In places without adequate health facilities, community health workers (CHWs) are employed by local governments to help families with health promotion activities. However, amidst the difficulties, mobile health applications (mHealth) are being increasingly developed in order to facilitate the work of the CHW. This work is a systematic review (SR) of the use of mHealth and the impact it has had so far in improving the health system and service delivery by the CHWs.
Method
This SR was based on the 27 PRISMA recommendations. We used the PICOS tool to specify the components of this review (eligibility criteria, keywords, etc.) and the StArt software to organize and control the articles exported from digital databases (PubMed, SciELO, etc.) from 2009 to 2019. The studies accepted for reading in their entirety underwent an analysis of their risk of bias, through the Cochrane risk of bias tool.
Results
The studies showed that mobile health intervention has a strong link with health care, mainly in the provision of community care services, maternal and child health care, sexual diseases, and infectious diseases, among others. This happens especially in rural or other areas of difficult access, such as countries in Africa, which occupies 61% of selected articles. However, it is believed that these applications have great potential and could help CHWs provide better disease prevention care.
Conclusion
The use of mHealth by CHWs has become typical in many regions of the world and is believed to have the potential to improve health service delivery in hard-to-reach or resource-limited settings.
Primary health care (PHC) has been highlighted as a health organization strategy that responds in an assertive and systematized way to the health needs of a region or population, besides enabling preventive and curative actions and guiding families and communities (Oliveira and Pereira 2013).
In this context, there are multidisciplinary teams composed of doctors, nurses, auxiliaries or technicians, and community health workers (WHO 1978). In the literature, the importance of the CHW is highlighted, due to the elevated level of information exchange about popular health, medical, and scientific knowledge between them and the community they serve. Usually, CHWs are people that belong to the community, and when hired by the municipality, they work in the same community in which they live. Another highlight of the PHC system is the health system improvement and the cost reduction due to the reduction in the number of doctors and nurses required (Buss 2000; Cipriano and Ferreira 2011; Duarte et al. 2007).
Despite their importance, CHWs do not need any specific academic qualification, and they are subject to the training or education carried out by the municipality (Nascimento and Correa 2008). Because of this, systemic barriers arise, such as lack of training and adequate supervision, which lead to the poor use of resources of the health unit and the poor quality of service rendered to the community. This lack of quality manifests as missing or incorrect data in data collection, duplication of work, difficulties in transmitting information to families and health teams, disorganized scheduling, or nonuse of the available mobile applications by CHWs (Duarte et al. 2007; Nascimento and Correa 2008; Wai and Carvalho 2009).Different instruments that use technology to support CHWs were found during the study, especially the mobile devices for data collection, education, visit scheduling, and health notifications. Some SRs about these technologies were found, which demonstrated the positive impacts on the community and the CHW, who were able to act outside the clinical setting, in remote areas or difficult-to-reach communities, making life easier for those patients who have difficulty attending hospitals (Aranda-Jan et al. 2014; Braun et al. 2013; Labrique et al. 2013; White et al. 2016).
However, these SRs do not mention risk study bias, leaving the quality of these mobile technologies and how much they represent in the daily work of the CHW in doubt. According to the PRISMA statement (Galvão et al. 2015), in items 12 and 15, it is recommended that the quality of these studies be assessed individually and/or together, specifying the method used and the results achieved.
In this SR, we chose the Cochrane Collaboration tool to assess the risk of study bias (Higgins et al. 2011; Sterne et al. 2016), the PICOS tool (Participants, Interventions, Comparators, Results, and Study Design) to support eligibility criteria and data extraction from studies (Santos et al. 2007), and the World Health Organization’s (WHO) “Digital Health Intervention Classification V.1.0” to categorize the technologies found. The systematic review protocol was published in the PROSPERO under record CRD42018085427.
The objective of this SR was to locate interventions made on community health workers in the literature, based on mHealth and the kind of benefits that were generated for these professionals in their community. Another objective of the review was to assess the quality of these mobile technologies and how they can improve planning in primary health care.
Method
The present study followed the 27 recommendations of the PRISMA statement, mainly the 5th item, which recommends the registration of the review protocol (Galvão et al. 2015) (see Appendix A). This protocol was registered under the number CRD42018085427 in PROSPERO (International Prospective Record of Systematic Reviews) and can be accessed at http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42018085427.
Search strategy and selecting studies
Systematic searches were performed on PUBMED, SCIELO, ESBCO, DOAJ, Periodic CAPES, ACM Digital Library, IEEE Xplore Digital Library, ScienceDirect (SD), Web of Science (WS), One File, Wiley, and Sage databases. The search was performed with the combination of categories, mobile health (mHealth), and CHW. The terms were mhealth apps, mobile internet, geo location apps, smartphone, cellular, community health workers, CHW, agent health, health promotion, family health, or prevention of diseases. No restrictions were imposed regarding language or publication date. The last search was performed on August 4, 2020.
The PICO tool (Santos et al. 2007) was used to specify the components related to the identified problem, that is, to define the eligibility criteria, search keywords, and variables for extraction and to structure the research question. How the PICO tool was used in this SR is provided below:
(P) Community health workers (CHW) or volunteer health worker (VHW) or community health advisors or agent (CHA)
(I) Mobile application native or web
(C) Other applications or no comparison
(O) Increased productivity to the health system, reduction of CHW performance errors, especially in data collection
After filling the PICO tool, it was possible to determine the main questions (Q) of this SR. Q1 – Can mobile applications increase and/or improve the health care professionals’ performance in your community? Q2 – Do the data obtained by these technologies allow better planning in the health area?
