
Abstract
Previous studies have shown that caffeine can improve performance on cognitive tasks in adults, but little work has been done in children and adolescents, who use caffeine less habitually. The primary aim of this study was to test the hypothesis that acute caffeine enhances performance on cognitive tasks in children and adolescents. Two secondary aims were to determine if these effects differ as a function of sex, puberty, and menstrual cycle phase and if these effects can be attributed to withdrawal reversal. Children were given a cognitive test battery using the Automated Neurological Assessment Metrics (ANAM) before and 60 min after administration of placebo or caffeine (1 or 2 mg/kg). The number of correct responses and throughput on the Stroop task were increased after caffeine administration. Caffeine also decreased reaction time on the Stroop and decreased the standard deviation of the reaction time on the Go/No-Go task. We further analyzed these data based on presence or absence of withdrawal symptoms and by usual caffeine use and found that the effects of caffeine remained. We found interactions between sex and caffeine for Go/No-Go task time and the standard deviation of the reaction time on the Stroop task and an interaction between caffeine dose and menstrual cycle phase on the standard deviation of the reaction time on the Go/No-Go task. These results are consistent with previous studies showing caffeine facilitates performance on some cognitive tasks and that these improvements are not related to reversal of withdrawal effects. This study is among the first to report sex differences in responses to caffeine on cognitive tasks in children and adolescents.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Caffeine is the most widely consumed psychoactive stimulant in the world (Nawrot et al., 2003). While caffeine consumption in adults has been relatively stable in the past few decades, there has been an increase in availability and consumption of caffeine-containing products in children since the 1970s (Harnack et al., 1999). The majority of existing research on the effects of caffeine has been conducted in adults. With increased availability of sodas and energy drinks that are specifically marketed to children, it is important to understand how caffeine might affect this population differently (Clauson et al., 2003).
There have been numerous studies examining cognitive benefits after caffeine administration in adults, such as improved psychomotor performance, attention, and vigilance (Warburton, 1995; Jarvis, 1993; Kenemans & Lorist, 1995). Improvements in reaction time have been seen at doses ranging from 12.5 mg (Smit & Rogers, 2000) to above 250 mg (Rees et al., 1999). This suggests that even low doses of caffeine, in the range of what children may consume, can have an impact on cognitive performance. Some studies suggest the cognitive benefits of caffeine are stronger in caffeine consumers following short periods of abstinence (Smith et al., 1994). This may be due to acute caffeine reversing the detrimental effects of caffeine withdrawal (Rogers et al., 2013; Rogers et al., 2005). Others believe that caffeine administration can induce periods of increased focus and awareness in the absence of withdrawal reversal (Smith, 2002). Because children and adolescents use caffeine in lower amounts and with less regularity (Bernstein et al., 1998; Luebbe & Bell, 2009) and exhibit withdrawal symptoms less consistently than do adults (Bernstein et al., 1998; Heatherley et al., 2006), the mechanism for changes in cognitive performance after caffeine administration may be different in youth than in adults.
There is evidence in both adults and in children that caffeine can impact males and females differently. For example, caffeine use is associated with attenuation of cognitive decline in elderly women, but not in elderly men (Arab et al., 2011). In other cases, sex differences that exist in task performance, such as reaction time, have been shown to be eliminated after acute caffeine consumption (Botella et al., 2001). Our previous studies in children and adolescents have shown that many of the effects of caffeine differ as a function of sex, such as reinforcing value of beverages and subjective and cardiovascular responses to caffeine (Temple & Ziegler, 2011; Temple et al., 2009; Temple et al., 2014; Temple et al., 2015). To date, no studies have examined potential sex differences in the cognitive effects of caffeine among youth. In addition, few studies conducted in children and adolescents have investigated whether withdrawal reversal is the mechanism by which acute caffeine exerts its positive effects.
The primary aim of this study was to test the hypothesis that acute caffeine enhances performance on cognitive tasks in children and adolescents. Two secondary aims were to determine if these effects differ as a function of sex, puberty, and menstrual cycle phase and if these effects can be attributed to withdrawal reversal.
Methods
Participants and Recruitment
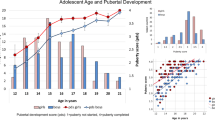
In order to recruit a population of participants who could be classified as pre-pubertal and post-pubertal, we enrolled 8–9- and 15–17-year-old boys and girls (n = 106). Eligibility criteria included lack of adverse reaction to caffeine, not using hormone-based contraceptives, non-smokers, not pregnant, or taking medication known to have interactions with caffeine (ex. medications for treatment of ADHD and depression) and willingness to visit the laboratory on six separate occasions for approximately 2 h each time. The 15–17-year-old girls had to be willing to monitor their menstrual cycles and ovulation. One hundred six participants enrolled in the study, but five participants withdrew from the study due to scheduling conflicts (n = 3), reported dizziness (n = 1), and having pubertal scores that were between 2 and 4 (n = 1), and five more participants were removed due to incomplete data, leaving a total of 96 participants to be used in the analysis: male (n = 26) and female (n = 24) ages 8–9 years and males (n = 26) and females (n = 20) 15–17 years.
