
Abstract
In the past 30 years, the life expectancy in China continues to rise yet at a slower pace because of, in large part, the heavy burden of chronic diseases on older age groups. Based on data obtained from the United Nations World Population Prospects 2019 and the Global Burden of Disease Study 2019, this study applies Arriaga’s decomposition method to decompose the age/cause-specific contributions to life expectancy gap between China and South Korea during 1990–2019, which could provide understanding on mortality patterns and heavy burden by chronic disease resulting from an aging society. The study has found that the life expectancy gap between these two countries for females has remained constant, while that of males has been increasing during the same period. Another finding is that non-communicable diseases, like cardiovascular diseases among the elderly (aged 60+), explain a large and enlarging part of the life expectancy gap between China and South Korea, especially among males. In addition, maternal and neonatal disorders among children (age group 1–4ys) contribute less and less to life expectancy gap. Those observations suggest a convergence of mortality pattern among younger age groups as well as the continued existence of substantial gaps among older age groups. Additionally, given the precedent of South Korea, China should also take suicide as another issue with greater attention in the future. Finally, this study concludes by suggesting targeted public health policies to reduce mortality in certain age groups and save more lives from certain diseases.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
In the past few decades, with remarkable economic development, China has obtained such an achievement as becoming an upper-middle-income country. Meanwhile, the progress in public health is another brilliant accomplishment (Ebenstein et al., 2015). From 1990 to 2019, life expectancy at birth in China increased by 9.50 from 68.09 to 77.59 years for both genders (GBD, 2020).
In early years, such increase could mainly be attributed to improved healthcare for mothers and children promoted by the Chinese government to control maternal and infant mortality (Xu et al., 2014). In recent years, however, the declining mortality rates among those elderly with chronic diseases have become prominent factors contributing to the gains in China’s life expectancy (Chen et al., 2020) thanks to better medical infrastructure. Since mechanisms affecting life expectancy is so multi-leveled and multi-faceted (Summoogum & Fah, 2016), relevant researches are still warranted in the social context of population aging and low fertility rates.
Despite gains in life expectancy at birth, there are still considerable gaps between China and other Asian countries/regions with high life expectancy (Adair et al., 2019; Kim et al., 2021; Zheng et al., 2019). As a neighbor to the northeast of China, the Republic of Korea (hereinafter referred to as South Korea) have a variety of commonalities with China with regard to history, culture, lifestyles, dietary habits and social contexts (Fan et al., 2017; Feng et al., 2015; Jones, 2019; Liang et al., 2013; Nam et al., 2010).
While both countries face low fertility rate and an aging population, life expectancy gaps between China and South Korea have widened from 4.04 to 5.32 years from 1990 to 2019 (GBD, 2020). South Korea is a country with one of the highest life expectances around the world, increasing the life expectancy of its citizens by 10.78 from 72.13 years in 1990 to 82.92 years in 2019 (GBD, 2020). Some even estimate that South Korea could surpass Japan in terms of life expectancy and become the country with the highest life expectancy in Asia in 2030 (Kontis et al., 2017).
Though previous studies have revealed health disparities due to different aspects among East Asian countries (Kim et al., 2019; Sun et al., 2020), few of them have explored the health differences regarding age groups and mortality causes. The purpose of this study, therefore, is to reveal age-specific and cause-specific reasons behind life expectancy gaps during 1990–2019 from a perspective of national comparison, so as to help the Chinese government draw lessens from what have happened in South Korea.
In statistics, life expectancy at birth is obtained from calculation considering the mortality of different age groups (Auger et al., 2014). Conventionally, Arriaga’s decomposing method is used to investigate age-specific and cause-specific contributions to the life expectancy gap between two populations (Arriaga, 1984). The application of such method can help understand essential factors that contribute to life expectancy gaps between China and South Korea, so as to further reveal mortality disparities in different age groups and diseases.
Therefore, the research objectives of this study are: (1) to estimate life expectancy gaps between China and South Korea from 1990 to 2019, with particular focuses on years of 1990, 2000, 2010 and 2019; (2) to decompose age-specific and cause-specific contributions to life expectancy gaps between China and South Korea in the same time period and with the same focuses on particular years; and (3) to examine whether cause-specific contributions vary by ages.
Previous studies (Bahk & Jung-Choi, 2020; Chen et al., 2020; Kim et al., 2020; Yang et al., 2010) have revealed contributions to the increasing life expectancies in China and South Korea, respectively. To be specific, reduced mortality in non-communicable diseases, including cardiovascular diseases, chronic respiratory diseases and neoplasms, are the main driver for the increase of life expectancy in these two countries, which is also a trend observed in other industrialized countries (Acosta et al., 2022; Ho & Hendi, 2018) and developed regions (Zheng et al., 2019). Reduced mortality in non-communicable diseases could also could widen life expectancy gaps in multi-dimensional aspects like gender (Wu et al., 2022; Yang et al., 2012; Zhang et al., 2015), socioeconomic status (Bahk & Jung-Choi, 2020; Yang et al., 2010, 2012), cross-city (Khang & Bahk, 2019), and ethnicity (Riddell et al., 2018).
However, few studies have focused on life expectancy gaps between countries and changes of contributions to such gaps over a long period. Therefore, this study intends to offer a case in point between two east Asian countries, both with high life expectancy, to fill the research gap about factors contributing to life expectancy gaps among different populations.
2 Methods
2.1 Statistical analysis
Arriaga’s decomposition method is used to estimate age-specific and cause-specific contributions to life expectancy gaps between the two populations (Arriaga, 1984; Auger et al., 2014). The application of such a method requires the construction life tables for two populations and then decomposing life expectancy gaps resulted from these life tables. In this study, \(_{n}{a}_{x}\), the average number of person–years living in the interval by those dying in the interval, is assumed as half length of the age interval. The life tables for China and South Korea are further constructed by gender at four research time points. The life expectancies are then recalculated by these new life tables.
The Arriaga’s decomposition method consists of two main functions. The first one calculates age-specific mortality contributions to gap in life expectancy (\(_{n}\varDelta _{x}\)) between population A and population B within ages x and x + n. In this study, it is expressed as.
where, SK represents the Republic of Korea and CN represents China. The total sum of \(_{n}\varDelta _{x}\) for a given age group is the contribution by this age group to the overall life expectancy gap.
The second function gauges age/cause-specific mortality contributions to gap in life expectancy (\(_{n}{\varDelta }_{x}^{i}\)) within ages x and x + n. In this study, it is expressed as.
where \(_{n}{R}_{x}^{i}\) is the proportion of deaths between ages x and x + n due to cause i while \(_{n}{M}_{x}\) is the all-cause mortality between ages x and x + n. Therefore, the total sum of the (\(_{n}{\varDelta }_{x}^{i}\)) for all age groups is the contribution of the cause to the life expectancy gap.