Eligibility criteria
The selection of the articles was based on the identification of the titles and abstracts of interest, defined in the PICOS tool. The selected articles were then filtered using the eligibility criteria:
Inclusion criteria: Only studies that were published in complete texts and publications of the last 10 years (2009–2019) and relating the variables defined in the PICO tool were included.
Exclusion criteria: Hypothetical models, books, systematic review, congress proceedings, theses, dissertation, and articles with incomplete text were excluded.
Data selection and extraction
This study included articles that mentioned the use of mobile devices by CHWs for improving health service quality, meaning any intervention using cell phones, personal digital assistants (PDA), smartphones, tablets, phablets, and hybrid laptops. The interventions that met the inclusion criteria were organized and categorized into two groups: (1) carried out by health workers or (2) involving communication between health services and the population. In each of the groups cited above, there are subcategories: group 1, education, diagnosis and management, communication and information gathering, and group 2, medical advice notices and medical examination results (see Appendix B).
Primary outcomes were defined as any measure that improved the delivery of health services. Secondary outcomes were defined as any measure related to the behavior of the health agent in the health care system. The results are important to distinguish the type of technique or usability questionnaire that was applied on the CHW and on the families during these interventions. The StArt v3.0.3 software was used in this study for the systematic review (Fabbri et al. 2010). The StArt software helps the construction of systematic reviews and meta-analysis in three phases:
1.
Planning – Determination of rules and characteristics of the review, i.e., eligibility criteria, PICO, researched databases, keywords, and data extraction fields, among others.
2.
Execution – There are three stages in the execution phase: The first stage was to identify the studies in the databases, that is, within the StArt, the search sessions were recreated to allow the import of the articles; the second stage dealt with the selection of these articles using the eligibility criteria; and the last stage performed the data extraction.
3.
Summarization – The extracted data were transformed into graphs and exported to the CSV format.
Firstly some extraction data were defined in the StArt including the type of study, the number of participants, target audience, region/country, health issue addressed, the type of device, the type of operating system, the form that this technology uses to communicate, the purpose of the technology, the interoperability involved, the tools used for development, if any usability testing had been done, whether it had been shared in open source tools, if the results offer any modification in the CHW routine, families, and/or health programs (see Appendix C).
The data extraction and evaluations were performed by a single rater and verified by an independent reviewer, who then met to discuss the findings. No divergences of opinion were found between the rater and the independent reviewer.
Data analyses
The experimental and nonexperimental studies that met the inclusion criteria underwent a careful individual evaluation of the methodological quality through the Cochrane RoB tool and Cochrane ROBINS-I (Higgins et al. 2011; Sterne et al. 2016). Each tool is divided into two parts, and they are composed of seven domains. For experimental studies, the following were evaluated: random sequence generation, allocation concealment, and blinding of participants and professionals. In nonexperimental studies, the following were evaluated: bias due to confounding and the bias in the selection of participants into the study. The bias in the measurement of interventions was evaluated as follows: bias due to departure from intended intervention, bias due to missing data, bias in the measurement of outcomes, and bias selection of reported results.
The first part of each tool refers to the description of what was reported in the evaluated study and needs to have enough details and information for a good judgment. The second part is the bias risk judgment for each of the domains analyzed, which can be classified into three categories in the Cochrane RoB tool (low risk of bias, high risk of bias, or risk of uncertain bias) and five categories in the ROBINS-I (low, moderate, severe, critical risk of bias, or no information to assess the risk of bias). For the judgment of each domain, a summary was made available by each Cochrane tool, which helps in the decision-making, making the judgment more transparent in all domains.
In this data analysis, a retrospective was conducted on the main tools related to the CHW, focusing on mobile technologies and how they could be used to improve performance, education, awareness, and access to data for the strengthening of health information systems. It was also considered how mHealth could support patient monitoring, clinical decision-making, and drug and supplies tracking. “Classification of Digital Intervention in Health V.1.0” of the World Health Organization (WHO 2018) was used to categorize the technologies that strengthen the health system.
Results
Characteristics of included studies
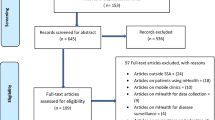
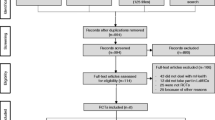
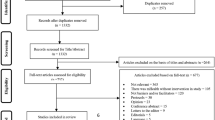
In six search sessions (from July 2019 to July 2020), we obtained 3255 documents: 1725 from PubMed, 335 from ScienceDirect, 325 from OneFile, and 870 from EBSCO, DOAJ, Scopus, and IEEE. These documents were exported to StArt for better control and definition of article status (accepted, rejected, or duplicated). There was a reduction to 2673 documents due to the publication date filter (2009–2019) and articles that were duplicates. Most studies were excluded because they were not based on mobile technologies for CHWs, either because they did not provide any description about the results achieved or because they were conference summaries. Only 582 articles passed the eligibility criteria through a complete reading. Finally, 62 articles were included in the SR. Figure 1 illustrates the stages of this systematic review and Table 1 the characteristics of included studies.
These 62 publications reported mobile health projects for CHW in 23 countries. A majority of the projects (52%) took place in developing countries, 38% were in underdeveloped countries, and 10% were in developed countries. It was observed that most of these projects were from Africa (61%), followed by the Americas (20%) and Asia (18%). Moreover, most of these projects were based in rural areas (76.2%), followed by urban/rural (14.3%) and urban (9.5%) areas. Figure 2 illustrates the number of publications by country.
