
Abstract
Illicit drug use is a critical and challenging issue globally, but there is a lack of thorough understanding of the underlying mechanisms of drug use, which is essential for policy interventions, in many threatened places. This study aims to explore the socioeconomic determinants of drug use to support policy design in Hong Kong and other regions with similar issues. Multiple linear regression models and fixed-effects models are employed to examine the socioeconomic determinants of drug use based on the most comprehensive data on drug use and population in Hong Kong from 1991 to 2016. The estimates show that demographic and socioeconomic characteristics are important predictors of illicit drug use. The highest rate of drug use is observed for people aged between 20 and 30, as well as for those with primary education. Compared with males, the female drug use rate is 15 (or 46) per 10,000 people lower for the newly (or previously) addicted cases. A 10% increase in monthly income is associated with a 14% drop in drug use rate at the district level. The average annual expenditure on drug use is USD 32.6 million in Hong Kong. Drug policies shall pay more attention to these at-risk groups, and shall consider more financial support to lower the drug use rates.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Illicit drug use imposes substantial costs on the individuals and society, including health damages, labor and wage losses, drug-related violence and crimes, widely in both developed and developing countries (Deykin et al. 1987; Dobkin and Nicosia 2009; Lin 2010; Liu et al. 2006; Martikainen et al. 2018; McGrath and Chan 2005; Nutt et al. 2007; Shek et al. 2011; Smith et al. 2019). Tackling drug use is universally challenging due to addiction and huge profits of drug supply. Recently, there is a growing trend in drug production in regions such as Golden Triangle in Southeast Asia,Footnote 1 and recreational drug use is decriminalized in parts of North America,Footnote 2 potentially affecting a large population worldwide.
A clear and up-to-date understanding of drug use patterns and changes by sub-population is critical for health and social care policy targeted at reducing drug use and catering for varying needs of different groups (Arat et al. 2016; Botvin 2000; Chein et al. 1964; McHugh et al. 2015; Pollack et al. 2002; Quinn 2010). An extensive literature has explored the causes of drug use and its interventions, including the roles of economic activity, education, drug and alcohol prices, legislation, law enforcement and rehabilitation programs (Bachman et al. 2007; Becker and Murphy 1988; Botvin et al. 1995; Caetano et al. 2018; Chu 2014; Corman and Mocan 2000; DiNardo and Lemieux 2001; Deng et al. 2007; DeSimone and Farrelly 2003; Järvinen 2017; Kerrison 2018; Schuermeyer et al. 2014; Williams 2004). Still, observations are limited and insufficient for evidence-based policymaking in many regions. In particular, evidence on the relationship between socioeconomic conditions and drug use is mixed worldwide (Long et al. 2014; Saffer and Chaloupka 1999), and the relationship is empirically unclear in Hong Kong. Hong Kong connects the Golden Triangle with international markets of illicit drugs, and has been facing threats for decades. Despite the overall decline in reported drug use cases in recent years, challenges remain in identifying at-risk groups and local determinants of drug use (Census and Statistics Department 2016; Cheung and Ch’ien 1996; Wu et al. 2014). Previous studies focused on the characteristics of drug users using limited survey data (Abdullah et al. 2002; Cheung and Cheung 2006; Loxton et al. 2008; Tse et al. 2016), or explored the trends in the number of drug users (Cheung and Cheung 2018; Joe Laidler 2005). However, given the rapidly ageing population in Hong Kong, such quantitative analyses shall take into account the changes in population over time (which received little attention) to consistently measure and compare drug use rate by population besides the absolute numbers (Kandel 1991).
This paper is among the first to quantitatively examine the relationship between drug use rate and various demographic and socioeconomic factors in Hong Kong. We exploit the most representative data on drug users in Hong Kong for a long period from 1991 to 2016, allowing us to examine the historical and latest changes in drug use. Importantly, we take into account the population changes (such as population ageing) in the long run, which have been overlooked in the academic literature, social policy and practice. We first construct drug use rates by various categories such as age, gender, education and district. Then, we exploit multiple linear regression models to quantify the differentials in drug use by demographic and socioeconomic factors. We further estimate the cost of drug use by drug expenditure. The study can help understand the situation, trends and determinants of drug use over time and space, which is crucial for improving targeted interventions on drug use and further protecting public health and improving social welfare in Hong Kong. The analyses and findings can also contribute to the literature on drug use with novel evidence from Hong Kong, which provides reference for other regions with similar issues in population ageing and illicit drug use.
