all correlational and regression analyses to account for these missing data. Heart rate data were unavailable for a small number of participants due to excessive noise in the data (n = 5) or equipment malfunction (n = 1). Participants’ HRV data were not included in analyses if they reported taking medications that affect heart rate and heart rate variability, including antipsychotics (n = 6), stimulants (n = 4), and non beta blocker anti-arrhythmic medications (n = 1; see Alvares et al., 2016; Kelly et al., 2014; Zuanetti et al., 1991 for additional details on HRV and medication use). In addition to those whose data were excluded due to medication, HRV measures were missing for 27 participants due to a high number of ectopic beats (> 10% premature atrial or ventricular contractions in both 5-min long HRV samples, n = 26) or equipment malfunction (n = 1). Excessive noise and/or unreliable time stamps at specific points during the lab visit precluded us from obtaining cardiovascular reactivity, recovery or RSC data for some participants (no more than 9% per measure). Finally, 6 participants did not complete the childhood adversity and trait mindfulness questionnaires, and 5 participants did not complete the life satisfaction and emotion regulation measures.
Results
Preliminary Analyses
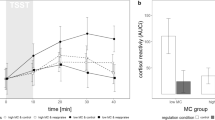
Means, standard deviations, intraclass correlations (ICCs), and bivariate correlations for key study variables are presented in Tables 1 and 2. The general pattern of affective and cardiovascular responses to the tasks in the lab visit is shown in the Supplementary Fig. 2. Participants experienced a large increase in negative affect from baseline to immediately after the TSST, Wald’s W = 31.61, p < .001, d = .80.Footnote 5 Similarly, participants experienced an increase in heart rate (M = 6.68, SD = 8.00 beats per minute) from the pre-TSST baseline to the first minute of the speech portion of the TSST, W = 4.95, p = .02, d = .59.
RSC and rVT Mediating Links Between Childhood Adversity and Stress Responses
The proposed model, positing RSC and rVT as parallel mediators of the links between childhood adversity and responses to stress, was estimated with MSEM. The overall model provided an excellent fit to the data, PPP = .24 (Fig. 4). Convergence diagnostics for Markov Chain Monte Carlo (MCMC) chains are available in the Supplementary Material.

Full MSEM model testing the links among childhood adversity, RSC, rVT, and responses to stress. Standardized coefficients are presented. Black lines, 95% CrI excludes 0; gray lines, 95% CrI overlaps with 0. Dashed lines, direct paths after accounting for indirect paths. Bold black lines, significant indirect pathway
We found partial support for the hypothesis that RSC and rVT are linked to more adaptive responses to stress and to childhood adversity. Specifically, childhood adversity was negatively correlated with RSC, β = − .23, CrI [− .43, − .02]. However, there was no association between childhood adversity and rVT, β = .01, CrI [− .17, .19]. Individuals in this study who reported more childhood adversity also reported more negative affect after the TSST, βbivariate = .17, CrI [.007, .34] and took longer to recover, βbivariate = − .17, CrI [− .33, − .01], but there was no direct link between childhood adversity and cardiovascular reactivity, β = − .06, CrI [− .25, .14]. Consistent with our expectations, higher RSC in the full model was associated with faster cardiovascular recovery from stress, β = .24, CrI [.08, .41]. In the full MSEM model, the link between higher childhood adversity and slower cardiovascular recovery was mediated by lower RSC (unstandardized 95% CrI [− .15, − .002]).Footnote 6 This indirect effect accounted for 30.9% of the total link between childhood adversity and speed of cardiovascular recovery. There were no other significant indirect effects in the full MSEM model.
Higher RSC was linked to higher cardiovascular reactivity, β = .36, CrI [.20, .51]. In addition, although there was a small negative correlation between RSC and negative affect outside of the MSEM model, βbivariate = − .14, p = .04, this relationship was no longer significant once we controlled for other elements of the model, β = − .09, CrI [− .26, .08]. As hypothesized, higher rVT predicted lower cardiovascular reactivity to the TSST βbivariate = − .17, p = .03. However, this relationship was not significant when tested as part of the full MSEM model, β = − .13, CrI [− .28, .02]. Contrary to our expectations, rVT was not linked with the speed of cardiovascular recovery, β = − .11, CrI [− .25, .05] or self-reported negative affect after the social stress test, β = − .05, CrI [− .19, .10]. Finally, there was no significant association between rVT and RSC, rbivariate = − .11, p = .16.