Experimental Procedures
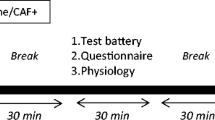
The study presented here was part of a larger double-blind, placebo-controlled, dose-response study. In the original study (Temple et al., 2014), participants visited the laboratory six times, with three visits scheduled in 1 week with a day in between each and three visits scheduled 2 weeks later. For post-pubertal girls, three sessions occurred during the mid-follicular phase and three visits occurred during the mid-luteal phase. Since these phases were approximately 2 weeks apart from each other, the pre-pubertal participants and post-pubertal males had each set of visits scheduled 2 weeks apart. In each set of visits, participants had 0, 1, or 2 mg/kg of caffeine given in the same order. Prior to their first visit, participants were randomized to one of six orders of caffeine administration, with the order being the same for the first and second weeks of the study. Therefore, participants had the same dose of caffeine in visits 1 and 4, visits 2 and 5, and visits 3 and 6. The cognitive testing for the current study was conducted on visits 2 and 5. Therefore, approximately one third of participants had placebo on these visits (n = 30), one third had 1 mg/kg of caffeine (n = 31), and the last third had 2 mg/kg of caffeine (n = 34). Participants were instructed to abstain from caffeine for 24 h and food or drink (besides water) for 2 h prior to each visit. Upon arrival to the laboratory, participants and parents read and signed consent and assent forms. Although caffeine was the only thing that was added to these beverages, in order to reduce expectancies about the effects of caffeine, parents and participants were told that the beverages used in the study may have one or more of the following substances manipulated: sugar, aspartame, Splenda®, caffeine, or artificial coloring. Participants then completed a 24-h dietary recall, the Caffeine Symptom Questionnaire, and same-day physical activity recall questionnaire with the aid of a trained research assistant. During this time, parents completed a demographic questionnaire and were then escorted to the waiting area. At this time, parents and participants separately completed Tanner stage to assess pubertal status. Participants were then asked to provide saliva samples for hormone assays. The participant then had their height and weight measured. Participants then completed the cognitive testing battery (ANAM) described below before and 1 h after consuming 300 mL of their preferred beverage (Sierra Mist™, orange juice, or lemonade) containing either placebo or 1 or 2 mg/kg of caffeine. Participants were given 5 min in which to consume the entire beverage. These beverages were chosen because they are not caffeinated and participants would not have expectancy about caffeine being contained within these beverages. The sugar and energy content of these beverages ranged from 22 to 28 g and 127 to 152, respectively. In the larger study, participants had blood pressure and heart rate measured every 10 min over this time period (Temple et al., 2014). The study design is outlined in Table 1. The study protocol was approved by the Social and Behavioral Sciences Institutional Review Board at The University at Buffalo.
Measurements
Weight, Height, and BMI
Youth weight was assessed by use of a digital scale (SECA). Height was assessed using a SECA stadiometer. Body weight was used to determine the amount of placebo or caffeine given.
Demographic Questionnaire
This questionnaire was used to assess parental education, occupation, household income, employment status, and parental and participant race and ethnicity.
Tanner Stage Evaluation
Participants and parents were given line drawings of the five stages of pubertal development and asked to circle the one that looked most like them/their child. The 8–9-year-olds had to report a Tanner score of 2 or less in order to be considered pre-pubertal. The 15–17-year-olds had to report a Tanner score of 4 or higher to be considered post-pubertal. Self-assessment of pubertal stage has been shown to be accurate and an acceptable substitute when physical examinations are not feasible (Bonat et al., 2002; Schlossberger et al., 1992).
Caffeine Use Questionnaire
This questionnaire was adapted from Miller (2008) and assessed sources, amounts, and frequency of caffeinated food and beverage intake as well as reasons why children and adolescents used and/or did not use caffeine (Warburton, 1995; Hewlett & Smith, 2007; Smith et al., 2013). Participants were asked if they drink a variety of beverages including coffee, tea, soda, and energy drinks. They were then asked how often they drink these beverages. The possible responses ranged from every day to once a month. They were then asked how much they drink at a time of one of these beverages. The possible responses ranged from less than one to more than seven cups. They were then asked the same questions about chocolate and caffeine pills. Using this information along with the caffeine estimates in the drinks and food from the US Department of Nutritional Services, their average daily caffeine intake was calculated.