The analysis revealed that the assessment related to CHWs and mobile health presented substantial variations in research design and methods used. Many studies used mixed methodologies (quantitative and qualitative analysis together), while others preferred to use only qualitative or quantitative results. A total of 36 studies were considered nonexperimental, because they demonstrated the validation of a mobile health technology or application without any evaluation of results or impacts. Moreover, 10 studies were considered quasi-experimental, because they presented a control group and compared the intervention based on mobile technology to a paper intervention but without randomization of the participants. Finally, 17 experimental studies were designed with a random selection of control and intervention groups. Table 2 illustrates the sample size and the intervention time for each study design.
The 36 nonexperimental studies presented a median sample size of 33 CHWs (min = 3, max = 432). The average intervention time was 160 days (min = 1, max = 1095).
The 10 quasi-experimental studies presented a median of 94.5 CHWs (min = 3, max = 474). The average intervention time was 122 days (min = 7, max = 547).
The 17 experimental studies presented a median of 124 CHWs (min = 3, max = 3775). The average intervention time was 243.5 days (min = 3, max = 1004).
The 62 studies presented a median of 42.5 CHWs (min = 3, max = 3775). The average intervention time was 160 days (min = 1, max = 1096).
Experimental and quasi-experimental studies were categorized and judged by the Cochrane RoB tool. Nonexperimental studies were categorized and judged using ROBINS-I. Appendix D shows the bias risk summary of RoB and ROBINS-I.
Fig. 3
Risk of bias for experimental and quasi-experimental studies
Figure 4 illustrates the percentage of study quality for nonexperimental studies.
Devices and technologies used to CHW
This review revealed that there is a great technological variety in the devices and systems used in CHW intervention in the last 10 years. The first appearance of mHealth for CHW was in 2010 by Haberer et al. The highest index of publications was in 2015 with 11 articles. In 2019, there were 5 articles with the same goal, with the last one being in September 2019 by Hackett et al.
All the studies unanimously aimed to improve the delivery of health services provided by CHWs using mHealth. However, in this study, considering that only the functions most used by them have been reported, it was decided to categorize them through the “Classification of Digital Intervention in Health V.1.0” of the WHO. Figure 5 illustrates this classification; 71% of the studies presented a health system challenge (HSC) related to the lack of access to information or data, 23% in communication obstacles, and 6% in healthcare provider’s poor adherence to clinical guidelines.
Fig. 5
Infographic “Classification of Digital Intervention in Health V.1.0” of the WHO
In 36 of the studies (58.1%), the projects were focused on a specific disease or treatment, mainly in the areas of maternal/child health care (24%), sexual diseases (11.3%), infectious diseases (8.1%), and others. In 26 of the studies (41.9%), health promotion and disease prevention stood out; that is, these surveys involved all health issues cited to inform professionals or collect population data.
Regarding the digital intervention in related health (DHI) used in the HSC, 71% of the studies presented some type of health management information system (HMIS) or electronic medical record, with the objective of “routine collection and management of health indicator data” or “storage and aggregation.” 23% used telemedicine to “provide prompts and alerts based according to protocol” or “communication and performance feedback to healthcare provider(s).” 6% used learning and training system to “learning and training system healthcare provider(s)” or “assess capacity of healthcare provider(s).” Figure 7 illustrates an infographic regarding the types of technologies or devices related to DHI in CHW
Fig. 7
Infographic regarding the types of technologies or devices related to DHI in CHW
In 60% of the studies, a basic cell phone (which only supports voice calls and/or text messages) was used, while the other 40% used some device with an operational system (Android, iOS, Windows, etc.).
In 37.7% of the studies, SMS/MMS technology was the most used on their devices to send and/or receive text, audio, or video messages. On the other hand, 23% of the studies featured a mobile app for Android smartphones. Finally, in 16.4% of the studies, the type of technology applied was not reported.
In 11.3% of the studies, the acceptability and feasibility questionnaire was used, which is provided in ISO/IEC 25010 (2011) and Nielsen’s ten heuristics (2013) to define essential characteristics in quality and usability in software and applications. In 3.2% of the studies, they mentioned the white and black box tests of software engineering, with the purpose of finding bugs and flaws before carrying out the intervention with CHW. Finally, 100% of the studies did not make the source code available on code versioning repositories (GitHub, Bitbucket, etc.), making them limited in terms of evolution or expansion of the study into other similar projects.
Discussions
This systematic review revealed that the number of mHealth assessments for CHW has increased in the past 6 years, mainly in rural or difficult to access areas, such as countries in Africa, which occupies 61% of selected studies.
Through WHO “Classification of Digital Health Intervention V.1.0,” it was possible to determine that 71% of the studies used a health management information system (HMIS) or electronic medical record to standardize data entry (Lozano-Fuentes et al. 2013; Schoen et al. 2017; Shishido et al. 2014) and allow real-time analysis of health problems in a community (Shishido et al. 2014), besides decreasing the loss of data for residents or patients. 23% used telemedicine to facilitate communication between CHW and their supervisors, providing medical advice or medical help support instantly (Chang et al. 2013; Chen et al. 2014; Mushamiri et al. 2015). Finally, 6% used the learning and training system to assess CHWs’ ability and reduce healthcare problems with low adherence by these professionals to clinical guidelines (Hoffman et al. 2010; Lim et al. 2011; Ramachandran et al. 2010).
