
Abstract
This study aimed to examine the quality of life (QoL) in the rural regions of Tehran metropolis in Iran, with a focus on the large population of rural migrants residing there. To conduct the study, a total of 61,402 households residing in the rural areas of Tehran metropolis were considered as the statistical population. To obtain a sample that accurately represents this population, a multi-stage random sampling approach was utilized. The resulting sample size consisted of 382 households (n = 382). The present survey study utilized a non-experimental, causal-correlational methodology to examine the state of quality of life (QoL) and its association with overall health and life satisfaction in Rural and peripheral regions. The findings showed that among the four aspects of QoL, physical health (with an average of 3.62) had the highest rank. Furthermore, psychological health, social relations, and environmental situation were in the second to fourth ranks, respectively with averages of 3.37, 3.17, and 3.15. The results revealed that the total score of QoL in the range of (4–20) was equal to 13.31, and in the range of (0–100), it was 58.18. Hence, the quality of life (QoL) in the rural regions of the Tehran metropolis is unsatisfactory and requires immediate attention. The findings of this study provide valuable insights into the QoL in rural areas on the outskirts of the Tehran metropolis. By identifying the factors that contribute to the QoL, policymakers and local authorities can develop targeted interventions to improve the living conditions and well-being of residents in these areas. This predicament is widespread in many developing countries, and the findings of this investigation can be utilized to prioritize policy and strategic planning in rural areas adjacent to metropolises. Moreover, it can facilitate the attainment of the Millennium Goals.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Today, with the development of societies and the improvement of living standards, the issue of Quality of Life (QoL) has gained considerable importance because the ultimate goal of development is to achieve the desired life (Amazonas et al., 2019; Catré et al., 2021). Obtaining information about the status of QoL of different populations can be considered basic information for planning and policy-making. The discussion of QoL has been the subject of many studies in various fields and disciplines such as health and medicine, environmental studies, psychology, economic studies, human geography, sociology, development studies, and other fields. It has not been possible to provide a comprehensive and uniform definition for it. One of the main reasons for this failure is the multifaceted nature of the concept (Darbanastaneh & Mahmoudi, 2016).
In General, within the past few eras, there has been a rising focus on understanding and measuring people's health beyond traditional health indicators. One of these indicators is the World Health Organization's QoL Index. Health is one of the sets and components of QoL, which is considered in this questionnaire (Skevington & Epton, 2018).
In the last three decades, developing countries have seen increasing urban population growth. This overflow of the population had consequences, one of which was the transformation on the outskirts of cities. Villages around these cities are not left without these changes and changes occur in their socio-economic, environmental, and physical structure and sometimes cause the formation of settlements. RURBAN or rural urbanization is the integration of urban and rural social structures around metropolitan areas. Demographic changes in the metropolitan area of Tehran also show that in the last three decades, the urban population has tripled and the surrounding areas of the metropolis of Tehran have increased eightfold (Talkhabi et al., 2018). Therefore, most of the overpopulation of the Tehran metropolitan area has settled in the surrounding areas.
Now, this research aims to investigate the quality of life of the villagers of the Tehran metropolis and to determine the status of the stability of the QoL components based on the World Health Organization's definition. It also examines the relationship of QoL with general health and life satisfaction among rural people of the Tehran metropolis.
Overall, the present study seeks the following two questions
-
1)
What is the status of QoL in rural spaces in the Tehran metropolis?
-
2)
What is the relation of QoL with life gratification and general health?