Response System Coherence and Individual Functioning
Consistent with our expectations, individuals with higher levels of trait mindfulness also had higher RSC during the lab visit, r = .18, p < .01. In a series of additional exploratory analyses, we examined whether trait mindfulness facets moderated the within-individual association between heart rate and negative affect. We found that individuals with higher scores on the Describing facet of the FFMQ had tighter coherence between feelings and physiology, r = .25, p < .001. There is also evidence that higher RSC may be associated with higher scores on the Awareness facet, r = .15, p = .05. A more detailed summary of these additional analyses is presented in the Supplementary Table 4.
Finally, replicating previous findings, we found that individuals with higher RSC reported higher levels of life satisfaction, r = .12, p < .01. Higher RSC in this sample was also associated with a greater tendency to reappraise, r = .10, p = .044, and less tendency to suppress the expression of emotion, r = − .21, p < .001.
Discussion
The ability to manage negative emotions in the face of everyday challenges is one of the fundamental building blocks of emotional and physical well-being. The present study extends earlier work on the sources of individual differences in this ability by examining the roles of RSC and rVT in mediating the links between childhood adversity and responses to stress.
Our findings show that childhood adversity is linked to lower RSC, but not rVT, and that RSC mediates the link between adversity and cardiovascular recovery. This finding points to uncoupling between physiological and experiential streams of emotion as one of the potential mechanisms driving the long-term effects of early life stress. Such uncoupling may be driven by early adversity’s impact on individuals’ ability to identify and describe emotional experiences (Brown et al., 2016; Matti et al., 2008). Another related possibility is that individuals who experienced more childhood adversity tend to rely more heavily on disengagement- and suppression-oriented regulatory strategies (Borwn et al., 2013; Gratz et al., 2007; Hagan et al., 2017). Use of such strategies has been linked to lower RSC (Dan-Glauser & Gross, 2013; Sommerfeldt et al., 2019) and greater difficulty recovering from stressful events (e.g., Kross & Ayduk, 2008). It is also conceivable that low-RSC individuals may remember their early experiences as more stressful. Longitudinal studies would help clarify the short- and long-term effects of early life stress on RSC.
Although the absence of a link between childhood adversity and rVT in this study is consistent with some previous work (e.g., Duprey et al., 2019; Hagan et al., 2017), it raises questions deserving further consideration. Did our focus on the overall amount of adversity obscure unique effects of different forms and timings of adversity on parasympathetic nervous system functioning? Additional exploratory analyses found that rVT was not associated with any of the six adversity factors (see Supplementary Materials). Future studies should examine if adverse experiences that take place during specific periods in development may be particularly detrimental to the long-term functioning of the parasympathetic nervous system. Potential nonlinear effects of early life stress on rVT and responses to stress (see Kogan et al., 2013) should also be considered.
In addition to establishing the connection between RSC and childhood adversity, the present study is the first to examine RSC and rVT simultaneously in the context of the same stressor. Notably, RSC and rVT in the present study were associated with different phases of the stress response. rVT was linked with the intensity of individuals’ immediate physiological responses to stress. RSC, on the other hand, was linked with more downstream outcomes related to re-establishing emotional and physiological equilibrium. These differences may have important implications for health and well-being. Understanding the mechanisms underlying this specificity in the effects of RSC and rVT is a critical research goal. Previous research demonstrates that the tendency to dwell on negative emotions after a stressor has terminated has been shown to be a risk factor for a wide range of maladaptive outcomes (e.g., McLaughlin & Nolen-Hoeksema, 2011). Similarly, cardiovascular recovery has been shown to predict later cardiovascular health outcomes (e.g., Steptoe & Marmot, 2005). Consistent with these findings, high-RSC individuals who can recover and let go of negative emotions more quickly may still show, over longer periods of time, positive signs of well-being even if their immediate reactions to stressors tend to be more intense. Future work aimed at examining this possibility and identifying ways of promoting greater coherence may have important implications for clinical practice. Another intriguing possibility that deserves further attention is that high RSC and rVT may not only facilitate more adaptive affective reactions to discrete stressors but help promote more flexible responses to changing environmental demands (Bonanno & Burton, 2013; Kashdan & Rottenberg, 2010).