2 Materials and methods
2.1 Data
2.1.1 Drug use
The drug use data were provided by Central Registry of Drug Abuse (CRDA) in Hong Kong (Wat 1985). Drug use is defined as the taking of substance that harms or threatens to harm the physical, mental or social wellbeing of an individual, in doses above or for periods beyond those normally regarded as therapeutic (Census and Statistics Department 2016). Reporting agencies in the CRDA system include governmental departments (such as the police, hospitals, correctional services, etc.), non-government organizations (NGOs, such as Drug Treatment and Rehabilitation Centres, Counselling Centres for Psychotropic Substance Abusers, Centres for Drug Counselling, etc.), and schools. The information collected includes demographics (such as age, gender, education, economic activity, district of residence) and type of drugs used by each drug user.Footnote 3 CRDA assigns a case number to each drug user, whom can be reported multiple times over time and space. In total, there were 666,665 cases from 98,016 drug users reported during 1991–2016 in Hong Kong.
A universal concern with all the studies on drug use is the potential underreporting of drug-abusing population. Nevertheless, the underreporting ratio in CRDA is expected to be lower than 10% (Narcotics Division 2011). The CRDA data is also consistent with alternative data sources and approaches such as school surveys and the capture-recapture method (Narcotics Division 2013). Recent scientific studies using wastewater to measure drug use also find consistent patterns with the CRDA data in Hong Kong (Lai et al. 2013). In addition, we assume no bias in underreporting of particular groups in the CRDA, since there is no relevant evidence on it. Therefore, it presumably will not alter the coefficients from linear regression models. In general, CRDA data is representative of the overall drug use situation in Hong Kong.
2.1.2 Census
The Hong Kong Census data cover 5% of the population every 5 years. Our census data overlap with the CRDA data from 1991 to 2016, and report key demographic and socioeconomic characteristics similarly. Since the information on district of residence was unavailable in 1991 due to confidentiality concerns, our analysis on the drug use rate by district is focused on the period 1996–2016.
2.2 Construction of drug use rate
We compare the number of drug users with the population data, the latter of which were interpolated linearly in-between each census point to obtain annual estimates of population in Hong Kong during 1991–2016. The population data were then matched with CRDA drug use data by demographic characteristics (age, gender, education, residence) in each year, allowing for calculating the rate of drug use by these specific groups. We then examine the changes in rates of drug use for each group or stratification.
It is worth noting that both the absolute number and rate of drug use are important from the perspectives of social policy and welfare. The number measures the overall severity of drug use, whereas the rate reveals the relative severity of drug use across different groups, thus is more suitable for consistent comparison over time and space.
2.3 Multiple linear regression
Our empirical analysis is built on the pre-existing theoretical framework on illicit drug use that is well-established in the literature. In particular, Becker and Murphy (1988) and Becker et al. (2004) developed theoretical models on addiction and demand of illicit drugs, which maximize individual’s utility as a function of consumption of normal goods and drugs, subject to expenditure constraints over the life cycle. We follow the framework and define the drug use decision of individual i at time t as a function of socioeconomic conditions \({E}_{it}\), and demographics \({D}_{it}\) as follows:
The model shows that levels of income, stress, and the discount rate can affect the likelihood of becoming addicted. For instance, illicit drugs are relatively cheaper to the poor due to easier access to drugs, higher probability of involvement in trafficking, and lower opportunity costs. However, as aforementioned, the empirical evidence is mixed, and the relationship between drug use and socioeconomic conditions and demographics are unclear in Hong Kong.