Literature Review & Theory
Health-related QoL is a multi-aspect notion that comprises social, psychological, physical, and environmental aspects. In this view, these dissimilar aspects of HRQOL structure layers of life satisfaction and general health (Yin et al., 2016). Life satisfaction indicates the degree of satisfaction of basic human desires and needs, and it is why the concept of satisfaction is related to need. Therefore, life satisfaction can be considered as satisfying human needs, positive perceptions, and pleasant feelings of people towards the realms of life (Di Castro et al., 2018). Michalos (2014) in his research confirmed that there is a noteworthy relationship between QoL and life satisfaction. Furthermore, in a study entitled “The Relationship Between Life Satisfaction with QoL and Subjecting Wellbeing in Tehran Teachers,” the results showed that life satisfaction can be predicted through two variables, namely personal well-being and QoL (Farahani et al., 2009). According to Maja and Ayano (2021), population and natural resource growth are significantly associated with climate change and the ability of farmers to adapt to climate change, particularly in developing countries with fast changes in resource-dependent demographic and economic changes. One of the important factors in environmental degradation is rapid population growth, which is a fundamental force and threat to the sustainable use of natural resources. These issues reduce the quality of natural resources and their quantity through land fragmentation, intensive agriculture, and over-exploitation. Lack of arable land in areas with increasing populations leads to reduced soil fertility and shorter fallow removal and farm incomes due to farmland fragmentation. In addition, landless people, or those who work on small farms, settling or cultivating. Food insecurity is exacerbated by low-income farmers working on small farms, limiting their ability to use some of the technologies adapted to climate change. In another research entitled “Relationship Between Life Satisfaction and QoL in Turkish Nursing School Students,” there was an important relationship between life gratification and QoL (Yildirim et al., 2013). Other studies showed that QoL is a predictor of general health (Aghaei et al., 2013). An individual’s general health is the condition of his/her body and the degree to which it is free from disease or is capable of fighting it. The only question “How is your health in general?” is an unpolished and easy measure that has been broadly used, as it grants researchers a brief description of an individual's general state of health (Simon et al., 2005; Galenkamp et al., 2020). This scale is confirmed to be a strong forecaster of people’s health, and this general health is strongly affected by the QoL of individuals.
Previous studies (Badiora & Abiola, 2017; Hongthong & Somrongthong, 2015; Nyamathi et al., 2017) have concluded that the satisfaction of people with life may be hemostatic, meaning that their level of satisfaction with life remains constant. This may not be possible in terms of life satisfaction for low-income families in rural communities. The satisfaction of rural communities may have changed with a combination of higher levels of relentless rural poverty and a welfare reform constitution. Understanding the realization of deprivation, which is the perceived difference between people's desire and success, may indicate a level of life satisfaction. Eventually, life satisfaction contributes to QoL, sometimes known as feelings of happiness or mental well-being. QoL may be described as the level to which individuals can meet their psychological needs or as a general understanding of the satisfaction of their needs over time. With the use of data from a project such as the current research on rural low-income families, we evaluated the influence of variables representing different forms of capital (public health and satisfaction of life) in low-income villages. This study investigated the perception of life satisfaction and QoL in a highly disadvantaged, yet neglected, group using longitudinal data and four dimensions of QoL in a unique combination. In addition, rural areas are very heterogeneous with urban areas in terms of income level, poverty, and QoL. The significant rate of rural poverty is an important justification for research into its characteristics. Another justification based on these observations is that rural experiences of QoL are often different from those in urban areas and this can affect the QoL, life gratification, and general health of villagers. Improving the QoL in rural communities is recognized as the final aim of development programs in rural regions. However, the primary precondition for achieving the mentioned goal is to provide suitable living situations that can improve the QoL for villagers. In addition, there is a great challenge today for many planners to understand that living conditions can provide a good quality of life for any individual or community.
Today, QoL as a key element in policymaking is called one of the basic indicators of development. Numerous studies have been conducted in this field and research shows that the QoL in the medical field is 8 times higher than the study of the QoL in the social sphere. The following are some of these studies. It should be mentioned that Kar et al. (2017), Yang et al. (2017), Sreedevi et al. (2016), and Lodhi et al. (2019) used the WHOQOL-BREF questionnaire to calculate the QoL; Yildirim et al. (2013) investigated the “Relationship Between Life Satisfaction and QoL in Turkish Nursing School Students,” and Simon et al. (2005) paid attention to the relation between general health and QoL (Table 1). However, none of the previous studies has examined the effect of QoL on life satisfaction and general health, which is one of the innovations of the present study, and this research intends to fill this knowledge gap.
So based on the literature review and field studies, it intends to measure the status of QoL in 4 general dimensions (Physical, Psychological, Social, and Environmental) in the rural areas of Tehran province and evaluate the impact of these dimensions on life satisfaction and general health (Fig. 1).

