
Key summary points
Our aim was to examine the relationship between type 2 diabetes (T2D) and its treatment with mortality in older adults who present to the emergency department with a fall.
AbstractSection FindingsPeople with T2D had a similar clinical frailty score, were more likely to be male and receive more concomitant medicines. Hypoglycaemia-inducing agents may contribute to the greater one-year mortality observed in people with T2D.
AbstractSection MessageFalls are a significant burden, and diagnosis of T2D and possibly hypoglycaemia-inducing medications may contribute to the greater mortality observed in people with T2D. Clinician awareness can support de-prescribing for patients with frailty and HbA1c < 64 mmol/mol.
Abstract
Introduction
Type 2 diabetes mellitus (T2D) is associated with poor health outcomes whilst tight glycaemic targets are questionable in those aged over 70 years with increased frailty. Our aim was to examine whether people with T2D admitted to hospital with a fall, were more likely to have greater frailty, increased mortality and co-morbidity burden, or risk factors for falls than people without T2D, and whether these differences were associated with medications used for the treatment of T2D.
Methods
The Older Persons Assessment Service (OPAS) is a local emergency department (ED) service, which accepts patients on frailty criteria. The OPAS accepts patients primarily aged over 70 years who present with frailty and geriatric syndromes such as falls, with retrieval from the ED department directly to the service from triage. The OPAS databank was analysed for people with T2D admitted with a fall between June 2020–September 2022. We examined clinical outcomes relating to medication, age, Charlson co-morbidity index (CCI) and clinical frailty score (CFS).
Results
1081 patients were included: 294 (27.2%) with T2D and a mean HbA1c of 53.9 (± 15.8) mmol/mol [7.1%]. People with T2D had a similar mean CFS and age compared to those without T2D, but higher mean CCI (7.0 ± 2.2 vs 5.9 ± 2.1, p < 0.001). Of those people with T2D, 175 (59.5%) and 240 (81.6%) had a HbA1c ≤ 53 mmol/mol [7.0%] and ≤ 64 mmol/mol [8.0%], respectively. In total, 48 (16.3%) people with T2D were identified to have a capillary blood glucose below 4.0 mmol/L on admission to the ED. At 12 months’ follow-up, 831 (76.9%) patients were alive and 250 (23.1%) had died. People with T2D treated with insulin and/or gliclazide had a greater 1-year mortality (36.6% vs 23.6%, p < 0.05), greater frequency of hypoglycaemia (35.4% vs 11.8%, p < 0.001), and greater HbA1c (65.5 ± 17.2 mmol/mol [8.2] vs 48.9 ± 12.1 mmol/mol [6.6%]) compared to those who used other agents. Logistic regression confirmed a diagnosis of T2D was associated with 1-year mortality, but mortality was not significantly associated with hypoglycaemic-inducing agents. People with T2D were not more likely to live in deprived areas.
Conclusions
A diagnosis of T2D is associated with greater 1-year mortality, and may be influenced by use of hypoglycaemia-inducing diabetes medications. Clinician awareness can support de-prescribing for patients with frailty and HbA1c < 64 mmol/mol.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Falls have a significant burden on health systems as they are a frequent cause of hospital admission and may be associated with significant injury. Age is a major risk factor, and evidence supports the findings that older adults are more likely to fall than younger adults [1]. Falls are often multifactorial in origin [2], and are more common in nursing home residents and those with frailty [3]. In addition, falls are the leading cause of death due to unintentional injury in people aged over 65 years [4] in the USA and are the second cause of unintentional injury deaths worldwide [5]. In England between 2020 to 2021, there were more than 2023 per 100,000 emergency department (ED) hospital admissions related to falls in patients aged over 65 years, with 5174 per 100,000 in patients aged ≥ 80 years [6]. Of note, recurrent falls are responsible for significant morbidity and mortality in older adults. In addition to physical injury, recurrent falls may result in “post-fall syndrome”, where an older person refuses to move for fear of recurrent falls and further injury. It is estimated that approximately one-third of these individual’s experience one or more falls per year, while 10% experience multiple falls annually [7, 8]. The risk of falls is higher in octogenarians and nonagenarians, with an annual incidence of 50% [9,10,11,12,13].