Our study adds to the growing evidence that coherence between different streams of emotional experience confers regulatory advantages. We employed a time- and cost-efficient approach to measuring coherence between feelings and heart rate using three time points around a stressor. Using this approach, we successfully replicated findings from studies that used more complex and costly RSC measures to show that coherence is associated with subjective well-being and emotion regulation (Brown et al., 2020; Sommerfeldt et al., 2019). Furthermore, our study empirically establishes the connection between RSC and trait mindfulness. Supplementing our core analyses with exploratory ones using individual facets of mindfulness, we found that individuals who can accurately describe their experiences and those who tend to act with awareness have tighter coherence between feelings and physiology. These findings lend support to the previously theorized relationship between RSC and a nonjudgmental way of paying attention to emotional and bodily experiences (e.g., Mauss et al., 2005; Sommerfeldt et al., 2019).
Some limitations of this research should also be acknowledged. First, the lack of clear temporal separation between the measures in the lab visit requires caution in inferring the direction of influence among variables in the mediation model. It is possible, even likely, that more complex bi-directional links exist between RSC/rVT and responses to stress. Consistent with this possibility, our findings join those of previous studies in showing that RSC is linked with more intense (cardiovascular) responses to stress. This raises questions about the balance between stable intra-personal and situationally-driven influences on RSC. Another potential limitation is that self-reported negative affect after the TSST was used both as a part of the RSC measure and as one of the outcomes in the present study. Because RSC was operationalized as the slope of the within-person association between heart rate and person-mean-centered negative affect, and because only one of the six datapoints that were used to calculate RSC coefficients was also examined as an outcome in the present study, it is highly unlikely that this overlap inflated associations between levels of coherence and affective responses. To test this, future studies should employ separate tasks for establishing RSC and examining its regulatory sequelae. Additionally, despite the good demonstrated validity of the RSC measure in the present study, caution must be exercised when using similar approaches in future research. A small number of time points for estimating RSC coefficients restricts the amount of within-person variability in negative affect and physiology, thus making this approach less well suited for capturing coherence in situations that lack a potent stressor like the TSST. Finally, childhood adversity in this study was measured by retrospective reports, which may be subject to a number of biases (Hardt & Rutter, 2004).
In conclusion, the present study elucidates the potentially distinct roles of RSC and rVT in shaping reactivity to and recovery from stress and provides evidence that individuals reporting greater childhood adversity have less coherence between physiological and emotional streams of affective experience.
Notes
Of those who did not participate in the stressful task, 21 were screened out due to health concerns (either high baseline blood pressure, n = 19, or psychiatric conditions, n = 2). An additional 5 participants elected not to participate in the task.
The exact timing of self-report 3 (pre-writing task) was not reliably recorded for all individuals and, thus, could not be used to calculate RSC scores.
Previous studies of RSC have used alternative strategies to handle negative coherence coefficients, including allowing the sign of the coefficient to be negative (e.g., Sommerfeldt et al., 2019), or using the absolute value of the coefficients. The latter strategy is particularly compelling when both physiological and self-reported measures are collected at a high temporal resolution, so that discrete changes in subjective emotional experience (that can be associated with discrete increases or decreases in physiological activation) are captured (e.g., Brown et al., 2020; for a more detailed discussion of this issue, see Bradley & Lang, 2007). To examine whether other ways of dealing with the negative coefficients might affect key results in this study, we estimated the full hypothesized model using both censored and un-censored RSC scores. No significant differences in parameter estimates or their significance levels emerged. Results reported throughout the paper are based on analyses that use censored RSC scores. Results using un-censored scores are reported in the online supplement (Supplementary Figure 1).
To compare the pre- and post-TSST means while taking the nesting into account, we specified a mixture model that has two known classes corresponding to time 1 (pre-TSST) and time 2 (during/post-TSST). Each class-specific sub-model only has the individual-level mean of heart rate or negative affect in it. We then imposed an equality constraint on the two time-specific sub-models and used the Wald’s test to assess the constraint.