Finally, the total life expectancy gap between China and South Korea are decomposed as age-specific and cause-specific contributions. A research survey on Iran has pointed out that while racial, ethnic, socio–economic, geographical and other kinds of factors could all bring impacts on the inequality of life expectancy, age and cause of death are the key factors causing such inequality (Mehregan et al., 2022). The advantage of this approach is that the disaggregation results are more comparable and it is possible to assign responsibility for mortality changes to specific age groups or causes of death (Beltrán-Sánchez et al., 2008).
2.2 Data
This study constructs life tables to calculate life expectancies and the corresponding gaps between China and South Korea, by collecting population data from the United Nations World Population Prospects 2019 and mortality data from the Global Burden of Disease Study 2019. The Global Burden of Disease Study gathers age-specific and cause-specific deaths from countries around the world and estimates the life expectancy at birth for each country every year. These were data from vital registration systems, sample registration systems, household surveys (complete birth histories, summary birth histories and sibling histories), censuses (summary birth histories and household deaths) and Demographic Surveillance Sites (DSS).
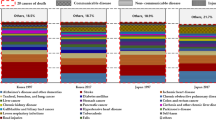
For calculating age-specific and cause-specific contributions to life expectancy gap in the later part of this study, data are further processed. Since the UN provides age-specific population data in a single year, the current study further processes the data into 5-year-old-long age groups, except for < 1 year-old, 1–4 years-old and the last open–ended age group (90 years old and above). The cause-specific deaths from the GBD are hierarchically organized into level 1 and level 2 by ages. The highest level (level 1) consists of non-communicable diseases (NCD), infectious diseases and injuries (unintentional injuries not include transport injuries). The other 21 subtypes in level 2 are shown in Table 1.
3 Results
3.1 Life expectancy gap

Trend of life expectancy for China and South Korea, Female and Male, 1990–2019
Figure 1 shows the trend of life expectancies in China and South Korea by gender during 1990–2019. The trends of life expectancy gap are significantly different between male and female: the female life expectancy gap keeps stable for nearly three decades (5.89 years in 1990, 5.98 years in 2000; 5.95 years in 2010 and 4.87 years in 2019). The life expectancy of Korean females rose from 76.11 years in 1990 to 85.65 years in 2019. In China, corresponding figures are 70.22 in 1990 and 80.78 in 2019. The narrowing of the gap for female life expectancy in 2019 is mainly due to the stagnation of growth in life expectancy for Korean female, which recorded a small negative growth (− 0.05%) compared with that of 2018.
Conversely, a strong increase in the life expectancy gap could be observed for males. The life expectancy of Korean men increased from 68.15 years old in 1990 to 80.04 years old in 2019, while that of Chinese men increased from 66.17 years old to 74.47 years old. The life expectancy gap thus widened from 1.98 years in 1990 to 5.3 years in 2019 (in between, 3.58 years in 2000 and 5.13 years in 2010). However, although life expectancy gap for males has widened, the increases of life expectancy in Chinese and Korean males have not undergone any negative growth.
3.2 Age-specific contributions to national life expectancy gap

Age-specific contributions to life expectancy gap between China and South Korea, Female and Male in 1990, 2000, 2010 and 2019
Figure 2 shows the change of age-specific contributions to life expectancy gaps between China and Korea over the same time period. While female life expectancy gap has remained relevantly stable, the main age group contributing to the life expectancy gap has experienced a shift from the young to the old. Infants (aged under 1) and young children (aged 1 to 4) contributed the most in 1990 (1.3 and 0.68 years), but their contributions have decreased in 2019 to 0.27 years and 0.08 years. The contribution of the elderly female (aged 60 and above) increases over this time period (2.20 years in 1990 and 4.83 years in 2019).
Meanwhile, the 80–84 age group (0.98 years in 2019) has gradually become the one that contributes the most to the corresponding life expectancy gap. Moreover, a cohort effect could be observed: women who were born between 1926 and 1930 contributed the most to life expectancy gap in 2000 (by 0.65 years when they are 70–74 years old) and 2010 (by 0.98 years when they are 80–84 years old).
For men, drastic changes in mortality patterns in China and South Korea have contributed to a widening gap in male life expectancy. In 1990, the gap of life expectancy for males was narrow, mainly due to the negative contribution of middle-aged men (0.86 years by those aged 30–59) and positive contribution of infant boys (2.08 years by those aged 0–4) offsetting each other.
Since 2000, the contributions (0.31 years) of young-aged and middle-aged people (aged 15–44) have changed from negative to positive while the positive contribution (1.15 years) of the middle-aged and the elderly (aged 55 and above) have increased. In addition, contributions of male babies and young boys are still-high, therefore the gap of life expectancy for male in 2000 suddenly increased by 1.56 years. After 2010, although the contributions of male babies and young boys decreased and that of male aged 90 or above contributed negatively, the contributions (3.47 years) of older men (aged 60–89) increased. Finally, an age-specific contribution pattern dominated by older men (aged 60–89, 4.28 years) in 2019 was formed, leading to a further widening of the overall gap of life expectancy for males.
3.3 Cause-specific contributions to national life expectancy gap

Level 1 cause-specific contributions to life expectancy gaps between China and South Korea, Female and Male in 1990, 2000, 2010 and 2019

Level 2 cause-specific contributions to life expectancy gaps between China and South Korea, Female and Male in 1990, 2000, 2010 and 2019
According to Fig. 3, causes-specific contributions change over time, with the proportion of NCD gradually increasing. For female, the pattern of cause-specific contributions has been shifted, although the overall life expectancy gap for female narrowed in a negligible way. For male, the reversal in the cause-specific contributions was more significant and accompanied by an increase in life expectancy.
As shown in Figs. 3 and 4, female NCD accounts for the prominent contribution to the life expectancy gap and has increased during this time period (2.89 years in 1990 and 5.59 years in 2019), including cardiovascular diseases with the highest contribution (0.53 years in 1990 and 3.95 years in 2019), chronic respiratory diseases (1.83 years in 1990 and 1.04 years in 2019) and neoplasm (0.41 years in 1990 and 0.54 years in 2019). A reduction could be observed in female infectious diseases (1.91 years in 1990 and 0.07 years in 2019), including respiratory infections and tuberculosis (1.07 years in 1990 and 0.06 years in 2019). Contributions of female injuries are negative and insignificant (0.43 years in 1990 and − 0.09 years in 2019), among which self-harm and interpersonal violence have decreased the most (0.36 years in 1990 and − 0.22 years in 2019).
Figures 3 and 4 also show that contributions of male NCD helped to narrow the life expectancy gaps in the early period (− 0.15 years in 1990) but significantly widened those gaps in the later period (5.45 years in 2019), because the negative contributions of digestive diseases (− 0.81 years in 1990 and − 0.13 years in 2019) and diabetes and kidney diseases (− 0.16 years in 1990 and − 0.09 years in 2019) offset the positive contribution of cardiovascular diseases (− 0.35 years in 1990 and 3.98 years in 2019) and neoplasm (− 0.07 years in 1990 and 0.65 years in 2019).