2.3.1 Demographic determinants
In order to explore how the drug use rate differs by demographics such as age, gender and education, we employ the following equation:
where \({Y}_{it}\) is the rate of drug use in group i in year t.\({Age}_{it}\), \({Gender}_{it}\) and \({Edu}_{it}\) denote the age, gender and educational attainment of group i. Specifically, \({Age}_{it}\) includes 10-year bins of age by [0, 10), [10, 20), [20, 30), [30, 40), [40, 50), [50, 60), [60, 70), and [70,). The age group between 0 and 10 years old is used as the reference group, since they are unlikely to take illicit drugs as shown by the drug use data. Therefore, the vector \({\beta }_{0}\) captures the relative difference in drug use rate between each age group and the reference group (which is zero). \({\beta }_{1}\) reveals the gender difference between males and females using males as the reference group. Similarly, \({Edu}_{it}\) categorizes educational attainment into five bins: no schooling/kindergarten, primary education, lower secondary education (S1–S3), upper secondary education (S4–S7), and tertiary education. No schooling/kindergarten is the reference group, and \({\beta }_{2}\) reports the difference in drug use rate between group i and the reference group. Since people with no schooling/kindergarten are more likely to take illicit drugs than other groups, we expect \({\beta }_{2}\) to be negative. Lastly, all the coefficients may be different by drug category. Hence, we also report the age differences for each drug category, respectively. \({\alpha }_{0}\) is the intercept, and \({\xi }_{it}\) is the residual term.
2.3.2 Economic determinants
We leverage income information to explore the economic determinants of drug use. Income can be calculated from the monthly earnings reported by each individual in the Census and were aggregated by group. Different from Eq. (1), we construct a panel of drug use rates by district and year. Since we do not have information on people who do not take drugs as counterfactuals, aggregation above the individual level is necessary for analysis. The finest spatial resolution in the CRDA data is by district. Therefore, we calculate the number and rate of drug use at the district-year level. There are 18 districts in Hong Kong, with a large heterogeneity across districts in many aspects, including drug use rate, income and economic structure (as described later).
We estimate the association between income and drug use rate by district as follows:
where \({Y}_{dt}\) is the drug use rate in district d in year t.Footnote 4\({Income}_{dt}\) denotes the monthly average income of residents in district d in year t. \({\beta }_{3}\) is the parameter of interest, which captures the effect of income on drug use rate. \({\tau }_{d}\) denote district fixed effects, which controls for time-invariant factors that are specific to a district (such as natural endowment, economic structures and patterns). It also reports the differences in drug use rate across districts. \({\pi }_{t}\) are the year fixed effects which control for temporal changes that are common to all districts in Hong Kong, such as major changes in the economy, policy and overall drug supply and demand in Hong Kong that affect all the districts at the same time. To allow for temporal autocorrelations, we cluster the standard errors \({\xi }_{dt}\) at the district level.
Equation (2) is a fixed-effects panel regression model, allowing us to explain the income effect and district differences by controlling for much of the unobserved confounders that are either time-invariant and district-specific or common to all districts. Essentially, we are leveraging only within-district variations in income and drug use over different years. Although the fixed-effects models are still likely associational, they can presumably explain a large proportion of the variations in drug use rate. Thus, they can credibly help quantify the relationship between drug use and demographic/socioeconomic factors.
3 Results
3.1 Drug use by district
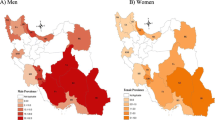
Table 1 reports the numbers, percentage shares, and ratios of drug users by district in Hong Kong in each census year during 1996–2016. We observe both a large number and rate of drug users in districts with higher population densities (including Sham Shui Po and Yau Tsim Mong), but there are notable differences revealed by the two metrics. Although Kwun Tong also has a high share of drug users each year (around 10%), the rate of drug use is almost half of that in Sham Shui Po (16 vs 29 per 10,000 in 2016) due to a much larger population. Therefore, the severity of drug use is much higher in Sham Shui Po. We highlight this difference for policies to allocate more resources to Sham Shui Po than those to Kwun Tong. In addition, drug users are also likely to reside in remote and poorer areas with high criminal records, such as Yuen Lung.Footnote 5 In comparison, the prevalence of drug use is low in commercial regions with financial and real estate industries on the Hong Kong Island, such as Central/Western and Wan Chai. The average wages in these regions are higher than those in Kowloon (including Sham Shui Po and Yau Tsim Mong). For instance, the monthly average incomes in Wan Chai, Sham Shui Po and Yau Tsim Mong are HKD 26,643, 15,171 and 17,237, respectively.