References
Alvares, G. A., Quintana, D. S., Hickie, I. B., & Guastella, A. J. (2016). Autonomic nervous system dysfunction in psychiatric disorders and the impact of psychotropic medications: A systematic review and meta-analysis. Journal of Psychiatry & Neuroscience, 41(2), 89–104. https://doi.org/10.1503/jpn.140217.
Asparouhov, T., & Muthén, B. (2010). Bayesian analysis using Mplus: Technical implementation. http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.310.3903&rep=rep1&type=pdf
Bartels-Ferreira, R., de Sousa, É. D., Trevizani, G. A., Silva, L. P., Nakamura, F. Y., Forjaz, C. L. M., Lima, J. R. P., & Peçanha, T. (2015). Can a first-order exponential decay model fit heart rate recovery after resistance exercise? Clinical Physiology and Functional Imaging, 35(2), 98–103. https://doi.org/10.1111/cpf.12132.
Berntson, G. G., Uchino, B. N., & Cacioppo, J. T. (1994). Origins of baseline variance and the law of initial values. Psychophysiology, 31(2), 204–210. https://doi.org/10.1111/j.1469-8986.1994.tb01042.x.
Bohlmeijer, E., ten Klooster, P. M., Fledderus, M., Veehof, M., & Baer, R. (2011). Psychometric properties of the Five Facet Mindfulness Questionnaire in depressed adults and development of a short form. Assessment, 18(3), 308–320. https://doi.org/10.1177/1073191111408231.
Bolger, N., DeLongis, A., Kessler, R. C., & Schilling, E. A. (1989). Effects of daily stress on negative mood. Journal of Personality and Social Psychology, 57(5), 808–818. https://doi.org/10.1037/0022-3514.57.5.808.
Bonanno, G. A., & Burton, C. L. (2013). Regulatory flexibility: An individual differences perspective on coping and emotion regulation. Perspectives on Psychological Science, 8(6), 591–612. https://doi.org/10.1177/1745691613504116.
Bradley, M. M., & Lang, P. J. (2007). Emotion and motivation. In J. T. Cacioppo, L. G. Tassinary, & G. G. Berntson (Eds.), Handbook of psychophysiology (pp. 581–607). Cambridge University Press. https://doi.org/10.1017/CBO9780511546396.025.
Brown, C. L., Oudekerk, B. A., Szwedo, D. E., & Allen, J. P. (2013). Inter-parent Aggression as a Precursor to Disengagement Coping in Emerging Adulthood: The Buffering Role of Friendship Competence: Parent Conflict and Coping. Social Development. https://doi.org/10.1111/sode.12026.
Brown, C. L., Van Doren, N., Ford, B. Q., Mauss, I. B., Sze, J. W., & Levenson, R. W. (2020). Coherence between subjective experience and physiology in emotion: Individual differences and implications for well-being. Emotion, 20(5), 818–829. https://doi.org/10.1037/emo0000579.
Brown, S., Fite, P. J., Stone, K., & Bortolato, M. (2016). Accounting for the associations between child maltreatment and internalizing problems: The role of alexithymia. Child Abuse & Neglect, 52, 20–28. https://doi.org/10.1016/j.chiabu.2015.12.008.
Cohen, L. H., Gunthert, K. C., Butler, A. C., O’Neill, S. C., & Tolpin, L. H. (2005). Daily Affective Reactivity as a Prospective Predictor of Depressive Symptoms. Journal of Personality, 73(6), 1687–1714. https://doi.org/10.1111/j.0022-3506.2005.00363.x.
Comrey, A. L., & Lee, H. B. (1992). Interpretation and Application of Factor Analytic Results. In A. L. Comrey (Ed.), A First Course in Factor Analysis (p. 2). Hillsdale: Lawrence Eribaum Associates.
Crosswell, A. D., Moreno, P. I., Raposa, E. B., Motivala, S. J., Stanton, A. L., Ganz, P. A., & Bower, J. E. (2017). Effects of mindfulness training on emotional and physiologic recovery from induced negative affect. Psychoneuroendocrinology, 86, 78–86. https://doi.org/10.1016/j.psyneuen.2017.08.003.
Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348–362. https://doi.org/10.1037/0022-3514.85.2.348.