Conceptual framework
Research Methods
Research Area
Tehran province is one of the largest provinces in the country that accommodates more than 20% of the total population, and the villages of the province have more special demographic conditions than other provinces of the country. Tehran province is placed between 34 and 36.5 degrees’ northern latitude and 50 and 53 degrees’ eastern longitude. This province is limited to Mazandaran state from the north, Qom state from the south, Markazi state from the southwest, Alborz state from the west, and Semnan state from the east. According to the 2016 census, the population of this province was 13,267,637, of which 12,452,230 live in urban areas and 814,698 in rural areas. It consists of 10 counties (Fig. 2).

Map of the study area
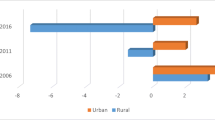
The population growth of Tehran province in the last three censuses has always been higher than the country's growth. The population growth of the Tehran province in the 1996–2006 period was 3.03%; this number for urban and rural areas was 3.75% and 3.27%, respectively. According to statistics, the rural population of Tehran province has been increasing during this period. Meanwhile, the growth trend of the country's rural population has been -0.44% and has been decreasing. This indicates the migration of a large number of villagers from other villages of the country to Tehran. From 2006 to 2011, the percentage of population growth in Tehran province was 1.44, which was 1.95 and -1.5 for urban and rural areas, respectively. This period is the beginning of the evacuation of the population in rural areas of Tehran province. This trend also continued and in the 2011–2016 period, despite the increasing trend of the province's population, i.e., 1.72%, the figure in urban areas increased to 2.6%, while this rate for rural areas of Tehran province has reached -7.43% (Fig. 3). One of the reasons for the evacuation of the mentioned population is the reduction in QoL of Tehran villagers, which shows the need to pay more attention to the research questions.

Percentage of population growth rate in urban and rural areas of Tehran province (Department of Statistics & Information of Tehran Province, 2016)
Data Collection and Analysis
In the past decades, many tools and questionnaires with different approaches (health, urban biology, economics, environmental quality, living standards, basic needs, etc.) have been developed and designed, each from a different perspective. Meanwhile, one of the tools that measure the QoL of individuals is the World Health Organization's QoL Questionnaire (WHO, 1995; Kim, 2014). The WHOQOL-BREF questionnaire has been transformed into different languages and validated in various regions due to the reduction of domains and items and the ease of use and scoring instructions. In Iran, this questionnaire was first translated and validated in 2006 (Nejat et al., 2006). The questionnaire includes four areas of “physical health (7 items), psychological health (6 items), social relationships (3 items), and environmental status (8 items)” (Nedjat et al., 2010) (Table 4), and two overall questions about the general health quality and general life satisfaction. All items were measured in the 5-point Likert range, from 1 = very low to 5 = very high. It is noteworthy that none of the previous studies assessed the relationship between QoL and feelings of good (general health and life satisfaction), and this research seeks to answer this question.
In the present study, the statistical population includes 61,402 families living in rural areas of the Tehran metropolis in 2019–2020. The sampling method was multi-stage random sampling. The Karaj-Morgan Table (1970) was used to determine the sample size, according to which, the number of samples was 382 according to the following table (Table 2).
Results of Cronbach alpha, AVE, and CR revealed good reliability and validity of the research tool in the studied area. In addition, Structural Equation Modeling (SEM) was used to confirm the study model. For the goodness of fit (GOF) of the model, indices such as GFI (“Goodness of Fit Index”), AGFI (“Adjusted Goodness of Fit Index”), NFI (“Normalized Fit Index”), TLI (“Tucker-Lewis Index”), IFI (“Incremental Fit Index”), CFI (“Comparative Fit Index”), and RMSEA (“Root Mean Square Error of Approximation”) (Cheraghi et al., 2019) have been used.
Findings
Ruralization is a special form of human settlement and livelihood and is a clear manifestation of economic and social life that has lasted with a more or less stable system for centuries. The role and position of villages in the processes of financial, communal, and political development on a provincial, national, and global level and the outcomes of underdevelopment of rural areas such as deprivation, growing discrimination, urbanization expansion, and unemployment and so on, have caused serious attention to rural development and its urgency over metropolitan development. With this attitude, the present article aims to calculate the QoL in rural spaces from the perspective of the sample community, and the number of respondents was 382, of which 353 (92.4%) were men and 369 (96.6%) were married. The youngest and the oldest respondents were 29 and 80 years old, respectively. Most of them (49%) were between the ages of 46 and 63. Regarding the degree of education of the studied people, it was shown that the literacy level of 311 respondents (81.4%) was undergraduate. Among the sample, 236 people (61.8%) reported that they had good health status, 123 people (32.2%) had moderate health status, 18 people (4.7%) had poor health status, and five people (1.3%) were in very good health status. The average general health status was 3.54. Regarding general life satisfaction, 47 (12.3%) people had low, 223 (58.4%) moderate, 100 (26.2%) good, and 12 (3.1%) very good life satisfaction status (Table 3) and the average overall life satisfaction was 3.07.