Meanwhile, contributions of infectious diseases changed from positive to negative and decreased (1.61 years in 1990 and − 0.003 years in 2019), including maternal and neonatal diseases (0.33 years in 1990 and 0.09 years in 2019). Contributions of injuries saw a similar decline (− 0.42 years in 1990 and − 0.04 years in 2019), including self-harm and interpersonal violence (0.06 years in 1990 and − 0.48 years in 2019). However, those declines cannot offset the widening of life expectancy gap due to the increase in cardiovascular diseases.
3.4 Cause-specific contributions to national life expectancy gap varied by ages

Cause-specific contributions to life expectancy gaps by non-communicable diseases between China and South Korea, varied by ages and gender, 1990, 2000, 2010 and 2019

Cause-specific contributions to life expectancy gaps by infectious diseases between China and South Korea, varied by ages and gender, 1990, 2000, 2010 and 2019

Cause-specific contributions to life expectancy gaps by injuries between China and South Korea, varied by ages and gender, 1990, 2000, 2010 and 2019
Figures 5, 6 and 7 report cause-specific contributions to life expectancy gaps by ages for 3 groups of causes. The positive contributions to female life expectancy gaps can be mainly explained by cardiovascular diseases among the elderly, although the increase of contribution is limited in the later period.
In Fig. 5, among the older age group (60 and above), cardiovascular diseases are the prominent contributors to the life expectancy gaps, but after an explosive increase in 2010, the contribution of cardiovascular diseases began to stabilize (2010: 4.87 years, 2019: 4.80 years). This is because mortality due to cardiovascular disease among elderly Korean women dropped rapidly in 2010 and then slowed down, resulting in a limited increase in life expectancy gap in 2019. Chronic respiratory diseases among the middle-aged (aged 40–64) contributed significantly (1990: 1.81 years) to life expectancy gaps and then decreased gradually with the affected age delayed to aged 65 years and above (2019: 0.88 years). This is because mortality due to chronic respiratory diseases in China has decreased over the period, although still being higher than that in Korea.
In Fig. 6, respiratory infections and tuberculosis contributed a large part among infant group (aged 0–4) in the early stage (1990: 0.91 years, 2000: 0.51 years), and then such impact decreased (2010: 0.13 years, 2019: 0.06 years). Even in as late as 2019, respiratory infections and tuberculosis had a negative contribution among the elderly population (70 and above) (2019: − 0.13 years). Contributions of maternal and neonatal diseases are mainly attributed to the infant (aged under 1), and also decreased over time (1990: 0.23 years, 2019: 0.07years).
In Fig. 7, contributions of self-harm and interpersonal violence among the young and the middle-aged (20–54) expanded the gap in early stages (1990: 0.21 years, 2000: 0.07 years), but narrowed the gap in later stages (2010: − 0.21 years, 2019: − 0.17 years).
Figures 5, 6 and 7 also reveal that the insignificant male life expectancy gap in the early period could mainly be explained by the negative contribution of digestive diseases (1990: − 0.79 years), cardiovascular diseases (1990: − 0.38 years), neoplasm (1990: − 0.15 years) among middle-aged and elderly groups (aged 35–79) and transport injuries among the 5–79 years age group (1990: − 0.54 years) that offset the positive contribution of respiratory infections and tuberculosis among the 0–4 age group (1990: 0.87 years) and maternal and neonatal diseases (1990: 0.34 years) in Fig. 5.
Moreover, positive contribution of cardiovascular diseases (2010: 2.99 years, 2019: 3.59 years) and neoplasm (2010: 0.33 years, 2019: 0.61 years) among the 45–89 age groups increased in the later period and, therefore, further widened the male life expectancy gap. The increasing negative contributions of neoplasm (2019: − 0.13 years), neurological disorders (2019: − 0.09 years), diabetes and kidney diseases (2019: − 0.06 years), respiratory infections and tuberculosis (2019: − 0.12 years) among the elderly (aged 90 and above) and self-harm and interpersonal violence among the 20–90 years old groups (2019: − 0.47 years) cannot offset the increasing positive contributions mentioned above.
4 Discussion
While life expectancy gap between China and Korea has remained rather stable for females from 1990 to 2019, the gap has widened for males over the same time period. This study applies Arriaga’s decomposition method to study the age-specific and cause-specific contributions to life expectancy gap for both genders, revealing the health patterns in high-life expectancy countries by the change of contributions over time.
The results showed that age-specific contributions to widen life expectancy gap have changed from the 0–4 age group in 1990 to 65–89 age groups in 2019 for both genders.
South Korea became a low fertility society earlier than China and has effectively controlled its infant mortality rate (Yang et al., 2010). In consequence the life expectancy gap due to infant mortality remained until 2000. The success is largely attributed to nationwide programs established to promote improved health care for pregnant women, childbirth newborns, and infants (Chang et al., 2011). Moreover, aging in China has intensified in recent decades and the incidence of diseases related to the elderly has increased, while long-term care system hasn’t improved compared to Korea, further widening the life expectancy gap in China and South Korea since 2000.
The significant contribution of the elderly to life expectancy gap is also observed in other research (Chen et al., 2020; Khang & Bahk, 2019). The contributions of the young and middle age groups are negligible, probably because both China and South Korea have entered a state of relatively stable economic development and offer a more secure life with low mortality for both countries in these age groups. In contrast, another study on the life expectancy gap between developed and developing countries shows that gun homicides among middle-aged people aged 20–64 account for most of the gap between Brazil and Canada (Auger et al., 2016).
Between 1990 and 2019, both China and South Korea experienced rapid economic development. China’s GDP per capita increased from $318 to $10,144, while South Korea’s GDP per capita increased from $6610 to $31,902 (World Bank, 2019). However, China’s rapid socio–economic development has not been followed by a corresponding development of its healthcare system compared to Korea (Liu, 2004).
The Korean government has released a series of preventive and supportive policies to better promote infant and child healthcare at an early stage, such as a test for inborn errors of metabolism and care for sick infants, medical expense support for premature and congenitally abnormal newborns, and nationwide support for the installation of neonatal intensive care units (NICUs). Furthermore, since 2007, children’s medical insurance has helped neonates exempt from hospital bills (Chang et al., 2011b). However, China still struggles with issues such as abandoned babies, an underreporting of infant deaths, a significant gap in NICUs with developed countries, and a severe shortage of pediatricians, nurses, midwives, and hospital beds per 10,000 people (Cao et al., 2019; Liu et al., 2018; Xu et al., 2014; Zhang et al., 2019).
Benefiting from rapid GDP growth, Korea had a higher budget for health expenditure. All residents are covered under the national health insurance scheme established in 1989, and the merger of all insurance funds into a unified organizational system in 2000 reduced inequalities in access to health care (Dronina et al., 2016; Kwon, 2009). In contrast, health insurance in China started later and has three different health insurance schemes with disparities between urban and rural residents, including the urban employee-based basic medical insurance scheme (1998), the rural new cooperative medical scheme (2003), and the urban resident basic medical insurance scheme (2007) (Meng et al., 2015). A large number of elderly people are left behind in rural areas of China and do not receive adequate healthcare, making them potential contributors to the life expectancy gap between with Korea (Li et al., 2013; Shi, 1993; Song et al., 2019; Wu et al., 2022; Ying et al., 2020).