Dale, L. P., Shaikh, S. K., Fasciano, L. C., Watorek, V. D., Heilman, K. J., & Porges, S. W. (2018). College females with maltreatment histories have atypical autonomic regulation and poor psychological wellbeing. Psychological Trauma: Theory, Research, Practice, and Policy, 10(4), 427–434. https://doi.org/10.1037/tra0000342.
Dan-Glauser, E. S., & Gross, J. J. (2013). Emotion regulation and emotion coherence: Evidence for strategy-specific effects. Emotion, 13(5), 832–842. https://doi.org/10.1037/a0032672.
Diener, E., Lucas, R. E., & Scollon, C. N. (2009). Beyond the hedonic treadmill: Revising the adaptation theory of well-being. In E. Diener (Ed.), The science of well-being (Vol. 37, pp. 103–118). Springer Netherlands. https://doi.org/10.1007/978-90-481-2350-6_5.
Duprey, E. B., Oshri, A., & Liu, S. (2019). Childhood maltreatment, self-esteem, and suicidal ideation in a low-SES emerging adult sample: The moderating role of heart rate variability. Archives of Suicide Research, 23(2), 333–352. https://doi.org/10.1080/13811118.2018.1430640.
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/S0749-3797(98)00017-8.
Ginzburg, K., Tsur, N., Barak-Nahum, A., & Defrin, R. (2014). Body awareness: Differentiating between sensitivity to and monitoring of bodily signals. Journal of Behavioral Medicine, 37(3), 564–575. https://doi.org/10.1007/s10865-013-9514-9.
Goessl, V. C., Curtiss, J. E., & Hofmann, S. G. (2017). The effect of heart rate variability biofeedback training on stress and anxiety: A meta-analysis. Psychological Medicine, 47(15), 2578–2586. https://doi.org/10.1017/S0033291717001003.
Graham, R. A., Scott, B. G., & Weems, C. F. (2017). Parenting behaviors, parent heart rate variability, and their associations with adolescent heart rate variability. Journal of Youth and Adolescence, 46(5), 1089–1103. https://doi.org/10.1007/s10964-016-0616-x.
Gratz, K. L., Bornovalova, M. A., Delany-Brumsey, A., Nick, B., & Lejuez, C. W. (2007). A laboratory-based study of the relationship between childhood abuse and experiential avoidance among inner-city substance users: The role of emotional nonacceptance. Behavior Therapy, 38(3), 256–268. https://doi.org/10.1016/j.beth.2006.08.006.
Grimm, K. J., Ram, N., & Hamagami, F. (2011). Nonlinear growth curves in developmental research: Nonlinear growth. Child Development, 82(5), 1357–1371. https://doi.org/10.1111/j.1467-8624.2011.01630.x.
Gunnar, M. R., & Donzella, B. (2002). Social regulation of the cortisol levels in early human development. Psychoneuroendocrinology, 27(1–2), 199–220. https://doi.org/10.1016/S0306-4530(01)00045-2.
Hagan, M. J., Bush, N., Mendes, W. B., Arenander, J., Epel, E., & Puterman, E. (2017). Associations between childhood adversity and daily suppression and avoidance in response to stress in adulthood: Can neurobiological sensitivity help explain this relationship? Anxiety, Stress, & Coping, 30(2), 163–175. https://doi.org/10.1080/10615806.2016.1259473.
Hardt, J., & Rutter, M. (2004). Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry, 45(2), 260–273. https://doi.org/10.1111/j.1469-7610.2004.00218.x.
Hayes, S. C. (2004). Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behavior Therapy, 35(4), 639–665. https://doi.org/10.1016/S0005-7894(04)80013-3.
Holzman, J. B., & Bridgett, D. J. (2017). Heart rate variability indices as bio-markers of top-down self-regulatory mechanisms: A meta-analytic review. Neuroscience & Biobehavioral Reviews, 74, 233–255. https://doi.org/10.1016/j.neubiorev.2016.12.032.
Imai, K., Sato, H., Hori, M., Kusuoka, H., Ozaki, H., Yokoyama, H., Takeda, H., Inoue, M., & Kamada, T. (1994). Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. Journal of the American College of Cardiology, 24(6), 1529–1535. https://doi.org/10.1016/0735-1097(94)90150-3.