Caffeine Symptom Questionnaire
This questionnaire, containing 31 adjectives or short phrases describing mood and psychological symptoms associated with caffeine withdrawal or use (Temple et al., 2009; Greden et al., 1981; Griffiths & Woodson, 1988; Richardson et al., 1996; Richardson et al., 1995; Temple et al., 2012), was administered at baseline and 60 min after drink consumption. The participant was asked to pick the number of the scale for each word or phrase that described how they feel “right now” on a 5-point Likert-type scale starting with “Not at all” (1) and ending with “Extremely” (5). The terms on this questionnaire were grouped according to a recent manuscript by Juliano et al. (Juliano et al., 2012) into seven categories (drowsiness/fatigue; decreased alertness/difficulty concentrating; mood disturbances; decreased sociability/motivation to work; nausea/stomach upset; flu-like feelings; headache).
ANAM Battery
The Automated Neurological Assessment Metrics (ANAM) cognitive testing battery was initially developed by the Department of Defense and is used by the military and sports medicine practitioners for concussion and mild traumatic brain injury surveillance (Cernich et al., 2007). We selected a subset of the testing battery (six tests) that had previously been administered to children: sleepiness scale, simple reaction time, 2-choice reaction time, memory search, Stroop, and Go/No-Go. The battery was administered on a laptop computer. The software provided each participant with the same test variables, but the order of the variables differed each time they took a particular test. This was meant to reduce the practice effect. The number keys 1, 2, and 3 were color-coded based on the Stroop test’s instructions, and the mouse buttons were labeled as “1” and “2” for tests that required mouse clicking. The dependent measures used in this study are reaction time, standard deviation of the reaction time (a measure of response variability), number correct, and percent correct.
Sleepiness Scale
This test permits self-assessment of the user’s sleep/fatigue state. Given that the primary effect of caffeine is to reduce fatigue and sleepiness and improve alertness and wakefulness, we included this scale. The user was presented with seven different statements of alertness/sleepiness, ranging from “Feeling very alert, wide awake, and energetic” to “Very sleepy and cannot stay awake much longer.” The user was instructed to select the one statement that best matches his/her current state. This task took approximately 30 s for the participant to complete.
Simple Reaction Time
The SRT task measures response speed to the presentation of a single stimulus by presenting the user with a series of “x” symbols on the display. The user was instructed to respond as quickly as possible by pressing a button each time the stimulus appears. There were 40 trials with an inter-trial interval of 750–1350 ms. This task took approximately 1 min for the participant to complete.
2-Choice Reaction Time
The 2CH task measures differential response speed to two different stimuli by presenting the user with an “x” or “o” on the display. The user was instructed to respond as quickly as possible by pressing the designated button for each stimulus as soon as the stimulus appeared. There were 40 trials with an inter-trial interval of 750–1350 ms. This task took approximately 1 min for the participant to complete.
Memory Search
This test assessed working memory and sustained attention. A set of six letters was displayed in a horizontal line for a maximum of 10 s. Then, individual letters were displayed and the participant was instructed to press designated buttons to indicate if each character was or was not a member of the memorized set. This task consisted of 40 trials and took approximately 2 min for the participant to complete.
Stroop Test
The Stroop test evaluated focused attention and integrated cognitive mechanisms. There were three sections for this task with participants instructed to complete as many trials in 45 s as they could complete accurately. In the first section, participants were asked to read the names of different colors (neutral stimulus). In the second section, participants were asked to name the color of a line of X’s (congruent stimulus). In the third section, they were asked to name the printed color of a word denoting a different color; for example, they read the word “blue” printed in green (color-word interference; incongruent stimulus). This task took approximately 3 min for the participant to complete.
Go/No-Go Test
This test was used to measure a participant’s capacity for sustained attention and response control. The user was presented with either an “x” or “o” on the display. The “x” was the target. The user then pressed a button as quickly as they could every time they saw the target (“x”). They were told not to press the button if they were presented with “o.” The display duration was 500 msec and participants completed 40 trials. This task took approximately 2 min for the participant to complete.