Published research has shown that early comprehensive geriatric assessment in association with a measurable frailty outcome such as the clinical frailty scale (CFS) is beneficial [14]. The Charlson comorbidity index (CCI), is an assessment tool designed specifically to predict long-term mortality associated with the accumulation of comorbidities, and has been validated in multiple populations [15]. The addition of frailty data to assess the physiological effects of an acute illness can guide mortality prediction [14].
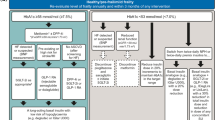
Recently, the Joint British Diabetes Societies for Inpatient Care [16], Association of British Clinical Diabetologists [17] and National Institute for Health and Care Excellence [18] have released updated guidance on the management of diabetes in people with significant frailty, usually defined as a CFS of 5 or more. One in six hospital beds are occupied by a person with diabetes and most of these are older adults. These patients have a greater length of hospital stay, morbidity and mortality than those without diabetes [19]. Careful consideration of medications used to treat type 2 diabetes (T2D) whilst avoiding clinical harm associated with some classes of diabetes medication are needed for this group. For example, medications such as gliclazide or insulin are associated with hypoglycaemia, whilst sodium-glucose co-transporter 2 (SGLT-2) inhibitors may be associated with diabetic ketoacidosis and urogenital infections [20].
With respect to the association between T2D and falls risk in the frail or older person, there is some published literature. One meta-analysis observed that older adults with T2D are associated with excessive falls risk compared to people without T2D, with greater risk in insulin-treated patients [21]. Hypoglycemia induced by intensive glycaemic control or chronic complications such as peripheral neuropathy and retinopathy may also increase the risk of falls. The mechanisms responsible for the falls risk in older patients are multifactorial and possible contributing factors include peripheral neuropathy, visual impairment, vestibular dysfunction, cognitive impairment, musculoskeletal/neuromuscular complications, or hypoglycaemia associated with insulin use [22]. Insulin treatment has previously been associated with excessive risk of falls, which may be related to longstanding diabetes complications, impaired hypoglycaemic awareness and the presence of other co-morbid conditions such as heart disease and chronic kidney disease [22].
Our aim was to examine whether people with T2D admitted to hospital with a fall, were more likely to have greater frailty, co-morbidity burden, or risk factors for falls. We also examined whether people with T2D had a worse outcome, including mortality, following admission and whether the use of insulin or gliclazide was associated with poor clinical outcome in a cohort of patients admitted to the emergency department (ED) with a fall.
Methods
Study design
This was a cross-sectional study examining patients admitted to the Older Persons Assessment Service (OPAS) at Morriston Hospital in Swansea. The OPAS is an ED service, which accepts patients on frailty criteria, such as patients aged over 70 years or who present with geriatric syndromes such as falls, delirium and un-met care needs. The OPAS is a dedicated unit within the ED, accepting the care of patients directly from either the ED triage or the Welsh Ambulance Service Trust. The OPAS team includes physiotherapists, occupational therapists, clinical nurse specialists, emergency nurse practitioners, advanced nurse practitioners and continuous consultant geriatrician input to provide a comprehensive geriatric assessment.
The OPAS databank was analysed for people with T2D admitted with a fall between June 2020 and September 2022. We compared age, medication usage, CCI and CFS [14, 15] in people with or without T2D. We also explored biochemical parameters such as HbA1c and data related to hypoglycaemia on admission. We reviewed patient mortality at prospectively at 12 months by reviewing electronic health records, and evaluated postcode data to derive the Welsh index of multiple deprivation (WIMD) to compare these measures in people with or without T2D. This work was undertaken as part of a service evaluation of the function of OPAS within the ED.
Statistical analysis
Continuous variables are presented as the mean ± standard deviation, whilst categorical variables are presented as the number (%). Statistical significance for continuous variables was determined using Student’s t-test and categorical variables were determined using Chi-squared test. Statistical significance was taken at p < 0.05. Logistic regression was performed using SPSS (Version 28) to evaluate associations between T2D and its treatment with one-year mortality.
