
Abstract
Objective
A minority of lesions found in the sellar region are non-adenomatous neoplastic, inflammatory, or cystic masses. Our study aims to describe the prevalence and characteristics of these lesions in a multidisciplinary pituitary outpatient clinic.
Design
We conducted an observational study which included 36 patients (15.9% of those followed up in this outpatient clinic between 2006 and 2016 who had pituitary surgery) submitted to pituitary surgery with histological results showing a non-adenomatous sellar lesion. We evaluated clinical, radiological, and biochemical (pituitary function) characteristics during the pre-operative and post-operative period.
Results
Thirty-six patients (50% female) with a mean age of 41.3 ± 21.9 years and a mean follow-up duration of 8.0 ± 9.0 years were included. Histologic diagnoses were divided into benign neoplasms (80.6%), malignant neoplasms (11.1%), inflammatory lesions (5.6%), and cystic masses (2.8%). The most common clinical presentation was headache (66.7%) and visual defects (61.1%). Forty-seven percent of patients had at least one pituitary axis insufficiency at the time of diagnosis. In the majority of cases (58.3%), a transsphenoidal approach was used for the initial pituitary surgery. Thirteen patients had more than one pituitary surgery and eight also had radiotherapy. At the time of data retrieval, five patients had no pituitary hormonal insufficiency and 13 patients had some visual defect improvement.
Conclusions
Although rare, non-adenomatous sellar lesions may be associated with significant causes of morbidity, such as hypopituitarism and visual defects, per se or due to the various treatment modalities employed. Moreover, since the lesions are difficult to distinguish from adenomas, these patients require a careful multidisciplinary approach.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The majority of masses found in the sellar region are pituitary adenomas (PA); however, about 10% of sellar tumors have a different etiology [1]. These lesions (some of them also referred to as rare sellar lesions) can include benign neoplasms (solid or cystic), malignant neoplasms, vascular lesions, and infectious/inflammatory lesions [2,3,4,5]. These non-adenomatous sellar lesions (NASLs) can sometimes be hard to distinguish from PA as they lack characteristic radiological, clinical, and biochemical features. As a result, surgery is usually necessary to establish a final diagnosis. Nowadays, transsphenoidal (TS) surgery is the recommended approach, though in some cases, transcranial (TC) surgery may be necessary in order to provide appropriate access to the lesion and remove it [6, 7]. Treatment can also include other options, such as radiotherapy and chemotherapy depending on the type of lesion and its outcome after surgery [5, 8, 9]. Varying degrees of hypopituitarism can occur both pre-operatively (pre-op) and post-operatively (post-op) [2, 4, 6, 8]. Here, we report our centre’s 10-year experience regarding pre-op and post-op clinical, radiological, and biochemical characteristics of patients who had pituitary surgery and a histological diagnosis of a NASL.
Materials and methods
We performed a single-centre retrospective study including patients followed up in the pituitary multidisciplinary outpatient clinic of Hospital de Egas Moniz, Lisbon, Portugal, due to a sellar mass, between 2006 and 2016. During this time period, a total of 644 patients were evaluated and, of these, 246 had pituitary surgery (TS or TC) at some time during their follow-up (also including patients who had surgery from 1980 to 2016). Of these, 39 had surgical histological results consistent with a non-adenomatous lesion – 15.9%.
After identifying all patients with a histological diagnosis of NASL, we reviewed all available recorded data in the hospital records, including clinical, biochemical, radiological, and pathological data. We excluded three patients due to incomplete data, namely, three craniopharyngiomas. The lesions were divided according to their histology into benign neoplasms, cystic masses, malignant neoplasms, and inflammatory lesions.
Patients were evaluated preoperatively by a multidisciplinary team (endocrinologist, neurosurgeon, and neuro-ophthalmologist) and had assessments of pituitary function and structure (magnetic resonance imaging [MRI]) before surgical referral.
All patients had TS or TC surgery (decided by the neurosurgical team): the removed mass was subsequently evaluated by the pathology department and a histological diagnosis was made. Immunohistochemistry evaluation was routinely performed.
After surgery, patients were assessed in the outpatient clinic by an endocrinologist, neurosurgeon, and neuro-ophthalmologist and had periodic MRI and endocrine biochemical evaluation. Additional treatment was considered on a case-by-case basis by the multidisciplinary team according to the histology result, occurrence of residual/relapsing lesion, clinical presentation, and the patient’s age/general status.