The findings show that among the four aspects of QoL, the physical dimension with an average of 3.62 has the highest rank. In addition, psychological health with an average of 3.37, social relations with an average of 3.17, and the environmental situation with an average of 3.15 are in the second to fourth ranks, respectively (Table 4).
Figure 4 shows the status of different dimensions of QoL. As it is depicted in the radar diagram, there is a big difference between different aspects of QoL.

Status of QoL components
QoL Score Divided into Four Dimensions
According to the guidelines of the questionnaire developed by the QoL Group of the WHO, the method of scoring the total QoL is in the ranges of (4–20) and (0–100). Table 5 shows the QoL scores in rural areas of Tehran province in the mentioned period and four dimensions.
The scores of the table revealed that the total score of QoL in the range of (4–20) was equal to 13.31, and in the range of (0–100), it was 58.18.
Structural Equation Modeling
In addition, in this study, to evaluate the effect of QoL on feeling good, which includes life satisfaction and general health, structural equation modeling (SEM) was used. Regarding the fit indices of the model (IFI, TLI, NFI, and GFI), the results showed that the values of these indices for the model were higher than 0.9, which is an acceptable value. Finally, the RMSEA index showed that the measurement error in the model is controlled. In general, the evaluation of the goodness of fit of the structural model was satisfactory (Table 6). In addition, the values of CR and AVE were calculated with a value of AVE greater than 0.5 and CR value greater than 0.7, which indicated the validity and reliability of the research tool.
Based on the results obtained in Table 6 and Fig. 3, which show the structural model of the research, it can be concluded that the model is appropriate. Given that, in addition to examining and testing the goodness of fit (GOF) of the research model and determining the amount of variance explained by independent research variables, it is clear that QoL affects people's life satisfaction and health, and 66% of the variance of feeling good (life satisfaction and health) is explained (Table 7).
In addition, from the regression equation, feeling good can be predicted through QoL as follows: QoL * (0.676) = Feeling good (Fig. 5).

The impact of QoL on Feeling good
Discussion & Conclusions
Improving the QoL in a place or for specific individuals and groups has always been the main focus of planners, and improving the QoL in any society is one of the most important goals of the public policies of that society.
The results of the present research revealed that the QoL in rural spaces is generally 58.18 in the 0–100 range, which is less than in other countries, such as the elderly in southern Brazil which is 67.3 (Gambin et al., 2015). Even compared to Hong Kong, although the arrangement of the dimensions is the same, i.e., physical, psychological, social, and environmental, the cultivars are very different, so in the present study, these scores are 65.5, 59, 54.25, and 53.7, respectively. However, these figures for similar dimensions in Hong Kong were 70.83, 65.43, 63.69, and 61.98, respectively (Wong et al., 2018). This shows a huge difference between the QoL in the compared areas. The difference between living standards in urban and rural areas of Iran is very huge. The QoL in many rural areas of Iran varies for various reasons, perhaps the most important of which is the lack of attention of officials, planners, and politicians. Factors such as access to human capital, physical capital, and financial and social capital will play an important role in satisfying and improving the quality of life in rural areas.
However, the results of current research displayed that the QoL of villagers living in the metropolitan area of Tehran is better than the QoL of COVID-19 patients, living in Wenzhou, China. The average health-related QoL between them was estimated below 50 and patients had low physical and psychological QoL status (Chen et al., 2020). In this regard, it is suggested that health-related QoL in rural areas infected with the coronavirus be examined.