3.2 Reason of drug use
Effective and efficient social policy and interventions require timely and accurate understanding of the reasons behind individual decisions on drug use. One advantage of the CRDA data is that it reports reasons for drug use for each individual since 1996. The main reasons include: curiosity, peer influence, partner influence, relief of boredom/depression/stress, self-medication, to avoid discomfort of its absence, to seek euphoria or sensory satisfaction. Overall, we find that peer influence (30%), curiosity (28%) and discomfort (19%) are the top three reasons for taking illicit drugs. Importantly, the primary reasons behind drug use differ by age. First, curiosity (35%) and peer influence (32%) play a dominant role for drug use among the young people below 30 years old. Second, as the age increases, discomfort becomes a more important driver for drug use decisions. For middle-aged groups between 30 and 60 years old, peer influence (29%) and discomfort (24%) are the main reasons. Notably, the share of relief of boredom/depression/stress for the middle-aged group is higher than those of the young and elderly. This reveals that social pressure and anxiety, which is also likely related with discomfort, may play a significant role in introducing new drug use for the middle-aged people. Third, over 37% of the elderly above 60 takes drugs to relieve discomfort in health. This suggests that the elderly is unlikely to take illicit drugs due to curiosity or pressure. The percentage of reasons for each group are plotted in Fig. 1.

Percentage shares of drug use reasons. The reasons for drug use are shown for the whole population, age 0–30, 30–60 and 60 above in the upper left, upper right, lower left and lower right panel, respectively
The reasons for drug use also vary by educational attainment. The top reasons for no-schooling, primary, lower-secondary, upper-secondary, and tertiary groups are: to avoid discomfort (37%), peer influence (29%), peer influence (31%), peer influence and curiosity (59%), relief of boredom/depression/stress (27%), respectively. In sharp contrast, physical discomfort is the main reason for the no-schooling group, whereas mental depression is the major cause for the well-educated group.
3.3 Gender, age and education
Previous studies observed higher prevalence of illicit drugs among males, the youth and less-educated groups, but the importance of gender, age and education is not quantified in Hong Kong. Table 2 reports our estimates from Eq. (1). Males, age group at 0–10, and people with no schooling are used as the reference groups to compare the differences in drug use over gender, age and education, respectively. Column (1) contains the estimates for all drug users, and columns (2)–(3) differentiate between newly addicted (or drug initiation) and previously addicted cases. On average, the drug use rate of women is lower than that of men by around 60 per 10,000 in Hong Kong. Female drug use rate is nearly 15 people fewer than males for the new-addiction cases, and is 46 people fewer than males for previously addicted cases. All the estimates are statistically significant at the 1% level (p < 0.01).
Age is another key factor of drug use decision. People aged between 20 and 30 have the highest drug use rate over 137 per 10,000, followed by age groups at 30–40, 10–20 and 40–50. The youth at age 10–20 is much more likely to start taking illicit drugs than those older than 30, as shown by column (2). In addition, the last four rows in Table 2 show the differences in drug use rates by educational attainment, conditional on gender and age. The highest rate is observed for people with primary education, which is 17 counts per 10,000 more than those with no schooling. The tertiary group has the lowest drug use rate. There is a negative correlation between education and new drug use in column (2), suggesting that higher education reduces the likelihood of drug use. A plausible explanation is that drug use brings higher private costs to individuals with higher education, such as opportunity and productivity losses.
The drug use rates may also be heterogeneous by different drugs. Table 3 represents the estimates of each demographic factor’s association with drug use rate in each age group. First, the relationship between narcotics analgesics use and age is concave downward, with the largest rates in the age group at 40–50 in column (1). Compared with the age-group below 10 years old with no drug use, the drug use rate of narcotics analgesics is higher by 7 per 10,000 for the youth between 10 and 20 years old. The concave relationship is also found for sedatives/hypnotics in column (5). The use rate of other drugs, including stimulants, depressants, tranquillizers, hallucinogens and ketamine, all reveal monotonically decreasing associations with age. Furthermore, narcotics analgesics are the most popular drugs, with much larger coefficients than many other drugs for each age group. The size of drug use rate among the youth at age 10–20 is also large for stimulants and ketamine, revealing a high popularity of these drugs among the youth. This may be related with the common “misconception” of many drug users that ketamine does less physical harm compared with other drugs, and it is more affordable with lower prices (Joe-Laidler and Hunt 2008).