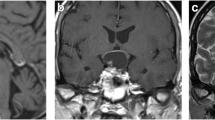
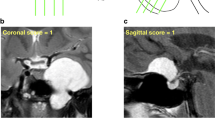
Lesions were radiologically classified, as described by the neuroradiologist, according to their maximum diameter (less than 1 cm; 1–3.99 cm, and more than 4 cm) and growth pattern (intrasellar; suprasellar [extension above the diaphragma sellae]; parasellar [extension to at least one of the cavernous sinus] or sphenoidal [extension into the sphenoidal sinus]).
Pituitary function was evaluated (determinations by the Hospital’s laboratory) both pre-op and periodically post-op, as ordered by the attending endocrinologist. All patients underwent measurements of gonadotropins and either estradiol or testosterone, fasting cortisol, and TSH and free T4 (fT4), while some also had IGF-1 and prolactin (PRL) measured.
Secondary hypogonadism was diagnosed, taking into account clinical data and the confirmation of a low value of morning total testosterone/estradiol with high-normal levels of gonadotropins. The diagnosis of secondary hypocortisolism was based on a fasting morning cortisol of less than 5 μg/dL alongside clinical elements and other analytical features (such as low ACTH, hyponatremia, hyperkalemia, and hypoglycemia). Secondary hypothyroidism was considered in the case of low fT4 in the presence of a low–normal TSH. These diagnoses were made after exclusion of other potential causes for these biochemical profiles.
Results
Patient demographics
A total of 36 patients were included, 50% of each sex. Age at diagnosis was between 5 and 76 years, with an average age of 41.3 ± 21.9 years. The mean follow-up duration was 8.0 ± 9.0 years.
Histological diagnosis (Table 1)
Benign neoplasms were the most commonly found type of lesions (29 cases, 80.6%), namely, craniopharyngiomas (n = 19). There were four cases of malignant tumors, three chordomas and one breast cancer metastasis. No infectious masses were found; however, we identified two cases of hypophysitis, one granulomatous and one xanthomatous. Only one cystic mass was diagnosed, namely, a Rathke’s cleft cyst.
Clinical presentation (Table 2)
Headache was the most common presenting symptom (n = 24, 66.7%), followed by a visual field defect or deterioration of visual acuity (n = 22, 61.1%). There were four cases of sellar masses discovered incidentally during an MRI performed due to unrelated causes. More unusual presentations included short stature (the case of a 6-year-old boy diagnosed with a craniopharyngioma and associated GH deficiency), galactorrhea (a female patient with a Rathke’s cleft cyst and hyperprolactinemia), oligomenorrhea (one craniopharyngioma, and one astrocytoma associated with hypogonadotropic hypogonadism) and polydipsia/polyuria (the case of pituitary breast cancer metastasis with central diabetes insipidus). Regarding III, IV, and VI nerve palsies, of the five patients who had parasellar tumoral invasion, some deficit was observed in two of them.
Pre-op pituitary function (Table 3)
A total of 17 patients (47.2%) had at least one pituitary axis hormonal insufficiency at the time of the initial biochemical evaluation. The most commonly diagnosed deficit was hypothyroidism (n = 15), followed by hypogonadism (n = 12), and hypocortisolism (n = 10). There were only two cases of diabetes insipidus pre-op: one breast tumor metastasis and one Rathke’s cleft cyst (a large expansive lesion with suprasellar extension). Prolactin was measured in 23 patients, 11 (47.8%) of which had elevated values. The mean PRL concentration was 32.4 ± 33.7 ng/mL. GH/IGF-1 was not measured in most patients and is therefore not addressed in this manuscript.
Radiological pre-op characteristics (Table 4)
Regarding the maximum lesion diameter as measured by MRI, most lesions were between 1 and 3.99 cm (n = 23). Only one tumor measured less than 1 cm, a mixed pituitary adenoma-gangliocytoma. Twelve lesions had a diameter of 4 cm or more and were mostly craniopharyngiomas (n = 9).
In terms of localization, only two cases did not have suprasellar extension: one meningioma and one mixed pituitary adenoma-gangliocytoma. Two lesions invaded the sphenoidal sinus: one chordoma and one cavernous hemangioma. Five tumors had parasellar involvement: two chordomas, two meningiomas, and one craniopharyngioma.