In 58.1% of the studies, they justified their digital intervention through specific health problems related to a community or region, such as sexual, respiratory, infectious, cardiovascular, maternal and child diseases, and others. In 41.9%, they preferred to include all the diseases involved in health promotion and disease prevention to carry out the intervention.
The type of device and technology employed has shown a great variety and evolution in the last 10 years (2009–2019). In 60% of the studies, they used a basic cell phone to send simple text messages and SMS reminders in order to notify CHW of family visits, healthy behaviors and/or vaccination in health posts. 40% adhered to smartphones (36%) or tablets (4%) to create native applications on the Android, iOS, and Windows mobile system or web applications for the purpose of collecting health data or for CHW to communicate in real time (P2P) with supervisors or patients via wireless network or mobile networks (3G/4G). The reason for the great use of these basic phones with SMS technology is due to the type of technology available at that time, i.e., many of them occurred from 2010 until 2016, and the rise in the use of smartphones and Tablets in the world market began in 2014. In 2015, the first applications for CHW on Android smartphones appeared. Already in 2019, the use of basic cell phones with SMS was becoming obsolete, and the choice of smartphones was more frequent among studies.
The selected articles presented a great level of heterogeneity in the design and type of study. Approximately 56.4% adopted a nonexperimental model with qualitative results to evaluate mHealth’s performance in solving health problems in that region or community, a median sample of 40 CHW, and a median intervention period of 160 days. 43.6% quasi-experimental or experimental results were defined with qualitative and quantitative results to compare the efficiency of those who use the smartphone with an application with those who use the printed form and pen, through two groups (experimental group and control group) with median samples of 50 CHW for quasi-experimental studies and 124 CHW for experimental studies. The median intervention times were, respectively, 122 days and 160 days. Through Cochrane’s RoB and ROBINS-I tools, 47 out of 62 studies were classified with low bias risk.
Through this systematic review, it was possible to eliminate the existing doubt regarding the improvement of the performance of health professionals who use mobile applications. Studies show unanimously that using mHealth on smartphones has made CHWs more efficient and effective in their data collection services for patients and individuals in communities.
Such results corroborate with previous reviews (International Organization for Standardization 2011; Nielsen and Budiu 2013); however, this new review brought a more in-depth analysis on this topic, mainly through the use of the Cochrane Collaboration tool to assess the risk of study bias (Higgins et al. 2011; Sterne et al. 2016), which reduces the possibility of risk of bias. Of the experimental studies, 88% were considered representative and had a low risk of bias. In addition, the use of the WHO “Classification of Digital Intervention in Health V.1.0” (WHO 2018) classified 71% of the studies as “management information in health system” with the purpose of analyzing in real time the data captured by the CHWs of that community or region to make the best decision or solution on disease prevention and health promotion problems. Finally, 11.3% of the studies used the acceptability and feasibility questionnaire to ascertain the level of satisfaction of CHW in relation to the use of mHealth. The application of this questionnaire is foreseen in ISO/IEC 25010 (2011) and Nielsen’s ten usability heuristics (2013) and is considered essential to reach the level of quality in the usability of software and applications. Therefore, the use of these tools in the study emphasizes quality and reaffirms the use of mHealth in the daily lives of CHWs.
It cannot be said for certain whether the data obtained by these technologies allow better planning in primary health care, due to the variability of studies and technologies used over the past 10 years, for example, the PDA that has become obsolete. Therefore, it was observed that at the beginning of the implementation of these studies or applications, that is, from 2010 to 2013, numerous technological and infrastructure challenges, such as poor access to the telephone network, unavailability of the electrical network, and the lack of cell phones to CHWs were very mentioned in the studies (Florez-Arango et al. 2011; Hoffman et al. 2010; Zurovac et al. 2011) and reviews (Gurman et al. 2012; Marcolino et al. 2018; Stephani et al. 2016). However, it is noticeable that the scenario about these problems has been decreasing in recent years, mainly in the evolution of cell phones to smartphones and the expansion of mobile Internet (Hackett et al. 2019; Schaeffer et al. 2019).
Finally, more studies are still needed to make decisions on primary healthcare planning to be effective and efficient, as most samples showed very limited variability in health data and sample size interviewed by CHW. For this, it is necessary that new studies begin to use the resources available in cloud computing to achieve these characteristics, because through it, it is possible to have a great variety, speed, truthfulness, value, and volume on the data captured.
Limitations
Our review was limited by the scope of our literature search, which included articles in English through indexed digital databases and removed those that were part of conferences and/or collections of monographs, dissertations, and theses. It was noted that most projects are focused on developing mHealth to improve health promotion and that CHW are well connected to these technological projects. However, the scientific gains of these projects were difficult to evaluate, especially in the nonexperimental studies. However, the positive results are almost unanimous, making the negative results less likely to be published. In addition, due to the heterogeneity of methods, it was not possible to make a meta-analysis.
Conclusion
Given the results, we can conclude that the use of mHealth by CHWs has become typical in many regions of the world. In fact, many of these projects showed similarities in their purpose, especially regarding the effectiveness of CHWs in health systems. The health sector has been most successful in smartphone data collection activities in rural areas of developing and underdeveloped countries, particularly in Africa. However, it is believed that upcoming research should include or emphasize software engineering techniques or better qualitative analysis, to understand how these tools can be designed or even replicated in countries that do not use this technology. Similarly, the exploration of usability tests for experimental studies, which would allow a better evaluation of the impact of these studies, would increase or improve the evidence base in this area. Ultimately, it is believed that these mobile applications have the potential to improve the delivery of health services in hard-to-reach or resource-constrained environments and that new projects will strengthen and guide the area of health-focused public policy.