Results
A total of 1081 patients were included for analysis, with a mean age 84.0 ± 7.9 years and 436 (40.3%) were male. The mean CFS of the total cohort was 5.3 ± 1.3 and CCI was 6.2 ± 2.2, and the mean number of medications used was 8.3 ± 3.7 per patient. At 12 months’ follow-up, 831 (76.9%) patients were alive and 250 (23.1%) had died. The mean WIMD decile of the total cohort was 5.4 ± 3.0.
Of patients included in the analysis, 294 (27.2%) had T2D and 787 (72.8%) people did not have T2D. People with T2D had a mean HbA1c 53.9 ± 15.8 mmol/mol [7.1%]. Of those with T2D, 175 (59.5%) and 240 (81.6%) had a HbA1c ≤ 53 mmol/mol [7.0%] and ≤ 64 mmol/mol [8.0%], respectively. In total, 48 (16.3%) people with T2D admitted with a fall were identified to have a capillary blood glucose below 4.0 mmol/L on admission. Compared to people without T2D, people with T2D were more likely to be male (53.1% vs 35.5%, p < 0.001), take a greater number of medications (9.1 ± 3.6 vs 8.0 ± 3.7, p < 0.001) and have greater CCI (7.0 ± 2.2 vs 5.9 ± 2.1, p < 0.001). Moreover, greater mortality was observed at 12 months’ follow-up in people with T2D compared to those without T2D (27.2% vs 21.6%, p < 0.05). Logistic regression was performed using mortality as the observed variable, with confounding variables of age, sex, CFS and T2D diagnosis. This observed that older age (p < 0.001), male sex (p < 0.001), greater CFS (p < 0.001), and a diagnosis of T2D (p < 0.05) significantly predicted 1-year mortality in the total cohort. The mean WIMD decile of those with T2D was 5.3 ± 2.9 compared to those without T2D 5.5 ± 3.0. (p = 0.30). These data are presented in Table 1.
In people with T2D, 82 (27.9%) were prescribed insulin and/or gliclazide, with the remainder prescribed oral agents or treated with dietary measures alone. At 12 months’ follow-up, people with T2D prescribed insulin and/or gliclazide had significantly greater mortality (36.6% vs 23.6%, p < 0.05). People with T2D prescribed insulin and/or gliclazide had a significantly higher HbA1c than those treated with dietary measures or oral agents (65.5 ± 17.2 mmol/mol [8.2] vs 48.9 ± 12.1 mmol/mol [6.6%]) but had a significantly greater frequency of hypoglycaemia observed on admission to hospital (35.4% vs 11.8%, p < 0.001). The mean WIMD decile of those with T2D prescribed insulin and/or gliclazide was 5.2 ± 2.6 compared to those without T2D 5.3 ± 3.1. (p = 0.85). These data are presented in Table 2. After excluding those prescribed insulin, the significant difference in greater HbA1c (61.5 ± 14.5 mmol/mol vs 49.1 ± 12.1 mmol/mol, p < 0.001) and frequency of hypoglycaemia on admission to hospital (21.4% vs 8.9%, p < 0.001) remained, though the greater mortality previously observed was no longer statistically significant (35.7% vs 25.0%, p = 0.15). Moreover, people with T2D prescribed insulin had a greater HbA1c (69.4 ± 18.1 mmol/mol vs 61.5 ± 14.5 mmol/mol, p < 0.05) and frequency of hypoglycaemia (55.6% vs 21.4%, p < 0.05) than those prescribed gliclazide, though the greater 12-month mortality in those prescribed insulin was not statistically significant (44.4% vs 35.7%, p = 0.47).