The results showed that physical health had the highest score and environmental situation score had the lowest position. In addition, in the present study, in comparison with the average values of 24 countries, the means are drastically different, so the QoL in rural spaces of the metropolis of Tehran for different physical, psychological, social, and environmental dimensions in the range of 4–20 is 14.48, 13.44, 12.68, and 12.60, and these figures were 16.2, 15, 14.3, and 13.5 in 24 countries (Skevington & Epton, 2018), respectively. In the rural areas of the Tehran metropolis, the QoL in the physical and psychological dimensions is higher, except for people with certain diseases and the elderly who have special problems in these two dimensions. For example, the mentioned numbers for people with sclerosis in the range of 4–24 were 13.19 and 13.11 (Pomeroy et al., 2020), and these figures were calculated for our respondents as 14.48 and 13.44, which is due to the physical problems of the mentioned people.
In addition, this study shows a positive and significant relationship between QoL and life satisfaction which is similar to the results of the study by Yildirim et al. (2013). However, in their research, the severity of this correlation was less than in the present study. In addition, in Abedi et al. (2014) research it was revealed that there was a positive and meaningful relationship between the QoL and a couple’s life satisfaction at a significant level of 5%, which is consistent with the present study.
In addition, regarding the relationship between QoL and general health, this study was in line with previous studies by Esmaeilpour and Jafarjalal (2019) and Najafi et al. (2018), which shows a positive and significant relationship between QoL and general health. Of course, it is worth mentioning that both of these studies have been performed on nurses and no research has been done on the relationship between the health-related QoL and the general health of villagers, which this research sought to find this connection.
In addition, the impact of QoL on feeling good (general health and satisfaction) had not been addressed in previous studies, which is one of the novelties of the present study.
The results of this study displayed that 66% of the variance of feeling good is affected by QoL, which is a high percentage of variance that can be considered in development planning. In addition, in the dimensions that affect the feeling of good, psychological, environmental, physical, and social factors are effective, respectively. Due to the low status of QoL in the psychological and environmental dimensions, these should be considered to improve the feelings of rural people specifically in developing countries. This study presents a limitation, which is intrinsic to its sampling process; that is, individuals living far from the area of selected households may present health profiles and lifestyles different from those evaluated, which could modify the observed results.
To further enhance the rural communities’ QoL, it is recommended that the focus should be placed on efforts to further improve infrastructure facilities, while programs, strategies, and plans on enhancing rural communities’ QoL should be focused on specific groups of lower-income minorities, females and lower education achievers. Therefore, it is recommended that rural women’s QoL be investigated since a gender-sensitive analysis of QoL can provide better solutions for rural development. In addition, factors affecting QoL should be investigated. Accordingly, rural development programs around urban areas, family hope programs that include social programs aimed at eliminating gender discrimination, reducing poverty, and nutrition care and support for children and the elderly should be a planning priority. The results of this study can be used in other similar/different rural areas. These findings can help rural development planners, the WHO, and national and regional health centers. By targeting the findings of this study, they can improve the living conditions, quality, and satisfaction of people in rural areas, identify challenges, and provide opportunities.
In this study, the QoL related to the health of rural men and women was not compared; it is suggested that this issue be addressed in future research. In addition, it is suggested that the same relationships in different age groups, i.e., young, middle-aged, and old, be examined and compared.
Data Availability
The datasets analyzed during the current study are available in the Dataverse repository: https://doi.org/https://doi.org/10.57760/sciencedb.09704.
References
Abedi, G., Darvari, S. H., Nadighara, A., & Rostami, F. (2014). The relationship between quality of life and marriage satisfaction in infertile couples using path analysis. Journal of Mazandaran University of Medical Sciences, 24(117), 184–193.
Aghaei, A., Khayyamnekouei, Z., & Yousefy, A. (2013). General health prediction based on life orientation, quality of life, life satisfaction, and age. Procedia - Social and Behavioral Sciences, 84, 569–573.
Amazonas, I. T., Kawa, N. C., Zanetti, V., et al. (2019). Using rich pictures to model the ‘good life’ in indigenous communities of the tumucumaque complex in Brazilian Amazonia. Human Ecology, 47, 341–354.
Badiora, A. I., & Abiola, O. B. (2017). Quality of life (QoL) of rural dwellers in Nigeria: A subjective assessment of residents of Ikeji-Arakeji, Osun-State. Annals of Ecology and Environmental Science, 1(1), 69–75.