References
Andreatta P, Debpuur D, Danquah A, Perosky J. Using cell phones to collect postpartum hemorrhage outcome data in rural Ghana. Int J Gynecol Obstet. 2011;113(2):148–51.
Aranda-Jan CB, Mohutsiwa-Dibe N, Loukanova S. Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health BioMed Central. 2014;14(1):188.
Bastawrous A, Rono H, Livingstone IAT, Weiss HA, Jordan S, Kuper H, et al. The development and validation of a smartphone visual acuity test (peek acuity) for clinical practice and community-based fieldwork. JAMA Ophthalmol. 2015;133(8):930–7.
Biemba G, Chiluba B, Yeboah-Antwi K, Silavwe V, Lunze K, Mwale RK, et al. A mobile-based community health management information system for community health workers and their supervisors in 2 districts of Zambia. Glob Heal Sci Pract. 2017;5(3):486–94.
Birur N, Gurushanth K, Patrick S, Sunny S, Raghavan S, Gurudath S, et al. Role of community health worker in a mobile health program for early detection of oral cancer. Indian J Cancer Wolters Kluwer Medknow Publications. 2019;56(2):107–13.
Bonnell S, Griggs A, Avila G, Mack J, Bush RA, Vignato J, et al. Community health workers and use of mHealth: improving identification of pregnancy complications and access to care in the Dominican Republic. Health Promot Pract United States. 2018;19(3):331–40.
Braun R, Catalani C, Wimbush J, Israelski D. Community health workers and mobile technology: a systematic review of the literature. PLoS One Public Library of Science. 2013;8(6):e65772.
Braun R, Lasway C, Agarwal S, L’Engle K, Layer E, Silas L, et al. An evaluation of a family planning mobile job aid for community health workers in Tanzania. Contraception United States. 2016;94(1):27–33.
Campbell N, Schiffer E, Buxbaum A, McLean E, Perry C, Sullivan TM. Taking knowledge for health the extra mile: participatory evaluation of a mobile phone intervention for community health workers in Malawi. Glob Heal Sci Pract. 2014;2(1):23–34.
Chang LW, Kagaayi J, Arem H, Nakigozi G, Ssempijja V, Serwadda D, et al. Impact of a mHealth intervention for peer health workers on AIDS care in rural Uganda: a mixed methods evaluation of a cluster-randomized trial. AIDS Behav. 2011;15(8):1776–84.
Chang LW, Njie-Carr V, Kalenge S, Kelly JF, Bollinger RC, Alamo-Talisuna S. Perceptions and acceptability of mHealth interventions for improving patient care at a community-based HIV/AIDS clinic in Uganda: a mixed methods study. AIDS Care. 2013;25(7):874–80.
Chen Y, Yang K, Jing T, Tian J, Shen X, Xie C, et al. Use of text messages to communicate clinical recommendations to health workers in rural China: a cluster-randomized trial. Bull World Health Organ. SciELO Public Health. 2014;92:474–81.
Cherrington AL, Agne AA, Lampkin Y, Birl A, Shelton TC, Guzman A, et al. Diabetes connect: developing a mobile health intervention to link diabetes community health workers with primary care. J Ambul Care Manage United States. 2015;38(4):333–45.
Cipriano FG, Ferreira LP. Queixas de voz em agentes comunitários de saúde: correlação entre problemas gerais de saúde, hábitos de Vida e aspectos vocais TT - voice complaints in community health agents: correlation between general health problems, lifestyle habits and vocal aspec. Rev Soc Bras Fonoaudiol. 2011;16(2):132–9.
Duarte LR, Silva DSJR d, Cardoso SH. Construindo um programa de educação com agentes comunitários de saúde. Interface - Comun Saúde, Educ. 2007;11(23):439–47.
Fabbri S, Ferrari F, Vincenzi AMR, Di Thommazo A. State of the Art through Systematic Review (StArt). Versão 3.0.3 [software]. Laboratório de pesquisa em Engenharia de Software da Universidade Federal de São Carlos [Internet]. Versão 3.0.3; 2010 [cited 2018 Mar 10]. Available from: http://lapes.dc.ufscar.br/tools/start_tool
Florez-Arango JF, Iyengar MS, Dunn K, Zhang J. Performance factors of mobile rich media job aids for community health workers. J Am Med Inform Assoc BMA House, Tavistock Square, London, WC1H 9JR: BMJ Group. 2011;18(2):131–7.
Fotso JC, Bellhouse L, Vesel L, Jezman Z. Strengthening the home-to-facility continuum of newborn and child health care through mHealth: evidence from an intervention in rural Malawi. Etude la Popul Africaine African Population Studies. 2015;29(1):1663.
Galvão TF, Pansani T d SA, Harrad D. Principais itens para relatar Revisões sistemáticas e meta-análises: a recomendação PRISMA. Epidemiol e Serviços Saúde. SciELO Public Health. 2015;24:335–42.
Gatuha G, Jiang T. KenVACS: Improving Vaccination of children through cellular network technology in developing countries.(Report). Interdiscip J Inf Knowl Manag. 2015;10:37.
Ginsburg OM, Chowdhury M, Wu W, Chowdhury MTI, Pal BC, Hasan R, et al. An mHealth model to increase clinic attendance for breast symptoms in rural Bangladesh: can bridging the digital divide help close the cancer divide? Oncologist Alphamed Press. 2014;19(2):177–85.