In addition, Korea conducted long-term care services since 2008, when the elderly population accounted for only 10% (Kim & Kwon, 2021). An eligibility selection process is established to assess the health status of elderly citizens aged 65 or older or younger than 65 with chronic illnesses or disabilities, and then the long-term care program makes the decision to provide services from the nursing home or long-term care hospital to the receivers (Ga, 2020). Although China had published long-term care services before, such as the Star Light Project (launched in 2001), this latter was not effective because of the high expenditure, the single financing mechanism, and the lack of healthcare labors. (Feng et al., 2020; Wong & Leung, 2012). As a result, long term care for the elderly in China depends on the family, which increases the burden of disease on families and prevents access to better treatments for the elderly (Han et al., 2020).
China may get old before it gets rich (Johnston, 2021). Due to the differentiated pension system between urban and rural areas in China, the annual income of significant portion of the elderly is low, forcing them to work for a living after retiring and exposing them to a higher risk of health deterioration over a longer period of time (Han et al., 2020; Wang, 2006). This makes the role of the elderly even more critical in the life expectancy gap between China and Korea.
The cause-specific contributions to widen the life expectancy gap are dominated by non-communicable diseases, including cardiovascular diseases, chronic respiratory diseases and neoplasms.
Even though China has achieved a great success in controlling mortality by cardiovascular diseases, the rate is still higher than South Korea due to weaker primary health care, poorer long-term health care management (Du et al., 2019) and imbalanced regional economic development (Liu et al., 2010, 2019). Air pollution, associated with China’s growing economy and industrialization, is a prominent risk accounting for the prevalence of cardiovascular diseases (Yang et al., 2019; Yin et al., 2020). China’s continued urbanization has generated a large number of migrant workers from rural areas to urban places, who are accompanied with increased hypertension, BMI and cholesterol, leading to an increasing number of people with coronary heart disease and stroke (Chan et al., 2012; Moran et al., 2010). The lack of physical activity, overweight, obesity, dyslipidemia, metabolic syndrome, diabetes in China and the higher prevalence of smoking are also responsible for cardiovascular diseases (Chen et al., 2020; Ma et al., 2020; Qin et al., 2015). Lifestyle like drinking alcohol contributes to increasing cardiovascular mortality (Grigoriev et al., 2014) while a low intake of fresh fruits will cause higher blood pressure and hyperglycemia, leading to broader prevalence of cardiovascular diseases. Chinese males have even a lower intake than females, and this is why cardiovascular diseases contribute more among male than female (Du et al., 2016).
The contributions of chronic respiratory diseases (CRD) to widen life expectancy gap were rather sustained for nearly thirty years but reduced over time due to the declining mortality rate of chronic obstructive pulmonary disease (COPD), asthma, pneumoconiosis, pulmonary interstitial diseases and pulmonary sarcoidosis (Long et al., 2022) in China. As China has introduced a series of environmental protection policies, including traffic control and new energy, pollutant discharge has declined and CRDs are consequently improved (Wang et al., 2014). However, aging weakens the public’s immunity to viruses or bacteria and, subsequently, increases people’s exposure to CRD (Yang et al., 2022). Aging-related skeletal muscle dysfunction and sarcopenia accompanied with COPD also exacerbate death (Cruz-Jentoft et al., 2010). In short, aging is a non-negligible reason for the high level of CRDs in China.
Neoplasm-related factors helped narrow the male life expectancy gap before 2010 but widened the gap for both genders in the later period and widen female life expectancy gap for the whole period. Lung cancer, stomach cancer, liver cancer and colorectal cancer are the most serious neoplasm in China and Korea, which are strongly connected with lifestyle and dietary habits (Zhu et al., 2019; Shin et al., 2018). Although liver cancer mortality of males in South Korea was higher than that in China after 2000, a possible reason for the life expectancy gap shifting from narrowing to widening is that the lung cancer and stomach cancer mortality rates of males in China have surpassed those in South Korea since 2000 (GBD, 2020). The relatively lower mortality of lung cancer and stomach cancer in South Korea indicated the effectiveness of screening and tobacco control (Chang et al., 2019; Choi et al., 2007; Park & Jang, 2016; Sun et al., 2020; Yang et al., 1999). In 2018, China had a lower incidence rate of stomach and colorectal cancer than South Korea, but a higher mortality rate. Liver and lung cancers in China also produced higher mortality than South Korea in 2018 (Sun et al., 2020), because higher screening rates helps South Korea to detect cancer in a timely manner to control mortality (Suh et al., 2016). Moreover, the risk factors still exist and widen the life expectancy gap in the later period, including longer sitting time, saturated fat intake, less physical activity and drinking (Ji et al., 1998; Whittemore et al., 1990; Wu et al., 2006).
The contributions of infectious diseases have significantly declined and there is a trend towards narrowing the life expectancy gap. The reductions in contributions of maternal and neonatal disorders among babies of 0–4 years old is attributed to family planning, immunization and nutritional support promoted by the Chinese government for maternal and child health care (Xu et al., 2014). Since China’s fertility is on a decline, the reductions in contributions of infectious diseases among 0–4-year-old is limited in the later period. China has trouble with high tuberculosis for decades and the occurrence of tuberculosis is uneven across 31 provinces (Guo et al., 2017; Tang et al., 2011). Therefore, a 10-year-long infectious and endemic disease control project has been launched by the Chinese government that successfully controlled the corresponding mortality rate, which helps to narrow the life expectancy gap (Zhang & Wilson, 2012). Moreover, concentration of tuberculosis in South Korea shifted from the middle-aged group to the elderly (Kim & Yim, 2015; Park et al., 2013), leading to negative contributions of respiratory infections and tuberculosis among the elderly.
Injuries account only for a slight proportion of life expectancy gap between the two countries, but such mortality shows different social issues. With earlier industrialization and more motor vehicles than China, Korea traffic injuries contributed negatively to the life expectancy gap before 2010. However, China’s traffic injuries become more serious as its economy grew in the later period (Wang et al., 2019). Self-harm and interpersonal violence bring an increasing contribution to narrow life expectancy gap, which is driven by South Korea and requires our vigilance. A spatial and temporal study has found that there is an increasing suicide rate in Korea, which attributes to divorce rates, unemployment and house prices (Yeom, 2021). The Young and middle age groups have higher suicide rates due to credit card crisis and rising unemployment (Jung-Choi et al., 2014). Social changes bring injuries to both countries. Given the fact that China might follow similar footsteps in its social development, the government should prevent self-harm and interpersonal violence from growing in the future.