Jennings, J. R., Kamarck, T., Stewart, C., Eddy, M., & Johnson, P. (1992). Alternate cardiovascular baseline assessment techniques: Vanilla or resting baseline. Psychophysiology, 29(6), 742–750. https://doi.org/10.1111/j.1469-8986.1992.tb02052.x.
Johnson, M., Deardorff, J., Davis, E. L., Martinez, W., Eskenazi, B., & Alkon, A. (2017). The relationship between maternal responsivity, socioeconomic status, and resting autonomic nervous system functioning in Mexican American children. International Journal of Psychophysiology, 116, 45–52. https://doi.org/10.1016/j.ijpsycho.2017.02.010.
Kashdan, T. B., & Rottenberg, J. (2010). Psychological flexibility as a fundamental aspect of health. Clinical Psychology Review, 30(7), 865–878. https://doi.org/10.1016/j.cpr.2010.03.001.
Kelly, A. S., Rudser, K. D., Dengel, D. R., Kaufman, C. L., Reiff, M. I., Norris, A. L., Metzig, A. M., & Steinberger, J. (2014). Cardiac autonomic dysfunction and arterial stiffness among children and adolescents with attention deficit hyperactivity disorder treated with stimulants. The Journal of Pediatrics, 165(4), 755–759. https://doi.org/10.1016/j.jpeds.2014.05.043.
Kirschbaum, C., Pirke, K.-M., & Hellhammer, D. H. (1993). The ‘Trier Social Stress Test’—A tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology, 28(1–2), 76–81. https://doi.org/10.1159/000119004.
Kogan, A., Gruber, J., Shallcross, A. J., Ford, B. Q., & Mauss, I. B. (2013). Too much of a good thing? Cardiac vagal tone’s nonlinear relationship with well-being. Emotion, 13(4), 599–604. https://doi.org/10.1037/a0032725.
Kok, B. E., & Fredrickson, B. L. (2010). Upward spirals of the heart: Autonomic flexibility, as indexed by vagal tone, reciprocally and prospectively predicts positive emotions and social connectedness. Biological Psychology, 85(3), 432–436. https://doi.org/10.1016/j.biopsycho.2010.09.005.
Kross, E., & Ayduk, O. (2008). Facilitating adaptive emotional analysis: Distinguishing distanced-analysis of depressive experiences from immersed-analysis and distraction. Personality and Social Psychology Bulletin, 34(7), 924–938. https://doi.org/10.1177/0146167208315938.
Laborde, S., Mosley, E., & Thayer, J. F. (2017). Heart rate variability and cardiac vagal tone in psychophysiological research—Recommendations for experiment planning, data analysis, and data reporting. Frontiers in Psychology, 08. https://doi.org/10.3389/fpsyg.2017.00213.
Lazarus, R. S. (1991). Emotion and adaptation. New York: Oxford University Press.
Lindsay, E. K., Young, S., Smyth, J. M., Brown, K. W., & Creswell, J. D. (2018). Acceptance lowers stress reactivity: Dismantling mindfulness training in a randomized controlled trial. Psychoneuroendocrinology, 87, 63–73. https://doi.org/10.1016/j.psyneuen.2017.09.015.
Luhmann, M., Hofmann, W., Eid, M., & Lucas, R. E. (2012). Subjective well-being and adaptation to life events: A meta-analysis. Journal of Personality and Social Psychology, 102(3), 592–615. https://doi.org/10.1037/a0025948.
Marsland, A. L., Gianaros, P. J., Prather, A. A., Jennings, J. R., Neumann, S. A., & Manuck, S. B. (2007). Stimulated Production of Proinflammatory Cytokines Covaries Inversely With Heart Rate Variability. Psychosomatic Medicine, 69(8), 709–716. https://doi.org/10.1097/PSY.0b013e3181576118.
Matti, J., Luutonen, S., Reventlow, H. V., Patterson, P., Karlsson, H., & Salokangas, R. K. R. (2008). Alexithymia and childhood abuse among patients attending primary and psychiatric care: Results of the RADEP study. Psychosomatics, 49(4), 317–325. https://doi.org/10.1176/appi.psy.49.4.317.
Mauss, I. B., Levenson, R. W., McCarter, L., Wilhelm, F. H., & Gross, J. J. (2005). The tie that binds? Coherence among emotion experience, behavior, and physiology. Emotion, 5(2), 175–190. https://doi.org/10.1037/1528-3542.5.2.175.