People with T2D who were deceased at 12 months’ follow-up were more likely to be male (58.8% vs 42.5%, p = 0.01), have greater CFS (5.8 ± 1.2 vs 5.1 ± 1.2, p < 0.001) or CCI (7.6 ± 2.5 vs 6.8 ± 2.1, p = 0.01) and prescribed a greater number of medications (9.8 ± 3.8 vs 8.8 ± 3.5, p = 0.03) than people who were alive at 12 months’ follow-up. In people with T2D, a logistic regression was performed using mortality as the observed variable, with confounding variables of age, sex, CFS, Hba1c and T2D treatment prescribed. This analysis observed that 1-year mortality was associated with male sex (p < 0.01), greater CFS (p < 0.001) and a lower HbA1c (p < 0.05) but not with the use of diabetes medications associated with hypoglycaemia (p = 0.62). The mean WIMD decile of those with T2D who were deceased was 4.9 ± 2.9 compared to those alive 5.4 ± 2.9. (p = 0.25). There was a trend to greater age (85.4 ± 7.4 vs 82.9 ± 7.6 years, p = 0.07) and lower HbA1c (50.3 ± 15.5 mmol/mol [6.7%] vs 55.2 ± 16.1 mmol/mol [7.2%], p = 0.07) in people who had died compared to those who were alive at 12 months’ follow-up which did not meet statistical significance. These data are shown in Table 3.
Discussion
A high proportion of our population with T2D were admitted to hospital with a hypoglycaemic event (16.3%). Previous observational data have observed that more than 70% of hypoglycaemia-related admissions occur in those aged 60 years and older, with gross numbers increasing [23]. Hypoglycaemic events are well known to be associated with falls especially in those who are aged greater than 65 years [24] and with more intensive HbA1c control compared to those with a HbA1c between 53–58 mmol/mol [7.0–7.4%] who have a lower risk of recurrent falls. We observed that those with T2D had a higher number of medications, which might be expected given the additional disease burden, but nevertheless polypharmacy is an independent risk factor for recurrent falls [25], which should prompt clinicians to perform a structured medication review. In addition, those with T2D had a higher CCI, which might be expected given that diabetes is scored in this clinical tool [15]. There was a significantly higher proportion of men in our cohort with T2D, again unsurprising, given that men are more likely to have T2D [26]. There was increased mortality in those with T2D, consistent with data from the United States [27]. This may be a consequence of associated complications observed in people with T2D, therapeutic inertia with respect to medication de-escalation, or the management of T2D may be overlooked by many clinicians with a reluctance to change diabetes medications. We found no difference with respect to social deprivation between those with and without T2D.
When exploring the characteristics and outcomes of people with T2D prescribed insulin and/or gliclizade compared with other agents, there was not a greater mortality associated with insulin and/or gliclazide compared with other agents for treatment of T2D, and their use was not associated with a lower HbA1c. Though, the use of insulin and/or gliclizade was associated with an increased risk of hypoglycaemia on hospital admission. Indeed, people with T2D prescribed insulin and/or gliclazide had a significantly higher HbA1c, and therefore the use of these drugs may better reflect these patients’ greater clinical need, with more significant or longer suboptimal glucose control in this group. However, hypoglycaemic events are known to be associated with falls and poor outcomes especially in those aged greater than 65 years [24]. Therefore, clinicians should consider the use of non-hypoglycaemia-inducing medications in the first instance in such a cohort of people with T2D, unless felt clinically necessary.. Importantly, these remain essential medications for older adults with poorly controlled T2D to prevent hyperglycaemic emergencies and should not be de-prescribed routinely, or avoided through fear of causing patient harm. Indeed, these data demonstrate a lack of association between insulin and/or gliclazide use and 1 year mortality outcomes. This requires the clinician to balance the risk and benefits of such a treatment strategy in the individual person with T2D [16,17,18,19,20], and to provide support for their use such as with community nursing care, frequently with secondary care diabetes team input. People prescribed insulin were most likely to have a hypoglycaemia-related fall during admission to hospital compared to those prescribed other agents including gliclazide. This is a well-known complication associated with insulin use, but an imperative take-home message. Nevertheless, gliclazide was also independently associated with increased hypoglycaemia-related admissions compared to other agents, showing that clinician selection of medications is important. This observation is relatively less well described in people admitted with falls compared with insulin use [24] and is another important clinical reminder of the impact of hypoglycaemia associated with the use of gliclazide in this at-risk cohort.
Logistic regression confirmed diagnosis of T2D was associated with 1-year mortality, but this was not significantly associated with hypoglycaemic-inducing agents. The increased mortality in those with T2D was associated with male sex [26], greater frailty [27] and polypharmacy [25]. This observation highlights the need for an individualised diabetes treatment plan and glycaemic targets for the older person with T2D. We found no difference with respect to social deprivation between those with T2D and mortality related to the use of hypoglycaemia inducing medications.