This study shows the life expectancy gap between two high life expectancy countries. Under similar social context, aging is a prominent factor worsening diseases burden. Therefore, the Chinese government should promote more long-term health care management and provide medical health insurance for the elderly. In addition, it is also essential to set up early detection mechanisms for chronic diseases to prevent their prevalence.
This study also has several limitations: first, as previous studies have mentioned, Arriaga’s decomposition method underestimates the contributions among the old (Wu et al., 2022); second, the range of the diseases being not exact enough, since the cardiovascular diseases account for the most contributions, the current study should be focused more on the subdivisions of cardiovascular disease; last but not least, this study did not considered calculating the completeness of death data, since the underreporting of death problems is serious in developing countries. (Chisumpa & Odimegwu, 2018). The data in this study are based on secondary estimated data, and there are differences in data collection between Korea and China. The Korean estimates are based on complete registration, while the Chinese estimates are based on sample registration or other unspecified source.
5 Conclusion
This study reveals the age-specific and cause-specific contributions to the life expectancy gap between South Korea and China, both with a comparatively high life expectancy on the global level. Since these two countries have experienced epidemiological transition, NCDs (especially CVD) among the elderly account for a significant proportion of the life expectancy gap in recent years and will probably continue for years in the future.
The Chinese government has promoted regulatory policies and medical health care to improve specific issues like air pollution, childhood diseases and traffic accident. However, aging-related diseases require long-term management, early screening and more medical insurance to support the elderly and ease the burden of their family. At the same time, lifestyles (smoking, drinking and lack of psychical activities) and dietary habits (excessive fat intake and over-salty cooking), which jeopardize people’s health when they get old, should be optimized under the context of aging in China. Last but not least, taking South Korea as a preceding example, the Chinese government needs to be alert for social issues and prevent suicide from becoming a new demographic public health problem at the end of its epidemiological transition.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Acosta, E., Mehta, N., Myrskylä, M., & Ebeling, M. (2022). Cardiovascular mortality gap between the united states and other high life expectancy countries in 2000–2016. The Journals of Gerontology: Series B, 77(Supplement_2), S148–S157. https://doi.org/10.1093/geronb/gbac032
Adair, T., Kippen, R., Naghavi, M., & Lopez, A. D. (2019). The setting of the rising sun? A recent comparative history of life expectancy trends in Japan and Australia. PLOS ONE, 14(3), e0214578. https://doi.org/10.1371/journal.pone.0214578.
Arriaga, E. E. (1984). Measuring and explaining the change in life expectancies. Demography, 21(1), 83–96. https://doi.org/10.2307/2061029.
Auger, N., Feuillet, P., Martel, S., Lo, E., Barry, A. D., & Harper, S. (2014). Mortality inequality in populations with equal life expectancy: Arriaga’s decomposition method in SAS, Stata, and Excel. Annals of Epidemiology, 24(8), 575–580e1. https://doi.org/10.1016/j.annepidem.2014.05.006.
Auger, N., Le Serbon, E., Rasella, D., Aquino, R., & Barreto, M. L. (2016). Impact of homicide and traffic crashes on life expectancy in the largest latin American country. Journal of Public Health, 38(3), 467–473. https://doi.org/10.1093/pubmed/fdv111
Bahk, J., & Jung-Choi, K. (2020). The contribution of avoidable mortality to the Life expectancy gains in Korea between 1998 and 2017. International Journal of Environmental Research and Public Health. https://doi.org/10.3390/ijerph17186499
Beltrán-Sánchez, H., Preston, S. H., & Canudas-Romo, V. (2008). An integrated approach to cause-of-death analysis: Cause-deleted life tables and decompositions of life expectancy. Demographic Research, 19, 1323. https://doi.org/10.4054/DemRes.2008.19.35.
Cao, Y., Jiang, S., & Zhou, Q. (2019). Introducing evidence-based practice improvement in chinese neonatal intensive care units. Translational Pediatrics, 8(3), 257–261. https://doi.org/10.21037/tp.2019.07.07.
Chan, F., Adamo, S., Coxson, P., Goldman, L., Gu, D., Zhao, D., Chen, C. S., He, J., Mara, V., & Moran, A. (2012). Projected impact of urbanization on cardiovascular disease in china. International Journal of Public Health, 57(5), 849–854. https://doi.org/10.1007/s00038-012-0400-y.
Chang, J-Y., Lee, K. S., Hahn, W-H., Chung, S-H., Choi, Y-S., Shim, K. S., & Bae, C-W. (2011). Decreasing Trends of neonatal and infant mortality rates in Korea: Compared with Japan, USA, and nations, O. E. C. D. Journal of Korean Medical Science, 26(9), 1115–1123. https://doi.org/10.3346/jkms.2011.26.9.1115.
Chang, Y., Kang, H. Y., Lim, D., Cho, H. J., & Khang, Y. H. (2019). Long-term trends in smoking prevalence and its socioeconomic inequalities in Korea, 1992–2016. International Journal for Equity in Health, 18(1), 148. https://doi.org/10.1186/s12939-019-1051-x.
Chen, H., Qian, Y., Dong, Y., Yang, Z., Guo, L., Liu, J., Shen, Q., & Wang, L. (2020). Patterns and changes in life expectancy in China, 1990–2016. PLOS ONE, 15(4), e0231007. https://doi.org/10.1371/journal.pone.0231007.
Chisumpa, V. H., & Odimegwu, C. O. (2018). Decomposition of age- and cause-specific adult mortality contributions to the gender gap in life expectancy from census and survey data in Zambia. SSM - Population Health, 5, 218–226. https://doi.org/10.1016/j.ssmph.2018.07.003.
Choi, Y., Kim, Y., Hong, Y. C., Park, S. K., & Yoo, K. Y. (2007). Temporal changes of lung cancer mortality in Korea. Journal of Korean Medical Science, 22(3), 524–528. https://doi.org/10.3346/jkms.2007.22.3.524
Cruz-Jentoft, A. J., Baeyens, J. P., Bauer, J. M., Boirie, Y., Cederholm, T., Landi, F., Martin, F. C., Michel, J. P., Rolland, Y., Schneider, S. M., Topinková, E., Vandewoude, M., & Zamboni, M. (2010). Sarcopenia: European consensus on definition and diagnosis: Report of the European working group on Sarcopenia in older people. Age and Ageing, 39(4), 412–423. https://doi.org/10.1093/ageing/afq034
Dronina, Y., Yoon, Y. M., Sakamaki, H., & Nam, E. W. (2016). Health system development and performance in Korea and Japan: A comparative study of 2000–2013. Journal of Lifestyle Medicine, 6(1), 16–26. https://doi.org/10.15280/jlm.2016.6.1.16
Du, H., Li, L., Bennett, D., Guo, Y., Key, T. J., Bian, Z., Sherliker, P., Gao, H., Chen, Y., Yang, L., Chen, J., Wang, S., Du, R., Su, H., Collins, R., Peto, R., & Chen, Z. (2016). Fresh fruit consumption and major cardiovascular disease in China. New England Journal of Medicine, 374(14), 1332–1343. https://doi.org/10.1056/NEJMoa1501451
Du, X., Patel, A., Anderson, C. S., Dong, J., & Ma, C. (2019). Epidemiology of cardiovascular disease in China and opportunities for improvement: JACC international. Journal of the American College of Cardiology, 73(24), 3135–3147. https://doi.org/10.1016/j.jacc.2019.04.036
Ebenstein, A., Fan, M., Greenstone, M., He, G., Yin, P., & Zhou, M. (2015). Growth, pollution, and life expectancy: China from 1991–2012. American Economic Review, 105(5), 226–231. https://doi.org/10.1257/aer.p20151094
Fan, J. G., Kim, S. U., & Wong, V. W. S. (2017). New trends on obesity and NAFLD in Asia. Journal of Hepatology, 67(4), 862–873. https://doi.org/10.1016/j.jhep.2017.06.003.