3.4 Income
Economic status is closely related with drug use decisions, but the relationship can be either positive or negative (e.g., Long et al. 2014; Saffer and Chaloupka 1999). On the one hand, higher incomes may increase consumption of drugs for pleasure, but may also increase investment on health as a normal good and reduce drug use. On the other hand, drug use can dampen work productivity and income. Since drug use and income can affect each other, there is an issue of reverse causality in identifying the effects of income on drug use. Despite the challenges, the drug-income relationship is empirically unclear in Hong Kong. To explore the association between income and drug use, we run the regression in Eq. (2), and report the estimates in Table 4. If we simply regress drug use rate on income, the coefficient is − 0.0015, with a statistical significance lower than 1%. In other words, if monthly income increases by HKD 10,000, the drug use rate will significantly decrease by 15 per 10,000 people in a district. Introducing district fixed effects greatly improved the R-squared (goodness of fit) from 0.27 to 0.88, as shown by columns (1) and (2), and the size of the income coefficient almost doubled. This suggests that the omitted time-invariant spatial differences in drug use can explain a large proportion of drug use variation. Further controlling for year fixed effects yields to similar estimates of the income effect while continuously improving the R-squared to 0.92, as shown by column (3). Our method can explain 92% of the variation in drug use at district level. Hence, we use this as our main specification. The yearly differences estimated in the same regression in column (3) are reported in column (6), with the year 1996 as the reference group. Drug use rates were declining from 1996 to 2016, with a few spikes in 2000–2002 and 2008–2009. In addition, we further differentiate between newly addicted and previously addicted cases in columns (4) and (5). Overall, the estimates in columns (3) to (5) shows that if monthly income increases by HKD 10,000 in a district, the drug use rate will decrease by 22 people per 10,000, among which 9 are newly addicted cases, and 13 are previously reported drug users. However, the estimate is insignificant for the previously reported cases. This suggests that income increase may not directly stop pre-existing drug abusers from continuing using drugs due to addiction. The average drug use rate at the district level is 27 per 10,000, and the average monthly income in a district is HKD 17,147 (USD 2,191). This means that a 10% (or 58%) increase in monthly average income is associated with a 14% (or 82%) drop in drug use rate at the district level.
Table 4 also reports the spatial differences in drug use rates by district conditional on income, with Central/Western as the reference group. If incomes in all districts are at the same level, the highest drug use rate would be in Yau Tsim Mong, which is 12 per 10,000 people higher than that in Sham Shui Po. It is worth noting that Sham Shui Po has the highest observed drug use rate listed in Table 1. These two observations do not contradict each other. Instead, Table 4 serves as the counterfactual of what the drug use rate would be like if the income differences across districts disappear. Moreover, the drug use rate in Yau Tsim Mong is driven by the previously addicted cases, whereas the highest rates of new addiction are in Wan Chai and Central/Western. These spatial differences are related with unobserved time-invariant factors at the district level.
3.5 Cost of drug use
CRDA covers valuable information on the frequency and cost of drug use of each individual since 2006. This information is self-reported by drug users during 2006–2016. On average, each individual takes drugs around 14 times per year. The average annual expense on illicit drugs for an individual is HKD 28,555. The average annual income of an individual is HKD 128,310 during 2006–2016. This means that a drug user can spend at least 22% of income on illicit drugs each year. This is a lower-bound estimate, since the income of drug users is likely lower than other people. In addition, the expense-age relationship follows an inverted-U shape. People aged between 40 and 50 pay the most for drugs, which is around HKD 35,492 per year. A person at 10–20 years old spends HKD 10,649 a year on illicit drugs, and a person at 70–80 years old spends HKD 26,074 a year on illicit drugs. The observed total annual expenditure or cost on drug use is HKD 255 million (USD 32.6 million) in Hong Kong on average. It is worth noting that other costs by drug use, such as health expenditure and labor losses (DeSimone 2002), are difficult to observe and are neglected in the cost calculation.