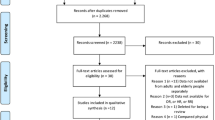
This study has some important limitations. Firstly, it is a cross-sectional with prospective follow-up in relation to mortality study, which is prone to usual biases associated with this type of study. To minimise this, patients with missing data and in this case these subjects were excluded from the analysis. In addition, limited information was available with respect to hospital readmission with often-incomplete routinely available electronic health records. Due to some patients being recently added to the databank, these do not have mortality outcomes at 12 months. There is a need for more robust prospective studies to adjust for such variables associated with mortality to infer causation between variables such as HbA1c, hypoglycaemia, medication use and polypharmacy in the cohort. Frailty is a dynamic measure, which is not fixed, and there can be a major bias in calculating the CFS especially when external factors such as cognitive impairment can limit someone’s functional ability [14]. This was mediated by all the CFS scores being checked by the same person (AJB), who was able to access each individuals’ comprehensive geriatric assessment including physiotherapy and occupational therapy assessments. The databank only focused on patients admitted with a fall, rather than other medical conditions or frailty syndromes. This limited comparison with people who did not fall to establish whether the mortality observed in this group was related to T2D or the underlying frailty syndrome itself. This could be expanded to look at frail, older adults in the community who have not fallen with T2D but are at a major increased risk of falls [28]. Further studies focusing on whether de-prescription actually affects the rate of falls or mortality would enable a more robust conclusion and would be of major clinical interest.
Conclusion
Falls are a significant burden, and hypoglycaemia-inducing agents may contribute to the greater mortality observed in people with T2D. People with T2D had a similar CFS, were more likely to be male and be prescribed more concomitant medicines. Clinician awareness can support de-prescribing for frail patients with HbA1c less than 64 mmol/mol. There should be increased awareness of the impact of hypoglycaemia, especially in those using insulin or gliclizade. Individualised care plans detailing co-morbidities, presence of frailty or functional loss (including cognition), individualised agreed goals of treatment, medications, frequency of monitoring, target capillary blood glucose and HbA1c, blood pressure and serum lipid levels are helpful.
Data availability
We consent to data sharing.
References
Rodríguez-Molinero A, Narvaiza L, Gálvez-Barrón C et al (2015) Falls in the Spanish elderly population: incidence, consequences and risk factors. Revista Espanola de Geriatria y Gerontologia 50:274–280
Rapp K, Freiberger E, Todd C et al (2014) Fall incidence in Germany: results of two population-based studies, and comparison of retrospective and prospective falls data collection methods. BMC Geriatr 14:105
Robertson K, Logan P, Ward M et al (2012) Thinking falls—taking action: a falls prevention tool for care homes. Br J Community Nurs 17:206–209
Shumway-Cook A, Ciol MA, Hoffman J et al (2009) Falls in the Medicare population: Incidence, associated factors, and impact on health care. Phys Ther 89:324–332
Tinetti ME, Speechley M, Ginter SF (1988) Risk factors for falls among elderly persons living in the community. N Engl J Med 319:1701–1707
Centers for Disease Control and Prevention (2016) Costs of falls among older adults. https://www.cdc.gov/falls/data/fall-cost.html. Accessed 5 Jan 2023
Just KS, Dormann H, Schurig M et al (2020) The phenotype of adverse drug effects: do emergency visits due to adverse drug reactions look different in older people? Results from the ADRED study. Br J Clin Pharmacol 86:2144–2154
Deandrea S (2010) Risk factors for falls in community-dwelling older people: a systematic review and meta-analysis. Epidemiology 21(5):658–668
GBD 2019 Ageing Collaborators. Global, regional, and national burden of diseases and injuries for adults 70 years and older: systematic analysis for the Global Burden of Disease 2019 Study. BMJ. 2022 Mar 10;376:e068208. https://doi.org/10.1136/bmj-2021-068208. PMID: 35273014; PMCID: PMC9316948.