Analytic Plan
Participant characteristics, measured on the initial laboratory visit only, were analyzed using analysis of variance (ANOVA) with pubertal stage and sex as between-subjects variables for continuous variables (age and caffeine use) and chi-squared analyses for categorical variables (ex. race, income, and education). These results are shown in Table 1. When we looked at the entire study population, there were no differences between visit 2 and visit 5, so these data were averaged for statistical analysis. Results from the cognitive tests were analyzed as change from pre to post using a mixed analysis of covariance (ANCOVA) with pubertal stage, sex, and caffeine treatment dose as between-subjects variables and usual caffeine intake as the covariate. We conducted further analysis of the caffeine effects to account for potential influences of withdrawal reversal. First, we grouped participants into three different caffeine use groups: low (< 25 mg/day), moderate (25–75 mg/day), and high (> 75 mg/day) and reanalyzed the data using a mixed ANOVA with caffeine treatment and caffeine use group as between-subjects variables. For these analyses, caffeine use was no longer considered as a covariate. Second, we classified responses on the Caffeine Symptom Questionnaire into seven different caffeine withdrawal factors according to Juliano and colleagues (Juliano et al., 2012) and used the composite score to classify individuals into caffeine withdrawal groups based on a median split (no withdrawal < 1.5 and withdrawal ≥ 1.5). We then repeated the analysis of the cognitive tests where we found an effect of caffeine using a mixed ANOVA with caffeine treatment and withdrawal symptom group as between-subjects variables. In addition, for post-pubertal girls only, the effects of menstrual cycle phase (follicular vs. luteal phase) on cognitive effects of caffeine were analyzed using a mixed ANCOVA with caffeine dose as the between-subjects variable and menstrual cycle phase as the within-subjects variable, and usual caffeine intake as the covariate. When significant interactions were found in the ANCOVA and ANOVA analyses, post hoc comparisons were conducted using linear contrasts with a Bonferroni correction for multiple comparisons (significance set at p < 0.017). All analyses were conducted using SYSTAT 12.0 and differences were considered statistically significant if p < 0.05.
Results
Participant Characteristics
Ninety-six participants (male (n = 26) and female (n = 24) participants ages 8–9 years and males (n = 26) and females (n = 20) 15–17 years) were included in the analyses. Table 2 shows the mean ± SEM for age, BMI, and average daily caffeine consumption of participants in each group. The sample was predominantly white (80%) and black or African American (17%) from middle class families where at least one parent had completed college or graduate school (73%). Additionally, the post-pubertal participants had higher daily caffeine intake and BMI and were older than the pre-pubertal participants (p < 0.0001). The groups did not differ in race, parental education, or income (all p > 0.05). There was also no difference in the choice of beverage (Sierra Mist™, lemonade, or orange juice) among the groups (χ2 = 1.8; p = 0.76), with the overwhelming majority of participants (75%) choosing Sierra Mist™, followed by 18% choosing lemonade and only 7% choosing orange juice.
Caffeine Withdrawal Symptoms
In order to analyze caffeine withdrawal symptoms, we grouped responses on the Caffeine Symptom Questionnaire into seven factors (as described above). We compared responses for those seven factors before and 60 min after caffeine administration as a function of sex, pubertal stage, and caffeine use group (Table 3). We found no difference in withdrawal symptoms as a function of sex (all p > 0.05) or pubertal stage (all p > 0.05). We did find a main effect of caffeine treatment on factors 1, 4, 5, and 6 (all p < 0.05). None of the factors differed as a function of usual caffeine use except factor 4 (p < 0.05), where individuals in the high use group showed a significant decrease in sociability/motivation to work that was not observed in the other caffeine use groups.
Effects of Caffeine on Cognitive Test Results
ANCOVA analysis revealed that there was an effect of caffeine dose on some, but not all, of the cognitive tests. We found a main effect of caffeine dose on the number correct in the Stroop task (F(2, 83) = 3.5, p = 0.04), with both doses of caffeine increasing the number correct relative to the placebo group. There was also a main effect of caffeine dose on reaction time on the Stroop task (F(2, 83) = 3.2; p = 0.048), with both doses of caffeine decreasing reaction time relative to placebo. There was a main effect of caffeine dose on throughput (number correct/min) on the Stroop task (F(2, 83) = 3.3; p = 0.042), with both doses of caffeine increasing throughput compared with placebo. Finally, there was a main effect of caffeine dose on the standard deviation of the reaction time on the Go/No-Go task (F(2, 83) = 4.8; p = 0.01), with both doses of caffeine reducing the standard deviation compared with placebo (Fig. 1). The significance of these effects was not altered by having usual caffeine use as a covariate. When we group participants into low (n = 46), moderate (n = 25), and high (n = 25) caffeine use groups and reanalyzed the data, we found that the effects of caffeine on these cognitive test results remained, even in the lowest caffeine use group (all p < 0.05; Fig. 2). Next, we separated participants into low (n = 53) and high (n = 43) withdrawal groups and found that the effects of caffeine on cognitive functioning remained (all p < 0.05).