Gisore P, Shipala E, Otieno K, Rono B, Marete I, Tenge C, et al. Community based weighing of newborns and use of mobile phones by village elders in rural settings in Kenya: a decentralised approach to health care provision. BMC Pregnancy Childbirth BioMed Central. 2012;12(1):15.
Gurman TA, Rubin SE, Roess AA. Effectiveness of mHealth behavior change communication interventions in developing countries: a systematic review of the literature. J Health Commun. 2012;17:82–104.
Haberer JE, Kiwanuka J, Nansera D, Wilson IB, Bangsberg DR. Challenges in using mobile phones for collection of antiretroviral therapy adherence data in a resource-limited setting. AIDS Behav. 2010;14(6):1294–301.
Hackett K, Kazemi M, Lafleur C, Nyella P, Godfrey L, Sellen D. It makes you someone who changes with the times’: health worker and client perspectives on a smartphone-based counselling application deployed in rural Tanzania. Health Policy Plan Oxford University Press. 2019;34(4):307–15.
Hamainza B, Killeen GF, Kamuliwo M, Bennett A, Yukich JO. Comparison of a mobile phone-based malaria reporting system with source participant register data for capturing spatial and temporal trends in epidemiological indicators of malaria transmission collected by community health workers in rural Zambia. Malar J BioMed Central. 2014;13(1):489.
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. British Medical Journal Publishing Group. 2011;343:d5928.
Hoffman JA, Cunningham JR, Suleh AJ, Sundsmo A, Dekker D, Vago F, et al. Mobile direct observation treatment for tuberculosis patients. Am J Prev Med Elsevier. 2010;39(1):78–80.
Ilozumba O, Dieleman M, Kraamwinkel N, Van Belle S, Chaudoury M, Broerse JEW. “I am not telling. The mobile is telling”: factors influencing the outcomes of a community health worker mHealth intervention in India. PLoS One United States. 2018;13(3):e0194927.
International Organization for Standardization. ISO/IEC 25010–2011. systems and software engineering - Systems and software Quality Requirements and Evaluation (SQuaRE) - System and software quality models. 2011.
Jennings L, Ong’ech J, Simiyu R, Sirengo M, Kassaye S. Exploring the use of mobile phone technology for the enhancement of the prevention of mother-to-child transmission of HIV program in Nyanza, Kenya: a qualitative study. BMC Public Health BioMed Central. 2013;13(1):1131.
Jones COH, Wasunna B, Sudoi R, Githinji S, Snow RW, Zurovac D. “Even if you know everything you can forget”: health worker perceptions of mobile phone text-messaging to improve malaria case-management in Kenya. Shiff C, editor. PLoS One. San Francisco, USA: Public Library of Science. 2012;7(6):e38636.
Joos O, Silva R, Amouzou A, Moulton LH, Perin J, Bryce J, et al. Evaluation of a mHealth data quality intervention to improve documentation of pregnancy outcomes by health surveillance assistants in Malawi: a cluster randomized trial. PLoS One. Public Library of Science. 2016;11(1):e0145238.
Kabakyenga J, Barigye C, Brenner J, Maling S, Buchner D, Nettle-Aquirre A, et al. A demonstration of mobile phone deployment to support the treatment of acutely ill children under five in Bushenyi district, Uganda. Afr Health Sci. Makerere University Medical School (Uganda). 2016;16(1):89–96.
Kallander K, Strachan D, Soremekun S, Hill Z, Lingam R, Tibenderana J, et al. Evaluating the effect of innovative motivation and supervision approaches on community health worker performance and retention in Uganda and Mozambique: study protocol for a randomised controlled trial. Trials England. 2015;16:157.
Kaphle S, Chaturvedi S, Chaudhuri I, Krishnan R, Lesh N. Adoption and usage of mHealth technology on quality and experience of care provided by frontline workers: observations from rural India. JMIR mHealth uHealth. 2015;3(2):e61.
Labrique AB, Vasudevan L, Kochi E, Fabricant R, Mehl G. mHealth innovations as health system strengthening tools: 12 common applications and a visual framework. Glob Heal Sci Pract. 2013;1(2):160–71.
Laktabai J, Platt A, Menya D, Turner EL, Aswa D, Kinoti S, et al. A mobile health technology platform for quality assurance and quality improvement of malaria diagnosis by community health workers. PLoS One United States. 2018;13(2):e0191968.
Lim S, Xue L, Yen CC, Chang L, Chan HC, Tai BC, et al. A study on Singaporean women’s acceptance of using mobile phones to seek health information. Int J Med Inform Elsevier. 2011;80(12):e189–202.
Lozano-Fuentes S, Wedyan F, Hernandez-Garcia E, Sadhu D, Ghosh S, Bieman JM, et al. Cell phone-based system (Chaak) for surveillance of immatures of dengue virus mosquito vectors. J Med Entomol. Oxford University press Oxford, UK. 2013;50(4):879–89.
Maleka BK, Van Der Linde J, Glascoe FP, Swanepoel DW. Developmental screening—evaluation of an m-health version of the parents evaluation developmental status tools. Telemed e-Health. Mary Ann Liebert, Inc. 140 Huguenot Street, 3rd Floor New Rochelle, NY 10801 USA. 2016;22(12):1013–8.
Mannik J, Figol A, Churchill V, Aw J, Francis S, Karino E, et al. Community-based screening for cardiovascular risk using a novel mHealth tool in rural Kenya. J Innov Heal informatics England. 2018;25(3):176–82.
Marcolino MS, Oliveira JAQ, D’Agostino M, Ribeiro AL, Alkmim MBM, Novillo-Ortiz D. The impact of mHealth interventions: systematic review of systematic reviews. JMIR mHealth uHealth. JMIR Publications. 2018:e23.