World Health Organization (2021) Falls. Fact sheets. https://www.who.int/news-room/fact-sheets/detail/falls. Accessed 5 Jan 2023
Office for Health Improvement & Disparities (2021) Public health profiles (counties and UAs from April 2021). https://www.gov.uk/government/organisations/office-for-health-improvement-and-disparities/about/statistics. Accessed 5 Jan 2023
Public Health England (2022) Guidance—falls: applying all our health. https://www.gov.uk/government/publications/falls-applying-all-our-health/falls-applying-all-our-health. Accessed 5 Jan 2023
Burns E, Kakara R (2018) Deaths from falls among persons aged ≥ 65 years—United States, 2007–2016. MMWR Morb Mortal Wkly Rep 67:509–514
Hollinghurst J, Fry R, Akbari A, Clegg A, Lyons RA, Watkins A, Rodgers SE (2019) External validation of the electronic Frailty Index using the population of Wales within the Secure Anonymised Information Linkage Databank. Age Ageing 48(6):922–926. https://doi.org/10.1093/ageing/afz110
Charlson ME, Carrozzino D, Guidi J, Patierno C (2022) Charlson comorbidity index: a critical review of clinimetric properties. Psychother Psychosom 91:8–35
Joint British Diabetes Societies for Inpatient Care (2019) Inpatient care of the frail older adult with diabetes. https://www.diabetes.org.uk/resources-s3/2019-10/frailty-jbds-ipfinal-28-10-19.pdf. Accessed 5 Jan 2023
Association of British Clinical Diabetologists (2019) Managing frailty and associated comorbidities in older adults with diabetes: position statement on behalf of the Association of British Clinical Diabetologists (ABCD). https://abcd.care/sites/abcd.care/files/site_uploads/Resources/Position-Papers/ABCD-Position-Paper-Frailty.pdf. Accessed 5 Jan 2023
NICE. Type 2 diabetes in adults: management. https://www.nice.org.uk/guidance/ng28/chapter/Recommendations. Accessed 5 Jan 2023
NHS Digital (2019) National Diabetes Inpatient Audit England, 2019. https://files.digital.nhs.uk/F6/49FA05/NaDIA%202019%20-%20Full%20Report%20v1.1.pdf. Accessed 5 Jan 2023
Taverner S, Eng C, Watson R et al (2022) A series of diabetic ketoacidosis associated with the use of sodium-glucose co-transporter-2 inhibitors in secondary care. Diabetes Metab Syndr 16:102658
Yang Y, Hu X, Zhang Q, Zou R (2016) Diabetes mellitus and risk of falls in older adults: a systematic review and meta-analysis. Age Ageing 45:761–767
Crews RT, Yalla SV, Fleischer AE, Wu SC (2013) A growing troubling triad: diabetes, aging, and falls. J Aging Res 2013:342650
Zaccardi F, Davies MJ, Dhalwani NN et al (2016) Trends in hospital admissions for hypoglycaemia in England: a retrospective, observational study. Lancet Diabetes Endocrinol 4(8):677–685
Cheng LY, Leung SY, Leung MKW (2022) The association of glycemic control and fall risk in diabetic elderly: a cross-sectional study in Hong Kong. BMC Prim Care 23:192
Dhalwani NN, Fahami R, Sathanapally H, Seidu S, Davies MJ, Khunti K (2017) Association between polypharmacy and falls in older adults: a longitudinal study from England. BMJ Open 7:e016358
Gale EA, Gillespie KM (2001) Diabetes and gender. Diabetologia 44(1):3–15
Bertoni AG, Julie S et al (2002) Diabetes-related morbidity and mortality in a national sample of US elders. Diabetes Care 25:471–475
Vinik AI, Camacho P, Reddy S et al (2017) Aging, diabetes and falls. Endocr Pract 23:1117–1139
Funding
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Ethical approval
This is a quality improvement study. The Swansea Bay University Health Board Research Ethics Committee has confirmed that no ethical approval is required. Informed consent was obtained from all individual participants included in the study. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Burgess, A.J., Williams, D.M., Collins, K. et al. Diabetes management in older adults who fall: a study amongst older adults presenting to the emergency department. Eur Geriatr Med 14, 1105–1110 (2023). https://doi.org/10.1007/s41999-023-00848-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41999-023-00848-0