4 Discussion
Our findings are helpful for governmental and non-governmental programs to allocate resources effectively to target at those most at-risk groups in Hong Kong, such as people with education below the upper secondary level, and the youth below 20 years old using stimulants and ketamine, and the middle-aged using narcotics analgesics. Previous policies primarily focus on the young people and develop education programs to discourage curiosity and peer influence. As Hong Kong is well-known for high social pressure, policies shall focus more on relieving boredom and stress for the middle-age people to prevent drug use at an early stage. As for the elderly, more health programs shall be devoted to reducing the physical discomfort. For the youth aged between 10 and 20, regulations shall be strengthened for stimulants, depressants and ketamine compared with other drugs. In particular, we call for policy attentions to poor families who are likely to reduce drug use if their incomes increase.
There are a few caveats in interpreting the findings. First, there is potential underreporting as mentioned in the data section. Second, we use linear interpolation to construct measures of drug use rate for each year in-between the census points, which may induce measurement error. These potential errors will not bias our estimates largely as long as they are uncorrelated with the characteristics of specific subgroups. This assumption may be violated for the young group, whose drug use may be more underreported than the middle-aged and the elderly. If so, our comparisons between the young and older groups shall be treated with caution, but it will not change our conclusion qualitatively, since the younger group already has a higher rate of drug use than other groups. Third, the multiple linear regression models capture only the average associations between income and drug use. Therefore, our estimates shall be interpreted as the average effects of demographic and socioeconomic determinants on the observed drug use rate in Hong Kong.
5 Conclusion
Understanding the determinants of illicit drug use is crucial for policy interventions. This study explores the demographic and socioeconomic differentials of drug use in Hong Kong during 1991–2016. Using the most comprehensive data on drug use and population in Hong Kong, we isolate the effects of population changes in the long run by constructing rates of drug use by sub-population. We find that drug use is adversely related with education and income levels, and the youth and males have higher drug use rates than their counterparts. The relationships are further quantified for each type of drugs in every Hong Kong district, together with the expenditure on drugs as a lower-bound measure of the costs associated with drug use. The estimates on the relationships and costs can provide reference for cost–benefit analyses of existing and future interventions, and can be used for comparison across regions, which is beyond the scope of this paper.
Our findings call for more diversified social interventions on illicit drug use for different groups in Hong Kong. Besides the continuous efforts in discouraging the youth from drug use, policies shall also pay attention to the other emerging at-risk groups including the middle aged and the less educated, and drug policies are also related with other social issues such as growing social pressure and population ageing. Our findings are very suggestive and serve as one of the first steps for evidence-based policymaking in drug abuse in Hong Kong. More careful research designs are needed for causal evidence to support policy evaluation and recommendation. For instance, more research can be done in the future to evaluate the effectiveness of policy interventions based on comprehensive datasets and analyses for causal inference, and to offer insights into improving policy treatment and social care to discourage illicit drug use in Hong Kong and other regions.
Notes
The most popular drugs are narcotics analgesics (opium, heroin, etc.), stimulants (methamphetamine, cocaine, etc.) and ketamine.
Alternatively, we can also employ a Poisson regression model using the logarithm of number of drug users as the dependent variable with the corresponding population as an offset. The results are consistent with our main specification, and are reported in Appendix Table 5.
References
Abdullah, A. S. M., Fielding, R., & Hedley, A. J. (2002). Patterns of cigarette smoking, alcohol use and other substance use among Chinese university students in Hong Kong. American Journal on Addictions, 11(3), 235–246.
Arat, G., Hoang, A. P., Jordan, L. P., & Wong, P. W. (2016). A systematic review of studies on ethnic minority youth development in Hong Kong: An application of the ecological framework. China Journal of Social Work, 9(3), 218–237.
Bachman, J. G., O'Malley, P. M., Schulenberg, J. E., Johnston, L. D., Freedman-Doan, P., & Messersmith, E. E. (2007). The education-drug use connection: How successes and failures in school relate to adolescent smoking, drinking, drug use, and delinquency. England: Psychology Press.
Becker, G. S., & Murphy, K. M. (1988). A theory of rational addiction. Journal of Political Economy, 96(4), 675–700.
Becker, G. S., Murphy, K. M., & Grossman, M. (2004). The economic theory of illegal goods: The case of drugs (No. w10976). National Bureau of Economic Research.
Botvin, G. J. (2000). Preventing drug abuse in schools: Social and competence enhancement approaches targeting individual-level etiologic factors. Addictive Behaviors, 25(6), 887–897.