McLaughlin, K. A., & Nolen-Hoeksema, S. (2011). Rumination as a transdiagnostic factor in depression and anxiety. Behaviour Research and Therapy, 49(3), 186–193. https://doi.org/10.1016/j.brat.2010.12.006.
Mehling, W. E., Gopisetty, V., Daubenmier, J., Price, C. J., Hecht, F. M., & Stewart, A. (2009). Body awareness: Construct and self-report measures. PLoS One, 4(5), e5614. https://doi.org/10.1371/journal.pone.0005614.
Morrill, M. I., Schulz, M. S., Nevarez, M. D., Preacher, K. J., & Waldinger, R. J. (2019). Assessing within- and between-family variations in an expanded measure of childhood adversity. Psychological Assessment, 31(5), 660–673. https://doi.org/10.1037/pas0000691.
Muthén, B., & Asparouhov, T. (2012). Bayesian structural equation modeling: A more flexible representation of substantive theory. Psychological Methods, 17(3), 313–335. https://doi.org/10.1037/a0026802.
Muthén, L. K., & Muthén, B. O. (1998-2017). Mplus User’s Guide (8th ed.). Los Angeles: Muthén & Muthén.
Peltola, M. A. (2012). Role of editing of R–R intervals in the analysis of heart rate variability. Frontiers in Physiology, 3. https://doi.org/10.3389/fphys.2012.00148.
Petrova, K., Nevarez, M.D., Waldinger, R.J., Preacher, K.J., & Schulz, M.S. (2021). Self-distancing and avoidance mediate the links between trait mindfulness and responses to emotional challenges. Mindfulness. https://doi.org/10.1007/s12671-020-01559-4.
Pierpont, G. L., Stolpman, D. R., & Gornick, C. C. (2000). Heart rate recovery post-exercise as an index of parasympathetic activity. Journal of the Autonomic Nervous System, 80(3), 169–174. https://doi.org/10.1016/S0165-1838(00)00090-4.
Preacher, K. J., & Selig, J. P. (2012). Advantages of Monte Carlo Confidence Intervals for Indirect Effects. Communication Methods and Measures, 6(2), 77–98. https://doi.org/10.1080/19312458.2012.679848.
Prenda, K. M., & Lachman, M. E. (2001). Planning for the future: A life management strategy for increasing control and life satisfaction in adulthood. Psychology and Aging, 16(2), 206–216. https://doi.org/10.1037/0882-7974.16.2.206.
Quintana, D. S., Alvares, G. A., & Heathers, J. A. J. (2016). Guidelines for reporting articles on psychiatry and heart rate variability (GRAPH): Recommendations to advance research communication. Translational Psychiatry, 6(5), e803–e803. https://doi.org/10.1038/tp.2016.73.
Repetti, R. L., Taylor, S. E., & Seeman, T. E. (2002). Risky families: Family social environments and the mental and physical health of offspring. Psychological Bulletin, 128(2), 330–366. https://doi.org/10.1037/0033-2909.128.2.330.
Scheines, R., Hoijtink, H., & Boomsma, A. (1999). Bayesian estimation and testing of structural equation models. Psychometrika, 64(1), 37–52. https://doi.org/10.1007/BF02294318.
Scott, B. G., & Weems, C. F. (2014). Resting vagal tone and vagal response to stress: Associations with anxiety, aggression, and perceived anxiety control among youths: Vagal tone, anxiety, and aggression. Psychophysiology, 51(8), 718–727. https://doi.org/10.1111/psyp.12218.
Selig, J. P., & Preacher, K. J. (2008). Monte Carlo method for assessing mediation: An interactive tool for creating confidence intervals for indirect effects [Computer software]. Retrieved from http://www.quantpsy.org/medmc/medmc.htm
Shapiro, S. L., Carlson, L. E., Astin, J. A., & Freedman, B. (2006). Mechanisms of mindfulness. Journal of Clinical Psychology, 62(3), 373–386. https://doi.org/10.1002/jclp.20237.
Sommerfeldt, S. L., Schaefer, S. M., Brauer, M., Ryff, C. D., & Davidson, R. J. (2019). Individual differences in the association between subjective stress and heart rate are related to psychological and physical well-being. Psychological Science, 30(7), 1016–1029. https://doi.org/10.1177/0956797619849555.