Effects of caffeine on cognitive function. Mean + SEM change from baseline for a) number correct on the Stroop, b) reaction time on the Stroop task, c) throughput (number correct/min) on the Stroop task, and d) standard deviation of the reaction time on the Go/No-Go task in participants who received 0, 1, or 2 mg/kg of caffeine. * = significantly different from placebo (p < 0.05)

Effects of caffeine on cognitive function in different caffeine use groups (< 25 mg/day, 25–75 mg/day, and > 75 mg/day). Mean + SEM change from baseline for a) number correct on the Stroop, b) reaction time on the Stroop task, c) throughput (number correct/min) on the Stroop task, and d) standard deviation on the Go/No-Go task in participants who received 0, 1, or 2 mg/kg of caffeine. * = significantly different from placebo (p < 0.05)
Effects of Sex, Menstrual Cycle, and Caffeine Dose on Cognitive Test Results
There were no main effects of sex or menstrual cycle phase on performance on the cognitive tasks. There was a significant interaction between sex and caffeine dose on reaction time on the Go/No-Go task (F(2, 83) = 3.8; p = 0.026), with females having lower reaction time on the Go/No-Go task than males after placebo, but no differences after 1 or 2 mg/kg. There was also a significant interaction between sex and caffeine dose on the standard deviation of the reaction time on the Stroop task (F(2, 83) = 4.7; p = 0.012), with males having a greater reduction from baseline than females after placebo, but no differences after 1 and 2 mg/kg doses of caffeine (Fig. 3). We found an interaction between caffeine dose and menstrual cycle phase on the standard deviation of reaction time in the Go/No-Go task (F(2, 17) = 7.7; p = 0.004). Linear contrasts revealed that all doses were significantly different from each other in the luteal phase of the menstrual cycle (1 and 2 mg/kg, F(1, 3) = 10.5; p = 0.007, 0 and 2 mg/kg, F(1, 11) = 30.9; p < 0.0001, and 0 and 1 mg/kg, F(1, 10) = 11.1; p = 0.008). The standard deviation of reaction time during the follicular phase of the menstrual cycle was not statistically different by dose. The significance of these effects was not altered by having usual caffeine use as a covariate.

Sex differences in response to caffeine. Mean + SEM change from baseline for reaction time in the Go/No-Go task (left) and standard deviation of the reaction time on the Stroop task (right) in males (black) and females (gray) who received 0, 1, or 2 mg/kg of caffeine. There was a sex difference in the 0 mg/kg group, but not in the 1 mg/kg or 2 mg/kg groups. Different letters denote conditions that are significantly different from each other (p < 0.05)
Discussion
The purpose of this study was to test the hypothesis that caffeine affects cognitive functioning and that its effects differ as a function of sex, pubertal phase, and menstrual cycle phase. In addition, we sought to determine the extent to which cognitive effects of caffeine are due to withdrawal reversal. In all age groups, caffeine improved performance on the Stroop task and a reduction in the standard deviation of the reaction time on the Go/No-Go task, which is an index of variability. There were no significant differences between the 1 and 2 mg/kg doses on any of the measures, and the effects remained when we controlled for usual caffeine consumption and for caffeine withdrawal symptoms. Males and females differed in responses on the Go/No-Go and Stroop tasks after placebo administration, but the sex differences were no longer present after caffeine. In the post-pubertal girls, there was a reduction in the standard deviation of the reaction time in the Go/No-Go task as caffeine dose increased during the luteal phase of the menstrual cycle, but not the follicular phase. There were no differences observed as a function of menstrual cycle phase for any of the other tasks. When taken together, these findings suggest that caffeine reduces reaction time and increases correct responses on the Stroop task in children and adolescents, but that these effects are not strongly influenced by sex or menstrual cycle phase. In addition, caffeine only had an effect on a subset of cognitive tasks, suggesting that caffeine does not have broad general effects on all aspects of cognitive functioning, but rather may be specific to certain tasks.
Our study showed that caffeine increased the number correct and throughput and reduced reaction time on the Stroop task. This is consistent with studies conducted in adults. For example, a study by Kenemens et al. (1999) showed that caffeine decreased interference, number of omissions, reaction time, and number of errors on the Stroop task (Kenemans et al., 1999). We also showed that caffeine reduced the standard deviation of the reaction time in the Go/No-Go task, but did not affect any other measures related to this task. Previous studies have shown that both 250 and 50 mg of caffeine decreased reaction time on the Go/No-Go task, but only the 50 mg reduced the number of errors (Barry et al., 2007; Foxe et al., 2012). The differences between our study and those published previously may be related to differences in the age of participants (children vs. adults), inconsistent abstinence instructions, and potential impacts of withdrawal reversal in adults that were not observed in our study in children. Our findings are consistent with previous studies showing that caffeine does not result in improvement in all measures of cognitive function, but may enhance performance on a subset of cognitive responses or specific cognitive tasks (Nehlig, 2010). For example, the majority of the positive effects of caffeine in our study were specific to the Stroop Task, which may indicate that caffeine can enhance processing speed (Dixit et al., 2012). We did not find significant improvements on accuracy on the Go/No-Go task, which is consistent with other studies in the literature (Marczinski et al., 2014) and may indicate that caffeine does not improve inhibitory control.