Feng, Q., Son, J., & Zeng, Y. (2015). Prevalence and correlates of successful ageing: A comparative study between China and South Korea. European Journal of Ageing, 12(2), 83–94. https://doi.org/10.1007/s10433-014-0329-5.
Feng, Z., Glinskaya, E., Chen, H., Gong, S., Qiu, Y., Xu, J., & Yip, W. (2020). Long-term care system for older adults in China: Policy landscape, challenges, and future prospects. The Lancet, 396(10259), 1362–1372. https://doi.org/10.1016/S0140-6736(20)32136-X.
Ga, H. (2020). Long-term care system in Korea. Annals of Geriatric Medicine and Research, 24(3), 181–186. https://doi.org/10.4235/agmr.20.0036
Grigoriev, P., Meslé, F., Shkolnikov, V. M., Andreev, E., Fihel, A., Pechholdova, M., & Vallin, J. (2014). The recent mortality decline in Russia: Beginning of the cardiovascular revolution? Population and Development Review, 40(1), 107–129. https://doi.org/10.1111/j.1728-4457.2014.00652.x
Guo, C., Du, Y., Shen, S. Q., Lao, X. Q., Qian, J., & Ou, C. Q. (2017). Spatiotemporal analysis of tuberculosis incidence and its associated factors in mainland China. Epidemiology & Infection, 145(12), 2510–2519. https://doi.org/10.1017/S0950268817001133.
Han, Y., He, Y., Lyu, J., Yu, C., Bian, M., & Lee, L. (2020). Aging in China: Perspectives on public health. Global Health Journal, 4(1), 11–17. https://doi.org/10.1016/j.glohj.2020.01.002.
Ho, J. Y., & Hendi, A. S. (2018). Recent trends in life expectancy across high income countries: Retrospective observational study. The BMJ, 362, k2562. https://doi.org/10.1136/bmj.k2562
Ji, B. T., Chow, W. H., Yang, G., McLaughlin, J. K., Zheng, W., Shu, X. O., Jin, F., Gao, R. N., Gao, Y. T., & Fraumeni, F. Jr., J (1998). Dietary habits and stomach cancer in Shanghai, China. International Journal of Cancer, 76(5), 659–664.
Johnston, L. A. (2021). Getting old before getting rich”: Origins and policy responses in China. China: An International Journal, 19(3), 91–111. https://doi.org/10.1353/chn.2021.0030
Jones, G. W. (2019). Ultra-low fertility in East Asia: Policy responses and challenges. Asian Population Studies, 15(2), 131–149. https://doi.org/10.1080/17441730.2019.1594656.
Jung-Choi, K., Khang, Y. H., Cho, H. J., et al. (2014). Decomposition of educational differences in life expectancy by age and causes of death among South Korean adults. BMC Public Health, 14, 560. https://doi.org/10.1186/1471-2458-14-560.
Khang, Y. H., & Bahk, J. (2019). Why is life expectancy in Busan shorter than in Seoul? Age and cause-specific contributions to the difference in life expectancy between two cities. Yonsei Medical Journal, 60(7), 687–693. https://doi.org/10.3349/ymj.2019.60.7.687
Kim, H., & Kwon, S. (2021). A decade of public long-term care insurance in South Korea: Policy lessons for aging countries. Health Policy, 125(1), 22–26. https://doi.org/10.1016/j.healthpol.2020.11.003.
Kim, J. H., & Yim, J. J. (2015). Achievements in and challenges of tuberculosis control in South Korea. Emerging Infectious Diseases, 21(11), 1913–1920. https://doi.org/10.3201/eid2111.141894
Kim, W., Huh, M. Y., Lee, S. P., & Shin, H. K. (2019). A study of healthcare management and technology in Asia: Focused analysis on South Korea, China and Japan. The Journal of Industrial Distribution & Business, 10(3), 17–23. https://doi.org/10.13106/ijidb.2019.vol10.no3.17
Kim, T., Bahk, J., Lim, H. K., & Khang, Y. H. (2020). Stagnation of life expectancy in Korea in 2018: A cause-specific decomposition analysis. PLOS ONE, 15(12), e0244380. https://doi.org/10.1371/journal.pone.0244380.
Kim, D., Chen, C., Tysinger, B., Park, S., Chong, M. Z., Wang, L., Zhao, M., Yuan, J. M., Koh, W. P., Yoong, J., Bhattacharya, J., & Eggleston, K. (2021). Smoking, life expectancy, and chronic disease in South Korea, Singapore, and the United States: A microsimulation model. Health Economics, 30(S1), 92–104. https://doi.org/10.1002/hec.3978.
Kontis, V., Bennett, J. E., Mathers, C. D., Li, G., Foreman, K., & Ezzati, M. (2017). Future life expectancy in 35 industrialised countries: Projections with a bayesian model ensemble. The Lancet, 389(10076), 1323–1335. https://doi.org/10.1016/S0140-6736(16)32381-9.
Kwon, S. (2009). Thirty years of national health insurance in South Korea: Lessons for achieving universal health care coverage. Health Policy and Planning, 24(1), 63–71. https://doi.org/10.1093/heapol/czn037.
Li, M., Zhang, Y., Zhang, Z., Zhang, Y., Zhou, L., & Chen, K. (2013). Rural–Urban differences in the long-term care of the disabled elderly in China. PLOS ONE, 8(11), e79955. https://doi.org/10.1371/journal.pone.0079955
Liang, J., Yamashita, T., & Brown, J. (2013). Leisure satisfaction and quality of life in China, Japan, and South Korea: A comparative study using Asia Barometer 2006. Journal of Happiness Studies. https://doi.org/10.1007/s10902-012-9353-3
Liu, Y. (2004). China’s public health-care system: Facing the challenges. Bulletin of the World Health Organization, 82, 532–538. https://doi.org/10.1590/S0042-96862004000700011.