Botvin, G. J., Baker, E., Dusenbury, L., Botvin, E. M., & Diaz, T. (1995). Long-term follow-up results of a randomized drug abuse prevention trial in a white middle-class population. JAMA, 273(14), 1106–1112.
Caetano, R., Vaeth, P. A., & Canino, G. (2018). Illegal drug use and its correlates in San Juan, Puerto Rico. Drug and Alcohol Dependence, 185, 356–359.
Census and Statistics Department. (2016). Drug abuse situation in Hong Kong. https://www.censtatd.gov.hk/.
Chein, I., Gerard, D. L., Lee, R. S., & Rosenfeld, E. (1964). The road to H.: Narcotics, delinquency, and social policy. New York, NY: Basic Books.
Cheung, N. W., & Cheung, Y. W. (2006). Is Hong Kong experiencing normalization of adolescent drug use? Some reflections on the normalization thesis. Substance Use and Misuse, 41(14), 1967–1990.
Cheung, Y. W., & Cheung, N. W. (2018). Changes of the drug scene in Hong Kong. In: A. C. Michalos., D. T. L. Shek., D. C. Shin., M-C. Tsai. (Ed.), Psychoactive Drug Abuse in Hong Kong. Quality of Life in Asia (Vol. 11). Singapore: Springer.
Cheung, Y. W., & Ch'ien, J. M. (1996). Drug use and drug policy in Hong Kong: Changing patterns and new challenges. Substance Use and Misuse, 31(11–12), 1573–1597.
Chu, Y. W. L. (2014). The effects of medical marijuana laws on illegal marijuana use. Journal of Health Economics, 38, 43–61.
Corman, H., & Mocan, H. N. (2000). A time-series analysis of crime, deterrence, and drug abuse in New York City. American Economic Review, 90(3), 584–604.
DeSimone, J. (2002). Illegal drug use and employment. Journal of Labor Economics, 20(4), 952–977.
DeSimone, J., & Farrelly, M. C. (2003). Price and enforcement effects on cocaine and marijuana demand. Economic Inquiry, 41(1), 98–115.
Deng, R., Li, J., Sringernyuang, L., & Zhang, K. (2007). Drug abuse, HIV/AIDS and stigmatisation in a Dai community in Yunnan China. Social Science and Medicine, 64(8), 1560–1571.
Deykin, E. Y., Levy, J. C., & Wells, V. (1987). Adolescent depression, alcohol and drug abuse. American Journal of Public Health, 77(2), 178–182.
Dobkin, C., & Nicosia, N. (2009). The war on drugs: methamphetamine, public health, and crime. American Economic Review, 99(1), 324–349.
DiNardo, J., & Lemieux, T. (2001). Alcohol, marijuana, and American youth: the unintended consequences of government regulation. Journal of Health Economics, 20(6), 991–1010.
Järvinen, M. (2017). From wanting to willing–controlled drug use as a treatment goal. Social Science and Medicine, 176, 69–76.
Joe Laidler, K. A. (2005). The rise of club drugs in a heroin society: the case of Hong Kong. Substance Use and Misuse, 40(9–10), 1257–1278.
Joe-Laidler, K., & Hunt, G. (2008). Sit down to float: The cultural meaning of ketamine use in Hong Kong. Addiction Research and Theory, 16(3), 259–271.
Kandel, D. B. (1991). The social demography of drug use. The Milbank Quarterly, 69(3), 365–414. https://doi.org/10.2307/3350102.
Kerrison, E. M. (2018). Exploring how prison-based drug rehabilitation programming shapes racial disparities in substance use disorder recovery. Social Science and Medicine, 199, 140–147.
Lai, F. Y., Bruno, R., Leung, H. W., Thai, P. K., Ort, C., Carter, S., et al. (2013). Estimating daily and diurnal variations of illicit drug use in Hong Kong: a pilot study of using wastewater analysis in an Asian metropolitan city. Forensic Science International, 233(1–3), 126–132.
Liu, Z., Liu, Z., Lian, Z., & Zhao, C. (2006). Drug use and HIV/AIDS in China. Drug and Alcohol Review, 25(2), 173–175.
Lin, W. I. (2010). The coming of an aged society in Taiwan: Issues and policies. Asian Social Work and Policy Review, 4(3), 148–162.