We found an interaction between sex and caffeine administration for the Stroop task and Go/No-Go task. Specifically, we found sex differences in task performance in the placebo condition that were not present in the caffeine groups. Other studies have also shown sex differences in performance on cognitive tasks without administration of caffeine. A study by Pesta and colleagues (2008) found that males had a significantly faster reaction time than females in a basic reaction time task (Pesta et al., 2008). In another study examining simple reaction time, men had faster reaction times than women (Mucignat-Caretta, 1998). Golden (1974) showed women performed better on the Stroop test than men (Golden, 1974). Previous studies from our laboratory and others have shown that caffeine has differential effects in males and females (Luebbe & Bell, 2009; Miller, 2008). For example, boys find caffeinated soda more reinforcing than girls and were more likely to report getting a rush or more energy from caffeine (Temple & Ziegler, 2011; Temple et al., 2009; Temple et al., 2015). One interpretation of this is that boys may be sensitive or more responsive to acute caffeine administration. The current results are consistent with some sex differences in response to caffeine. For example, boys had a significantly greater reduction in reaction time on the Go/No-Go task after 1 mg/kg compared with placebo, but there were no differences in girls in response to caffeine. We also found an interaction between caffeine dose and menstrual cycle phase on the standard deviation of reaction time in the Go/No-Go, where variability was reduced by both doses of caffeine relative to placebo, with the 2 mg/kg dose having a greater effect than the 1 mg/kg dose. There were no other main effects or interactions between sex or menstrual cycle phase and cognitive responses after caffeine intake. When taken together, these results suggest that, while caffeine had several main effects on performance on cognitive tasks, there were limited interactions with sex and menstrual cycle phase.
One potential mechanism for cognitive improvement by caffeine is withdrawal reversal. The majority of studies on the effects of caffeine on cognitive function utilize people who regularly consume caffeine and who are instructed to abstain from caffeine prior to the study. If these habitual users demonstrate physical dependence, abstinence leads to withdrawal symptoms such as headache, fatigue, and difficulty concentrating (Griffiths et al., 1990; Juliano & Griffiths, 2004). Thus, withdrawn consumers may have diminished performance on cognitive tasks than would be expected in non-habitual users of caffeine. Once caffeine is administered, often cognitive performance is improved, but this apparent improvement may be due to the reversal of the detriment seen with caffeine deprivation and not a true cognitive improvement. Other studies suggest that caffeine can have a positive impact on cognitive performance in the absence of withdrawal reversal (Warburton, 1995; Hewlett & Smith, 2007; Smith et al., 2013). For example, a study by Smith and colleagues showed that non-caffeine consumers and withdrawn consumers had improvements in several domains of cognitive performance after acute caffeine administration, suggesting that caffeine effects are not due to withdrawal reversal alone (Smith et al., 2013). In order to test primary cognitive enhancement of caffeine, it may be best to use individuals who do not regularly consume caffeine, but the widespread prevalence of caffeine consumption in the adult population makes this difficult (James & Rogers, 2005). This is one advantage of conducting these studies in children, who have lower and less habitual use when compared with adults (Heatherley et al., 2006; Barone & Roberts, 1984). When we examined our results as a function of usual caffeine use, we found that the cognitive effects remained, even in the group of participants that consume less than 25 mg of caffeine per day. When we examined the data in individuals who are low and high for caffeine withdrawal symptoms, we also found that the effects of caffeine on cognition remained, although the endorsement of withdrawal symptoms was universally low in this study (average 1.5 on a scale from 1 to 9). When taken together, these data suggest that the cognitive effects of caffeine observed in children and adolescents may be the result of positive effects of caffeine and not withdrawal reversal. Future studies need to examine this further by using long-term withdrawn consumers, by having a typical caffeine consumption control and by replicating the findings from this study under these conditions.
This study had several strengths. First, we used a double-blind, placebo-controlled, within-subjects, dose-response design. Second, we used children and adolescents, which are understudied populations in regard to caffeine use. Third, this may be the first study examining the effects of caffeine on cognitive performance across different developmental stages and the menstrual cycle. This study was not without limitations. First, our sample was homogenous in terms of race, income, and education. This limits the ability for us to generalize our findings to the general population because our sample was mainly from white, well-educated, upper-middle class populations. Second, by instructing participants to abstain from caffeine prior to each visit, we may have increased their awareness of caffeine manipulation. However, since there were three different dosages which they received twice, this awareness might not have impacted our findings. Third, we relied on the post-pubertal girls to report when they began menstruation and ovulation and confirmed with salivary steroid hormones, which is not as reliable as taking measurements of steroid hormones in the blood. Fourth, we examined withdrawal symptoms using a Caffeine Symptom Questionnaire, but responses on this questionnaire may have not been highly reliable in the age groups in which we examined. Fifth, we did not assess the age of caffeine initiation or any measure of historical caffeine use. Finally, we examined withdrawal reversal by grouping participants by usual caffeine use and by caffeine withdrawal symptoms, but this may not be the best way to control for withdrawal reversal.