Liu, J., Chen, G., Chi, I., Wu, J., Pei, L., Song, X., Zhang, L., Pang, L., Han, Y., & Zheng, X. (2010). Regional variations in and correlates of disability–free life expectancy among older adults in China. BMC Public Health, 10(1), 446. https://doi.org/10.1186/1471-2458-10-446
Liu, Y., Yang, L. L., Xu, S. Y., & Zhao, Z. Y. (2018). Pediatrics in China: Challenges and prospects. World Journal of Pediatrics, 14(1), 1–3. https://doi.org/10.1007/s12519-017-0117-3.
Liu, S., Li, Y., Zeng, X., Wang, H., Yin, P., Wang, L., Liu, Y., Liu, J., Qi, J., Ran, S., Yang, S., & Zhou, M. (2019). Burden of cardiovascular diseases in China, 1990–2016: Findings from the 2016 global burden of disease study. JAMA Cardiology, 4(4), 342–352. https://doi.org/10.1001/jamacardio.2019.0295
Long, Z., Liu, W., Qi, J. L., Liu, Y. N., Liu, J. M., You, J. L., Lin, L., Wang, L. J., Zhou, M. G., & Yin, P. (2022). Mortality trend of chronic respiratory diseases in China, 1990–2019. Zhonghua liu xing bing xue za zhi = Zhonghua liuxingbingxue zazhi, 43(1), 14–21. https://doi.org/10.3760/cma.j.cn112338-20210601-00443
Ma, L. Y., Chen, W. W., Gao, R. L., Liu, L. S., Zhu, M. L., Wang, Y. J., Wu, Z. S., Li, H. J., Gu, D. F., Yang, Y. J., Zheng, Z., & Hu, S. S. (2020). China cardiovascular diseases report 2018: An updated summary. Journal of Geriatric Cardiology: JGC, 17(1), 1–8. https://doi.org/10.11909/j.issn.1671-5411.2020.01.001.
Mehregan, M., Khosravi, A., Farhadian, M., & Mohammadi, Y. (2022). The age and cause decomposition of inequality in life expectancy between iranian provinces: Application of arriaga method. BMC Public Health, 22(1), 772. https://doi.org/10.1186/s12889-022-13092-1
Meng, Q., Fang, H., Liu, X., Yuan, B., & Xu, J. (2015). Consolidating the social health insurance schemes in China: Towards an equitable and efficient health system. The Lancet, 386(10002), 1484–1492. https://doi.org/10.1016/S0140-6736(15)00342-6.
Moran, A., Gu, D., Zhao, D., Coxson, P., Wang, Y. C., Chen, C.-S., Liu, J., Cheng, J., Bibbins-Domingo, K., Shen, Y.-M., He, J., & Goldman, L. (2010). Future cardiovascular disease in China. Circulation: Cardiovascular Quality and Outcomes, 3(3), 243–252. https://doi.org/10.1161/CIRCOUTCOMES.109.910711
Nam, K. C., Jo, C., & Lee, M. (2010). Meat products and consumption culture in the East. Meat Science, 86(1), 95–102. https://doi.org/10.1016/j.meatsci.2010.04.026.
Park, J. Y., & Jang, S. H. (2016). Epidemiology of lung cancer in Korea: Recent trends. Tuberculosis and Respiratory Diseases, 79(2), 58–69. https://doi.org/10.4046/trd.2016.79.2.58
Park, Y. K., Park, Y. S., Na, K. I., Cho, E. H., Shin, S. S., & Kim, H. J. (2013). Increased tuberculosis Burden due to demographic transition in Korea from 2001 to 2010. Tuberculosis and Respiratory Diseases, 74(3), 104. https://doi.org/10.4046/trd.2013.74.3.104.
Qin, X. D., Qian, Z., Vaughn, M. G., Trevathan, E., Emo, B., Paul, G., Ren, W. H., Hao, Y. T., & Dong, G. H. (2015). Gender-specific differences of interaction between obesity and air pollution on stroke and cardiovascular diseases in chinese adults from a high pollution range area: A large population based cross sectional study. Science of The Total Environment, 529, 243–248. https://doi.org/10.1016/j.scitotenv.2015.05.041.
Riddell, C. A., Morrison, K. T., Kaufman, J. S., & Harper, S. (2018). Trends in the contribution of major causes of death to the black–white life expectancy gap by US state. Health & Place, 52, 85–100. https://doi.org/10.1016/j.healthplace.2018.04.003
Shi, L. (1993). Health care in China: A rural–urban comparison after the socio–economic reforms. Bulletin of the World Health Organization, 71(6), 723–736.
Shin, H. Y., Lee, J. Y., Kim, J. E., Lee, S., Youn, H., Kim, H., Lee, J., Park, M. S., & Huh, S. (2018). Cause-of-death statistics in 2016 in the Republic of Korea. Journal of the Korean Medical Association, 61(9), 573–584. https://doi.org/10.5124/jkma.2018.61.9.573.
Song, S., Yuan, B., Zhang, L., Cheng, G., Zhu, W., Hou, Z., He, L., Ma, X., & Meng, Q. (2019). Increased inequalities in health resource and access to health care in Rural China. International Journal of Environmental Research and Public Health. https://doi.org/10.3390/ijerph16010049
Suh, M., Song, S., Cho, H. N., Park, B., Jun, J. K., Choi, E., Kim, Y., & Choi, K. S. (2016). Trends in participation rates for the national cancer screening program in Korea, 2002–2012. Cancer Research and Treatment: Official Journal of Korean Cancer Association, 49(3), 798–806. https://doi.org/10.4143/crt.2016.186
Summoogum, J. P., & Fah, B. C. Y. (2016). A comparative study analysing the demographic and economic factors affecting life expectancy among developed and developing countries in Asia. Asian Development Policy Review, 4(4), 100–110. https://doi.org/10.18488/journal.107/2016.4.4/107.4.100.110.
Sun, D., Cao, M., Li, H., He, S., & Chen, W. (2020a). Cancer burden and trends in China: A review and comparison with Japan and South Korea. Chinese Journal of Cancer Research, 32(2), 129–139. https://doi.org/10.21147/j.issn.1000-9604.2020.02.01.
Tang, S., Zhang, Q., Yu, J., Liu, Y., Sha, W., Sun, H., Fan, L., Gu, J., Hao, X., Yao, L., & Xiao, H. (2011). Extensively drug-resistant tuberculosis, China. Emerging Infectious Diseases, 17(3), 558–560. https://doi.org/10.3201/eid1703.100919.
Wang, D., & China. (2006). & World Economy, 14(1), 102–116. https://doi.org/10.1111/j.1749-124X.2006.00001.x
Wang, S., Xing, J., Zhao, B., Jang, C., & Hao, J. (2014). Effectiveness of national air pollution control policies on the air quality in metropolitan areas of China. Journal of Environmental Sciences, 26(1), 13–22. https://doi.org/10.1016/S1001-0742(13)60381-2.
Wang, X., Yu, H., Nie, C., Zhou, Y., Wang, H., & Shi, X. (2019). Road traffic injuries in China from 2007 to 2016: The epidemiological characteristics, trends and influencing factors. PeerJ, 7, e7423. https://doi.org/10.7717/peerj.7423.
