
Abstract
Pneumorrhachis is a condition in which air or gas is entrapped in the spinal canal. Due to its rarity, it can present a diagnostic challenge. Usually, pneumorrhachis represents an asymptomatic epiphenomenon; however, it can produce symptoms associated with its underlying pathology. Here, we report a rare case of symptomatic epidural pneumorrhachis after arthrodesis in a patient with gunshot wounds of the thoracic spine. Possible pathogenic mechanisms are discussed and a review of the literature is provided. A 28-year-old male patient with a gunshot wound receiving posterior spinal fixation without any intraoperative complications presented with intolerable and diffuse pain in the neck and back making it impossible for him to remain in the supine position. Epigastralgia and dysesthesia, especially in the upper limbs and right hemithorax, also lead to loss of sensitivity to touch, especially in the distal extremities of the upper limbs. Magnetic resonance imaging (MRI) examinations showed a clear presence of air (hypodense signal) in the treated thoracic region. A hyperbaric chamber was initially for five sessions and at the end of the five sessions the patient complained of dysesthesia and changes in distal fine motor skills, with almost complete recovery of strength. Five more sessions were performed with total improvement in sensory changes and almost complete recovery of strength. Pneumorrhachis, although usually asymptomatic, can present in some cases with several neurological impairments due to spinal cord compression.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pneumorrhachis is defined as the presence of air within the intradural or extradural compartments of the spinal canal [1]. Air within the epidural space is also referred to as epidural emphysema or epidural pneumorrhachis and has been described and associated with several other conditions and causes [2,3,4,5,6].
Pneumorrhachis is frequently asymptomatic and does not require any specific treatment because air is reabsorbed spontaneously without leaving any neurological sequelae [4, 7]. The onset of symptoms in pneumorrhachis cases is very rare; however, when they occur, they can cause discomfort and/or pain and even neurological deficits [7,8,9].
And although cases of pneumorrhachis are mainly treated with conservative approaches, in some cases, measures are needed to treat the entity that is causing the pneumorrhachis [8].
Herein, we report a rare case of symptomatic epidural pneumorrhachis after arthrodesis, defined as immobilization of one or more joints through surgical fusion of the adjacent bones, in a patient with gunshot wounds of the thoracic spine.
Case Report
Here, we report a case of pneumorrhachis occurring after posterior spinal fixation to treat a patient with gunshot wounds.
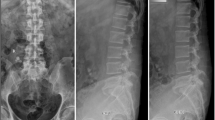
A 28-year-old male patient, with no prior comorbidities, who was a victim of a gunshot wound to the thoracic spine (T9), arrived at our service already paraplegic (ASIA A, with a sensitivity level of T8) (Fig. 1). Arthrodesis was performed to stabilize the fracture avoiding kyphotization and long-term pain. Spinal fixation was performed using a titanium rod and pedicle screws. The patient remained hospitalized for 7 days and was discharged without further complaints.

CT showing the presence of bullet fragments at the T8/T9 level
He remained stable and was followed up for two months after the surgery. He returned to our emergency room with a complaint of intolerable and diffuse pain in the neck and back, making it impossible for him to remain in the supine position, epigastralgia and dysesthesia, especially in the upper limbs and right hemithorax. He also reported a loss of sensitivity to touch, especially in the distal extremities of the upper limbs. In the initial evaluation, a fistula was identified, with an operative scar in good appearance, without phlogistic signs or secretions. The patient developed tetraparesis, losing strength in the upper limbs, worsening on the right side, and with reduced fine motor coordination. Cervicothoracic spine tomography revealed extensive pneumorrhachis extending from C2 to T10 and excessive compression of the spinal cord (Fig. 2).

CT scans showing the presence of pneumorrhachis at the intrumentated levels and above
A hyperbaric chamber was initially for five sessions, with clinical improvement of symptoms reported since the first session. In the control tomography after the fourth session, clear reabsorption of gas in the spinal canal was observed in the region of the thoracic spine (Fig. 3). At the end of the five sessions, the patient complained of dysesthesia and changes in distal fine motor skills, with almost complete recovery of strength. Five more sessions were performed with total improvement in sensory changes and almost complete recovery of strength.