In sum, this study adds to the growing body of literature on the effects of caffeine in children and adolescents. We demonstrated that caffeine improved performance on the Stroop task primarily by reducing reaction time and by improving accuracy. Our data also suggest that these effects were primary positive effects of caffeine and not a reversal of withdrawal-induced deficits on the task, as we found little evidence of withdrawal symptoms and the effects was unchanged when we controlled for usual caffeine intake. This work provides a foundation on which to build future studies that examine the impact of higher doses of caffeine and test mediators of these effects, such as attention and alertness.
References
Arab, L., et al. (2011). Gender differences in tea, coffee, and cognitive decline in the elderly: the Cardiovascular Health Study. Journal of Alzheimer’s Disease, 27(3), 553–566.
Barone, J.J., Roberts, H., Human consumption of caffeine. Caffeine, ed. P.B. Dews. 1984: Springer Berlin Heidelberg.
Barry, R. J., et al. (2007). Caffeine effects on ERPs and performance in an auditory Go/NoGo task. Clinical Neurophysiology, 118(12), 2692–2699.
Bernstein, G. A., et al. (1998). Caffeine withdrawal in normal school-age children. Journal of the American Academy of Child & Adolescent Psychiatry, 37(8), 858–865.
Bonat, S., et al. (2002). Self-assessment of pubertal stage in overweight children. Pediatrics, 110(4), 743–747.
Botella, P., et al. (2001). Sex differences in estimation of time intervals and in reaction time are removed by moderate but not high doses of caffeine in coffee. Human Psychopharmacology, 16(7), 533–540.
Cernich, A., et al. (2007). Automated Neuropsychological Assessment Metrics sports medicine battery. Archives of Clinical Neuropsychol, 22(Suppl 1), S101–S114.
Clauson, K. A., et al. (2003). Safety issues associated with commercially available energy drinks. J Am Pharm Assoc, 48(3), e55–e63 2008.quiz e64–7.
Dixit, A., et al. (2012). Effect of caffeine on information processing: evidence from stroop task. Indian J Psychol Med, 34(3), 218–222.
Foxe, J. J., et al. (2012). Assessing the effects of caffeine and theanine on the maintenance of vigilance during a sustained attention task. Neuropharmacology, 62(7), 2320–2327.
Golden, C. J. (1974). Sex difference in performance on the Stroop color word test. Perception and Motor Skills, 39, 1067–1070.
Greden, J. F., Procter, A., & Victor, B. (1981). Caffeinism associated with greater use of other psychotropic agents. Comprehensive Psychiatry, 22(6), 565–571.
Griffiths, R. R., & Woodson, P. P. (1988). Caffeine physical dependence: a review of human and laboratory animal studies. Psychopharmacology, 94(4), 437–451.
Griffiths, R. R., et al. (1990). Low-dose caffeine physical dependence in humans. The Journal of Pharmacology and Experimental Therapeutics, 255(3), 1123–1132.
Harnack, L., Stang, J., & Story, M. (1999). Soft drink consumption among US children and adolescents: nutritional consequences. J Am Diet Assoc, 99(4), 436–441.
Heatherley, S. V., Hancock, K. M. F., & Rogers, P. J. (2006). Psychostimulant and other effects of caffeine in 9- to 11-year-old children. Journal of Child Psychology and Psychiatry, 47(2), 135–142.
Hewlett, P., & Smith, A. (2007). Effects of repeated doses of caffeine on performance and alertness: new data and secondary analyses. Human Psychopharmacology, 22(6), 339–350.
James, J. E., & Rogers, P. J. (2005). Effects of caffeine on performance and mood: withdrawal reversal is the most plausible explanation. Psychopharmacology, 182(1), 1–8.
Jarvis, M. J. (1993). Does caffeine intake enhance absolute levels of cognitive performance? Psychopharmacology, 110(1–2), 45.
Juliano, L. M., & Griffiths, R. R. (2004). A critical review of caffeine withdrawal: empirical validation of symptoms and signs, incidence, severity, and associated features. Psychopharmacology, 176(1), 1–29.
Juliano, L. M., et al. (2012). Development of the caffeine withdrawal symptom questionnaire: caffeine withdrawal symptoms cluster into 7 factors. Drug and Alcohol Dependence, 124(3), 229–234.
Kenemans, J. L., & Lorist, M. M. (1995). Caffeine and selective visual processing. Pharmacology, Biochemistry and Behavior, 52(3), 461–471.