Pituitary surgery (Table 1)
Concerning the first surgery performed, the majority of patients had TS surgery (n = 21, 58.3%). Almost all TC surgeries were in craniopharyngioma patients (13 of a total of 15 TC surgeries). Only six craniopharyngiomas had TS surgery (31.6%). The lesions removal extent was gross-total in 14 cases and partial in 22. All surgeries performed before 2004 (n = 11) had a TC approach, i.e., 10 craniopharyngiomas and one astrocytoma.
Thirteen patients (36.1%) needed additional pituitary surgery due to persistent or recurrent disease. Nine patients had a total of two surgeries, three patients were submitted to three surgeries, and one patient (chordoma) had four surgeries in total.
Additional non-surgical therapies
Eight patients (22.2%) had radiotherapy performed in addition to pituitary surgery: two patients were submitted to proton therapy, six patients to conventional radiotherapy, and one patient to stereotactic radiosurgery. All three chordoma patients had some type of radiotherapy, as did four craniopharyngiomas and one astrocytoma.
Mass control outcomes (Table 4)
After the first pituitary surgery, there was radiological tumor persistence in 17 cases. A total of 10 patients remained in radiological remission at the end of follow-up. Regarding patients who experienced relapse/persistence of the sellar lesion after the first pituitary surgery, the majority (n = 5) presented a residual mass in the first post-op year; however, there were lesions that relapsed in the second, third, fourth, fifth, and sixth year (one patient in each year). At the end of follow-up (after all therapeutic interventions), most patients (n = 20, 55.6%) maintained some radiological evidence of the initial tumor in the last MRI.
Post-op pituitary function (Table 3)
Five patients (all submitted to TS surgery with partial lesion resection) had no hormonal pituitary deficiency at the time of data retrieval; all but one had basal IGF-1 determination, and these were normal. The remainder of patients had some degree of hypopituitarism diagnosed at the end of follow-up: hypothyroidism in 31 patients (85.1%), hypogonadism in 28 (77.8%), and hypocortisolism in 27 (75%). Regarding patients who developed a pituitary deficit de novo after surgery, 17 developed hypothyroidism, 17 hypocortisolism, and 16 hypogonadism. Patients submitted to TC surgery had a higher frequency of newly developed post-op pituitary dysfunction as compared to TS: hypothyroidism (73.3 vs 28.6%), hypogonadism (66.7 vs 28.6%), and hypocortisolism (53.3 vs 23.8%). Only one patient improved pituitary function after surgery, namely, a patient with a cavernous hemangioma who had his hypothyroidism resolved after TS surgery.
Concerning diabetes insipidus, there were eight patients who developed this condition temporarily following pituitary surgery. At the time of data collection, 15 patients (41.7%) needed desmopressin therapy, mainly craniopharyngiomas (13 patients). Patients who had TC surgery had a higher frequency of new onset of diabetes insipidus than those who had TS surgery, i.e., 53.3 vs 32.8%.
Clinical/neuro-ophthalmological outcomes
At the end of the registered follow-up, as evaluated by a neuro-ophthalmologist, 13 patients (59.1% of patients who had pre-op deficits) showed some visual improvement. Eleven patients (31.4%) remained similar to pre-op and ten (28.6%) patients had worsened visual status. With regard to the five patients who had initial parasellar tumoral extension, two of them had a III, IV, or VI nerve palsy, one of these being de novo after surgery. One patient experienced improvements in this regard after surgery.
Five patients had grade II or III obesity (all tumors with suprasellar extension: three craniopharyngiomas, one lipoma, and one astrocytoma).
There was a total of three deaths: one patient with a chordoma, one with craniopharyngioma (unrelated to his pituitary tumor), and one case of breast cancer metastasis.
Discussion
Sellar tumors account for 10–15% of all intracranial tumors and of these 90% are pituitary adenomas. NASLs include diverse entities, such as neoplasms (benign and malignant), cysts, inflammatory/infectious processes, and vascular lesions [1]. These lesions are usually very difficult to differentiate and are also difficult to distinguish from adenomas owing to their very similar clinical, radiological, and biochemical presentation (although hypersecretory syndromes are rarer in the case of NASLs) [3]. Thus, definitive diagnosis is histological after pituitary surgery, in which case, the TS approach is nowadays usually the preferred route [4].