Long, C., DeBeck, K., Feng, C., Montaner, J., Wood, E., & Kerr, T. (2014). Income level and drug related harm among people who use injection drugs in a Canadian setting. International Journal of Drug Policy, 25(3), 458–464.
Loxton, N. J., Wan, V. L. N., Ho, A. M. C., Cheung, B. K. L., Tam, N., Leung, F. Y., et al. (2008). Impulsivity in Hong Kong-Chinese club-drug users. Drug and Alcohol Dependence, 95(1–2), 81–89.
Martikainen, P., Korhonen, K., Moustgaard, H., Aaltonen, M., & Remes, H. (2018). Substance abuse in parents and subsequent risk of offspring psychiatric morbidity in late adolescence and early adulthood: A longitudinal analysis of siblings and their parents. Social Science and Medicine, 217, 106–111.
McGrath, C., & Chan, B. (2005). Oral health sensations associated with illicit drug abuse. British Dental Journal, 198(3), 159.
McHugh, R. K., Nielsen, S., & Weiss, R. D. (2015). Prescription drug abuse: from epidemiology to public policy. Journal of Substance Abuse Treatment, 48(1), 1–7.
Narcotics Division. (2011). Hong Kong Narcotics and Anti-Money Laundering Report 2007–2010. https://www.nd.gov.hk/en/report_2007-10.htm. Accessed 30 Sept 2018.
Narcotics Division. (2013). A review of estimation methods on prevalence of drug abuse population in Hong Kong. https://www.nd.gov.hk. Accessed 15 July 2020.
Nutt, D., King, L. A., Saulsbury, W., & Blakemore, C. (2007). Development of a rational scale to assess the harm of drugs of potential misuse. The Lancet, 369(9566), 1047–1053.
Pollack, H. A., Danziger, S., Seefeldt, K. S., & Jayakody, R. (2002). Substance use among welfare recipients: Trends and policy responses. Social Service Review, 76(2), 256–274.
Quinn, G. (2010). Institutional denial or minimization: Substance abuse training in social work education. Substance Abuse, 31(1), 8–11.
Saffer, H., & Chaloupka, F. (1999). The demand for illicit drugs. Economic Inquiry, 37(3), 401–411.
Shek, D. T., Keung Ma, H., & Sun, R. C. (2011). A brief overview of adolescent developmental problems in Hong Kong. The Scientific World Journal, 11, 2243–2256.
Schuermeyer, J., Salomonsen-Sautel, S., Price, R. K., Balan, S., Thurstone, C., Min, S. J., et al. (2014). Temporal trends in marijuana attitudes, availability and use in Colorado compared to non-medical marijuana states: 2003–11. Drug and Alcohol Dependence, 140, 145–155.
Smith, C. M., Garfield, J. B., Attawar, A., Lubman, D. I., & Lawrence, A. J. (2019). The influence of opioid dependence on salt consumption and related psychological parameters in mice and humans. Drug and Alcohol Dependence, 203, 19–26.
Tse, S., Zhu, S., Yu, C. H., Wong, P., & Tsang, S. (2016). An ecological analysis of secondary school students’ drug use in Hong Kong: A case-control study. International Journal of Social Psychiatry, 62(1), 31–40.
Wat, S. (1985). Central Registry of Drug Abuse. The International Journal of the Addictions, 20(2), 279–298.
Williams, J. (2004). The effects of price and policy on marijuana use: What can be learned from the Australian experience? Health Economics, 13(2), 123–137.
Wu, C. S., Wong, H. T., Shek, C. H., & Loke, A. Y. (2014). Multi-dimensional self-esteem and substance use among Chinese adolescents. Substance Abuse Treatment, Prevention, and Policy, 9(1), 42.
Acknowledgements
This research is funded by the Beat Drugs Fund Association (170062). The authors thank Central Registry of Drug Abuse at Narcotics Division and Census Department of Hong Kong for providing the drug use data and census data. The authors report no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Appendix
Rights and permissions
About this article

Cite this article
Liu, T., Gietel-Basten, S. A quantitative analysis of socioeconomics of illicit drug use for improving targeted interventions in Hong Kong. China popul. dev. stud. 4, 152–170 (2020). https://doi.org/10.1007/s42379-020-00062-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42379-020-00062-6