Catré, M. N. C., Ferreira, J. A., Catré, M. C., & Pereira, M. (2021). Development and application of a short-form questionnaire for assessing spiritual, religious, and personal beliefs related to quality of life (WHOQOL-SRPB-BREF) in Portugal. Applied Research in Quality of Life, 16, 241–258.
Chen, K. Y., Li, T., Gong, F. H., Zhang, J. S., & Li, X. K. (2020). Predictors of health-related quality of life and influencing factors for COVID-19 patients, a follow-up at one month. Frontiers in Psychiatry, 11, 668.
Cheraghi, S., Choobchian, S., & Abbasi, E. (2019). Factors affecting decision-making process in renewable energies investment in agricultural sector, Iran. Journal of Agricultural Science and Technology, 21(7), 1673–1689.
Darbanastaneh, A., & Mahmoudi, M. (2016). Assessment of the life quality in new Agropolitans case study: Banvareh in Kermanshah Province. Geography and Development Iranian Journal, 14(42), 199–218.
Department of Statistics and Information of Tehran Province. (2016). Available at: http://amar.org.ir
Di Castro, V. C., Hernandes, J. C., Mendonça, M. E., et al. (2018). Life satisfaction and positive and negative feelings of workers: A systematic review protocol. Systematic Reviews, 7, 243.
Esmaeilpour, L., & Jafarjalal, E. (2019). The Association of the quality of work life and general health of the nurses in psychiatric wards. Iran Journal of Nursing, 32(117), 69–79.
Farahani, M. N., Mohammadkhani, S., & Joker, F. (2009). The relationship between life satisfaction with the quality of life and subjecting wellbeing in Tehran teachers. Research in Psychological Health, 3(1), 5–0.
Feder, K., Michaud, D. S., Keith, S. E., Voicescu, S. A., Marro, L., Than, J., … van den Berg, F. (2015). An assessment of quality of life using the WHOQOL-BREF among participants living in the vicinity of wind turbines. Environmental Research, 142, 227–238.
Galenkamp, H., Braam, A. W., Huisman, M., & Deeg, D. J. (2020). Self-rated health: When and how to use it in studies among older people? International Handbook of Health Expectancies, 173–181.
Gambin, G., Molzahn, A., Fuhrmann, A. C., Morais, E. P., & Paskulin, L. (2015). Quality of life of older adults in rural southern Brazil. Our Remote Health, 15, e3300.
Hongthong, D., & Somrongthong, R. (2015). Factors influencing the quality of life (QoL) among Thai older people in rural areas of Thailand. Iranian Journal of Public Health, 44(4), 479.
Kar, N., Swain, S. P., Patra, S., & Kar, B. (2017). The WHOQOL-BREF: Translation and validation of the Odia version in a sample of patients with Psychological illness. Indian Journal of Social Psychiatry, 33, 269–273.
Kim, S. (2014). World Health Organization Quality of Life (WHOQOL) Assessment. In A. C. Michalos (Ed.), Encyclopedia of quality of life and well-being research. Springer. https://doi.org/10.1007/978-94-007
Lodhi, F. S., Montazeri, A., Nedjat, S., Mahmoodi, M., Farooq, U., Yaseri, M., Kasaeian, A., & Holakouie-Naieni, K. (2019). Assessing the quality of life among the Pakistani general population and their associated factors by using the World Health Organization’s quality of life instrument (WHOQOL-BREF): A population-based cross-sectional study. Health and Quality Life Outcomes, 17(1), 9.
Maja, M. M., & Ayano, S. F. (2021). The impact of population growth on natural resources and farmers’ capacity to adapt to climate change in low-income countries. Earth Systems and Environment, 5, 271–283.
Michalos, A. C. (2014). Quality of life, satisfaction with. In A. C. Michalos (Ed.), Encyclopedia of quality of life and well-being research. Springer. https://doi.org/10.1007/978-94-007-0753-5-2379
Najafi, F., Kermansaravi, F., & Gangoozehi, E. (2018). The relationship between general health and quality of work life of nurses working in Zahedan Teaching Hospitals. Iranian Journal of Rehabilitation Research in Nursing, 4(2), 53–59.