Published patient series (all of them surgical series) differ greatly in a number of aspects, including type of lesion inclusion criteria, type of surgical procedures analyzed, time period evaluated, and type of NASL classification employed [2, 4, 6, 8].These differences possibly account for the heterogeneity of published results. In our case, we present patients who had follow-up in a multidisciplinary pituitary outpatient clinic between 2006 and 2016, with a NASL histological diagnosis after pituitary surgery (including different surgical approaches) at some time during the patient’s medical history. Given that our data include surgeries from 1980 to 2016 and encompass a follow-up period of up to a maximum of 36 years, they span a large time period, while also comprising both adult and non-adult patients with a histological diagnosis of any NASL.
In this study, we report that during the analyzed time period, 15.9% of patients (n = 39) followed up in our pituitary outpatient clinic who had pituitary surgery received a histological diagnosis of a NASL. Of the 36 included patients, 29 (80.6%) of the removed masses were benign neoplasms, four (11.1%) were malignant neoplasms, two inflammatory lesions (5.6%), and only one was a cystic lesion (2.8%). By far the most frequent masses identified were craniopharyngiomas, this being a feature that differs from other published series and surely influences overall results. There are some potential explanations for this fact, such as our decision to include pediatric patients and the decision of other authors to exclude this type of lesion from their analyses given how common they are [4, 6]. Our study also seems to differ from others regarding the small number of cystic lesions, namely Rathke cleft cysts: this concerned only one patient in our series (2.8%), while others describe them in 28–42% of included cases [2, 8, 10]. These are usually small, intrasellar asymptomatic lesions which should prompt surgery only if they grow and become symptomatic [11]. In fact, our only included case of such a lesion was an extensive tumor which was diagnosed with an unusually serious clinical presentation (headache, visual loss, and panhypopituitarism with central diabetes insipidus) and had successful TS surgery. The remainder of suspected cases of Rathke cleft cysts remain followed up with serial imaging, as we believe that their mass effect/clinical presentation does not justify surgical intervention.
Regarding the age of definitive diagnosis, four patients were diagnosed at the age of 16 or younger, although at the time of data collection, they were all adult. Of these diagnoses, three were craniopharyngiomas and one was an astrocytoma. Two of these patients (both craniopharyngiomas) had biochemically proven GH deficiency and underwent GH treatment, both subjects having reached their estimated target height. This is in line with the previously described high rates of GH deficiency (26–75% of pediatric patients)—both in relation to the tumor per se and to the therapeutic interventions—and positive response to GH therapy seen in most childhood patients with craniopharyngiomas [12]. The age distribution of the incidence of craniopharyngiomas is reported elsewhere to be bimodal, with peak rates between 5 and 14 years and 50 to 74 years [12]. We did not confirm this in our series and found an approximately normal age distribution, with a peak incidence between 20 and 50 years (63% of patients). It is our belief that regarding this subject, our data are largely skewed by the relatively small number of pediatric patients referred to and followed in our centre.
Considering all included types of lesions, headache (66.7%) and visual field defect or deterioration of visual acuity (61.1%) were the most common presenting symptoms. These findings are in line with published data by Valassi et al. reporting headache to be the most frequent presenting complaint in their series in different types of lesions (overall, cystic, and inflammatory lesions) [2]. Headache is also variably described as the most common primary disease manifestation in the case of craniopharyngiomas, especially in pediatric patients [13, 14]. Malignant lesions had a higher percentage of visual symptoms (75%) than headache (25%): this is common in sellar chordomas, mainly secondary to chiasmatic/optic tract compression, and such was the case in all our patients [15].