Mc Kenna P, Babughirana G, Amponsah M, Egoeh SG, Banura E, Kanwagi R, et al. Mobile training and support (MOTS) service—using technology to increase ebola preparedness of remotely-located community health workers (CHWs) in Sierra Leone. mHealth. AME Publishing Company. 2019;5:35–5.
Medhanyie AA, Moser A, Spigt M, Yebyo H, Little A, Dinant G, et al. Mobile health data collection at primary health care in Ethiopia: a feasible challenge. J Clin Epidemiol. 2015;68(1):80–6.
Meyers DJ, Ozonoff A, Baruwal A, Pande S, Harsha A, Sharma R, et al. Combining healthcare-based and participatory approaches to surveillance: trends in diarrheal and respiratory conditions collected by a mobile phone system by community health workers in rural Nepal. PLoS One Public Library of Science. 2016;11(4):e0152738.
Modi D, Gopalan R, Shah S, Venkatraman S, Desai G, Desai S, et al. Development and formative evaluation of an innovative mHealth intervention for improving coverage of community-based maternal, newborn and child health services in rural areas of India. Glob Health Action Taylor & Francis. 2015;8(1):26769.
Musabyimana A, Ruton H, Gaju E, Berhe A, Grepin KA, Ngenzi J, et al. Assessing the perspectives of users and beneficiaries of a community health worker mHealth tracking system for mothers and children in Rwanda. PLoS One United States. 2018;13(6):e0198725.
Mushamiri I, Luo C, Iiams-Hauser C, Amor YB. Evaluation of the impact of a mobile health system on adherence to antenatal and postnatal care and prevention of mother-to-child transmission of HIV programs in Kenya. BMC Public Health. BioMed Central. 2015;15(1):102.
Neupane S, Odendaal W, Friedman I, Jassat W, Schneider H, Doherty T. Comparing a paper based monitoring and evaluation system to a mHealth system to support the national community health worker programme, South Africa: an evaluation. BMC Med Inform Decis Mak BioMed Central Ltd. 2014;14(1):69.
Ngabo F, Nguimfack J, Nwaigwe F, Mugeni C, Muhoza D, Wilson DR, et al. Designing and implementing an innovative SMS-based alert system (RapidSMS-MCH) to monitor pregnancy and reduce maternal and child deaths in Rwanda. Pan Afr Med J African Field Epidemiology Network. 2012:13.
Nielsen J, Budiu R. Usabilidade móvel. São Paulo: Elsevier; 2013.
O’Donovan J, Kabali K, Taylor C, Chukhina M, Kading JC, Fuld J, et al. The use of low-cost android tablets to train community health workers in Mukono, Uganda, in the recognition, treatment and prevention of pneumonia in children under five: a pilot randomised controlled trial. Hum Resour Health England. 2018;16(1):49.
Oliveira MA d C, Pereira IC. Atributos essenciais da atenção primária e a estratégia saúde da família. Rev Bras Enferm. 2013;66(spe):158–64.
Palazuelos D, Diallo AB, Palazuelos L, Carlile N, Payne JD, Franke MF. User perceptions of an mHealth medicine dosing tool for community health workers. JMIR mHealth uHealth. 2013;1(1):e2.
Rajan JV, Moura J, Gourley G, Kiso K, Sizilio A, Cortez AM, et al. Understanding the barriers to successful adoption and use of a mobile health information system in a community health center in São Paulo, Brazil: a cohort study. BMC Med Inform Decis Mak. 2016;16.
Rajput ZA, Mbugua S, Amadi D, Chepnǵeno V, Saleem JJ, Anokwa Y, et al. Evaluation of an Android-based mHealth system for population surveillance in developing countries. J Am Med Inform Assoc BMA House, Tavistock Square, London, WC1H 9JR: BMJ Group. 2012;19(4):655–9.
Ramachandran D, Goswami V, Canny J. Research and reality : using mobile messages to promote maternal health in rural India. Proc 4th ACM/IEEE Int Conf Inf Commun Technol Dev. 2010;35.
Ramirez M, Wu S, Ryan G, Towfighi A, Vickrey BG. Using beta-version mhealth technology for team-based care management to support stroke prevention: an assessment of utility and challenges. JMIR Res Protoc Canada. 2017;6(5):e94.
Rotheram-Borus M-J, Richter L, Van Rooyen H, van Heerden A, Tomlinson M, Stein A, et al. Project Masihambisane: a cluster randomised controlled trial with peer mentors to improve outcomes for pregnant mothers living with HIV. Trials. 2011;12(1):2.
Sa JHG, Rebelo MS, Brentani A, Grisi SJFE, Iwaya LH, Simplicio MA Jr, et al. Georeferenced and secure mobile health system for large scale data collection in primary care. Int J Med Inform. Elsevier. 2016;94:91–9.
Santos CM d C, Pimenta CA d M, Nobre MRC. The PICO strategy for the research question construction and evidence search. Rev Lat Am Enfermagem. 2007;15(3):508–11.
Schaeffer LE, Ahmed S, Rahman M, Whelan R, Rahman S, Roy AD, et al. Development and evaluation of a mobile application for case management of small and sick newborns in Bangladesh. BMC Med Inform Decis Mak. BioMed Central Ltd. 2019;19(1):116.
Schoen J, Mallett JW, Grossman-Kahn R, Brentani A, Kaselitz E, Heisler M. Perspectives and experiences of community health workers in Brazilian primary care centers using m-health tools in home visits with community members. Hum Resour Health London: BioMed Central. 2017;15:71.