Nedjat, S., Holakouie Naieni, K., Mohammad, K., Majdzadeh, R., & Montazeri, A. (2010). Quality of life among an Iranian general population sample using the World Health Organization’s quality of life instrument (WHOQOL-BREF). International Journal of Public Health, 56(1), 55–61.
Nejat, S., Montazeri, A., Holakouie Naieni, K., Mohammad, K., & Majdzadeh, S. (2006). The World Health Organization Quality of Life (WHOQOL-BREF) questionnaire: Translation and validation study of the Iranian version. Sjsph, 4(4), 1–12.
Nyamathi, A. M., Ekstrand, M., Yadav, K., Ramakrishna, P., Heylen, E., Carpenter, C., … Sinha, S. (2017). Quality of life among women living with HIV in rural India. Journal of the Association of Nurses in AIDS Care, 28(4), 575–586.
Pomeroy, I. M., Tennant, A., Mills, R. J., et al. (2020). The WHOQOL-BREF: A modern psychometric evaluation of its internal construct validity in people with multiple sclerosis. Quality of Life Research, 29, 1961–1972.
Praveen, V., & Rani, A. M. (2016). Quality of life among elderly in a rural area. International Journal of Community Medicine and Public Health, 3, 754–757.
Simon, J. G., De Boer, J. B., Joung, H., & Bosma, J. P. (2005). How is your health in general? A qualitative study on self-assessed health. European Journal of Public Health, 15(2), 200–208.
Skevington, S. M., & Epton, T. (2018). How will the sustainable development goals deliver changes in well-being? A systematic review and meta-analysis to investigate whether WHOQOL-BREF scores respond to change. BMJ Global Health, 3, e000609.
Sreedevi, A., Cherkil, S., Kuttikattu, D. S., Kamalamma, L., & Oldenburg, B. (2016). Validation of WHOQOL-BREF in Malayalam and determinants of quality of life among people with type 2 diabetes in Kerala, India. Asia Pacific Journal of Public Health, 28(1_suppl), S62–S69.
Talkhabi, H. R., Soleimani, M., Saeidnia, A., & Zanganeh, A. (2018). Metropolis explosion and sprawl of Tehran within the framework of urban decline theory. Geographical Urban Planning Research (GUPR), 6(3), 451–472. https://doi.org/10.22059/jurbangeo.2018.251153.859
Vo, T. Q., Tran, D. D., & Dinh, H. T. T. (2020). Health-related quality of life among undergraduate dentistry students in Ho Chi Minh, Vietnam: A cross-sectional WHOQOL-BREF study. Journal of Pharmacy & Pharmacognosy Research, 8(3), 201–210.
WHO. (1995). The World Health Organization Quality of Life Assessment (WHOQOL). Position paper from the World Health Organization. Social Science & Medicine, 41(10), 1403–1409.
Wong, F. Y., Yang, L., Yuen, J. W. M., et al. (2018). Assessing quality of life using WHOQOL-BREF: A cross-sectional study on the association between quality of life and neighborhood Environmental satisfaction, and the mediating effect of health-related behaviors. BMC Public Health, 18, e1113.
Yang, Y., Bekemeier, B., & Choi, J. (2017). Health-related quality of life and related factors among rural residents in Cambodia. Iran J Pub Health, 46(3), 422–424.
Yildirim, Y., Kilic, S. P., & Akyol, A. D. (2013). Relationship between life satisfaction and quality of life in Turkish nursing school students. Nursing & Health Sciences, 15(4), 415–422.
Yin, S., Njai, R., Barker, L., Siegel, P. Z., & Liao, Y. (2016). Summarizing health-related quality of life (HRQOL): Development and testing of a one-factor model. Population Health Metrics, 14, 22.
Acknowledgements
The authors hereby express their special gratitude to all the respondents who completed the study questionnaires with great patience as well as the surveyors and interviewers who did their best in terms of data collection.
Funding
This study received no findings from any organizations.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
No conflict of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ardestani, L., Choobchian, S., Sadighi, H. et al. Investigating the Quality of Life in Rural Areas on the Outskirts of Metropolises: Application of World Health Organization Standard Questionnaire. Int. Journal of Com. WB 7, 121–137 (2024). https://doi.org/10.1007/s42413-023-00203-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42413-023-00203-y