Steptoe, A., & Marmot, M. (2005). Impaired cardiovascular recovery following stress predicts 3-year increases in blood pressure. Journal of Hypertension, 23(3), 529–536. https://doi.org/10.1097/01.hjh.0000160208.66405.a8.
Sze, J. A., Gyurak, A., Yuan, J. W., & Levenson, R. W. (2010). Coherence between emotional experience and physiology: Does body awareness training have an impact? Emotion, 10(6), 803–814. https://doi.org/10.1037/a0020146.
Tamir, M., John, O. P., Srivastava, S., & Gross, J. J. (2007). Implicit theories of emotion: Affective and social outcomes across a major life transition. Journal of Personality and Social Psychology, 92(4), 731–744. https://doi.org/10.1037/0022-3514.92.4.731.
Tarvainen, M. P., Niskanen, J.-P., Lipponen, J. A., Ranta-aho, P. O., & Karjalainen, P. A. (2014). Kubios HRV—Heart rate variability analysis software. Computer Methods and Programs in Biomedicine, 113(1), 210–220. https://doi.org/10.1016/j.cmpb.2013.07.024.
Taylor, S. E., Lerner, J. S., Sage, R. M., Lehman, B. J., & Seeman, T. E. (2004). Early environment, emotions, responses to stress, and health. Journal of Personality, 72(6), 1365–1394. https://doi.org/10.1111/j.1467-6494.2004.00300.x.
Thayer, J. F., Hansen, A. L., Saus-Rose, E., & Johnsen, B. H. (2009). Heart rate variability, prefrontal neural function, and cognitive performance: The neurovisceral integration perspective on self-regulation, adaptation, and health. Annals of Behavioral Medicine, 37(2), 141–153. https://doi.org/10.1007/s12160-009-9101-z.
Weber, C. S., Thayer, J. F., Rudat, M., Wirtz, P. H., Zimmermann-Viehoff, F., Thomas, A., Perschel, F. H., Arck, P. C., & Deter, H. C. (2010). Low vagal tone is associated with impaired post stress recovery of cardiovascular, endocrine, and immune markers. European Journal of Applied Physiology, 109(2), 201–211. https://doi.org/10.1007/s00421-009-1341-x.
Willett, J. B. (1994). Measurement of Change. In T. Husen & T. N. Postlethwaite (Eds.), The International Encyclopedia of Education (2nd ed., pp. 671–678). Oxford: Pergamon Press.
Zuanetti, G., Latini, R., Neilson, J. M. M., Schwartz, P. J., & Ewing, D. J. (1991). Heart rate variability in patients with ventricular arrhythmias: Effect of antiarrhythmic drugs. Journal of the American College of Cardiology, 17(3), 604–612. https://doi.org/10.1016/S0735-1097(10)80172-X.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Acknowledgments
We would like to thank James Heathers, Ph.D., for his excellent contributions to our HRV data cleaning process and HRV artifact analysis.
Funding
This research was supported by the National Institute of Aging (R01AG045230).
Code Availability
All code that was used to carry out the primary analyses is available at: https://osf.io/jct46/.
Authors’ Contributions
All authors were involved in the conception, execution, and data collection/preparation. KP, MSS, and KJP conducted primary analyses. KP drafted the manuscript with assistance from MSS. All authors provided critical feedback and contributed to the final manuscript.
Data Availability
The language in the IRB-approved consent forms signed by participants does not allow the authors to make these data publicly available. However, covariance matrices and other statistics sufficient to replicate the main findings are available at: https://osf.io/jct46/.
Conflicts of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
The study was approved by Human Subjects Review committees at Massachusetts General Hospital (#2014P001116/MGH) and Bryn Mawr College (R15-002).
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Handling Editor: Peter J. Gianaros
Supplementary Information
ESM 1
(PDF 1543 kb)
Rights and permissions
About this article

Cite this article
Petrova, K., Nevarez, M.D., Rice, J. et al. Coherence Between Feelings and Heart Rate: Links to Early Adversity and Responses to Stress. Affec Sci 2, 1–13 (2021). https://doi.org/10.1007/s42761-020-00027-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42761-020-00027-5