Schoenberger Y-M, Phillips J, Mohiuddin MO, McNees P, Scarinci I. Acceptability of delivering and accessing health information through text messaging among community health advisors. JMIR mHealth uHealth. JMIR Publications Inc. 2013;1(2).
Schuttner L, Sindano N, Theis M, Zue C, Joseph J, Chilengi R, et al. A mobile phone-based, community health worker program for referral, follow-up, and service outreach in rural Zambia: outcomes and overview. Telemed e-HEALTH Mary Ann Liebert, Inc. 140 Huguenot Street, 3rd Floor New Rochelle, NY 10801 USA. 2014;20(8):721–8.
Shishido HY, Andrade RA d C, Eler GJ. mHealth data collector: an application to collect and report indicators for assessment of cardiometabolic risk. Nurs Informatics. 2014:425–32.
Sonderman KA, Nkurunziza T, Kateera F, Gruendl M, Koch R, Gaju E, et al. Using mobile health technology and community health workers to identify and refer caesarean-related surgical site infections in rural Rwanda: a randomised controlled trial protocol. BMJ Open England. 2018;8(5):e022214.
Stanton MC, Mkwanda SZ, Debrah AY, Batsa L, Biritwum N-K, Hoerauf A, et al. Developing a community-led SMS reporting tool for the rapid assessment of lymphatic filariasis morbidity burden: case studies from Malawi and Ghana. BMC Infect Dis BioMed Central. 2015;15(1):214.
Stephani V, Opoku D, Quentin W. A systematic review of randomized controlled trials of mHealth interventions against non-communicable diseases in developing countries. BMC Public Health. BioMed Central Ltd. 2016:572.
Sterne JAC, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. bmj British Medical Journal Publishing Group. 2016;355:i4919.
Surka S, Edirippulige S, Steyn K, Gaziano T, Puoane T, Levitt N. Evaluating the use of mobile phone technology to enhance cardiovascular disease screening by community health workers. Int J Med Inform Elsevier. 2014;83(9):648–54.
Tumusiime DK, Agaba G, Kyomuhangi T, Finch J, Kabakyenga J, MacLeod S. Introduction of mobile phones for use by volunteer community health workers in support of integrated community case management in Bushenyi District, Uganda: development and implementation process. BMC Health Serv Res BioMed Central. 2014;14(1):S2.
Vallieres F, McAuliffe E, van Bavel B, Wall PJ, Trye A. There’s no app for that: assessing the impact of mHealth on the supervision, motivation, engagement, and satisfaction of community health workers in Sierra Leone. Ann Glob Heal United States. 2016;82(5):936–49.
Varma DS, Hart M, McIntyre DS, Kwiatkowski E, Cottler LB. A research protocol to test the effectiveness of text messaging and reminder calls to increase service use referrals in a community engagement program. JMIR Res Protoc. JMIR Publications Inc. 2016;5(2).
Wai MFP, Carvalho AMP. O trabalho do agente comunitário de saúde: fatores de sobrecarga e estratégias de enfrentamento. Rev enferm UERJ. 2009;17(4):563–8.
White A, Thomas DSK, Ezeanochie N, Bull S. Health worker mHealth utilization: a systematic review. Comput informatics, Nurs CIN NIH Public Access. 2016;34(5):206.
WHO. Primary health care: report of the international conference on primary health care, Alma-Ata, USSR, 6-12 September 1978. Geneva: World Health Organization; 1978.
Zakus D, Moussa M, Ezechiel M, Yimbesalu JP, Orkar P, Damecour C, et al. Clinical evaluation of the use of an mhealth intervention on quality of care provided by community health workers in southwest Niger. J Glob Health NLM (Medline). 2019;9(1):010812.
Zimmerman L, OlaOlorun F, Radloff S. Accelerating and improving survey implementation with mobile technology: lessons from PMA2020 implementation in Lagos, Nigeria. Etude La Popul Africaine. African Population Studies. 2015;29(1):1699.
Zurovac D, Sudoi RK, Akhwale WS, Ndiritu M, Hamer DH, Rowe AK, et al. The eff ect of mobile phone text-message reminders on Kenyan health workers ’ adherence to malaria treatment guidelines : a cluster randomised trial. Lancet Elsevier Ltd. 2011;378(9793):795–803.
The authors are grateful to all contributors of this study, Coordination for the Improvement of Higher Education Personnel (CAPES), University of Mogi das Cruzes (UMC), and grant #2017/14016-7, São Paulo Research Foundation (FAPESP).
Author information
Authors and Affiliations
Technological Research Center, University of Mogi das Cruzes, Av. Dr. Cândido Xavier de Almeida e Souza, Mogi das Cruzes, São Paulo, 08780911, Brazil
F. D. L. Abreu, M. A. S. Bissaco, A. P. Silva, S. R. M. S. Boschi, T. A. Scardovelli, M. F. Santos & S. C. Martini
Service for HIV / Aids Patients SEAP, Hospital das Clínicas da Faculdade de Medicina da Universidade São Paulo, HC/FMUSP, Rua Ferreira de Araujo, 789, São Paulo, 05428-002, Brazil
Abreu, F.D.L., Bissaco, M.A.S., Silva, A.P. et al. The use and impact of mHealth by community health workers in developing and least developed countries: a systematic review.
Res. Biomed. Eng.37, 563–582 (2021). https://doi.org/10.1007/s42600-021-00154-3