In terms of endocrine function, pre-op testing identified 47.2% of patients with at least one adenohypophysis axis hormonal deficiency. Central hypothyroidism (41.7%) was the most common deficiency, followed by hypogonadism (33.3%) and hypocortisolism (27.8%). Other NASL surgical series report incidences of pre-op hypopituitarism (variably defined) between 10 and 45%; however, only Valassi et al. discriminate between different hormonal axis affected: hypogonadism in 23% of cases, hypothyroidism in 20%, and adrenal insufficiency in 23% [1, 2, 4, 8]. The finding of hypothyroidism as the most frequent pituitary insufficiency in our NASL series is unexpected, as this is not the case in other types of pituitary lesions. Mechanisms by which NASLs interfere with thyrotrophs preferentially have not been proposed to date, hence, we must consider that this predominance can be due to other reasons, such as the absence of formal TRH testing, the lack of GH axis information (this being one of the most commonly described deficiencies in sellar lesions), lack of dynamic testing of other pituitary lines, and perhaps the interference of confounders such as the use of glucocorticoids without our knowledge. Comparing available data on craniopharyngiomas (which were the most frequent benign neoplasms in our study) with our results, the overall hypopituitarism rates seem similar (40–87% in craniopharyngiomas series), as do specific axis deficiencies (hypogonadism 38–91%, hypocortisolism 21–68%, hypothyroidism 20–42%), although the published data are highly heterogeneous [12, 13]. Diabetes insipidus was diagnosed pre-op in two cases, one metastatic lesion and one Rathke’s cleft cyst, and indeed this is something that should raise suspicion of a NASL, even though it is very uncommon in the case of Rathke cleft cysts [3]. As in most published studies, some patients included in our study only had one pre-op endocrine function evaluation and none had undergone dynamic testing. As a result, the criteria utilized in our patient series for the diagnosis of hypopituitarism (notably, hypocortisolism and GH deficiency) is not totally in line with the present international diagnosis guideline recommendations, and this should be considered as a significant limitation of our study, possibly contributing to an underestimation of hypopituitarism cases.
We observed that 41.7% (66.7% of cases who had a first TC surgery vs 23.8% with a first TS surgery) of patients who had no known hypopituitarism before treatment developed at least one pituitary hormonal axis deficiency at some time during the follow-up period. Comparing patients with a first TC surgery vs TS surgery, cases of de novo pituitary dysfunction were as follows: hypothyroidism in 73.3 vs 28.6%, hypogonadism in 66.7 vs 28.6%, and hypocortisolism in 53.3 vs 23.8%. Only one patient (2.8%) improved pituitary function by resolving hypothyroidism after TS surgery (a case of cavernous hemangioma). Somma et al. reported 10% of cases of iatrogenic hypopituitarism and improvement of function in 9% in their NASL TS surgical patient series (which excluded craniopharyngiomas, Rathke’s cleft cysts and meningiomas), while Valassi et al. described an incidence of post-op (after TS surgery) hypopituitarism of 10% and an improvement of endocrine status in 21% [2, 4]. Eight patients (22.2%) developed temporary central diabetes insipidus following pituitary surgery and 12 patients (41.7%) were being treated with desmopressin at the end of the follow-up period, 53.3 vs 32.8% with TC surgery and TS surgery, respectively. Other NASL TS surgery series report incidence of permanent diabetes insipidus of less than 5% [2, 4, 8].
The different pituitary function outcomes observed in our series, namely, the higher rates of hypopituitarism, might be explained by various factors: the fact that we included patients (41.7%) who had TC surgery (thus, higher risks of iatrogenic hypopituitarism), the timing of our endocrine evaluation—we considered the testing at the end of follow-up (average duration of 8 years) after all therapeutic interventions (36.1% of patients had more than one surgery and 22.2% had radiotherapy)—and the composition of NASL included in our series (half were craniopharyngiomas)—pituitary surgery in craniopharyngiomas is associated with a high risk of iatrogenic hypopituitarism (66.7–75.9% as reported by Mortini et al.) [16, 17]. Nevertheless, our pituitary function outcomes, after various therapeutic actions, highlight the fact that these types of lesions are associated with high morbidity per se and with the entire treatment intervention, this being a point about which surgical patient series can be misleading, as they consider the outcomes only following the first surgery.
In our series, neuro-ophthalmologic status at the time of data collection showed improvements in 59.1% of patients who had pre-op visual deficits, while 28.6% of the total of patients were worse. Results published elsewhere are highly variable concerning NASL (improvement in 6.8–65%), this apparently largely due to the difference in the lesions included and the methodology employed [2, 4, 8]. Regarding benign neoplasms (mainly craniopharyngiomas), 58.8% showed some visual improvements at the end of the follow-up period; however, 32.1% worsened. These numbers are somewhat similar to other published series, although the significant percentage of patients who worsened can probably be explained by a variety of factors such as the high number of TC surgeries, the known long-term risk of treatment-associated (surgical and radiotherapy) visual deterioration, and the high risk of disease recurrence/persistence after treatment [12,13,14].