Whittemore, A. S., Wu-Williams, A. H., Lee, M., Shu, Z., Gallagher, R. P., Deng-ao, J., Lun, Z., Xianghui, W., Kun, C., Jung, D., Teh, C. Z., Chengde, L., Yao, X. J., Paffenbarger, R. S., Jr., & Henderson, B. E. (1990). Diet, physical activity, and colorectal cancer among Chinese in North America and China. JNCI: Journal of the National Cancer Institute, 82(11), 915–926. https://doi.org/10.1093/jnci/82.11.915
Wong, Y. C., & Leung, J. (2012). Long-term care in China: Issues and prospects. Journal of Gerontological Social Work, 55(7), 570–586. https://doi.org/10.1080/01634372.2011.650319.
Wu, M., Zhao, J. K., Hu, X. S., Wang, P. H., Qin, Y., Lu, Y. C., Yang, J., Liu, A. M., Wu, D. L., Zhang, Z. F., Frans, K. J., & van’t Veer, P. (2006). Association of smoking, alcohol drinking and dietary factors with esophageal cancer in high-and low-risk areas of Jiangsu province, China. World Journal of Gastroenterology: WJG, 12(11), 1686–1693. https://doi.org/10.3748/wjg.v12.i11.1686
Wu, J., KC, S., & Luy, M. (2022). The gender gap in life expectancy in urban and rural China, 2013–2018. Frontiers in Public Health, 10, 749238. https://doi.org/10.3389/fpubh.2022.749238
Xu, Y., Zhang, W., Yang, R., Zou, C., & Zhao, Z. (2014). Infant mortality and life expectancy in China. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research, 20, 379–385. https://doi.org/10.12659/MSM.890204.
Yang, G., Fan, L., Tan, J., Qi, G., Zhang, Y., Samet, J. M., Taylor, C. E., Becker, K., & Xu, J. (1999). Smoking in China findings of the 1996 national prevalence survey. Journal of The American Medical Association, 282(13), 1247–1253. https://doi.org/10.1001/jama.282.13.1247
Yang, S., Khang, Y. H., Harper, S., Davey Smith, G., Leon, D. A., & Lynch, J. (2010). Understanding the rapid increase in life expectancy in South Korea. American Journal of Public Health, 100(5), 896–903. https://doi.org/10.2105/AJPH.2009.160341
Yang, S., Khang, Y. H., Chun, H., Harper, S., & Lynch, J. (2012). The changing gender differences in life expectancy in Korea 1970–2005. Social Science & Medicine, 75(7), 1280–1287. https://doi.org/10.1016/j.socscimed.2012.04.026.
Yang, D., Li, K., Chua, M., Song, D., Bai, Y., & Powell, C. A. (2022). Application of internet of things in chronic respiratory disease prevention, diagnosis, treatment and management. Clinical eHealth, 5, 10–16. https://doi.org/10.1016/j.ceh.2021.08.001
Yeom, Y. (2021). Analysing spatial and temporal dynamics of suicide in South Korea: An application of the dynamic spatial panel data model. Geospatial Health. https://doi.org/10.4081/gh.2021.964
Yin, P., Brauer, M., Cohen, A. J., Wang, H., Li, J., Burnett, R. T., Stanaway, J. D., Causey, K., Larson, S., Godwin, W., Frostad, J., Marks, A., Wang, L., Zhou, M., & Murray, C. J. L. (2020). The effect of air pollution on deaths, disease burden, and life expectancy across China and its provinces, 1990–2017: An analysis for the global burden of disease study 2017. The Lancet Planetary Health, 4(9), e386–e398. https://doi.org/10.1016/S2542-5196(20)30161-3
Ying, M., Wang, S., Bai, C., & Li, Y. (2020). Rural–Urban differences in health outcomes, healthcare use, and expenditures among older adults under universal health insurance in China. PLOS ONE, 15(10), e0240194. https://doi.org/10.1371/journal.pone.0240194
Zhang, L., & Wilson, D. P. (2012). Trends in notifiable infectious diseases in China: Implications for surveillance and population health policy. PLOS ONE, 7(2), e31076. https://doi.org/10.1371/journal.pone.0031076
Zhang, H., Bago d’Uva, T., & van Doorslaer, E. (2015). The gender health gap in China: A decomposition analysis. Economics & Human Biology, 18, 13–26. https://doi.org/10.1016/j.ehb.2015.03.001.
Zhang, Y., Huang, L., Zhou, X., Zhang, X., Ke, Z., Wang, Z., Chen, Q., Dong, X., Du, L., Fang, J., Feng, X., Fu, J., He, Z., Huang, G., Huang, S., Ju, X., Gao, L., Li, L., Li, T., & Sun, K. (2019). Characteristics and workload of pediatricians in China. Pediatrics, 144(1), e20183532. https://doi.org/10.1542/peds.2018-3532
Zheng, Y., Chang, Q., & Yip, P. S. F. (2019). Understanding the increase in life expectancy in Hong Kong: Contributions of changes in age-and cause-specific mortality. International Journal of Environmental Research and Public Health. https://doi.org/10.3390/ijerph16111959
Zhu, J., Cui, L., Wang, K., Xie, C., Sun, N., Xu, F., Tang, Q., & Sun, C. (2019). Mortality pattern trends and disparities among chinese from 2004 to 2016. BMC Public Health, 19(1), 780. https://doi.org/10.1186/s12889-019-7163-9
Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019). Results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME) (2020). Available online at: https://vizhub.healthdata.org/gbd-results/ (accessed May, 2023).
World Bank (2019). World Bank Open Data [Data set]. https://data.worldbank.org
World Bank national accounts data, and OECD National Accounts data files (2021). https://data.worldbank.org/indicator/NY.GDP.MKTP.CD. Accessed May 2023
Yang, B. Y., Guo, Y., Markevych, I., Qian, Z.(Min)., Bloom, M. S., Heinrich, J., Dharmage, S. C., Rolling, C. A., Jordan, S. S., Komppula, M., Leskinen, A., Bowatte, G., Li, S., Chen, G., Liu, K. K., Zeng, X. W., Hu, L. W., & Dong, G. H. (2019). Association of Long-term Exposure to Ambient Air Pollutants With Risk Factors for Cardiovascular Disease in China. JAMA Network Open, 2(3), e190318
Acknowledgements
Thanks for the population data from the Department of Economic and Social Affairs Population Division of The United Nations. Thanks for the cause-specific mortality data from Institute for Health Metrics and Evaluation. The author gratefully acknowledges Dr Jinjing Wu from Asian Demographic Research Institute for guidance.
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lyu, S., Chen, C. & Marois, G. Contributions by age and cause to life expectancy gap between China and South Korea, 1990–2019: a decomposition analysis. China popul. dev. stud. 7, 160–180 (2023). https://doi.org/10.1007/s42379-023-00134-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42379-023-00134-3