Kenemans, J. L., et al. (1999). Caffeine and stroop interference. Pharmacology, Biochemistry, and Behavior, 63(4), 589–598.
Luebbe, A. M., & Bell, D. J. (2009). Mountain dew or mountain don’t?: a pilot investigation of caffeine use parameters and relations to depression and anxiety symptoms in 5th- and 10th-grade students. The Journal of School Health, 79(8), 380.
Marczinski, C. A., et al. (2014). Subjective state, blood pressure, and behavioral control changes produced by an “energy shot”. Journal Caffeine Research, 4(2), 57–63.
Miller, K. E. (2008). Wired: energy drinks, jock identity, masculine norms, and risk taking. Journal of American College Health, 56(5), 481–489.
Mucignat-Caretta, C. (1998). Changes in female cognitive performance after energetic drink consumption: a preliminary study. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 22(6), 1035–1042.
Nawrot, P., et al. (2003). Effects of caffeine on human health. Food Additives and Contaminants, 20(1), 1–30.
Nehlig, A. (2010). Is caffeine a cognitive enhancer? Journal of Alzheimer’s Disease, 20(Suppl 1), S85–S94.
Pesta, B. J., Bertsch, S., Poznanski, P. J., & Bommer, W. H. (2008). Sex differences on elementary cognitive tasks despite no differences on the Wonderlic Personality Test. Personality and Individual Differences, 45, 429–431.
Rees, K., Allen, D., & Lader, M. (1999). The influences of age and caffeine on psychomotor and cognitive function. Psychopharmacology, 145(2), 181–188.
Richardson, N. J., et al. (1995). Mood and performance effects of caffeine in relation to acute and chronic caffeine deprivation. Pharmacology, Biochemistry, and Behavior, 52(2), 313–320.
Richardson, N. J., Rogers, P. J., & Elliman, N. A. (1996). Conditioned flavour preferences reinforced by caffeine consumed after lunch. Physiology & Behavior, 60(1), 257–263.
Rogers, P., et al. (2005). Effects of caffeine and caffeine withdrawal on mood and cognitive performance degraded by sleep restriction. Psychopharmacology, 179(4), 742–752.
Rogers, P., et al. (2013). Faster but not smarter: effects of caffeine and caffeine withdrawal on alertness and performance. Psychopharmacology, 226(2), 229–240.
Schlossberger, N. M., Turner, R. A., & Irwin Jr., C. E. (1992). Validity of self-report of pubertal maturation in early adolescents. The Journal of Adolescent Health, 13(2), 109–113.
Smit, H. J., & Rogers, P. J. (2000). Effects of low doses of caffeine on cognitive performance, mood and thirst in low and higher caffeine consumers. Psychopharmacology, 152(2), 167–173.
Smith, A. (2002). Effects of caffeine on human behavior. Food and Chemical Toxicology, 40(9), 1243–1255.
Smith, A., et al. (1994). Effects of breakfast and caffeine on cognitive performance, mood and cardiovascular functioning. Appetite, 22(1), 39–55.
Smith, A. P., Christopher, G., & Sutherland, D. (2013). Acute effects of caffeine on attention: a comparison of non-consumers and withdrawn consumers. Journal of Psychopharmacology, 27(1), 77–83.
Temple, J. L., & Ziegler, A. M. (2011). Gender differences in subjective and physiological responses to caffeine and the role of steroid hormones. Journal of Caffeine Research, 1, 41–48.
Temple, J. L., et al. (2009). Sex differences in reinforcing value of caffeinated beverages in adolescents. Behavioural Pharmacology, 20(8), 731–741.
Temple, J. L., et al. (2012). Influence of caffeine on the liking of novel-flavored soda in adolescents. Psychopharmacology, 223(1), 37–45.
Temple, J. L., et al. (2014). Cardiovascular responses to caffeine by gender and pubertal stage. Pediatrics, 134(1), e112–e119.
Temple, J. L., et al. (2015). Subjective responses to caffeine are influenced by caffeine dose, sex, and pubertal stage. Journal Caffeine Research, 5(4), 167–175.
Warburton, D. M. (1995). Effects of caffeine on cognition and mood without caffeine abstinence. Psychopharmacology, 119(1), 66.
Funding
The authors thank our funding sources, including R01 DA030386 to JLT and a fellowship from the University at Buffalo Gender Institute to AMG.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study protocol was approved by the Social and Behavioral Sciences Institutional Review Board at The University at Buffalo.
Conflict of Interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Graczyk, A.M., Ziegler, A.M., Bendlin, A. et al. Effects of Caffeine Administration on Reaction Time, Attention, and Inhibitory Control in Children and Adolescents. J Cogn Enhanc 2, 276–286 (2018). https://doi.org/10.1007/s41465-018-0074-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41465-018-0074-3