In summary, in our series, histologically confirmed NASLs represented 6.1% of cases followed up in our centre’s pituitary multidisciplinary outpatient clinic between 2006 and 2016. Most of our cases were benign neoplasms, of which craniopharyngiomas were the most frequent. These NASLs commonly present with headaches and various visual and pituitary endocrine deficits at the time of diagnosis which can justify pituitary surgery. Nowadays, TS is the surgical approach adopted in most circumstances; nevertheless, some patients who had TC surgery were included in our series. In various instances, more than one surgery or radiotherapy was required due to recurrent or persistent disease, making iatrogenic hypopituitarism a meaningful risk. Nonetheless, a considerable percentage of patients experienced improvement of the visual symptoms by the time of data collection.
The complexity of the diagnosis (in many cases only possible post-op) and of treatment of this rare heterogeneous group of lesions underlines the importance of a multidisciplinary approach and the need for long-term patient follow-up.
References
Freda P, Post K (1999) Differential diagnosis of sellar lesions. Pituitary 28(1):81–117
Valassi E, Biller B, Klibanski A, Swearingen B (2010) Clinical features of non-pituitary sellar lesions in a large surgical series. Clin Endocrinol 73(6):798–807
Glezer A, Paraiba DB, Bronstein MD (2008) Rare sellar lesions. Endocrinol Metab Clin N Am 37(1):195–211
Somma T, Solari D, Beer-Furlan A, Guida L, Otto B, Prevedello D et al (2017) Endoscopic endonasal management of rare sellar lesions: clinical and surgical experience of 78 cases and review of the literature. World Neurosurg 100:369–380
Karavitaki N, Wass JAH (2009) Non-adenomatous pituitary tumours. Best Pract Res Clin Endocrinol Metab 23(5):651–665
Petrakakis I, Pirayesh A, Krauss JK, Raab P, Hartmann C, Nakamura M (2016) The sellar and suprasellar region: a “hideaway” of rare lesions. Clinical aspects, imaging findings, surgical outcome and comparative analysis. Clin Neurol Neurosurg 149:154–165
Liu JK, Weiss MH, Couldwell WT (2003) Surgical approaches to pituitary tumors. Neurosurg Clin N Am 14(1):93–107
Koutourousiou M, Kontogeorgos G, Seretis A (2010) Non-adenomatous sellar lesions: experience of a single centre and review of the literature. Neurosurg Rev 33(4):465–476
Czepielewski M, Rollin G, Casagrande A, Ferreira MG, Ferreira N (2005) Tumores Não Hipofisários da Região Selar. Arq Bras Endocrinol Metab 49(5):674–690
Freda P, Wardlaw S, Post K (1996) Masses in a large unusual causes of sellax/parasellar transsphenoidal surgical series. J Clin Endocrinol Metab 81(10):3455–3459
Han SJ, Rolston JD, Jahangiri A, Aghi MK (2014) Rathke’s cleft cysts: review of natural history and surgical outcomes. J Neuro-Oncol 117(2):197–203
Muller HL (2014) Craniopharyngioma. Endocr Rev 35(3):513–543
Karavitaki N, Cudlip S, Adams CBT, Wass JAH (2006) Craniopharyngiomas. Endocr Rev 27(4):371–397
Zoicas F, Schöfl C (2012) Craniopharyngioma in adults. Front Endocrinol 3:1–8
Thodou E, Kontogeorgos G, Scheithauer BW, Lekka I, Tzanis S, Mariatos P et al (2000) Intrasellar chordomas mimicking pituitary adenoma. J Neurosurg 92(6):976–982
Mortini P, Losa M, Pozzobon G, Barzaghi R, Riva M, Acerno S et al (2011) Neurosurgical treatment of craniopharyngioma in adults and children: early and long-term results in a large case series. J Neurosurg 114(5):1350–1359
Maartens NF, Kaye AH (2006) Role of transcranial approaches in the treatment of sellar and suprasellar lesions. Front Horm Res 34(1906):1–28
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Sousa Santos, F., Nunes Dias, L., Henriques, V. et al. Non-adenomatous sellar lesions: single-centre 10-year experience. Hormones 17, 557–563 (2018). https://doi.org/10.1007/s42000-018-0064-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42000-018-0064-y