CT scans showing complete resolution of pneumorrhachis in the thoracic spine and almost complete resolution of the cervical spine
Discussion
This report describes the occurrence of late-onset pneumorrhachis in a patient who underwent posterior fixation to treat a fracture derived from a gunshot.
The occurrence of pneumorrhachis is rare and usually it occurs in an asymptomatic fashion [7, 8]. There are very few reports in the literature regarding the presence of pneumorrhachis secondary to arthrodesis. Karavelioglu et al. (2014) reported a case of pneumocephalus, reviewed the literature, and found only six cases of pneumocephalus after spinal surgery [5]. Considering only pneumorrhachis, one article reported the occurrence of pneumorrhachis after spinal fusion and reported that during a scoliosis correction procedure, the evoked potential signal was almost lost due to the presence of an intradural pneumorrhachis [10]. Furthermore, another study reported the occurrence of delayed presentation of both pneumorrhachis and pneumocephalus due to CSF leakage [11]. Finally, Bautista et al. (2021) reported the occurrence of pneumorrhachis after cervical spinal surgery [12]. Although the specific cause of air influx into the canal is not well established, the leading hypothesis is that it could occur after small dural injuries unperceived during spinal procedures [12].
When presenting with a symptomatic case of pneumorrhachis, the team must try to identify the possible causative agent, remove it, or treat it with antibiotics, allied with hydration, bed rest, and correct positioning to avoid headaches and couching [12]. Another crucial factor to access when dealing with pneumorrhachis is the location of the entrapped air, as the clinical consequences of epidural pneumorrhachis and subarachnoid pneumorrhachis are different from each other. According to a previous case report, the first is innocuous and self-limiting, while the second can be complicated by tension pneumocephalus and meningitis [2, 8, 12].
Furthermore, it is important to conduct a thorough and daily neurological examination to evaluate and detect any changes that may indicate neurological deterioration due to an increase in the collection of air in the spinal canal; if this occurs, it is indicative of a new image exam immediately [1, 2]. Diagnosis is made through imaging tests, such as computed tomography, magnetic resonance imaging, or radiography. Most of the cases described had conservative treatment and continuous monitoring of the patient with serial neurological assessment [1, 2, 8].
No treatment methods or courses of treatment have been established for pneumorrhachis. Several authors have reported the use of conservative treatments such as bed rest and pain medicine. If the symptoms are intense, oxygen or hyperbaric treatment should be used, or more aggressive treatments such as laminectomy or dural repair should be used [7].
In the present report, the patient evolved with a slowly progressive and asymmetrical improvement in symptoms as the air collection was being absorbed—initially from paresthesia and later also from paresis of the upper limbs—and was discharged with almost complete improvement of the neurological deficits after 4 weeks of performing a total of ten sessions in a hyperbaric chamber. In association with pneumorrhachis treatment, the patient started using pregabalin to help with dysesthetic symptoms.
Conclusion
Herein, we describe a rare case of symptomatic epidural pneumorrhachis after arthrodesis in a patient with gunshot wounds of the thoracic spine. Although infrequent and very rarely symptomatic, surgeons must be aware of the clinical and imagological signals of pneumorrhachis, given its potential to cause neurological damage through spinal cord compression.
Data availability
Not applicable
Code Availability
Not applicable
References
Oertel MF, Korinth MC, Reinges MHT, Krings T, Terbeck S, Gilsbach JM. Pathogenesis, diagnosis and management of pneumorrhachis. Eur Spine J. 2006;15:636.
Vanmali A, Daji KD. Pneumorrhachis: an uncommon radiological entity. SA J Radiol. 2021. https://doi.org/10.4102/SAJR.V25I1.2255.
Derakhshan N, Baghban F, Haghnegahdar A. Cervical pneumorrhachis. Bull Emerg Trauma. 2013;1:186.
Pfeifle C, Henkelmann R, von der Höh N, Jarvers JS, Spiegl U, Josten C, Heyde CE. Traumatic pneumorrhachis. Injury. 2020;51:267–70.
Karavelioglu E, Eser O, Haktanir A. Pneumocephalus and pneumorrhachis after spinal surgery: case report and review of the literature. Neurol Med Chir (Tokyo). 2014;54:405.
Osunronbi T, Sofela A, Sharma H, Muquit S. Traumatic pneumorrhachis: systematic review and an illustrative case. Neurosurg Rev. 2021;44:731–9.
Koktekir E, Tatarli N, Ceylan D, Koktekir BE, Akdemir G. Symptomatic pneumorrhachis. J Neurol Surg A Cent Eur Neurosurg. 2014;75:140–5.
Kim SW, Seo HJ. Symptomatic epidural pneumorrhachis: a rare entity. J Korean Neurosurg Soc. 2013;54:65.
Krishna P, Gupta M. Symptomatic pneumorrhachis after an epidural blood patch. J Emerg Med. 2015;49:e49–52.
Bhat SB, Blumer S, Shah SA. Epidural pneumorrhachis causing intraoperative loss of motor potentials during instrumented fusion for scoliosis: a case report. JBJS Case Connect. 2017;7(3):e53. https://doi.org/10.2106/JBJS.CC.16.00191.
Kieser DC, Cawley DT, Tavolaro C, Cloche T, Roscop C, Boissiere L, Obeid I, Pointillart V, Vital JM, Gille O. Delayed post-operative tension pneumocephalus and pneumorrhachis. Eur Spine J. 2018;27:231–5.
Bautista M, Wright J, Pippalapalli J, Schramm MWJ, Anderson IA, Pandit MH. Pneumorrhachis following cervical spine surgery. Anaesth Rep. 2021. https://doi.org/10.1002/ANR3.12137.
Author information
Authors and Affiliations
Contributions
FF: conceptualization, investigation, and writing—original draft. GH: writing—original draft, visualization, and conceptualization. BSB and FAMF: conceptualization, methodology, formal analysis, and writing—review and editing, project administration, and supervision.
Corresponding author
Ethics declarations
Ethics Approval
Not applicable
Consent to Participate
The patient consented in have his images and information collected
Consent for Publication
The patient consented in have his images and information collected
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Fernando Antonio de Melo Filho: Membro Titular da Sociedade Brasileira de Neurocirurgia; Membro da Academia Brasileira de Neurocirurgia, Rio de Janeiro, Brazil
Bruno Santos Bogea: Membro Titular da Sociedade Brasileira de Neurocirurgia
This article is part of the Topical Collection on Surgery
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Fenner, F., de Melo Filho, F.A., Pokorny, G. et al. Symptomatic Pneumorrhachis After Arthrodesis Due to Gunshot Wounds—a Case Report. SN Compr. Clin. Med. 5, 211 (2023). https://doi.org/10.1007/s42399-023-01549-2
Accepted:
Published:
DOI: https://doi.org/10.1007/s42399-023-01549-2